
Abstract
Introduction
The COVID-19 pandemic has caused a significant impact on the delivery of healthcare services, 1 including consultation and operative volumes. 2 The impact is also seen in surgical wait times, 2 residency applications, 3 clinical training and trainees’ operative exposure.4,5 The healthcare system will face significant challenges to overcome the consultation and surgical backlog. 6
The delivery of Plastic and Reconstructive Surgery (PRS) services has also been particularly impacted by the decrease in surgical volumes and prioritizing emergency care. 7 While some of the implemented changes can continue during the pandemic, 8 strategies to address the growing backlog for the long-term will require a better understanding of the exact impact of COVID-19 on PRS services.
A systematic review showed a reduction in elective orthopedic surgery by 69% to 93%. 1 The meta-analysis quantified the reduction in elective surgeries by 80%, with a 63% reduction in outpatient visits. 1 The exact impact on the surgical volumes and wait times in PRS is still unknown. 9 There is a growing need for population-level data to plan relief strategies. Information about the volumes and wait times are essential to assist healthcare policymakers in planning resources for the increasing backlog.
The study aimed to assess the impact of COVID-19 on the surgical volume and wait times for PRS in Ontario, Canada.
Methods
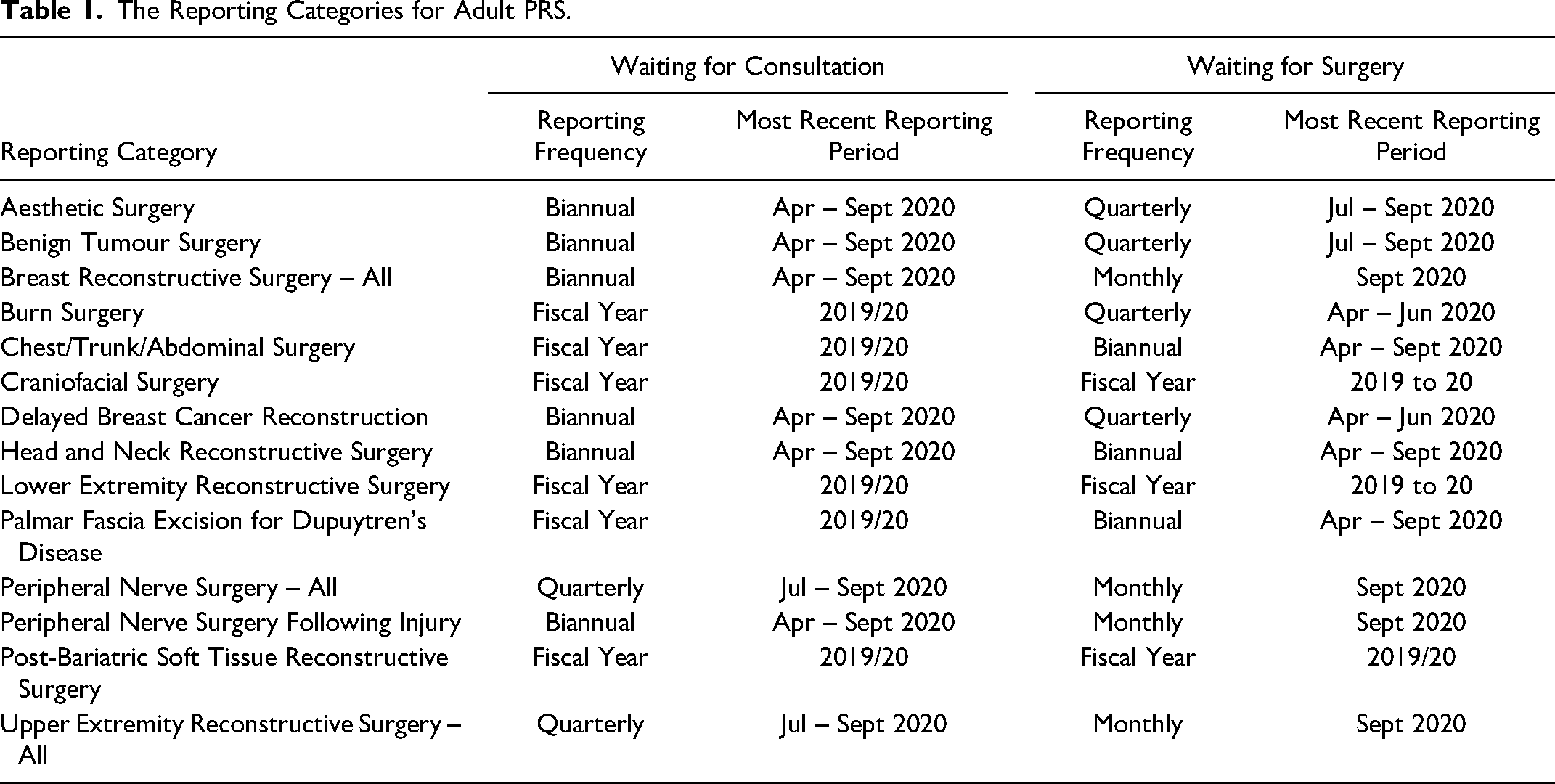
Wait time data were accessed using the publicly available information from Ontario Health (Access to Care). 10 Surgical wait times are reported across the province for several surgical specialities, including Adult PRS. There are 14 reporting categories for Adult PRS, including craniofacial surgery, breast, upper extremity surgery and other reconstructive surgeries. For peripheral nerve surgery, there are two reporting categories; traumatic peripheral nerve injury and other peripheral nerve surgeries. 11 Two wait times are reported; wait times for consultation and for surgery. Wait time for consultation is measured from receiving a referral by a specialist to the time of consultation. Wait time for surgery is measured from the operative decision to the date of the surgery. The province sets target wait times according to the priority assigned by the referring physician or the surgeon for the consult and the surgical wait times, respectively. Emergency cases, ie, priority one, are not captured in the database. Priority 1 is defined as emergency cases that need to be completed immediately. Priority 2 refers to severe cases or symptoms that are likely to worsen. Priority 3 refers to cases with symptoms that do not have a large impact on the quality of life. Priority 4 are cases where medical management might be failing. 12 For consultations, the target wait times are 30 days, 90 days and 182 days for priorities two, three and four, respectively. For surgical wait times, the target is set at 28 days, 84 days and 182 days for priorities two, three and four, respectively. The province reports the volume, average wait times and percentage of cases meeting the provincial target. The reporting frequency ranges from monthly to annual reporting based on the surgical volume. In this study, we used all the reporting data except for the annual reports, as the impact of COVID-19 was not yet demonstrated when the article was prepared. Thus, we were able to investigate 8 and 11 out of the 14 reporting categories for consult wait time and surgical wait times, respectively. Table 1 summarizes the reporting categories and the frequency of reporting on each category within Adult PRS. The aesthetic surgery category only included cases performed in publicly funded operating rooms, and it excluded cases performed in private facilities.
