
Abstract
Background:
Recalcitrant auricular keloids are keloids that have recurred after any previous treatment. They have been shown to have an increased likelihood of recurrence. There is no consensus on how best to treat recalcitrant auricular keloids. Here, we perform the first systematic review and meta-analysis investigating the evidence for treating recalcitrant auricular keloids.
Methods:
We searched MEDLINE, EMBASE, CINAHL, and EBM Reviews using specific keywords. Prespecified inclusion and exclusion criteria were used to assess article eligibility. Data were extracted for number of recalcitrant keloids, treatment modality, recurrence, and minimum follow-up time. Included articles were stratified by treatment and assigned a level of evidence (LOE) based on the Oxford Centre for Evidence-Based Medicine guidelines. A meta-analysis was performed to estimate recurrence rates with 95% confidence intervals for each treatment modality.
Results:
A total of 887 unique articles were identified and 13 included. Eleven were LOE III and 2 were LOE IV. Recurrence rates were found to be 9% (95% CI: 3%-25%) for excision with adjuvant brachytherapy, 14% (95% CI: 12%-17%) for excision with adjuvant compression therapy, 17% (95% CI: 3%-56%) for excision with adjuvant external beam radiation, and 18% (95% CI: 4%-53%) for excision with adjuvant steroid injections. No statistical significant difference was found.
Conclusions:
Data for treatment of auricular keloids are heterogeneous with few high-quality studies. Excision with adjuvant brachytherapy has the lowest recurrence rate in our analysis. Narrow confidence intervals reported here for brachytherapy and compression therapy may help surgeons more confidently recommend either of these treatment modalities to patients.
Background
Keloids are benign neoplasms characterized by dysregulated deposition of connective tissue extending beyond the boundaries of the original wound. Auricular keloids are most commonly caused by ear piercings, 1 with an incidence close to 2.5%. 2,3 The reported treatment methods include surgical excision, 4,5 steroid injection, 6,7 radiotherapy, 8,9 compression therapy, 10 cryotherapy, 11 imiquimod, 12 or a combination of the above. 13,14 The recurrence rate after surgery alone is frequently reported in the literature as 45% to 100%. 1,15 -17 A recent systematic review suggests triamcinolone or radiation treatment following surgical excision to be equally effective for treatment of auricular keloids. 18
To the authors, “recalcitrant keloid” represents those keloids that recur after any previous treatment. Recalcitrant keloids pose an even greater challenge to the plastic surgeon. Previous treatment history, as opposed to no previous treatment history, in the setting of excision with adjuvant compression therapy has been shown to increase the likelihood of keloid recurrence at an odds ratio of 6.93. 10 Similarly, an increased risk of recurrence for recalcitrant keloids has also been shown in the setting of excision with adjuvant radiotherapy. 19 When compared to primary auricular keloids, recalcitrant auricular keloids have different growth rates 7,10 and require a greater number of adjuvant steroid injections following excision to achieve treatment success. 7 Despite more aggressive steroid administration, the recurrence rate for treatment with excision and adjuvant steroid injection is as high as 40%. 7 Treatment with adjuvant radiotherapy following surgical excision is another common practice; 20 however, the efficacy is unclear as treatment with excision plus adjuvant external beam radiation has yielded recurrence rates of 0% 21 to 59%. 22 Evidently, there is no consensus on how best to treat recalcitrant auricular keloids. We have performed the first systematic review and meta-analysis evaluating the treatment of recalcitrant auricular keloids. Our primary goal is to determine which of the following treatments yield the lowest recurrence rate with a minimum follow-up of 1 year: excision plus brachytherapy, excision plus compression therapy, excision plus external beam radiation or excision plus steroid injection.
Methods
Literature Search
Research of the literature for this review article was implemented according to the protocol presented in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses. 23 Our search strategies were developed in consultation with a health sciences librarian. We performed an updated literature search on March 9, 2018, using Ovid MEDLINE (1946 to present), Ovid EMBASE (1974 to present), CINAHL (1937 to present), and Ovid EBM Reviews (1991 to present). Review articles were searched for further relevant studies. Keywords used in our search included the following: ear*, keloid*, treat*, therap*, manag*, surg*, excis*, triamcinolone, steroid*, corticosteroid*, cryosurg*, cryotherap*, fluorouracil, 5- FU, Interferon, IFN, laser*, silicon*, Silicon Gel Sheeting, radiation*, radiotherap*, and compression. We did not restrict the publication type in our search methods in an attempt to include gray literature. An example of our full electronic search strategy can be found in the Supplemental Material.
Eligibility Criteria
Reports were selected using the following inclusion criteria: (1) any excision plus adjuvant treatment modality for recalcitrant keloids with recurrence as the outcome variable, (2) a description or statement identifying the lesion as a keloid, (3) minimum follow-up of 1 year. The following exclusion criteria were used to eliminate articles: (1) single case reports, (2) letters, (3) animal or in vitro studies, (4) prophylactic treatment, (5) insufficient data to determine recurrence for recalcitrant keloids, (6) no auricular keloids, (7) papers that stated both hypertrophic scars and keloids, but did not differentiate between them, (8) not in the English language, and (9) repeated data sets.
