
Abstract
Background:
Chronic pelvic pain is a complex condition. Few studies have focused on patient expectations of diagnosis and treatment in female chronic pelvic pain populations. Not knowing this information can lead to disparity and frustration between provider care and patient expectations resulting in poor patient outcomes. The aim of this study was to explore patient expectations and understanding of diagnosis prior to engaging in an interdisciplinary pelvic pain program.
Methods:
This is a cross sectional study of women enrolled in a tertiary Chronic Pain Center pelvic pain program in May 2019. Data were extracted from intake questionnaires to classify demographic variables and analyzed using descriptive statistics. Expectations and diagnoses were clustered in themes. Student’s t-test was used to compare biomedical focus and biopsychosocial focus groups to the Pain Disability Index (PDI) and the EQ-5D results, and to compare self-reported diagnoses with treatment expectations between groups.
Results:
When asked about perceived diagnosis, 74% reported a gynecologic cause for their pain, 25.7% reported musculoskeletal causes, and 21.9% reported other health conditions. For treatment expectations: 46.6% believed they required rehabilitation, 30.8% responded “I don’t know”, and 21.2% reported perceived need for medication. There was no difference in PDI or EQ-5D scores between patients who identified perceived treatment options and those who reported “I don’t know”.
Conclusions:
Most patients identified a perceived cause for their pain, but there was uncertainty and ambiguity about treatment options. Understanding and addressing the perception and expectations of individuals is imperative to patient-centered care and can lead to improved outcomes.
Keywords
Background
Chronic pelvic pain is characterized as pain that lasts more than 6 months and is perceived to originate from the pelvis. 1 Chronic pain affects one in five Canadians, 2 and pelvic pain affects 14%–26% of women. 3 Chronic pain continues to be poorly understood and managed, and patients often feel that the health care system has not met their needs. 4
Research has shown that patient expectations can impact clinical outcomes, where expecting a positive outcome is linked to increased benefit from the treatment. 5 When there are discrepancies between patient and provider expectations of care, patient frustrations are often exacerbated leading to worse outcomes.6,7 Earlier studies on patient expectations prior to attending a chronic pain clinic revealed these emerging themes: desire for explanations and diagnosis, pain relief and management strategies, and uncertainty about diagnosis and treatment. However, some patients reported not having any expectations.8–10
There is limited research on the connection between patient expectations and outcomes in chronic pain populations and, to date, there are few studies specifically looking at patient expectations and beliefs when entering a chronic pelvic pain program. Most of these studies have focused on specific conditions, such as endometriosis, in the general population.11,12 The aim of this study was to explore patient expectations and beliefs about their diagnosis and their perceived treatment needs options prior to engaging in an interdisciplinary pelvic pain program. This information would allow the beginning of a dialogue to inform a model of patient centered care.
Methods
This is a cross sectional survey of female patients enrolled in a tertiary Chronic Pain Center pelvic pain program in May 2019. All patients who were enrolled in the pelvic pain program qualified and were approached to participate in the study. Patients were excluded if they were biologically male or identified as male, if their questionnaires were missing, or they declined to participate. This study received research and ethics approval.
The Chronic Pain Center is an interdisciplinary pain program that embodies a comprehensive biopsychosocial approach to pain management. Within the program a specific pelvic pain stream exists for women who have had pelvic pain for more than 6 months. These women have been assessed and treated by a general gynecologist prior to referral. The Pelvic Team sees over 150 new consults per year. The team is comprised of a nurse clinical coordinator, physician (gynecologist), psychologist, pelvic physiotherapist, and kinesiologist. Access to other providers (including dietician, social worker, pharmacist, and psychiatrist) is also available and multiple group programs addressing the multifaceted areas of pain are available to patients throughout their 1-year program. The program also includes pelvic interventions as needed (injections, nerve blocks, and surgery).
At entry into the program, all patients complete an intake questionnaire asking about demographic information, pain history, and treatments. Included in the pre-assessment package are the questions: “What do you believe is the cause of the pain?”; “What treatments do you think you need?”. These questions are open ended and allow women to list, in order, their answers.