The Reporting Categories for Adult PRS.
The Province of Ontario issued a directive in March 2020 where all elective surgeries were paused during the peak of the COVID-19 pandemic. In May 2020, the directive was amended, and elective surgeries were resumed. 13 However, each hospital had a different approach in resuming elective surgeries based on their capacity.
We selected two periods to compare the impact of COVID-19 on each reporting category, the most recent available data and the baseline data from the previous year. The exposure period was defined as the period following the pandemic shutdown starting from April first, 2020. The baseline period included the same calendar months of the previous year to account for potential confounders, such as summer scheduling and seasonal variations that can potentially impact the delivery of healthcare services. The baseline period appeared stable graphically in the surgical volume and wait times. A six-month-period was used for all the reporting categories except for monthly-reported categories due to missing data from April to June 2019. Thus, all the other categories were measured from April to September 2020 in the exposure period, and the monthly-reported categories were measured from July to September 2020, which only included operative wait times for breast reconstruction, hand and peripheral nerve surgeries.
Similarly, we reviewed the paediatric surgery reporting categories, and we identified a single category for all Paediatric PRS. We selected the study period from April to September 2020 and compared it to the previous year. Currently, there are no reporting categories for Paediatric PRS. For this reason, we only described the changes, and we did not include the paediatric data in the pooled analysis. As we used publicly available information, the study was exempt from an ethical review.
Statistical Analysis
For each category, we reported the volume of cases and the percentage of cases meeting the provincial target. Then, we calculated the percentage change to the baseline period for each outcome measure. After stratifying the results according to the assigned priority, we reported the average wait time and the percentage change from baseline. We calculated the percentage change prior to rounding to increase the reporting accuracy. Differences in the total volume and the summed volumes per priority are attributed to cases with unassigned priority between 2 to 4. Small cells (ie, less than 5 cases), were hidden as per the Ministry of Health and Long-Term Care (MOHLTC) privacy policy. 14 When the reporting period was more frequent than 6 months, we summed the volume of cases and averaged the wait times to represent consistent study periods and allow comparisons. We used a similar approach for the three-month study periods based on the data availability. We performed a two-sided paired t-test on the before and after changes in the consults or operative volumes and the average wait times for each priority. The normality assumption was verified using the Shapiro-Wilk test. When the normality assumption was not met, we used the nonparametric equivalent, Wilcoxon signed-rank test. We reported data on the Paediatric PRS category, but we did not include it in the analysis. We compared the proportion of cases meeting the provincial target between the two study periods using a chi-squared test with continuity correction. We used an alpha value of 0.05 as the statistical significance threshold. We plotted the values against time without statistical modelling. Missing values were not included in the plots due to small cells. We performed all the analyses on aggregate data using R 4.0.1 GUI 1.72 statistical software.
Results
There was a total of 15,000 cases performed during the study period across 11 out of the 14 reporting categories in Ontario, 9563 cases in the baseline period and 5437 cases during the study period. The highest volume of cases was performed in the upper extremity reconstruction category (n = 3022), followed by the aesthetic surgery category (n = 2914). The volume of surgical consults in the available 8 categories was 9990 consults, 6665 in the baseline period and 3325 in the study period. The highest volume of consults was in the upper extremity reconstruction category (n = 3407) and the breast reconstruction category (n = 1970).
Wait Times for Consultation
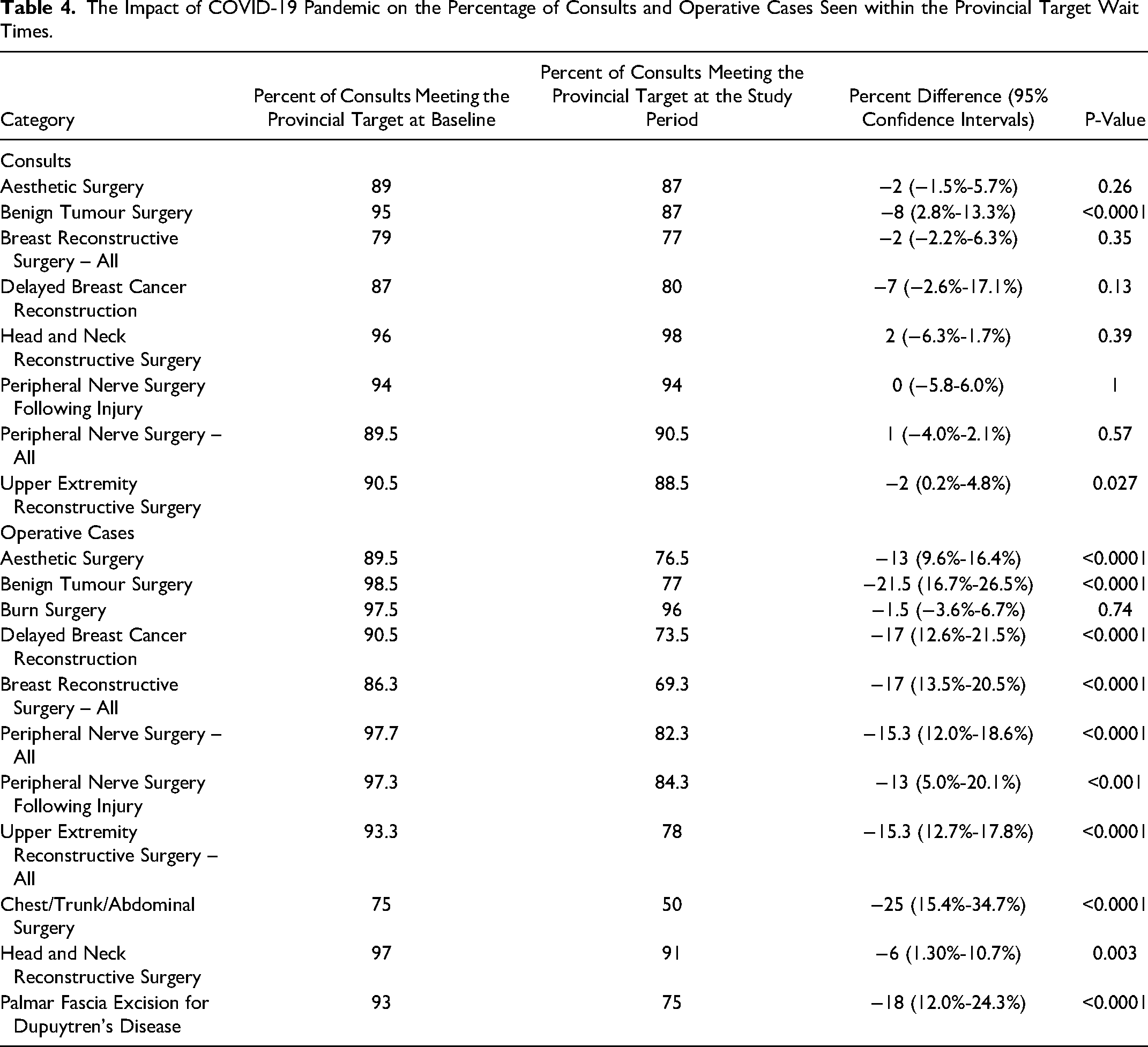
Overall, there was a 50% reduction in the volume of consults during the study period compared to the baseline period (p-value = 0.004). The reduction ranged from 46% to 75% after stratifying the results according to each category. The percentage of consults meeting the provincial target decreased by 2% (p-value = 0.009). The mean wait times were analyzed according to the surgical priority at the aggregate level. Overall, there was an increase in consult wait times by a mean of 7 days (p-value = 0.03). After stratifying the data by priority, there was no statistically significant difference between the mean consultation wait times for priorities 2, 3 and 4 at the aggregate level (p-values = 0.13, 0.84 and 0.07, respectively). Tables 2 and 3 summarize the differences between the baseline period and the study period in different reporting categories. Table 4 details the percent changes in consults seen within the provincial target wait times for each category. Figure 1 illustrates the changes in consults volume before and after the onset of the pandemic.