Study Selection
Two nonblinded independent reviewers (L.Z. and B.R.) applied prespecified inclusion and exclusion criteria to identify eligible studies. Articles were screened using titles and abstracts, followed by review of the full text for studies where the abstract did not contain sufficient information to determine eligibility. Disagreements on article eligibility were resolved via discussion between the 2 reviewers and if unresolved in this way, a third author (A.V.S.) would decide. We wrote a script in R (a statistical programming language) 24 to remove duplicate articles. The search results of each database are exported as text files. The script takes the text files as an input and identifies duplicate articles by giving each article a unique identifier using the concatenation of the first 4 letters of the author’s name, the article’s title, and the publication year. The results are then printed to an excel file containing a list of only the unique articles. We manually found and removed duplicates not found with the R script due to author and title spelling differences across databases. If the full text could not be found, we contacted the author to retrieve the article. We excluded articles from unresponsive authors and articles in non-English languages. We grouped by treatment modality and excluded any treatment modality with only one supporting article or less than 20 recalcitrant auricular keloids.
Studies with follow-up time for each patient, but a minimum study follow-up time less than 1 year were assessed to see if any patient had follow-up time of more than 1 year. Patients with adequate follow-up time were then included, while those from the same study with inadequate or unreported follow-up time were excluded. We excluded papers if less than 2 recalcitrant auricular keloids could be extracted. Many articles that included both recalcitrant and primary keloids did not specify recurrence for the recalcitrant keloids. In this case, we contacted for clarification and excluded articles from unavailable authors.
Data Extraction
Two independent reviewers extracted data from included articles. Disagreements were resolved via discussion between the 2 reviewers. Data were collected on the number of recalcitrant keloids, treatment modality, recalcitrant keloid recurrence, prior treatment history, follow-up time, and number of patients. The articles were assigned a level of evidence (LOE) adapted from the Oxford Centre for Evidence-based Medicine guidelines (Table 1). 25 A risk of bias assessment was performed using the MINORS tool (Supplemental Material). Where number of patients and not the number of keloids was presented, it was assumed that each patient had a single keloid. Number of auricular keloids that had received any prior treatment from each study was extracted for analysis. We used recurrence rate as the outcome measure in our study.
Levels of Evidence (Adapted from Oxford Centre for Evidence-Based Medicine Guidelines).
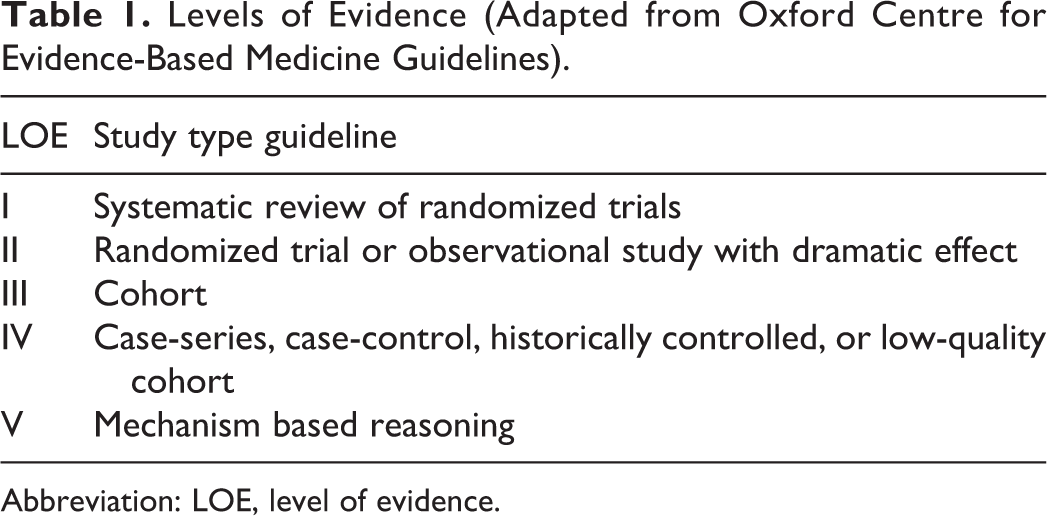
Abbreviation: LOE, level of evidence.
Statistical Analysis
We consulted a statistician to analyze our data with the most appropriate statistical methods. R statistical software 24 was used to conduct the meta-analysis to determine an estimated overall recurrence rate for each treatment modality. For each treatment modality, forest plots were generated to visualize the individual and estimated overall recurrence rates. For each rate, 95% confidence intervals were calculated using a generalized linear mixed effects model via the metafor package. 26 To assess the percentage of total variation across studies due to heterogeneity we used the I 2 statistic. To test for possible differences between treatments, a generalized meta-analytic mixed effects model was fit to all the data, with treatment as a moderating variable. A P value of less than .05 was determined to be significant.