Patients also complete the EQ-5D-5L and Pain Dis-ability Index (PDI) questionnaires at intake. The EQ-5D-5L is a validated 13 self-assessed, health related, quality of life questionnaire. 14 In addition, this tool also has an overall health scale where the rater selects a number between 1 and 100 to describe the condition of their health (100 being the best imaginable). The Pain Disability Index (PDI) measures the degree of pain-related disability in seven domains with a range from 0 to 70 (maximum disability). 15 The Pain Disability Index (PDI) is a valid16,17 and reliable 18 instrument.
Data were extracted from intake questionnaires to characterize demographic variables including: age, ye-ars with pain, parity, EQ-5D-5L (measure of quality of life), PDI (pain-related disability), source of income, number of medications and type, previous surgeries (type and number), percentage of pain relief “they feel they would need to do important things” (on a scale with 10% increases from 0 to 100), and other medical diagnoses.
Statistical analysis
Descriptive statistics were used to describe patient demographic variables. For continuous variables, means with standard deviations were used; for categorical variables, proportions with ranges were used.
Patient answers to the question, “What do you believe is the cause of the pain?” and, “What treatments do you think you need?” were used as the presumed diagnoses and expected treatment, respectively.
Presumed diagnoses were clustered in themes by one individual (CJ) with agreement by another (MR). These were then expressed as proportions. The answers for presumed diagnosis were ranked in the order they were listed if more than one answer was given. Participants were given the opportunity to list as many as they felt were relevant. Themes included (1) gynecologic conditions (including endometriosis, dysmenorrhea, and ovarian cysts), (2) mental health conditions, (3) nerve issues, (4) infections, (5) a composite musculoskeletal group (including incorporated musculoskeletal conditions, joint problems, muscular issues, and pelvic floor dysfunction), and (6) other health co-morbidities.
Presumed expected treatments were clustered in themes by one individual (CJ) with agreement by another (MR). These were then expressed as proportions. Patients could list as many expected treatments as desired. They were ranked in the order they were listed. The order and number of answers were catalogued. Themes included (1) mental health treatment, (2) pain management, (3) further investigations, (4) alternative therapies, (5) medication including injections such as steroids or botulinum toxin, (6) specific treatments for a named condition, and (7) rehabilitation which included exercise, physical therapy, and lifestyle changes.
The individual’s presumed diagnoses were dichotomized between identifying only a biomedical diagnosis (e.g. endometriosis) or a more comprehensive biopsychosocial approach (e.g. endometriosis and depression, stress). In a similar fashion, the treatment modalities that individuals felt they required were dichotomized into a biomedical approach (e.g. medications and surgery) or a biopsychosocial approach (e.g. pain management).
Student’s t-test was used to compare PDI and EQ-5D-5L scores between those individuals characterized as a biomedical approach to diagnosis and those with a biopsychosocial approach to diagnosis. These groups were also compared with respect to treatment expectations.