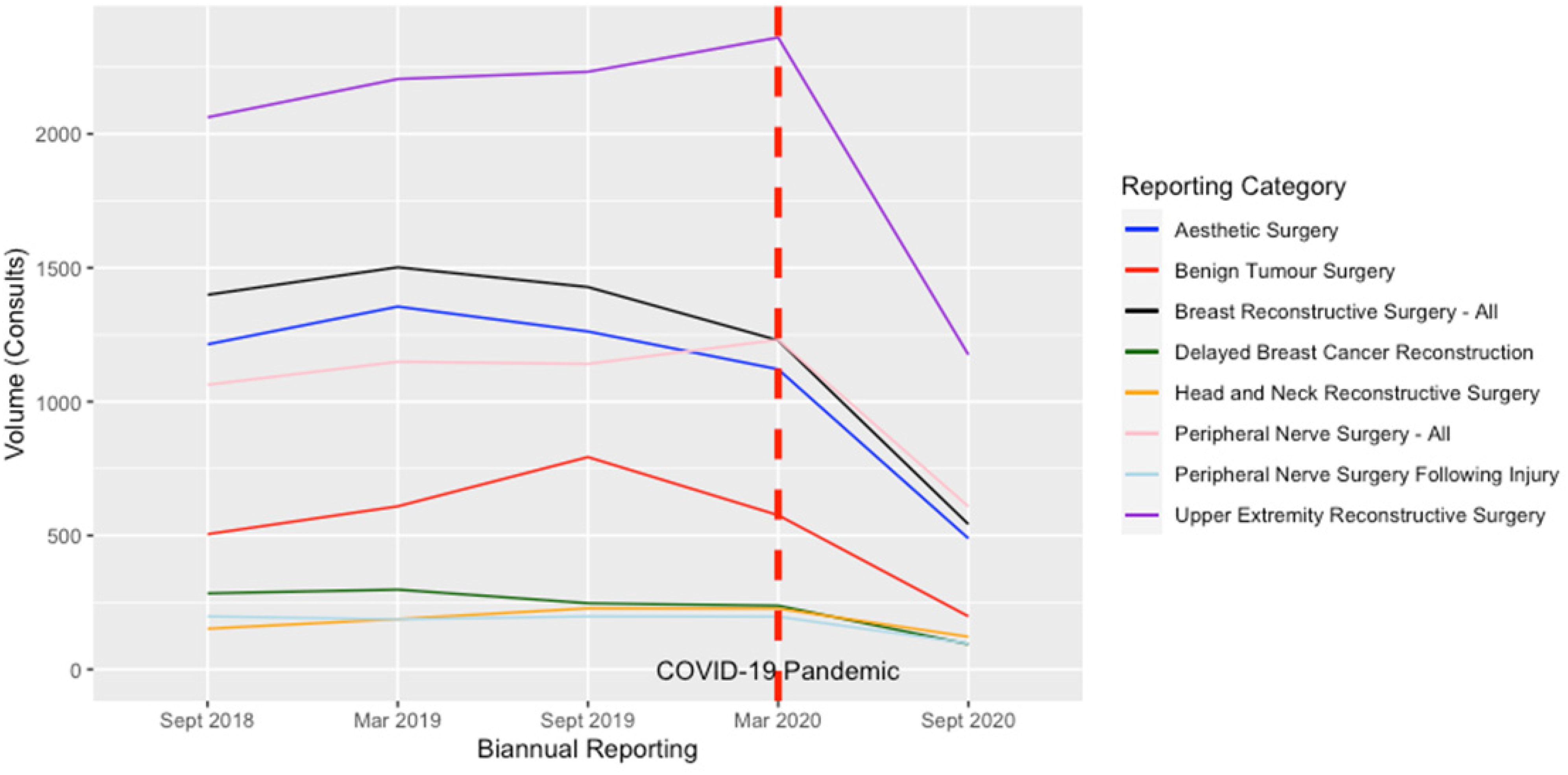
The Changes to the Consult Volumes Before and After the COVID-19 Pandemic.
The Impact of COVID-19 on Waiting for a Consultation or for a Hand and Peripheral Nerve Surgery.