Results
Study Selection
Figure 1 shows the study selection process. In all, 1214 articles were retrieved from our database searches. The removal of duplicates yielded 887 unique articles. Screening of titles and abstracts excluded 600 articles. The full text of the remaining 287 articles was evaluated using the inclusion and exclusion criteria. A further 274 articles were excluded. Of these, 168 had insufficient data. Two articles were not found and were excluded. Five articles were found to be a repeated data set. Sixteen review articles, 23 case reports, and 28 letters were excluded. A further 32 articles were excluded because of treatment modality as described above in the study selection methods. A total of 13 articles were included in the final analysis, grouped into 4 treatment modalities for comparison.
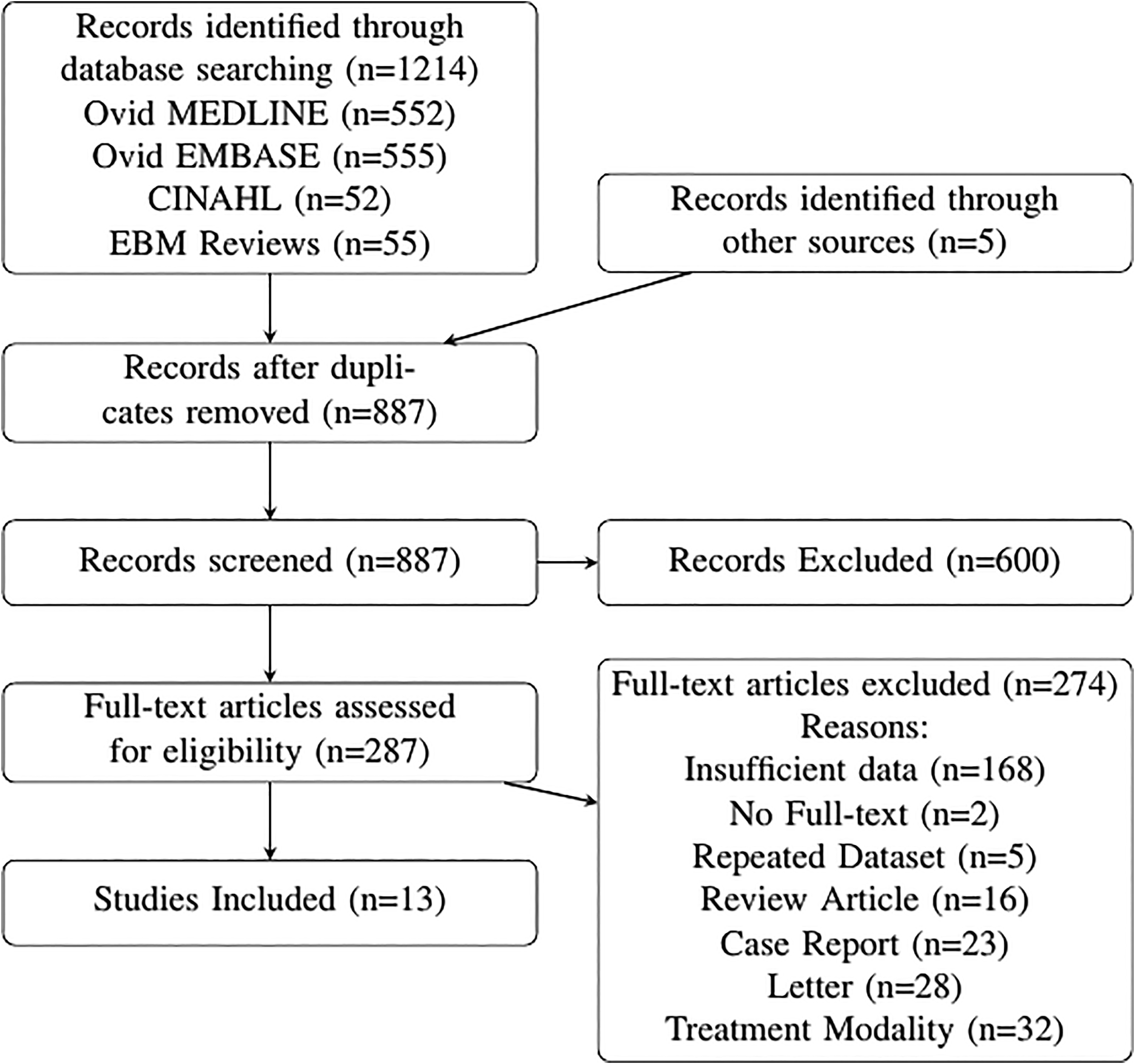
Flow diagram of study selection.
