
Abstract
Importance
Despite efforts to ensure equitable access to medically necessary services, disparities in care may persist in pediatric otolaryngology services.
Objective
To examine the relationship between socioeconomic marginalization and surgical wait times for tympanostomy tube insertion in the healthcare system of Ontario.
Study design
Population-based, retrospective cohort study utilizing administrative health data.
Setting
Ontario, Canada.
Participants
Patients ≤12 years who underwent bilateral tympanostomy tube insertion between 2010 and 2023 were included.
Exposures
Socioeconomic marginalization measured by the Ontario Marginalization Index, rurality and immigrant status.
Main Outcome Measures
ENT visit within 90 days of surgery, age at ENT visit, time from ENT visit to surgery, number of ENT visits during each year of follow-up, time to tympanostomy tube removal, and delayed tympanostomy tube removal (≥5 years post-surgery).
Results
A total of 76,574 tympanostomy tube patients were analyzed. As compared to the least marginalized patients, the most marginalized patients were significantly less likely to have an ENT visit within 90 days of surgery (75% vs 81.3%, P < .001). The number of emergency department visits (1: −15%, ≥2: −29%) was protective, decreasing age at ENT visit (P < .001). Furthermore, rural residence significantly increased the risk of higher age at ENT visit (+7%) (P < .001). Immigrant children were older at their final ENT visit and had longer surgical wait times compared to non-immigrant children (P < .001).
Conclusion
Significant disparities exist in accessing tympanostomy tubes; socioeconomic marginalization, prior emergency department visits, sex, immigrant and rural status delaying the age at final ENT visit before surgery.
Relevance
These findings underscore the need for targeted strategies to improve equitable access to pediatric ENT services.

Key Message
Marginalized, rural, and patients who are immigrants accessed ENT care at an older age and were associated with an increased delay to surgery.
Differences in emergency department use may reflect disparities in accessing longitudinal primary care.
There is a need for targeted strategies to improve equitable access to pediatric ENT services.
Background
The values of universality and accessibility are the pillars of the Canadian healthcare system. 1 Unfortunately, pronounced social inequalities in access and availability to healthcare are particularly endemic to already marginalized communities. This can result in delayed care, which often transforms an acute and potentially reversible illness or injury into a chronic, irreversible condition that involves permanent disability.
Social determinants of health can impact when and how a patient seeks care and the quality of care they receive. Numerous pediatric surgical procedures are impacted by the length of time to diagnosis and timely surgical intervention. Insertion of tympanostomy tubes (TTs) is one of the most common surgical procedures in children. 2 TTs are frequently inserted for patients with an otitis media with effusion (OME). 2 OME disproportionately affects children younger than 7 as their eustachian tube and immune systems have not completely matured. 2 Current treatment guidelines suggest TTs be inserted in children with OME of 3 months or longer (chronic OME) or in those with recurrent acute otitis media and OME at the time of assessment. There are serious complications of delayed diagnosis and treatment such as persistent ear infections, increased risk of complications, hearing loss, and decreased quality of life. 2
In Canada, Health Quality Ontario categorizes the majority of patients with OME as Priority 3. 3 This signifies that patients should be seen by the surgeon within 90 days of received referral. 3 Furthermore, it outlines, “a moderate probability that delay in treatment will adversely affect physical, emotional, or psychosocial development.” 3 Priority 3 patients are recommended to have the time from decision of surgery to TT to be within 42 to 70 days. 3 These target times are within which 9 out of 10 patients should be seen.
In the Canadian healthcare system, pediatric patients generally require referral from a family physician or pediatrician to access otolaryngology care. As a result, access to specialty care is closely linked to primary care attachment and referral pathways. The timely insertion of TT helps relieve symptoms, improve hearing, and prevent complications. For these reasons, this study investigated whether marginalization impacts age at last ENT visit before surgery and subsequent time to surgery.
Methods
Study Design
This retrospective cohort study utilized administrative and clinical health data held at ICES (formerly the Institute for Clinical Evaluative Sciences). The study examined pediatric bilateral TT insertion in Ontario Canada, from April 1, 2010, to March 31, 2023.
ICES is a prescribed entity under section 45 of Ontario’s Personal Health Information Protection Act. Research conducted at ICES that meets the Privacy and Compliance Office requirements does not need patient consent or approval of a research ethics board.