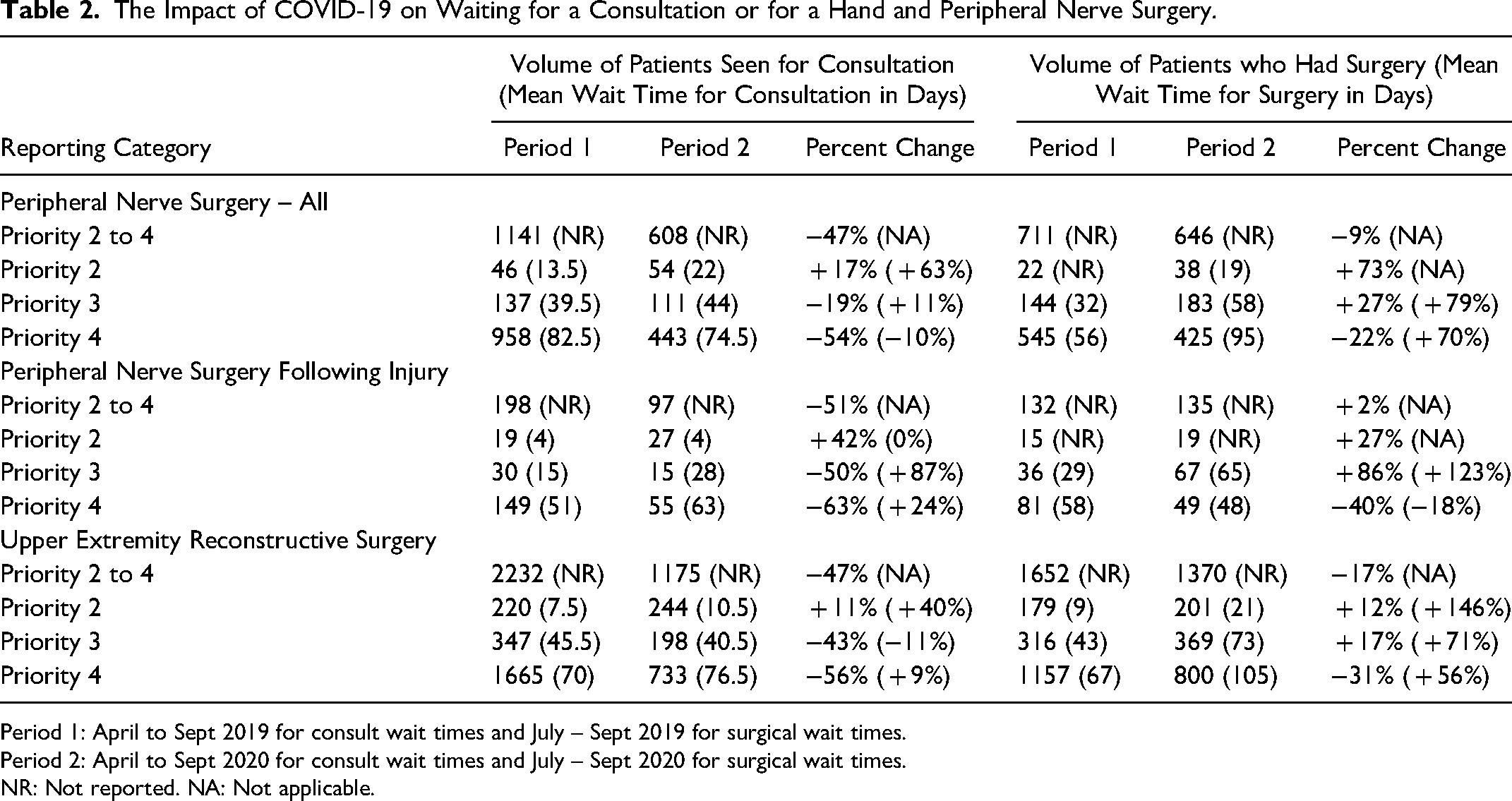
Period 1: April to Sept 2019 for consult wait times and July – Sept 2019 for surgical wait times.
Period 2: April to Sept 2020 for consult wait times and July – Sept 2020 for surgical wait times.
NR: Not reported. NA: Not applicable.
The Impact of COVID-19 on Head and Neck, Breast, Aesthetic and Benign Tumour Surgeries.
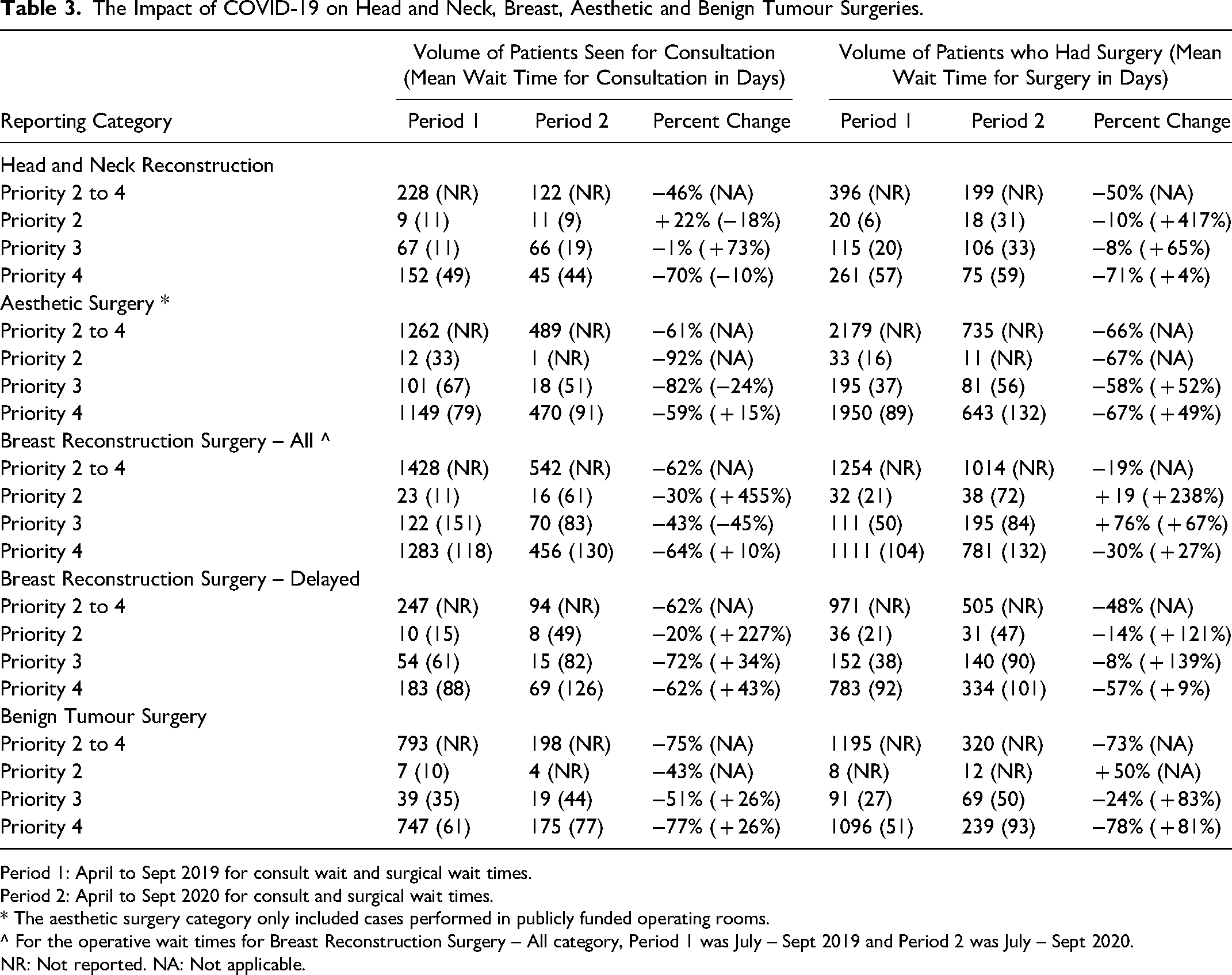
Period 1: April to Sept 2019 for consult wait and surgical wait times.