Study Characteristics
The extracted data for the 13 studies included in the analysis is listed in Table 2. Eleven studies were graded LOE III, and 2 studies were evaluated to be LOE IV (Table 2). A total of 795 recalcitrant auricular keloids were identified across all included studies. Four treatment options met our inclusion criteria: (1) surgical excision and compression, (2) surgical excision and external beam radiation, (3) surgical excision and brachytherapy, and (4) surgical excision and steroid injections. All included studies had at least 1 year of follow-up. The data for each treatment modality are listed in Table 3. Our risk of bias assessment demonstrated a potential risk of bias for individual studies and a potential for bias across studies. We found variable reporting of pre-specified inclusion criteria and recurrence definition. There was blind evaluation of recurrence in only one study (Supplemental Material).
Outcome Data Extracted From Included Studies.
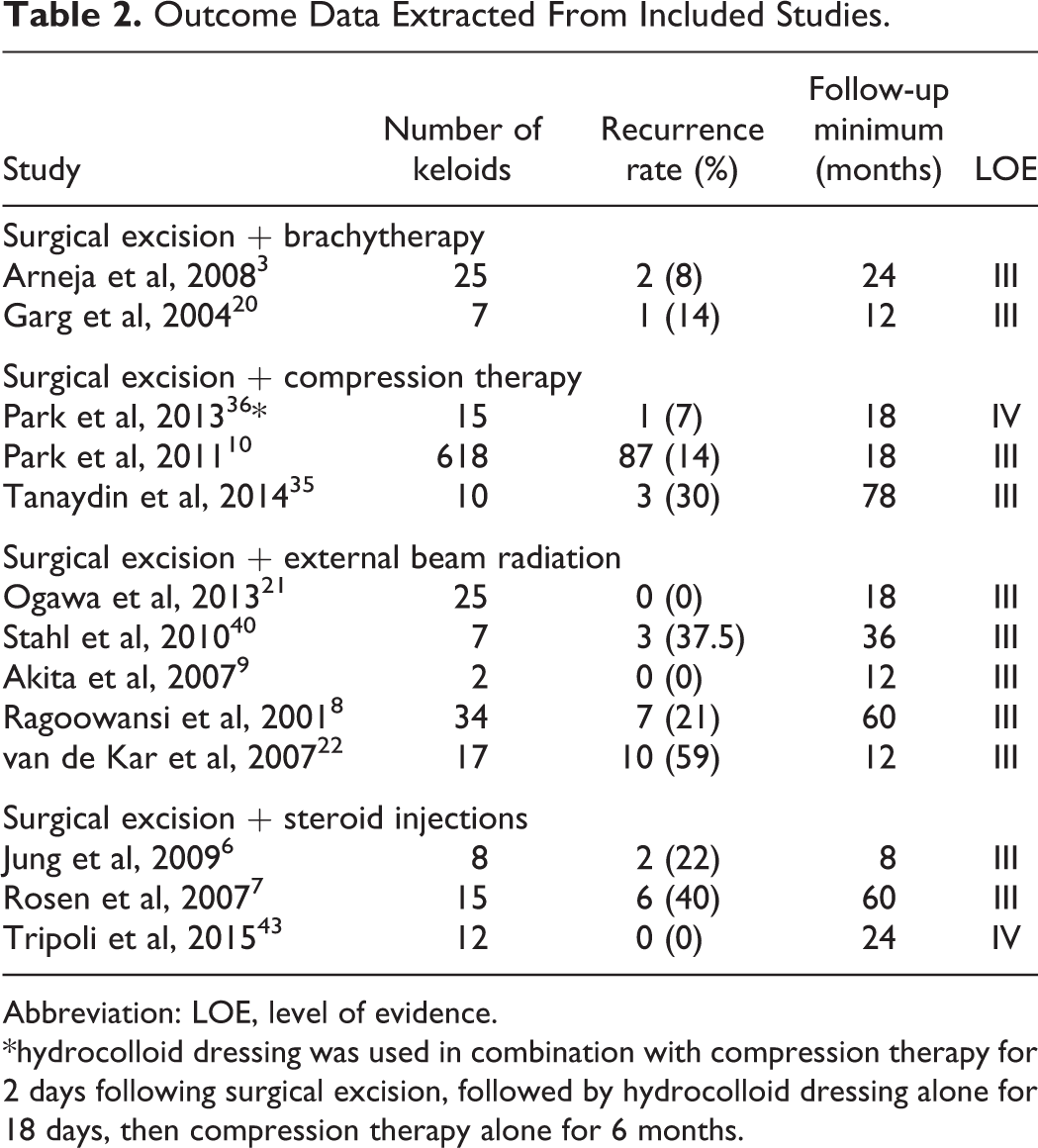
Abbreviation: LOE, level of evidence.
*hydrocolloid dressing was used in combination with compression therapy for 2 days following surgical excision, followed by hydrocolloid dressing alone for 18 days, then compression therapy alone for 6 months.
