
Abstract
Purpose:
Minor hand surgeries can be done under field sterility in procedure rooms. Surgeons are still sceptical about the usage of wide awake local anaesthesia no tourniquet (WALANT) technique. They perceive that patients can tolerate tourniquet for a brief period while they perform minor surgeries under local anaesthesia (LA). We compared the perceived comfort experienced by patients during minor hand surgeries with WALANT and LA/tourniquet. We investigated the difference in preoperative preparation time, operating time and blood loss between the two groups.
Methods:
Between July and October 2016, a total of 72 patients were diagnosed with carpal tunnel syndrome, trigger finger or ganglion, at the University Malaya Medical Centre. Forty patients consented to participate in this study and were randomized into WALANT and LA/tourniquet groups. Anaesthesia was administered accordingly and tourniquet was applied. The time taken for preoperative preparation and surgery was recorded. Each surgeon estimated the blood loss. The perceived comfort level of each patient was quantified using a visual analogue score (VAS). Data were analysed using SPSS.
Results:
The mean VAS for the WALANT group was 2.33 ± 1.94, whereas it was 4.72 ± 3.05 for the LA/tourniquet group, and the difference was statistically significant (p < 0.05). The mean time for preoperative preparation in WALANT group was 19.17 ± 12.61 min and LA/tourniquet group was 7.05 ± 3.44 min. The difference between these groups was statistically significant (p < 0.01). There was no significant difference in operating time and blood loss.
Conclusion:
WALANT technique was associated with better patient comfort. Tourniquet was the main reason for discomfort during surgeries. WALANT is an alternative in minor hand surgeries for a bloodless surgical field without the discomfort of tourniquet application.
Introduction
The tourniquet is a device used conventionally to minimize blood loss and create a bloodless surgical field in minor hand surgeries. A bloodless surgical field is important in order to perform a good surgery under magnification. 1 Local anaesthesia (LA) is useful for minor procedures as the risk of general anaesthesia can be averted.
However, tourniquet usage can be disabling and painful when used in the absence of general anaesthesia or brachial plexus block. In two independent studies on tourniquet tolerance among healthy volunteers, the average tolerance to forearm tourniquet was 13 and 25 min, respectively. Both studies reported that arm tourniquet was less tolerable compared to forearm tourniquet. Participants experienced temporary pain and paraesthesia. 2,3 Complete paralysis was experienced within 7 minutes of forearm tourniquet inflation. 2 Prolonged tourniquet usage may cause nerve damage, leading to transient neurological deficit. 4
Usage of tourniquet can be avoided if haemostasis can be achieved with other methods. Epinephrine infiltration causes vasoconstriction and is capable of minimizing bleeding, effective enough not to interfere with the quality of surgery. 5,6 Previously, epinephrine was forbidden in finger surgeries, as there were reported cases of complications. It has been proved that necrosis of fingers were due to expired procaine. 7 Lately, there are many studies that have proved the safety and efficacy of epinephrine in hand surgeries. 5 –7 WALANT (wide awake local anaesthesia no tourniquet) is a technique where lidocaine and epinephrine are injected for LA and vasoconstriction effect, respectively, in order to allow surgeries to be done without the use of tourniquet.
It may appear that in minor surgeries, there is no difference in the outcome of surgery between WALANT and LA/tourniquet. The duration of surgery and the amount of blood loss may not be significant. However, we believe that the application of tourniquet even for a short duration of time may cause discomfort. It has been reported that the severity of tourniquet pain in carpal tunnel release was twice compared to LA/epinephrine injection. 8
We attempt to quantify the perceived comfort level of patients, in general, undergoing minor hand surgeries in our operating theatre, comparing WALANT and LA/tourniquet. We also investigated the difference in operating time, preoperative time and blood loss between these groups.
Methods
This study was conducted at the University Malaya Medical Centre from July to October 2016. Those who were eligible for this study were patients who had been diagnosed with carpal tunnel syndrome, trigger finger or ganglion by a specialist in the orthopaedic clinic. A total of 72 patients fulfilled the criteria. Forty patients who had consented to participate and were scheduled for surgery were equally randomized into two groups by drawing lots: WALANT and LA/tourniquet. Both the patients and investigators were aware of the procedures conducted. Patients with anxiety, psychiatric illness, vascular insufficiency, or peripheral vascular disease were excluded.