Period 2: April to Sept 2020 for consult and surgical wait times.
* The aesthetic surgery category only included cases performed in publicly funded operating rooms.
^ For the operative wait times for Breast Reconstruction Surgery – All category, Period 1 was July – Sept 2019 and Period 2 was July – Sept 2020.
NR: Not reported. NA: Not applicable.
The Impact of COVID-19 Pandemic on the Percentage of Consults and Operative Cases Seen within the Provincial Target Wait Times.
Wait Times for Surgery
There was a 43% reduction in the number of operative cases performed during the study period compared to the baseline period (p-value = 0.005). A reduction was seen across all the categories except for burn surgery and traumatic peripheral nerve surgery, which had a slight increase in the operative volume (2%) as they were less affected by elective surgery's shutdown. In all the other categories, the reduction ranged from 9% to 73%, with the lowest reduction reported in aesthetic surgery. The percentage of cases meeting the provincial wait time target decreased by 15% (p-value<0.0001, 95% CI:14.0-16.6%). The reduction was observed in all operative categories and ranged from 1.5% to 25%. There was a statistically significant increase in the mean wait times for surgery at the aggregate level by a mean of 32 days (p-value<0.0001). For priorities 2, 3 and 4, the mean increase was 27 days, 33 days and 33 days, respectively (p-values = 0.01, <0.001 and 0.005, respectively). Tables 2, 3 and 5 summarize the differences between the baseline period and the study period in different reporting categories. Table 4 provides the percent differences in surgical cases meeting the provincial target for each category. Figure 2 illustrates the changes in the surgical volume before and after the pandemic.
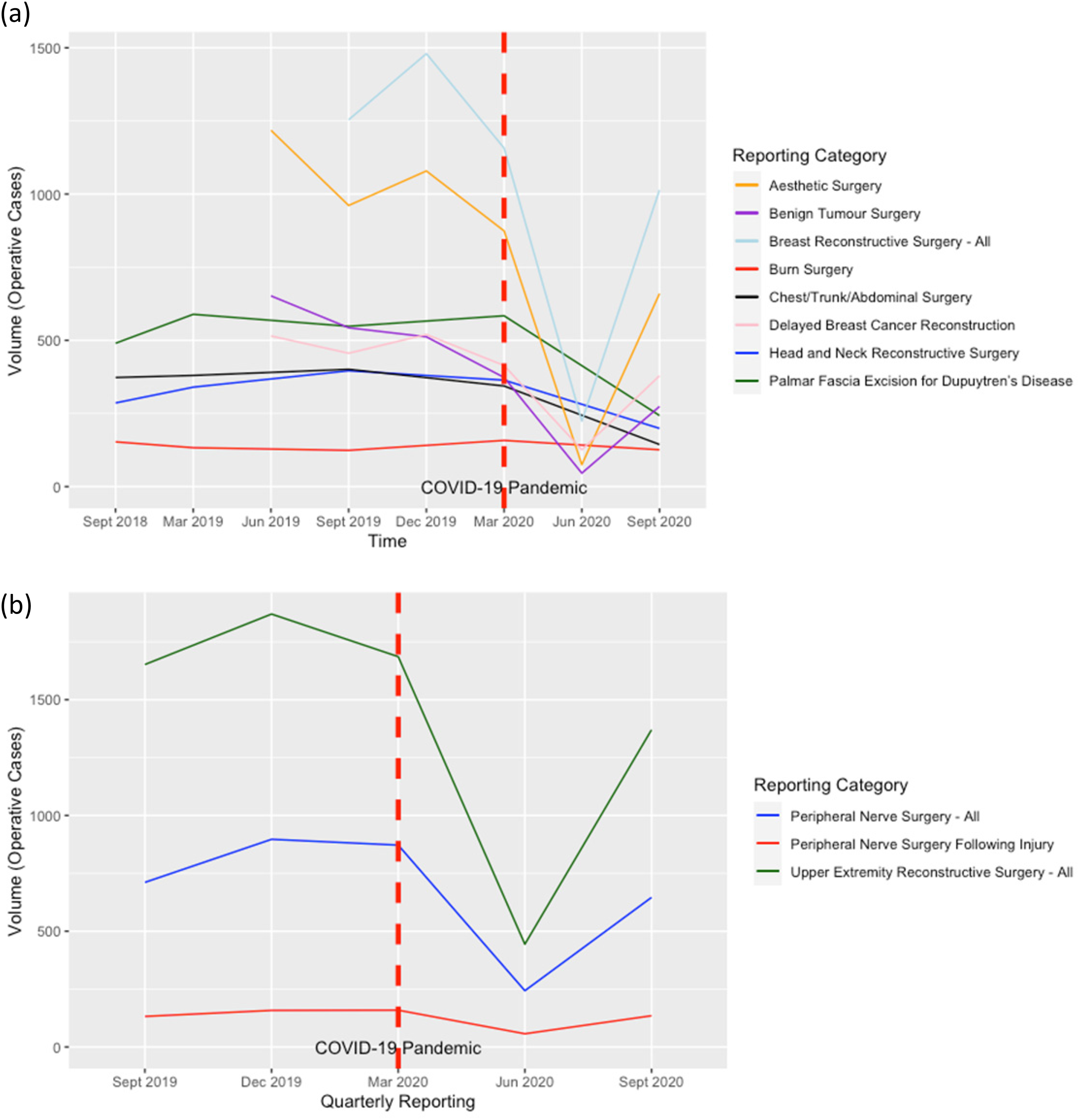
The Changes to the Surgical Volumes Before and After the COVID-19 Pandemic.
The Impact of COVID-19 on Burn and Other Reconstructive Surgeries.