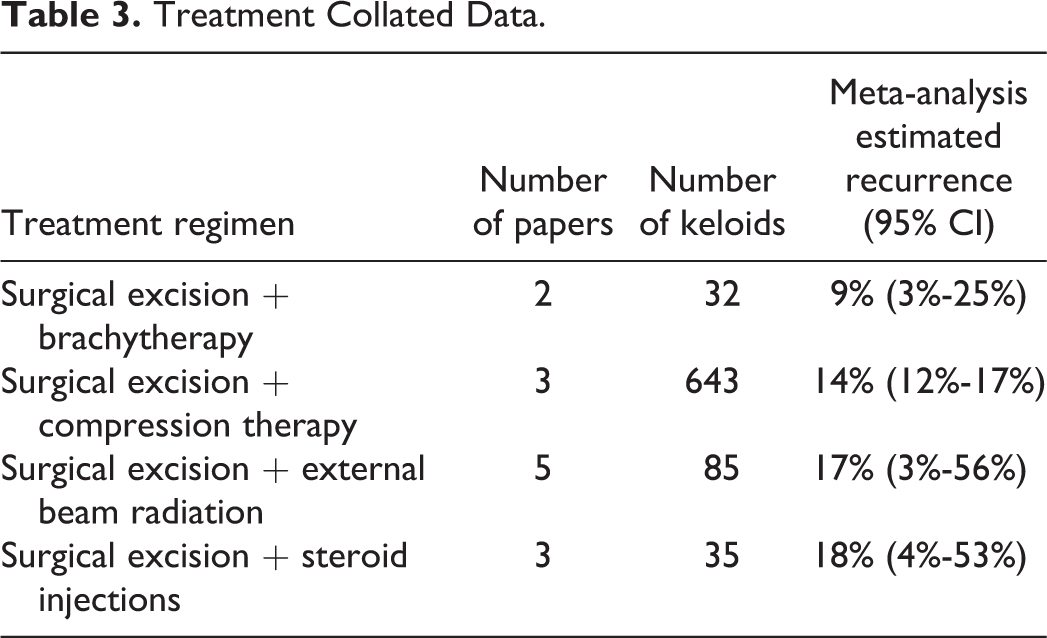
Treatment Collated Data.
Efficacy of Treatment Modalities
The efficacy of each treatment modality for treatment of recalcitrant auricular keloids was appraised using recurrence rates (Table 3). The recurrence rate for excision plus adjuvant brachytherapy was estimated as 9% (95% CI: 3%-25%), I 2 = 0%. The recurrence rate for excision with adjuvant compression therapy was estimated as 14% (95% CI: 12%-17%), I 2 = 0%. The recurrence rate for excision plus adjuvant external beam radiation was estimated as 17% (95% CI: 3%-56%), I 2 = 84%. The recurrence rate for excision plus adjuvant steroid treatment was estimated as 18% (95% CI: 4%-53%), I 2 = 60%. Figure 2 illustrates the meta-analysis results for each treatment modality. There was no overall difference in treatments (P = .79, Omnibus test applied to treatment as a moderating variable).
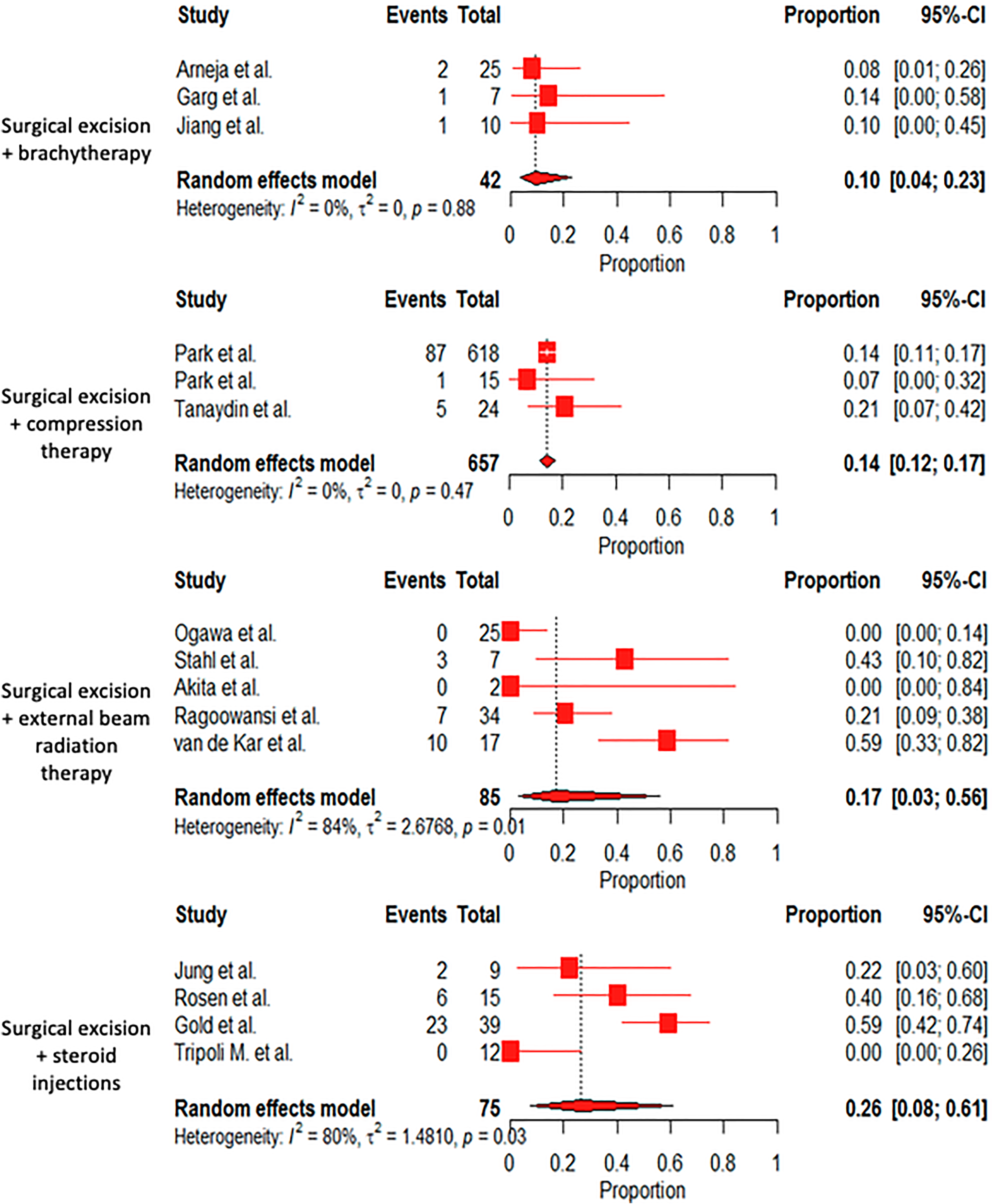
Forest plots showing the estimated recurrence rates for each treatment modality. The diamond in each forest plot represents the overall estimated recurrence rate of pooled studies in each treatment modality.
To assess the effect of follow-up time on our results, we ran a separate analysis using a 6-month follow-up minimum cutoff. We re-evaluated all studies that were excluded for a follow-up time of less than 1 year. Of these, if a study had a follow-up time of at least 6 months and satisfied all other inclusion and exclusion criteria it was included in our 6-month follow-up analysis. This provided 2 additional studies for inclusion 27,28 for a total of 15 studies and 859 recalcitrant auricular keloids. The recurrence rate for excision plus adjuvant brachytherapy was estimated to be similar at 10% (95% CI: 4%-23%). The recurrence rate for excision with adjuvant compression therapy was nearly identical to the group with the 1-year follow-up, estimated at 14% (95% CI: 12%-17%). The recurrence rate for excision plus