Databases
The Canadian Institute for Health Information (CIHI) Discharge Abstract Database (DAD) and Same Day Surgery (SDS) databases and the Ontario Health Insurance Plan (OHIP) database were used to identify the study cohort as well as to capture baseline variables and outcomes. The Immigration, Refugees and Citizenship Canada (IRCC) database was used to capture immigration status. The Registered Persons Database (RPDB) was used for demographic variables such as age, sex, rural/urban residence, and income quintile and the ICES Physician Database (IPDB) was used in conjunction with OHIP to identify ENT visits. Additionally, the National Ambulatory Care Reporting System was used to capture Emergency Department (ED) visits.
The Ontario Marginalization Index (ON-Marg) was used to estimate the level of marginalization for patients included in the study. 4 ON-Marg data are census-based and are applied to patients geographically based on postal code. It is reported in quintiles, with a higher score indicating a higher level of marginalization. ON-Marg is comprised of 4 dimensions: age and labor force, material resources, racialized and newcomer populations, and household dwellings. 4 Material resource examines factors such as access to income, employment, and housing stability. 4 Age and labor force examines age demographics and labor force participation levels. 4 The racialized and newcomer population index considers the concentration of immigrant and racialized populations. 4 The households and dwellings dimension assesses housing density and suitability of living conditions, among other factors. 4 We additionally calculated a summary score, which represented the average quintile score across the ON-Marg dimensions.
Inclusion/Exclusion Criteria
The study cohort included pediatric patients aged 12 and under who underwent at least one TT procedure as documented by the Z914 OHIP billing code and a procedure code for TT in the independent CIHI DAD or SDS database. A full list of fee codes for tube insertion, removal, and demographic factors has been included in the appendix (Appendix Table S1).
Patients were excluded if they were missing demographic or ON-Marg data. Patients who were non-Ontario residents, underwent unilateral TT insertion, did not have a TT OHIP billing record, or who had undergone a previous TT insertion were excluded.
Variables
Baseline variables collected include age, sex, rural residence, income quintile, ON-Marg scales and summary scores, ED visits in the previous year, primary care provider type, and immigration status (not born in Canada). Comorbid conditions, such as Down syndrome, cleft palate, Charlson Comorbidity Index (CCI) score, and previous intensive care unit (ICU) admissions were identified.
The primary variables included age at last ENT consult before surgery, time from last ENT visit to TT insertion, and age at surgery.
Outcome measures were defined as ENT visit within 90 days of surgery, number of ENT visits during each year of follow-up (years 1, 2, and 3), time to TT removal (9 months to 8 years), and delayed TT removal (≥5 years post-surgery). Number of ENT visits during each year of follow-up and delayed tube removal was captured for a subgroup of patients based on accrual date.
Data Validation
Data validation steps ensured consistency between datasets (eg, matching OHIP records with DAD/SDS procedures). Reviews were conducted at each stage to confirm adherence with the prior study plan.
Statistical Analysis
Descriptive statistics summarized baseline characteristics overall and were stratified by ON-Marg score. As directed by the scale developers, prior to calculation of the summary score, a correlation matrix was explored to ensure that each of the ON-Marg dimensions was correlated with study outcomes in the same direction. The newcomer and racialized populations dimension was found to correlate in the opposite direction as the other 3 and was consequently not included in the ON-Marg summary score. Continuous variables were reported as means (SD) or medians (IQR), and categorical variables as counts (%). The baseline variables were dichotomized to the upper 50th percentile versus lower 50th percentile of the ON-Marg summary score. Outcomes are also reported for groups based on the 50th percentile of the ON-Marg summary score, as well as by quintile of the summary score. Outcomes were compared across quintiles using the Cochran–Armitage trend test for categorical outcomes and one-way ANOVA and Kruskal–Wallis tests for continuous outcomes. The standardized mean differences (SMD) were reported for baseline variables. SMD were considered clinically significant when greater than 0.10. 5
A subgroup analysis was conducted, excluding patients impacted by COVID-19. In this analysis, patients were included if they had TT inserted prior to March 15, 2020. Additionally, subgroup analysis was performed for both time to TT removal (patients with TT insertion prior to March 31, 2020) and delayed tube removal (patients with TT insertion prior to March 31, 2015). Delayed tube removal was defined as ≥5 years post-surgery to allow for sufficient follow-up. Restricting accrual to dates that accommodated this predefined follow-up window ensured complete follow-up for all included patients in this analysis.
Linear regression models were used to evaluate the relationship between marginalization and age at final ENT visit and time from final ENT visit to surgery. The following covariates were included in the model: ON-Marg summary score, sex, age (log transformed), ED visits in the previous year and rurality.