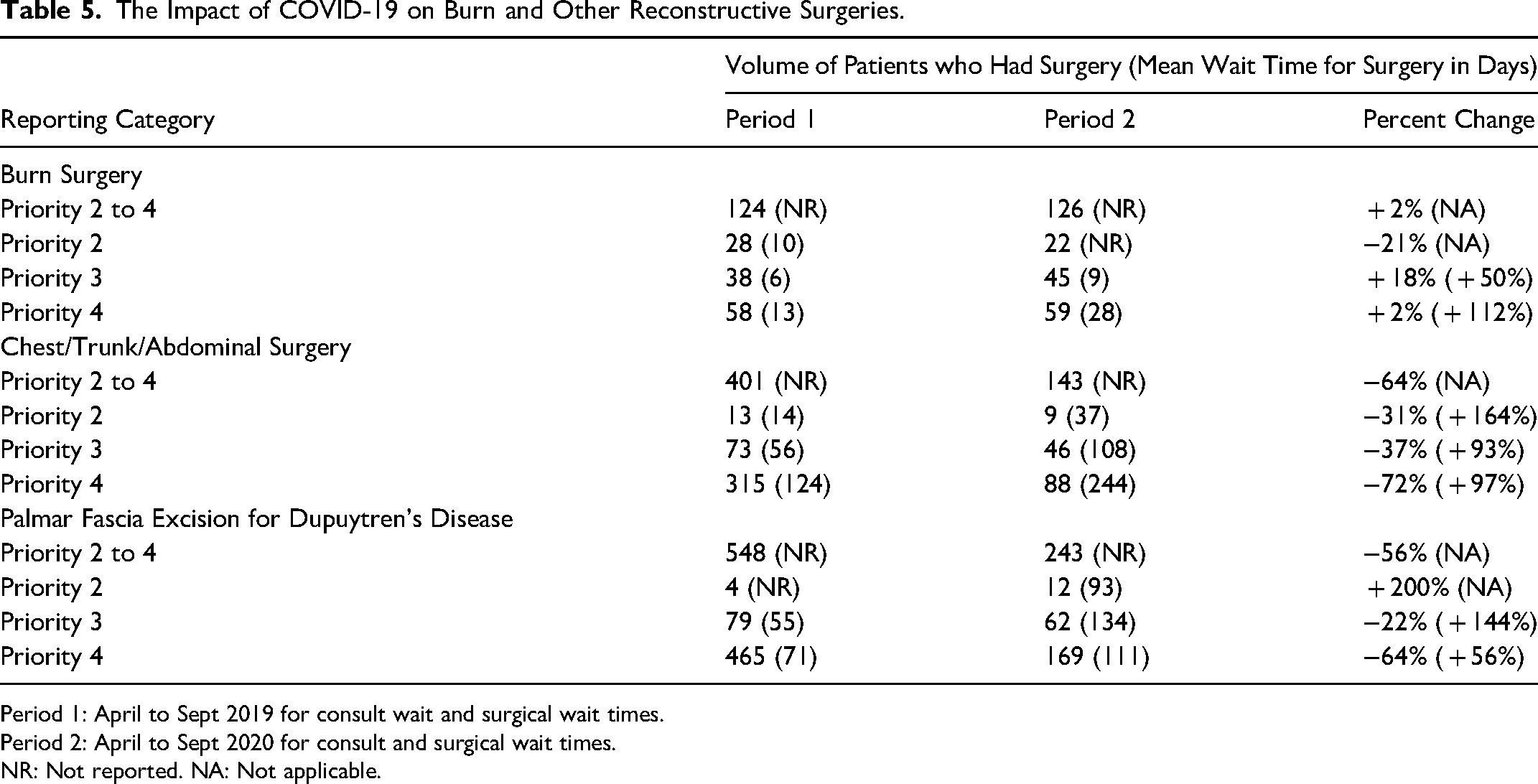
Period 1: April to Sept 2019 for consult wait and surgical wait times.
Period 2: April to Sept 2020 for consult and surgical wait times.
NR: Not reported. NA: Not applicable.
Time Trends for Consultation and Surgical Wait Times
Plotting the wait times highlighted the impact of the pandemic on the surgical wait times for certain categories, such as breast reconstruction surgery, including priority 2 and 3. A similar trend in increased wait times was seen in aesthetic and benign tumour surgeries. Wait times for some categories were less impacted by the pandemic in specific priorities. For example, head and neck reconstruction surgery had similar trends over time for priority 4, but priority 2 had a steep increase following the pandemic. A notable increase across all priorities was seen in surgical wait times for burn, trunk and upper extremity surgery. Overall, wait times for consults were less sensitive to the pandemic compared to surgical wait times, likely due to the wide spread use of telemedicine. Figure 3 summarizes the wait time trends for three large categories (breast reconstruction, upper extremity reconstruction and peripheral nerve surgery).