LA was prepared using two methods; WALANT consisted of 100 ml of 1% lignocaine, 1 ml of epinephrine (1:1000) and 10 ml of 8.4% sodium bicarbonate (total 111 ml); and LA consisted of 1% lignocaine. At the waiting room, LA was injected according to the randomized group using a 25G needle. The volume of anaesthesia needed depended on the surgery, as described in literatures. 6,7,9 In fact, we injected a total of 10 ml of lidocaine or lidocaine/epinephrine/sodium bicarbonate for carpal tunnel release and ganglion excision, whereas only 2 ml was injected for trigger release. These volumes were less than the recommended dosages. All injections were given at subcutaneous level until a tumescent effect was achieved. 4,7,10 None of the patients required extra injections.
Preoperative preparation time, defined as the duration between the injection and skin incision, was recorded. Post injection, they were brought into the operating theatre and prepared for surgery. Tourniquet was applied over the arm for LA/tourniquet group. Patients were continuously monitored during the procedure. The starting time (skin incision made) of the surgery and the end time surgery (completed last suture) were recorded. According to the number and amount of gauze soaked, the blood loss was estimated by the surgeon. Post surgery, they were required to fill a questionnaire. The perceived comfort during surgery was quantified using a visual analogue scale (VAS). All patients were reviewed in the clinic 2 weeks postoperatively to assess for any complications.
Continuous variables were described as mean ± standard deviation, while categorical variables were described as frequency and percentages. The difference in continuous data was measured using t-test statistics. Linear regression analysis was performed with VAS as outcome. Statistical analysis was performed using SPSS version 21. This study was approved by the University Malaya Medical Centre Ethics Committee (Ethics Approval Number: 201726-4896).
Results
The mean age of patients who participated was 63 years (SD 11.7, range 38–87). The study patients included 31 females and 9 males. Eight patients were diagnosed with carpal tunnel syndrome, 20 with trigger finger and two with ganglion (Table 1).
Demographic data of patients who participated in this study.

SD: standard deviation.
The mean VAS for the WALANT group was 2.33 ± 1.94, whereas it was 4.72 ± 3.05 for the LA/tourniquet group, and the difference was statistically significant (p < 0.05) (Table 2).
Patient and clinical characteristics between techniques of anaesthesia.
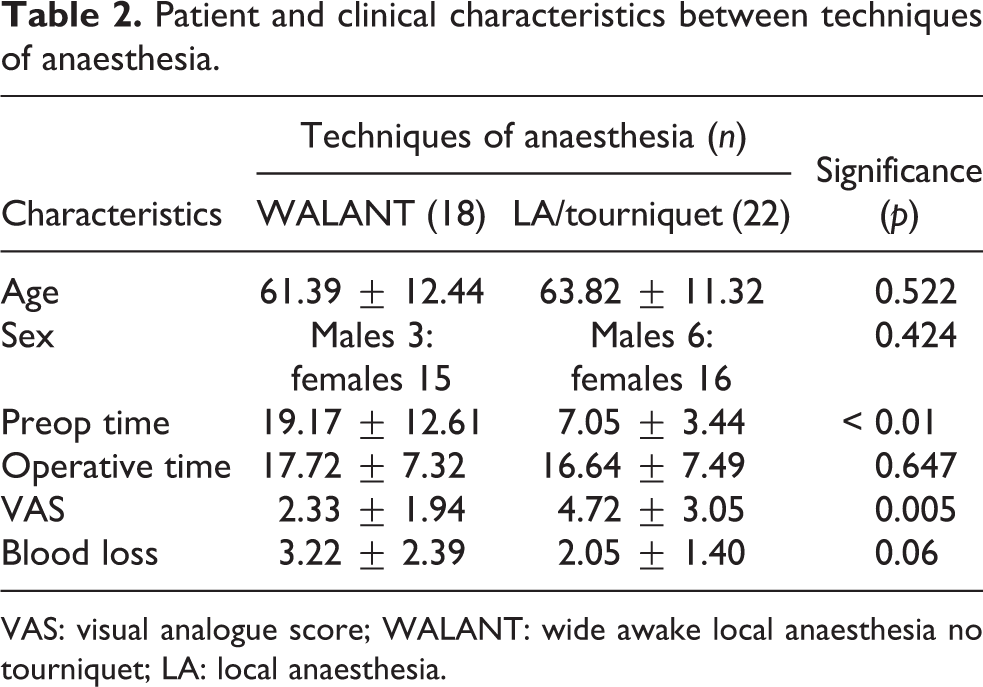
VAS: visual analogue score; WALANT: wide awake local anaesthesia no tourniquet; LA: local anaesthesia.
Based on Table 3, in the crude model, WALANT was associated with a lower VAS (B = −2.39, p = 0.007).
Association between techniques of anaesthesia and discomfort level (VAS).