adjuvant external beam radiation did not change and was estimated as 17% (95% CI: 3%-56%). The estimated recurrence rate for excision plus adjuvant steroid treatment increased to 26% (95% CI: 8%-61%). However, similar to comparing the treatment modalities using the 1-year follow-up, there was no overall difference in treatment efficacy (P = .40, Omnibus test applied to treatment as a moderating variable).
Discussion
Recalcitrant auricular keloids are difficult to treat, and there is currently no evidence reliably suggesting the best treatment. High-quality literature on auricular keloids is sparse, and only one systematic review with meta-analysis exists that compares surgical excision with adjuvant triamcinolone injections to surgical excision with adjuvant radiotherapy. 18 Shin and colleagues found both modalities to be equally effective with recurrence rates of 15.4% (95% CI: 9.4%-24.1%) and 14% (95% CI: 9.6%-19.9%), respectively. 18 However, the authors did not differentiate between primary and recalcitrant keloids, and evidence shows that the latter have higher recurrence rates. 10,19 Further, Shin and colleagues do not differentiate between external beam radiation or brachytherapy. In contrast, our systematic review and meta-analysis investigated only recalcitrant auricular keloids and to our knowledge is the first to evaluate treatment for this difficult population of auricular keloids.
Excision With Brachytherapy
Recalcitrant auricular keloids treated with excision and adjuvant brachytherapy had a recurrence rate of 9% (95% CI: 3%-25%): the lowest recurrence rate of all modalities compared in our meta-analysis. Combined recurrence rates for the treatment of both primary and recalcitrant auricular keloids are thought to be close to 12%. 29,30 Reviews looking at treatment of primary and secondary keloids in multiple anatomical locations found rates of 10.5% and 15%. 31,32 Our results are consistent with these previous findings.