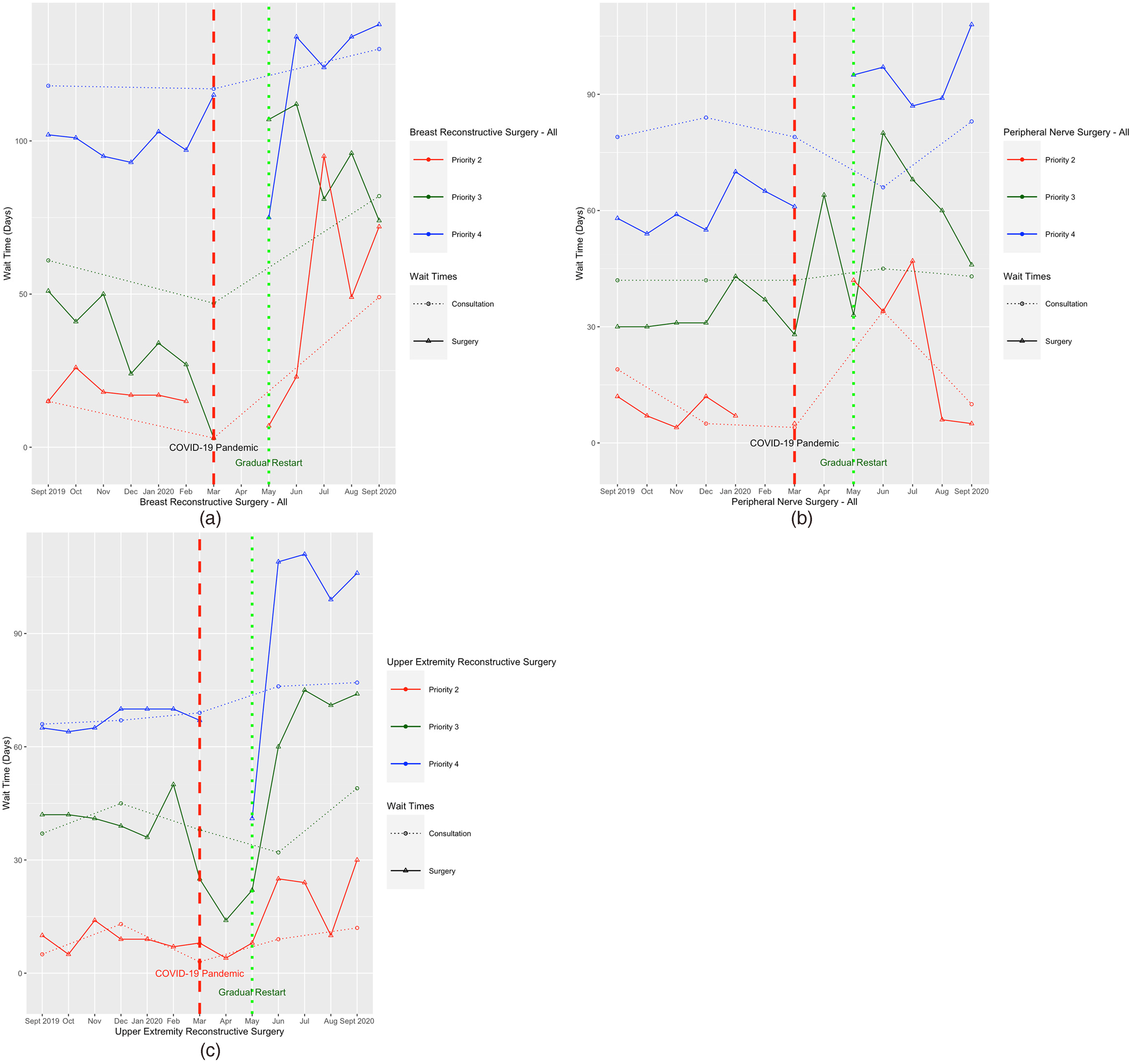
Recent Time Trends in Wait Times for Consultation and Surgery: Breast, Aesthetic and Benign Tumour Surgery.
Paediatric PRS
A total of 372 paediatric consults were completed during the study period compared to 740 consults in the baseline period, representing a 49.7% reduction in the consult volume after the start of the pandemic. The operative volume during the study period was 884 cases compared to 1501 cases in the previous year (41.1% reduction). The percentage of consults completed within the provincial target wait times increased by 3.5% (80.5% during the study period and 77% during the baseline period, p-value = 0.23, 95% CI: − 1.9%–8.6%). The percentage of surgeries meeting the provincial wait time targets decreased by 11% (74.5% during the study period and 85.5% during the baseline period, p-value<0.0001, 95% CI: 7.5%–14.4%). Table 6 summarizes the changes in wait times stratified by priority.
The Impact of COVID-19 on Paediatric PRS.
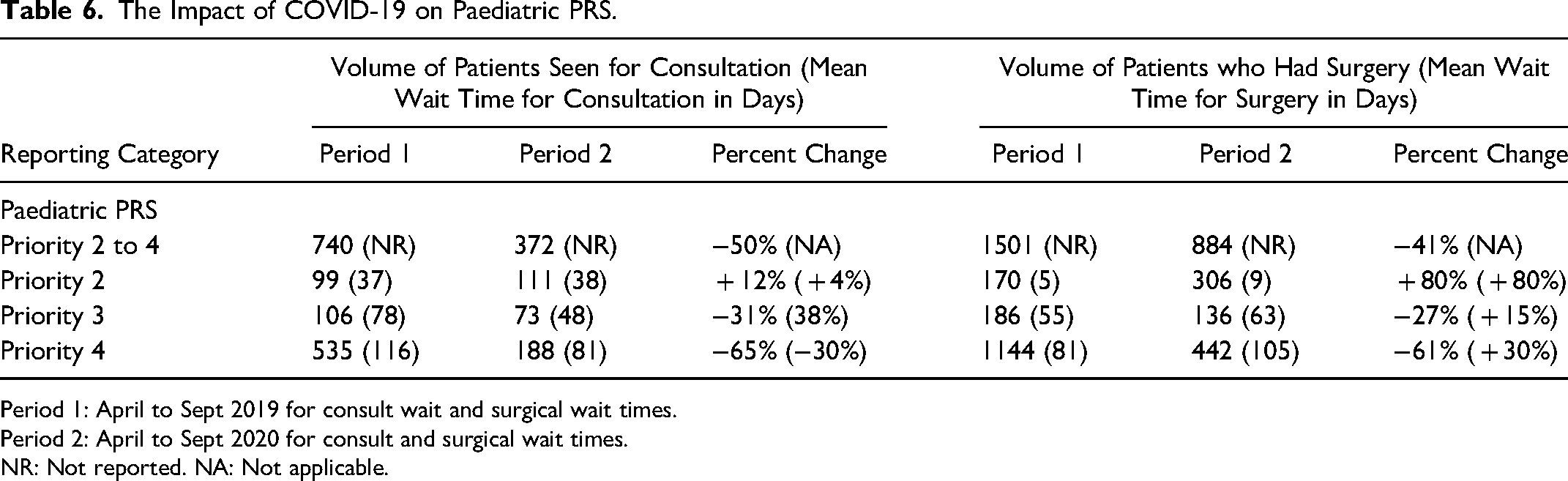
Period 1: April to Sept 2019 for consult wait and surgical wait times.
Period 2: April to Sept 2020 for consult and surgical wait times.
NR: Not reported. NA: Not applicable.
Discussion
This study identified a significant impact of COVID-19 on the delivery of PRS healthcare services across multiple categories. Despite a significant reduction in the volume for consultations and surgery, there was an overall increase in wait times that impacted the provincial benchmarks for healthcare delivery.
The current PRS literature consists primarily of strategies to circumvent the pandemic's effect on service delivery. 9 In a systematic review, most of the current literature consists of expert opinions, commentaries, case reports and surveys. 9 Our study presents population-level data that identifies the system-wide effect of the pandemic across multiple categories for both the adult and the paediatric population. We also examined the effect of the increased wait times on each priority to provide more insight on the delay for more urgent consults and surgeries.