Results
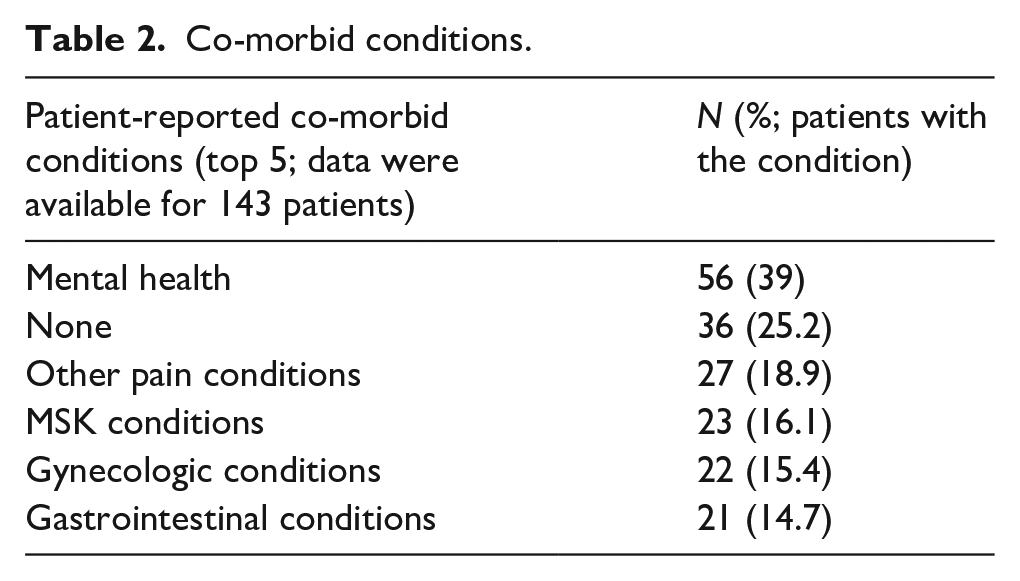
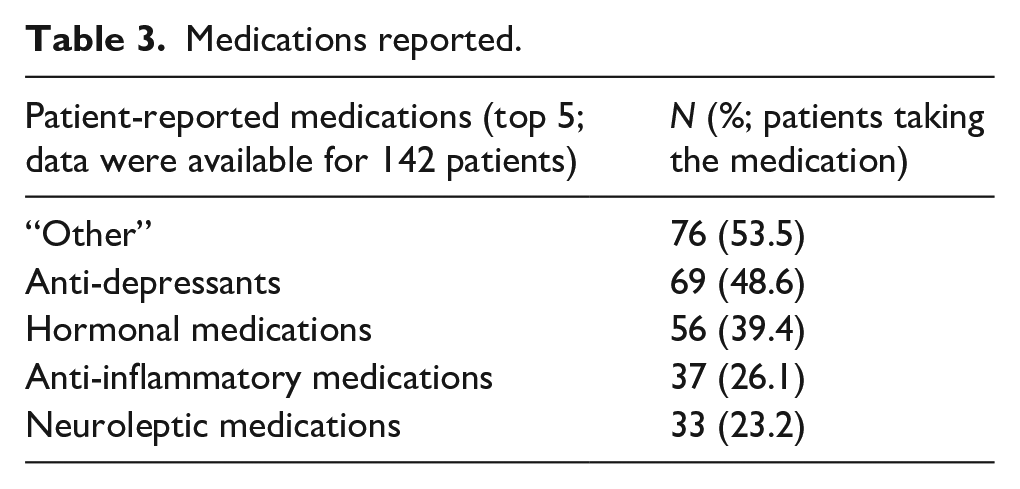
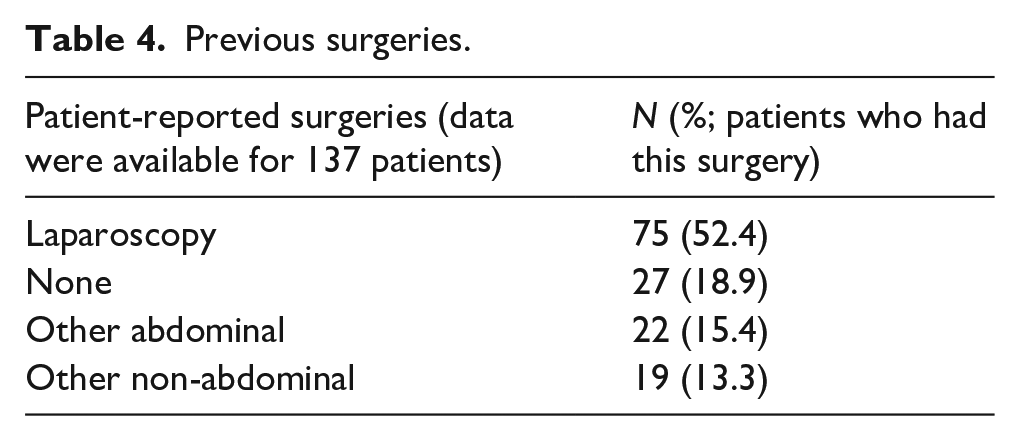
In May 2019, there were 181 patients enrolled in the program and 143 complete questionnaires were obtained (see Figure 1). Patient demographic characteristics are listed in Table 1, with information on reported co-morbid conditions reported in Table 2, reported medications in Table 3, and reported previous surgeries in Table 4.