Brachytherapy involves placing radioactive material inside or next to the desired region of interest. This is achieved first with implantation of a hollow catheter at the site of the excised keloid tumor, and then the patient is subsequently sent to the radiation oncology department for brachytherapy delivery through the catheter. 3 A treatment planning system is used to provide uniform high dose distribution and minimal dose to surrounding tissues. 27 In our analysis, we include two studies that use Ir-192 high-dose rate brachytherapy for treatment of recalcitrant auricular keloids with a dosing regimen of 15 Gy in 3 fractions. 3,20 One fraction of 5 Gy is given following keloid excision on the same day, followed by 5 Gy on postoperative days 1 and 2. After completion of three treatments, the catheter is removed. 3
Brachytherapy may be preferable to external beam radiation, given the lower dose of radiation needed to achieve similar effect and decreased toxicity to adjacent tissues. 3 In addition, our narrow confidence interval may help clinicians recommend brachytherapy to patients over external beam radiation or intralesional steroid injections as the recurrence rates for these last 2 treatment modalities are more variable (Table 3).
Excision With Compression Therapy
We calculated an estimated recurrence rate of 14% (95% CI: 12%-17%) for recalcitrant auricular keloids treated with excision and adjuvant compression therapy. Reported recurrence rates range from 0% to 30% for auricular keloids not specific to the recalcitrant population 33,34 although few high-quality studies exist.
We found that compression therapy varied in device type and treatment duration. Most studies recommended the patient to wear the device for at least 12 h/d, with a duration of therapy ranging from 4 to 15 months. 10,34 -36 Pressures in the range of 24 to 30 mm Hg are recommended to achieve the necessary hypoxic effect while avoiding ischemic complications 37 such as ulceration and necrosis, 33,35 which can also be mitigated with the design of the splint. 35,38 Only 2 studies report the amount of pressure exerted by the compression device. 10,36 Another complicating factor of compression therapy is patient non-compliance 10,39 due to discomfort and aesthetics of the device. 35 Park and colleagues attempted to address device aesthetics using magnets, 36 but this device does not allow for pressure adjustment. 35 Similar to brachytherapy, we are more confident in recommending compression therapy as a treatment modality for recalcitrant auricular keloids compared to external beam radiation or intralesional steroid injection which were found to have significantly wider confidence intervals (Table 3).
Excision With External Beam Radiation Therapy
We found a recurrence rate of 17% (95% CI: 3%-56%) for recalcitrant auricular keloids treated with adjuvant external beam radiation. A recent systematic review found a recurrence rate of 14% (95% CI: 9.6%-19.9%) for the combined treatment of primary and recalcitrant auricular keloids; however, this was not specific to external beam radiation. 18 This suggests that recalcitrant auricular keloids may have similar recurrence rates when treated with adjuvant external beam radiation when compared to primary auricular keloids, although the uncertainty around our estimate is large.
In our study, treatment regimens varied between included studies with the radiation dose ranging from 10 to 30 Gy. 8,9,21,40 In one study, radiation was performed pre- and post-surgery. 40 In all other studies, radiation began within 8,22 or after 24 hours post-surgery. 21 One study found that this timing difference may have negligible effects on keloid recurrence. 19 Radiation therapy has been noted to cause hyperpigmentation and telangiectasia, 41 and exposure to radiation also has the potential to increase the risk of cancer; however, a systematic review of 6656 keloids treated with adjuvant radiotherapy found only 5 cases of possible radiation induced cancers. 42 Nevertheless, more research is needed to determine whether external beam radiation therapy is a safe and effective treatment modality for recalcitrant auricular keloids.
Excision With Intralesional Steroid Injection
Our analysis found a recurrence rate of 18% (95% CI: 4%-53%) for recalcitrant auricular keloids. A recent systematic review found a recurrence rate of 15.4% (95% CI: 9.4%-24.1%) for the combined treatment of primary and recalcitrant auricular keloids, 18 suggesting that steroid injections may be equally effective for treating primary or recalcitrant auricular keloids. Recurrence rates of 3% to 60% have been reported for treatment of keloids, whether primary or secondary, with surgical excision and adjuvant steroid injections. 1 This is consistent with the results from our study.
In our review, the dose of triamcinolone acetonide ranged from 20 to 40 mg/mL, and injections were given pre-operatively and postoperatively, 6 intraoperatively, 7,43 postoperatively in 1-month intervals, 6,7 or as 1 postoperative injection. 43 The different treatment regimens make direct comparisons of recurrence among studies difficult. Adverse effects associated with steroid injections have been found in up to 63% of patients 1,44 and should be weighed, along with the variable recurrence rates, against the benefits of administering steroid injections.
Other Treatments
We identified 16 other treatment regimens for recalcitrant auricular keloids including (1) surgical excision and imiquimod; 12,45 (2) radiofrequency ablation; 46,47 (3) surgical excision, mitomycin C, and steroids; 48 (5) surgical excision, steroid injections, radiation, and compression; 13 (6) cryosurgery; 49 (7) laser and steroids; 50,51 (8) surgical excision and CO2 laser; 52 (9) surgical excision and mitomycin C; 53 (10) collagenase injections and compression; 54 (11) ksharsutra and agnikarma; 55 (12) verapamil and compression; 56 (13) surgical excision + verapamil; 57 (14) surgical excision and platelet-rich plasma; (15) surgical excision, steroid injections, and compression; 14 and (16) surgical excision, compression, and steroid tape. 58 Although some of these treatments show promising results, there is limited data and we did not include them in our analysis.