For all analyses, reported P-values are from 2-tailed tests where a value of <.05 was considered statistically significant. All analyses were performed using SAS EG version 7.15 (SAS Institute, Cary, NC, USA).
Results
We initially identified 103,870 patients who met the inclusion criteria. Following data quality steps and application of exclusion criteria, 76,574 patients remained (Appendix Figure S1). The baseline demographics, temporal trends, and outcomes are summarized in Appendix Tables S2 to S5. Primary results were analyzed below with a linear regression model analysis (Tables 1-3).
Results From Linear Regression Model Predicting Log-Transformed Age at ENT Visit.

Abbreviation: ON-Marg, Ontario Marginalization Index.
Results From Linear Regression Model Predicting Log-Transformed Delay From ENT Visit to Surgery.

Abbreviation: ON-Marg, Ontario Marginalization Index.
Compare Final ENT Visit by Immigrant Status.

Baseline Demographics
The baseline demographic analysis dichotomized the patients into the upper (n = 36,641) and lower (n = 39,933) 50th percentile based on their ON-Marg summary score (Appendix Table S2). The upper 50th percentile reflects the more marginalized patients whereas the lower 50th percentile represents the less marginalized patients.
The patient population consisted of 61.5% males and a mean age of 3.17 ± 2.11 years with no significant difference in age (SMD = 0.06). As expected, patients with a higher degree of marginalization were more likely to have a lower household income (SMD = 0.92 for income quintile 1).
Comorbidities—Down syndrome, cleft palate, CCI, ICU admissions
There were no differences in the number of patients with Down syndrome and cleft palate between cohorts (SMD = 0.01 and 0.03, respectively). Similarly, no significant difference in the Charlson Comorbidity Index and ICU admissions was demonstrated between cohorts (SMD = 0.02 and 0, respectively).
Hospital and physician encounters
Baseline data demonstrated no meaningful difference in the number of ENT visits in the previous year between the upper and lower 50th percentile (SMD = 0.04). Notably, patients in the upper 50th percentile were more likely to have had 2 or more ED visits in the previous year (SMD = 0.19). The proportion of patients with less than 2 or more OHIP billings under a pediatrician or general practitioner was higher in the upper 50th percentile than in the lower 50th percentile (2.4% vs 1.5%) (P < .001). The mean duration from the final ENT visit to surgery was 56.21 ± 53.36 days, with a slight difference between cohorts (SMD = 0.03).
Post-Operative ENT Visit and Tube Outcomes Analysis
The mean number of ENT visits during the first follow-up year was 2.17 ± 1.44, with the upper 50th percentile having significantly less ENT visits during the first year of follow-up (P < .001) (Appendix Table S4). Similarly, in the second- and third year of follow-up, the upper 50th percentile continued to have a lower mean number of post-operative ENT visits (year 2: 1.54 ± 1.51 vs 1.71 ± 1.54; year 3: 1.07 ± 1.40 vs 1.18 ± 1.45; P < .001). Furthermore, there were nearly double the patients in quintile 5 (11.6%) that did not have an ENT visit within the first year, compared to quintile 1 (6.9%) (P < .001).
Among patients with follow-up data available for tube removal (n = 69,132), there was no significant difference in mean time to tube removal between cohorts (P = 0.527). Similarly, at the 8-year follow-up, there was no significant difference between cohorts (P = 0.977). Delayed tube removal was rare, occurring in 2.0% of the eligible cohort (684/34,898), with no significant differences between ON-Marg groups (P = 0.355).
Outcomes Quintile
The more marginalized a patient, the fewer number of ENT visits within 90 days of surgery and in follow-up (Appendix Table S5). The overall mean number of ENT visits during follow-up was significantly lower in quintile 5 (4.55 ± 3.30) than quintile 1 (5.23 ± 3.43) (P < .001) (see Figure 1). Similarly, 79.3% of patients had an ENT visit within 90 days of surgery, with a significant downward trend from quintile 1 (81.3%) to quintile 5 (75%) (P < .001) (see Figure 2).