CI: confidence interval; VAS: visual analogue score; WALANT: wide awake local anaesthesia no tourniquet; LA: local anaesthesia.
In the adjusted model (controlling for age, sex and type of surgery), WALANT was still associated with a lower VAS score (B = −2.06, p = 0.03). Therefore, WALANT procedure was associated with lower discomfort among study participants.
The mean time for preoperative preparation in WALANT group was 19.17 ± 12.61 min and in LA/tourniquet group was 7.05 ± 3.44 min. The difference between these groups was statistically significant (p < 0.01). The average time taken to perform the surgeries in both groups was similar, 17.72 ± 7.32 min under WALANT and 16.64 ± 7.49 min under LA/tourniquet (p > 0.05). The blood loss was not significant in WALANT surgeries (mean volume 3.22 ± 2.39 ml; p = 0.06) compared to the blood loss in LA/tourniquet surgeries (mean volume 2.05 ± 1.40 ml) (Table 2). No complications were encountered during the surgeries. One patient had a surgical site infection that resolved with oral antibiotics. There were no post-tourniquet complications.
Discussion
Carpal tunnel release and trigger finger release are minor surgeries done in procedure rooms under field sterility with very low infection rates. 6,10 In our centre, these surgeries are performed in the minor operation theatre. The average time taken to perform these surgeries was 17.18 min, independent of the type of anaesthesia used.
We investigated the overall perceived comfort of patients during surgery and quantified it using a VAS, with 10 being the least comfort and 0 being the most comfort level. We found a significant difference in perceived comfort level between WALANT and LA/tourniquet. WALANT patients were more comfortable intraoperatively. They claimed that they would recommend this procedure to others. Patients who were planned for another minor surgery at the contralateral site even requested for the surgery to be performed under WALANT. All of them blamed the tourniquet for their discomfort.
Generally, patients can tolerate tourniquet for about 20 min. 11 Arm tourniquets were less tolerable compared to forearm tourniquets; the maximum tolerance for forearm tourniquet was quantified as 13 min 2 and 25 min 3 in two independent studies. Beyond that, they have discomfort due to either direct compression of skin and soft tissues under tourniquet or forearm and hand muscles ischaemia. 11 By completely eliminating the usage of tourniquet, WALANT provides good comfort level during surgery.
The preoperative preparation was significantly more time-consuming in WALANT compared to LA/tourniquet. The surgery was deliberately delayed based on the recommendation to wait at least 26–30 min for the adrenaline to cause optimal vasoconstriction for haemostasis during surgery. 7,11 For a more practical setting, patients can be given WALANT earlier and were made to wait 30 min, while the operating theatre is prepared and consultation given. Therefore, the waiting time is well utilized.
Generally, WALANT is reported as safe, cost- and time-efficient compared to general anaesthesia 9 and sedation, 12 and enables the assessment of active movements intraoperatively. 11 Tendon repair or transfers, fracture fixation, arthrodesis and arthroplasty could be done under WALANT. 11 In a large series of WALANT surgeries, no ischaemic fingers were reported. 13,14 The only reported adverse effects were self-limiting fine tremor and vasovagal episodes that can be prevented with injection in supine position. 5 Lately, there were a few reported cases of finger ischaemia after epinephrine injection. 15,16 Zhang reported that a case of trigger release was done for three fingers under the same setting, wherein epinephrine was injected into the tendon sheath, resulting in the patient developing gangrenous fingertips that were eventually amputated. Zhu reported that a case of ipsilateral carpal tunnel release and trigger release of middle finger with WALANT resulted in prolonged ischaemia. 15 Phentolamine, an α-blocker rescue, was given 14 hours post surgery to reverse the vasoconstriction effect. Later, the patient was found to have cold intolerance. Thus, the WALANT technique must be avoided in patients with vascular insufficiency. Injection must strictly follow recommendations of dosages and technique. Surgeons must ensure that phentolamine is available prior to epinephrine injections.
This study was conducted prospectively. Patients were given the opportunity to state their experiences immediately. Previous literatures investigated patient satisfaction, pain and anxiety level, retrospectively, 7,17 which could be inaccurate as perception may change over time. Our limitation in this study was that a single surgeon was involved in the surgery done and in administering injections. Blood loss measurements were estimated by the respective surgeons, which could be inaccurate.
Conclusion
WALANT technique was associated with better comfort for patients. Tourniquet was the main reason for discomfort during surgeries. Thus, WALANT is an alternative in minor hand surgeries for a bloodless surgical field without the discomfort of tourniquet application, provided safety recommendations are addressed.
Footnotes
Acknowledments
We thank Dr Cassidy Devarajooh for his assistance in data and statistical analysis.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.