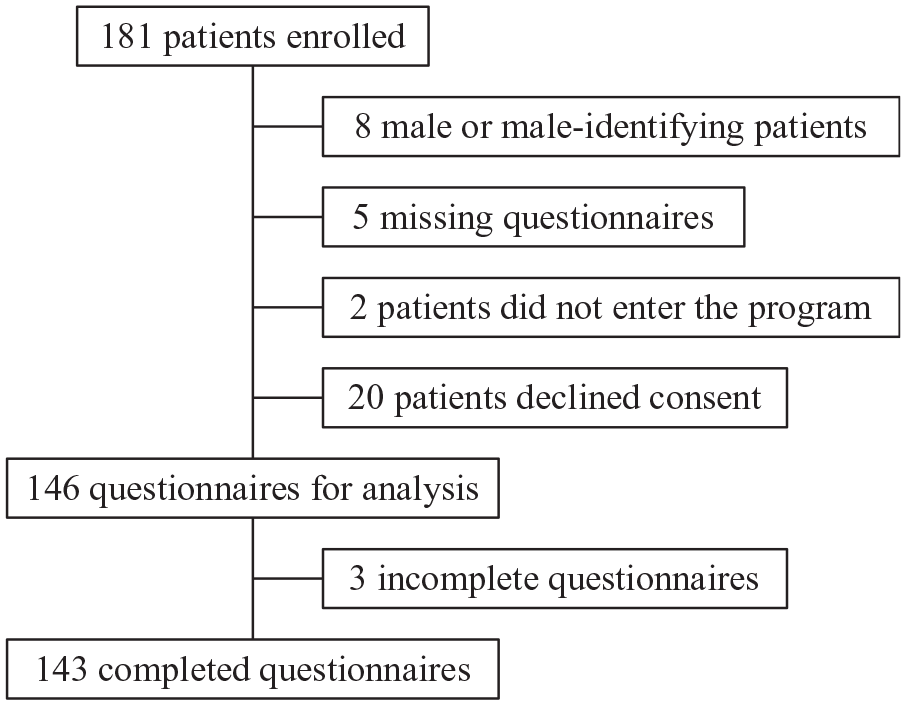
Inclusion and exclusion criteria.
Demographics.
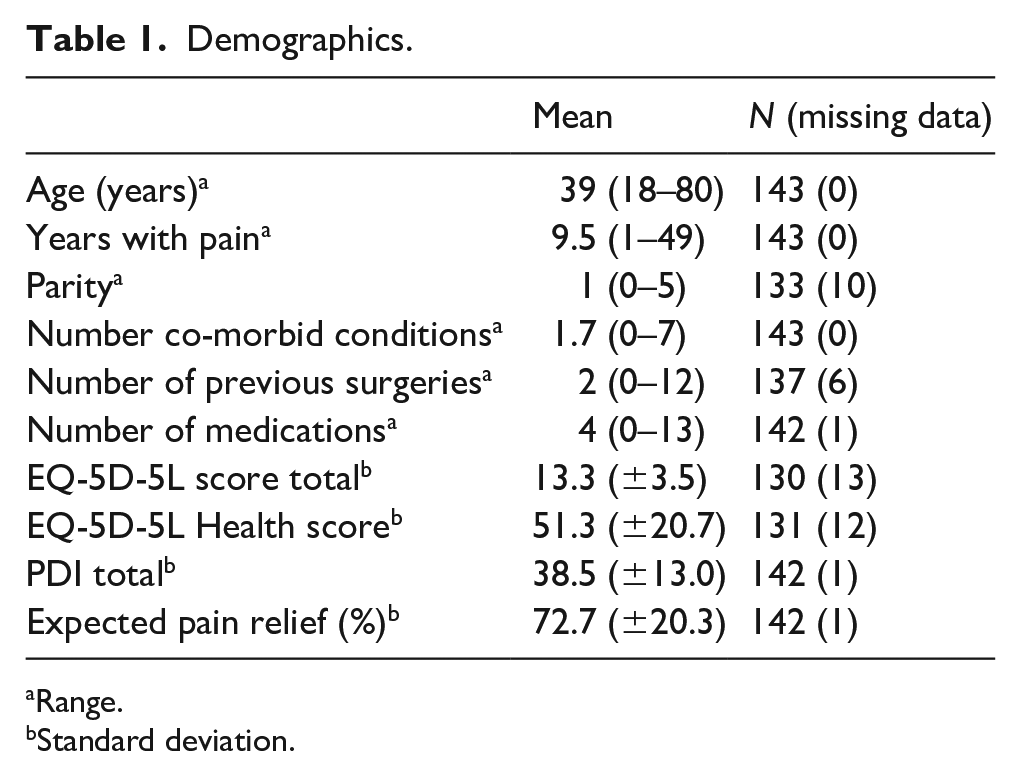
Range.
Standard deviation.
Co-morbid conditions.
Medications reported.
Previous surgeries.
Income source
Data were available for 140 patients.
The top three sources of patient income were: personal employment (n = 83, 59%), spouse income (n = 24, 17%), and Alberta Works (n = 9, 6.4%). Alberta Works provides income support and job training for low income or unemployed Albertans. 19