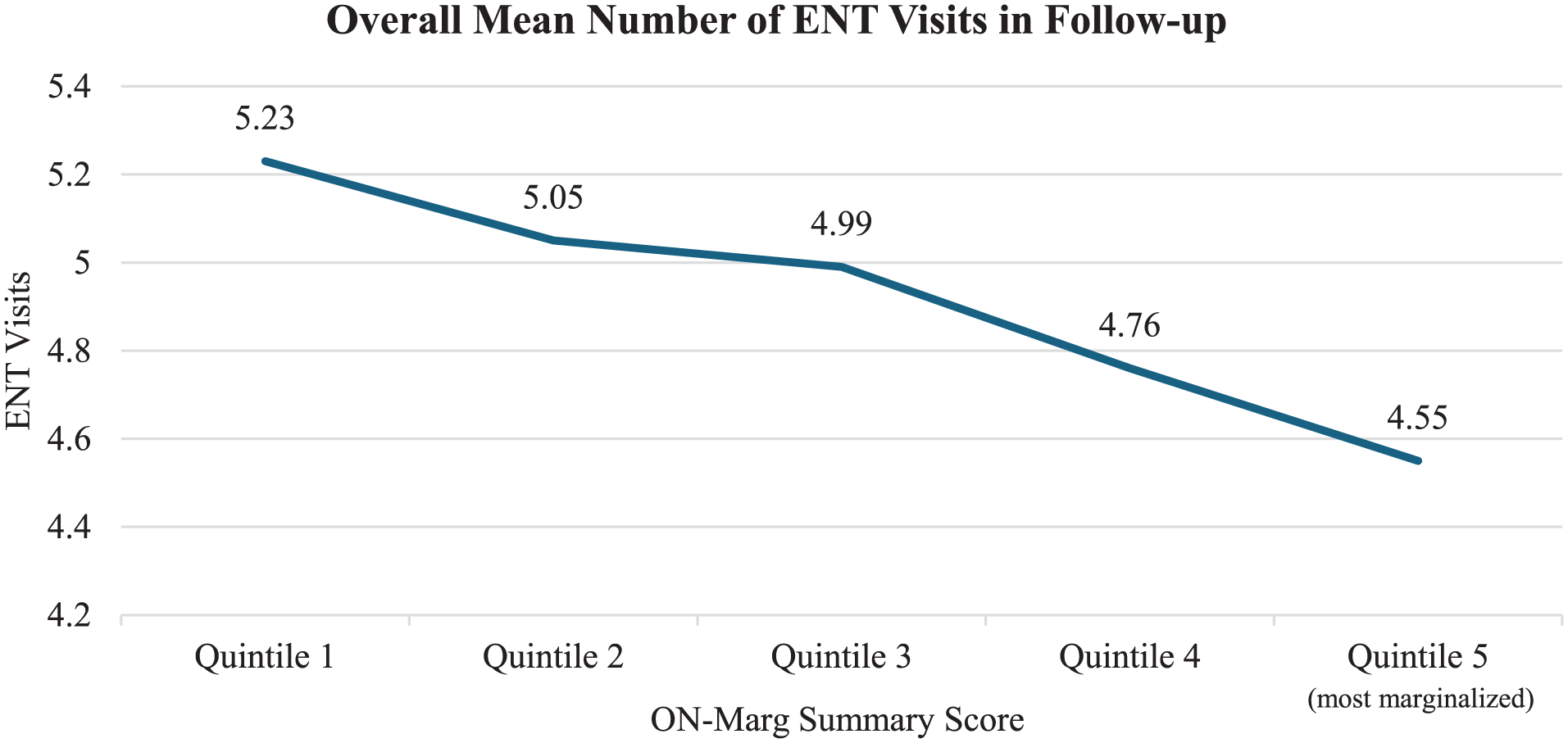
Overall mean number of ENT visits in follow-up (3-year interval) by ON-Marg quintile. ON-Marg, Ontario Marginalization Index.

Proportion of patients per ON-Marg quintile with an ENT visit within 90 days of surgery. ON-Marg, Ontario Marginalization Index.
Subgroup Outcomes Analysis (Non-COVID Impacted Patients)
This subgroup outcome analysis removed patients impacted by the COVID-19 pandemic, resulting in a cohort of 48,883 patients (Appendix Table S6).
The data demonstrated that patients in the upper 50th percentile had a lower number of ENT visits within 90 days of surgery and future follow-up than the lower 50th (P < .001).
Similarly to the entire cohort, trends throughout the 3-year follow-up period demonstrated the upper 50th percentile to have decreased mean visits compared to the lower 50th (P < .001).