There are several reasons to investigate the impact of the pandemic on PRS. First, it allows the identification of system-wide volume changes in certain categories. Second, it will assist healthcare policymakers in planning future resources to address the increasing backlog. For example, in our study, we identified minimal changes in the volume of burn surgery. However, there was a steep increase in surgical wait times. Adding additional operative time and resources for regional burn centres and funding additional allied health professionals to manage the postoperative patients may reduce the wait times. A similar approach can be taken for other categories in academic and community settings. Finally, measuring the time trends for surgical volume and wait times can allow advanced modeling strategies to predict the expected time to return to the baseline volumes, and the effect of relief strategies in further reducing this period. 15
The backlog of consults and elective surgeries is substantial. A single-centre study conducted in South Africa showed that it would take 315 days to clear their surgical backlog. 16 The amount of time required to clear the PRS backlog at the population level is unknown. Shaw et al. postulated that it would take months to years to address this gap. 7 After a hypothetical 12-week cancellation of all elective surgeries, a modeling study predicted that it would take 90 weeks to manage the backlog if the baseline volumes were increased by 10%. 15 The study used projections, and modeling the population-level data will provide more accurate estimates. 15 There are many challenges to meet the target wait times following the pandemic. 6 Squitieri and Chung identified the need to establish protocols for prioritizing procedures and surge capacity planning. 17 Planning for resource allocation is needed to ensure the recovery of the healthcare system. There are opportunities for our speciality to take the lead in managing the growing backlog. 18
The impact of the reduced surgical volumes and increased wait times on the patient-level is not well-defined. For certain categories, such as traumatic peripheral nerve injuries, there is a more urgent need for timely intervention. In the wake of the pandemic, a Canadian peripheral nerve consensus recommended definitive management for patients with traumatic nerve injuries within 6 months, including consultation, investigations and surgery. 19 We have previously described the wait times for traumatic peripheral nerve surgery, and we identified that more than 90% of the cases were meeting the provincial target wait times. 11 In this study, the wait times for traumatic peripheral nerve surgery increased by more than one-fold for priority 3, with a slighter increase in wait times for consultations. It is not clear from our data if the delays were related to public health policies or patient factors. Nonetheless, delays in the surgical management for nerve injuries can impact motor and sensory recovery.19–23 Thus, timely surgical delivery is essential for traumatic peripheral nerve injuries.
Another concern with delays to healthcare access involves patients’ distress. A study in patients waiting for joint replacement surgery patients identified a high level of psychological distress and poor health-related quality of life. 24 Breast reconstruction patients also experience psychological distress and impaired body image with surgical delay.25–27 Delays in surgery can also impact the return-to-work times for some patients. 6 Some patients may present with advanced conditions due to surgical delay. 6 In our study, we identified overall trends of increased wait times despite a substantial reduction in volumes. Resuming the baseline volumes across the province may further increase the wait times. For all the above reasons, it is critical to implement strategies to manage the wait times in the long-term similar to previous surge management plans. 17 One approach is upgrading the priority level for patients who wait two times longer than the target wait time for their priority level.
Several strategies have been proposed to manage the volume reduction and increased wait times. Boyce et al. reviewed the PRS literature systematically and identified the two most common strategies to minimize the pandemic's impact were prioritizing urgent care and telemedicine. 9 In PRS, high patient satisfaction was found after implementing telemedicine, with clear benefits for patients with access to care barriers.28,29 Our study identified that most wait times for consultation were meeting the provincial target for wait times with a minimal reduction after the onset of the pandemic. However, there was a significant reduction in the consultation volumes. Telemedicine use is effective during the pandemic, but it has its challenges resulting in lower consultation volumes. 30 Patel and colleagues reviewed the outpatient visits in the United States. Despite the increase in telemedicine visits, the total outpatient visits decreased by 9.1%. 30 Their data were not stratified by speciality, and it is unknown how much PRS outpatient visits were reduced. 30 In the PRS literature, a single institution study identified a 45% reduction in clinic volumes despite an increase in telemedicine visits to account for 45% of all outpatient visits. 31 Other limitations of telemedicine include the thorough assessment of surgical incisions and wounds and the inefficient utilization of the surgeon's clinic time.31–33 Although telemedicine was utilized in an unknown proportion of the consultation visits in our study, the overall volume reduction was far more pronounced. The pandemic's effect can be further mitigated with additional resources and personnel supporting telemedicine visits to increase efficiency and consult volumes while maintaining high quality of healthcare services. 34 Other suggested recovery strategies include the use of Wide Awake Local Anaesthetic No Tourniquet (WLANT) methods, the availability of outpatient minor operative settings, and the utilization of absorbable sutures to minimize outpatient visits.7,9 The ongoing monitoring of the wait times may aid in evaluating the implemented strategies.
Our study had several limitations. We were limited by analyzing the data at the aggregate levels, which reduced the power to detect smaller differences within each category. Nonetheless, we were able to detect statistically significant differences in the study given the magnitude of change. We also did not adjust our analysis with potential confounders, such as accounting for academic and community sites, as this information was not publicly available. Due to the available data range, we used a six-month study period for most but not all of the reporting categories. There might have been some outliers in specific categories that skewed the results. Although we observed a substantial reduction in volumes and an increase in wait times, data on clinical outcomes were not available to the authors. Despite a theoretical risk with surgical delay in some reconstructive surgeries, we were unable to investigate the impact of delay on clinical conditions. Finally, the aesthetic surgery category only represented consultations and surgeries performed in publicly funded settings, and the data do not represent all cases in the province. Thus, the data should be interpreted with caution.
Conclusion
In Ontario, COVID-19 has had a profound impact on PRS across multiple categories. The overall trends were a decrease in operative volumes, an increase in surgical wait times, and a decrease in the percentage of cases meeting the provincial wait time target. Healthcare policymakers need to plan resources to facilitate the recovery of the healthcare service following the pandemic. Strategies to reduce the long wait times and increase volume following COVID-19 will be essential to ensure timely healthcare delivery. Surgical wait times will continue to serve as a benchmark for the delivery of healthcare services.
Footnotes
Acknowledgment
The authors acknowledge the role of Ontario Health (Access to Care) team in reviewing the manuscript before submission. Parts of this material are based on data and information provided by Ontario Health. The opinions, reviews, view and conclusions reported in this publication are those of the authors and do not necessarily reflect those of Ontario Health. No endorsement by Ontario Health is intended or should be inferred.
Author Contributions
Dr Saggaf contributed to the design of the study, analysis and interpretation of the results, drafted the article, and approved the final version for publication.
Dr Anastakis contributed to the concept of the study, interpretation of the results, critically revised the manuscript, and approved the final version for publication.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Disclosures
Dr Saggaf has no Disclosures. Dr Anastakis is the Clinical Lead for Plastic and Reconstructive Surgery, Access to Care, Ontario Health. Dr Anastakis receives financial payment for work done as Clinical Lead ($10,000/annum).
Ethics Statement
The submitted study used publicly available data, and it was exempt from IRB approval. However, the study is conforming to the Declaration of Helsinki.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.