Diagnoses that patients felt were the cause of their pelvic pain
Data were available for 146 patients (Table 5). One patient did not answer this question. Forty-eight patients (33%) listed only one condition, 61 (42%) listed two, and 36 (25%) listed three or more perceived causes for their pain. Sixty-seven percent of participants identified more than one cause for their pain.
Conditions reported as cause of pain (all rankings).
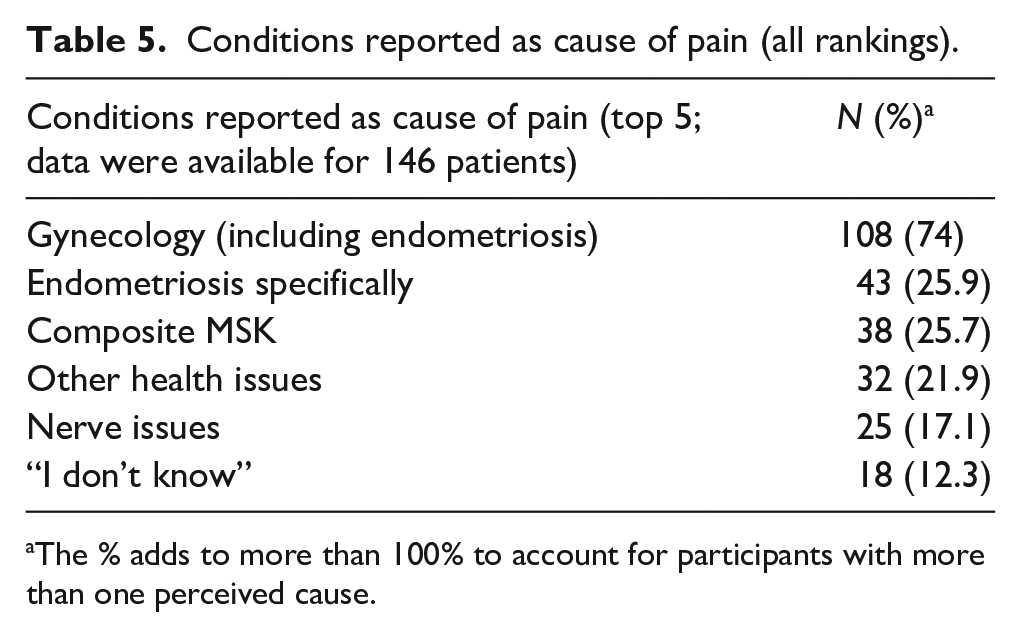
The % adds to more than 100% to account for participants with more than one perceived cause.