Follow-Up Interval
While keloids have been reported to recur more than 2 years later, 19 many studies have found that the majority of recurrence is within the first year after treatment; accordingly, it is generally well accepted to have a minimum follow-up of at least 1 year. 59 In our analysis, we did not find a significant difference between treatment modalities using a 6-month (P = .40) or 1-year follow-up period (P = .71). This may provide justification for the use of a 6-month follow-up period; however, future studies would be needed to confirm these findings.
Limitations
The primary limitation of this study was the lack of high-quality studies available. The LOE of our included studies was III or IV, and the overall number of studies for each treatment was low. This is consistent with a literature review that found the majority of evidence for keloid treatments to be based on LOE IV studies. 60 Many studies on the treatment of keloids have small numbers of patients, 10,59 leading to high uncertainty around the estimated recurrence rates. We found a potential for risk of bias in our included studies, all of which, were nonrandomized observational studies. Despite the potential risk of bias, there is a great need to synthesize the heterogenous literature available as there is no consensus on the best treatment for recalcitrant auricular keloids. Our review clearly demonstrates the need for better study design.
There is large heterogeneity across studies, which makes strong interpretations of the data challenging; however, we attempted to mitigate this with rigorous inclusion/exclusion criteria. Relevant clinical predictors including keloid size, histopathological confirmation, keloid age, keloid growth rate, family history of hypertrophic scars/keloids, and ethnicity are inconsistently reported between studies, making it impossible to control for these variables when comparing treatment modalities. 15 Recurrence is variably defined and sometimes not defined at all. Keloids can present with pruritus or pain, 44 and therefore, recurrence can be assessed as return of symptoms or the amount of regrowth. The dosage, frequency, and timing vary between studies within each treatment modality. Anatomical location was heterogeneously reported across studies, and we were unable to differentiate earlobe and non-earlobe keloids. Evidence has shown that there may not be a difference in recurrence rates between earlobe and helical auricular keloids; 10 however, this is not specific to recalcitrant auricular keloids.
We were not able to control for the type of prior treatment for the included recalcitrant keloids. These data were either not reported or reported without quantification of which keloids had which primary treatment. Therefore, we had insufficient data to further analyze the effect of primary treatment on secondary treatment of the included recalcitrant auricular keloids. We attempted to reduce data loss by contacting authors in cases with incomplete manuscripts. We limited our study to papers in English and excluded unobtainable papers, which may bias our results. Where number of patients and not the number of keloids was reported, we assumed that each patient had a single keloid. Resultantly, we may have underestimated our sample size for five included studies as patients may have had more than one keloid. 3,10,28,34,36,40,43
Conclusions
The data for the treatment of recalcitrant auricular keloids are heterogeneous and include few high-quality studies. This is reflected in our analyses as we found large variability in our meta-analyses accentuated by smaller study sizes combined with few studies in each treatment modality. After rigorous application of inclusion/exclusion criteria, our analysis demonstrates that surgical excision with adjuvant brachytherapy has the lowest recurrence rate when compared with adjuvant compression therapy, radiotherapy, and steroid injections. In the literature, adjuvant brachytherapy has low recurrence rates for treatment of keloids. Although we did not achieve statistical significance, there may be an important clinical difference between treatment modalities that may be revealed as research in this field expands and the number of recalcitrant auricular keloids being treated in the literature increases. The narrow confidence intervals reported here for brachytherapy and compression therapy may help surgeons more confidently recommend either of these treatment modalities to patients, as opposed to external beam radiation or intralesional steroid injection which carry greater variability in their reported recurrence rates (Table 3). While difficult to make any direct comparisons, our results suggest that treatment with surgical excision and adjuvant steroid injection or adjuvant external beam radiation may result in higher recurrence rates for recalcitrant auricular keloids when compared to primary auricular keloids. This review and meta-analysis should draw attention to the need for further investigation using high-quality studies, preferably randomized controlled trials and prospective cohort studies with adequate controls.
Supplemental Material
Supplemental Material, sj-docx-1-psg-10.1177_2292550321995746 - What Do We Know About Treating Recalcitrant Auricular Keloids? A Systematic Review and Meta-Analysis
Supplemental Material, sj-docx-1-psg-10.1177_2292550321995746 for What Do We Know About Treating Recalcitrant Auricular Keloids? A Systematic Review and Meta-Analysis by Luke R. R. Zawadiuk, Aaron C. Van Slyke, Jeffrey Bone, Baillie Redfern, Nicholas J. Carr and Jugpal S. Arneja in Plastic Surgery
Footnotes
Acknowledgments
The authors acknowledge Maia A. Smith for her contribution to the R code automating initial duplicate detection of results from our database searches and Anthony-Alexander Christidis from the Applied Statistics and Data Science Group through the UBC Department of Statistics. We also acknowledge Dean Guistini from the UBC Biomedical Branch Library for his expertise in the development of our search strategies.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.