Of this cohort, 11.2% (n = 5462) underwent TT removal. There was no difference in time to tube removal between ON-Marg groups (P = .159). Similarly, at the 8-year follow-up, TT removal rates were similar across cohorts (16.3% overall) (P = .977).
Multivariable Linear Regression Analysis
Age at ENT visit
In the multivariable linear regression analysis, we assessed the impact of ON-Marg quintile, sex, number of ED visits, and rural residence on the age at ENT visit (see Table 1). Compared to the least marginalized (ON-Marg quintile 1), there was a stepwise increase in the risk of a higher age at ENT visit (from 2.8% to 9.0%), and each level was significantly increased compared to the least marginalized ON-Marg quintile. Male sex (−6.6%) and number of ED visits (1: −15%, ≥2: −29%) significantly decreased the risk of an increased age at ENT visit. While rural residence significantly increased the risk of higher age at ENT visit (+7%).
Predicting delay from ENT visit to surgery
The data from the linear regression demonstrated that ON-Marg summary scores and sex do not have a significant association with delay from ENT visit to surgery (P > .05) (Table 2).
Interestingly, one or more ED visits were associated with a reduction in delay (−3.2%) to surgery. Compared to urban patients, rural patients experienced a longer delay (+7%) in surgery.
Immigrant versus non-immigrant comparison
Statistical analysis comparing age at final ENT visits and surgical delays between patients who are non-immigrants (n = 75,597) and immigrants (n = 977) demonstrated pronounced differences (see Table 3). Patients who are immigrants were nearly double the age at the time of final ENT visit (5.31 ± 2.48 years) than that of non-immigrant patients (2.99 ± 2.08 years). Additionally, patients who are immigrants experienced significantly longer wait times to surgery (61.96 ± 63.03 days) compared to patients who are not immigrants (56.13 ± 53.23 days).
Discussion
This population-based study highlights how marginalization, rurality and immigrant status contribute to disparities in access to ENT care among children. Using the validated ON-Marg tool, our results demonstrate a clear association between the level of marginalization and older age at ENT consultation prior to surgery. While the difference in mean age at last ENT visit before surgery between the most and least marginalized patients (3.1 years vs 3.0 years) may not be clinically significant in isolation, it reflects a consistent, statistically significant trend across a large population. In a healthcare system that is universally funded, any systematic delay in access based on socioeconomic status raises concern. Notably, the magnitude of difference is larger for certain subgroups (ie, immigrant children). The fact that marginalized, rural, and patients who are immigrants are older at the time of their last ENT visit before surgery suggests deeper issues in how and when care is accessed.
Through an intersectional lens, it is evident that social determinants of health impact ability to seek care and the quality-of-care patients receive. Immigrant patients demonstrated nearly a 2-fold increase in age at their final ENT visit and a greater delay to surgery. These disparities may be influenced by limited care in their country of origin, challenges with the immigration process and barriers accessing healthcare upon arrival. Furthermore, among immigrant families, differences in English language proficiency and primary language spoken may affect access to primary care and tympanostomy tube care.
Geographic barriers also played a critical role in access to care. Children residing in a rural area were associated with an older at age of ENT visit with a greater delay to surgery. Rural children may encounter difficulty accessing primary care, delaying the diagnosis of their condition. Unfortunately, the delayed diagnosis and thus surgery can have downstream effects impacting their communication skills in a pivotal developmental window. 2
Interestingly, ED visits were inversely associated with age at ENT consultation. While this pattern may reflect the severity or persistence of symptoms prompting expedited, it may also suggest fragmented care. Marginalized, immigrant, and rural patients may face consistent barriers to community-based care, whether due to limited availability, language barrier, geographic isolation, or other obstacles. The reliance on the ED for access to otolaryngology specialty care may reflect potential gaps in primary healthcare services for marginalized populations.
Temporal analysis demonstrated significant variations in patient age at ENT consult and surgical wait times over the study period. Notably, there was a sharp increase in surgical wait times during the COVID-19 pandemic, peaking in 2020 compared to the year prior. This disruption likely resulted from elective surgery cancellations and healthcare system strain. While surgical volumes have since rebounded, our findings highlight the long-term consequences of pandemic-related delays, particularly for marginalized populations who already experience healthcare access barriers.
The most recent American Academic of Otolaryngology-Head and Neck Surgery clinical practice guideline on TT in children specifically discussed health disparities. 2 Studies have confirmed that the recommendation for surgical intervention in children is influenced by social determinants of health. 2 Three previous studies have used population data to examine TT insertion in children in Ontario.6 -8 Beyea et al showed that 25% of patients did not receive a preoperative audiogram and 31% did not receive a post-operative audiogram, both of which are recommended as best practices in the clinical practice guideline. 8 There was also geographic variability in pre- and post-operative audiometric testing for the 316,599 patients undergoing bilateral TTs over the study period. 8 These previous studies did not assess the impact of marginalization on access or wait times to TT insertion6 -8 Our study utilizes the ON-Marg index tool to investigate the relationship between marginalization and delays in access to TTs.
The use of a large, population-based dataset and the validated ON-Marg indices allows for robust population analysis. The ON-Marg index combines data from several sources, including Census and Municipal Property Assessment Corporation (MPAC) data, to create a tool that measures multiple spheres of marginalization at the neighborhood level. Published literature demonstrates that the ON-Marg scale is a valuable tool to measure the impact of marginalization on healthcare utilization and outcomes. 4 Previous studies validated ON-Marg as a viable tool in evaluating socioeconomic status on individual health, as a marginalization index in surgery, and used in measuring the association between marginalization and multimorbidity.4,9,10
There are several limitations to this study. As this is a retrospective study, it relies on past data, which may not be complete or accurate. However, where possible we have used multiple data sources to reduce the risk of misclassification. As an observational study, there are potential unmeasured confounders, which can affect the relationship between the exposure and the outcome. The results may be influenced by unmeasured genetic, environmental, or clinical factors that affect tympanostomy tube care and sequelae. Furthermore, audiometric outcomes could not be assessed, as audiogram data are not available within the administrative datasets used. Additionally, ON-Marg data were applied based on geographical neighborhood. There is a potential for ecological fallacy, which arises from grouping of populations together and interpreting their respective outcomes.
Conclusion
This study provides evidence for the urgent need for targeted interventions to provide equitable care to pediatric patients. Future studies should consider interventions for marginalized communities and an evaluation of their impact on surgical wait times. Interventional trials such as community outreach programs, mobile ENT clinics, and expansion of telemedicine services may be possible avenues to explore. We hope this study serves as a catalyst for policy initiatives prioritizing resource allocation to marginalized populations and incorporating equity-based metrics into healthcare planning.
Supplemental Material
sj-docx-1-ohn-10.1177_19160216261422572 – Supplemental material for Does Marginalization Impact Access to Tympanostomy Tube Insertion in Pediatric Patients in Ontario?
Supplemental material, sj-docx-1-ohn-10.1177_19160216261422572 for Does Marginalization Impact Access to Tympanostomy Tube Insertion in Pediatric Patients in Ontario? by Camille Duggal, Britney Le, J. Andrew McClure, Blayne Welk, Sumit Dave and Julie Strychowsky in Journal of Otolaryngology - Head & Neck Surgery
Footnotes
Acknowledgements
This study was supported by ICES, which is funded by an annual grant from the Ontario Ministry of Health (MOH) and the Ministry of Long-Term Care (MLTC). Core funding for ICES Western is provided by several partners, including the Academic Medical Organization of Southwestern Ontario, Schulich School of Medicine and Dentistry, Western University, and the Lawson Health Research Institute. This document used data adapted from the Statistics Canada Postal CodeOM Conversion File, which is based on data licensed from Canada Post Corporation, and/or data adapted from the Ontario Ministry of Health Postal Code Conversion File, which contains data copied under license from ©Canada Post Corporation and Statistics Canada. Parts of this material are based on data and/or information compiled and provided by the Canadian Institute for Health Information, MOH, and Immigration, Refugees and Citizenship Canada (IRCC; current to March 2023). The analyses, conclusions, opinions, and statements expressed herein are solely those of the authors and do not reflect those of the funding or data sources; no endorsement is intended or should be inferred.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a Catalyst Grant from the Department of Otolaryngology—Head and Neck Surgery, Western University, London, Ontario, Canada.
Ethical Considerations
ICES is a prescribed entity under section 45 of Ontario’s Personal Health Information Protection Act. Research conducted at ICES that meets the Privacy and Compliance Office requirements do not need patient consent, or approval of an ethics research board.
Data Availability Statement
The dataset from this study is held securely in coded form at ICES. While legal data sharing agreements between ICES and data providers (eg, healthcare organizations and government) prohibit ICES from making the dataset publicly available, access may be granted to those who meet pre-specified criteria for confidential access, available at ![]() (email:
(email:
Supplemental Material
Additional supporting information is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.