When ranked as the first condition (n = 145), the most common diagnosis was gynecologic conditions (41% (n = 59), of which 23% (n = 34) said endometriosis, followed by musculoskeletal (MSK) conditions (n = 15, 10%) and “I don’t know” (n = 14, 10%). The remaining conditions were diverse. The second ranked conditions answered by 97 women included: gynecologic conditions (n = 34, 35%), followed by musculoskeletal (n = 16, 17%), and then other health conditions (n = 12, 12%).
Considering a comprehensive biopsychosocial model of pain, only 14 of 146 (9.6%) considered a non-biomedical cause for their pain compared to 132 of 146 (90.4%) who considered a biomedical cause for their pain. This included: stress/anxiety (n = 6), neurological causes (central sensitization, “firing too often”, referred pain; n = 4), psychological factors (n = 2), fear (n = 1), and abuse (n = 1). In consideration of adding “nerve pain”, this would include another 17 women.
Treatments that patients perceived as beneficial
Data was available for 146 patients (Table 6). Seven patients did not answer this question and were added in the “I do not know” theme. Eighty-two patients listed one treatment (including “I do not know”), 28 listed two treatments, and 36 listed three or more treatments for their pain (56%, 19.2%, and 25% respectively).
Treatments reported as needed for management.
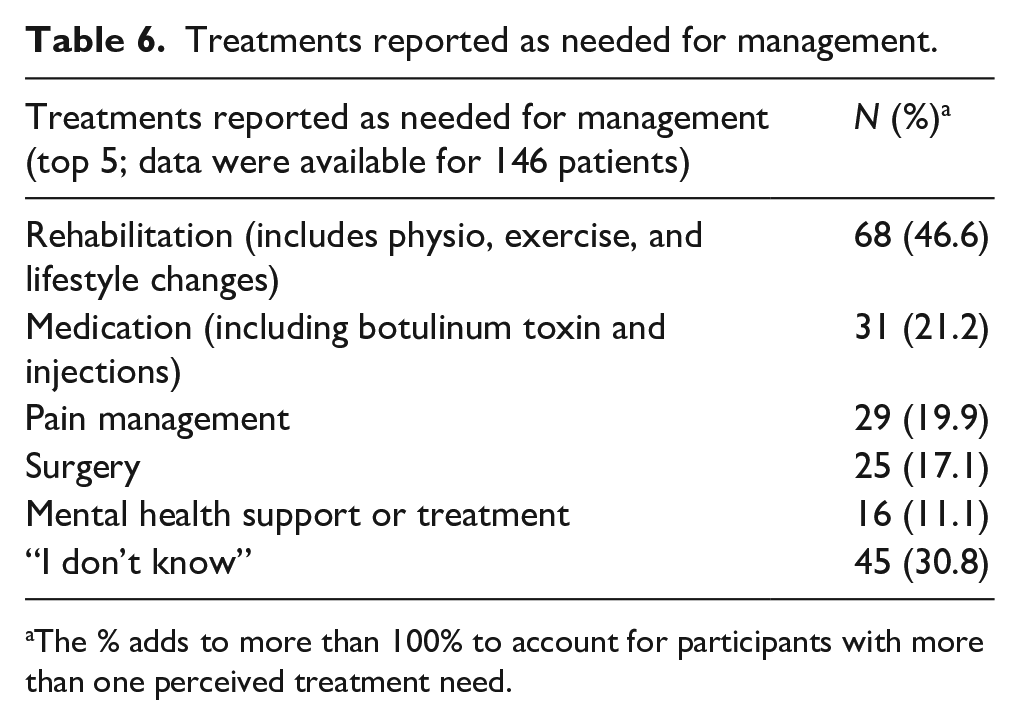
The % adds to more than 100% to account for participants with more than one perceived treatment need.
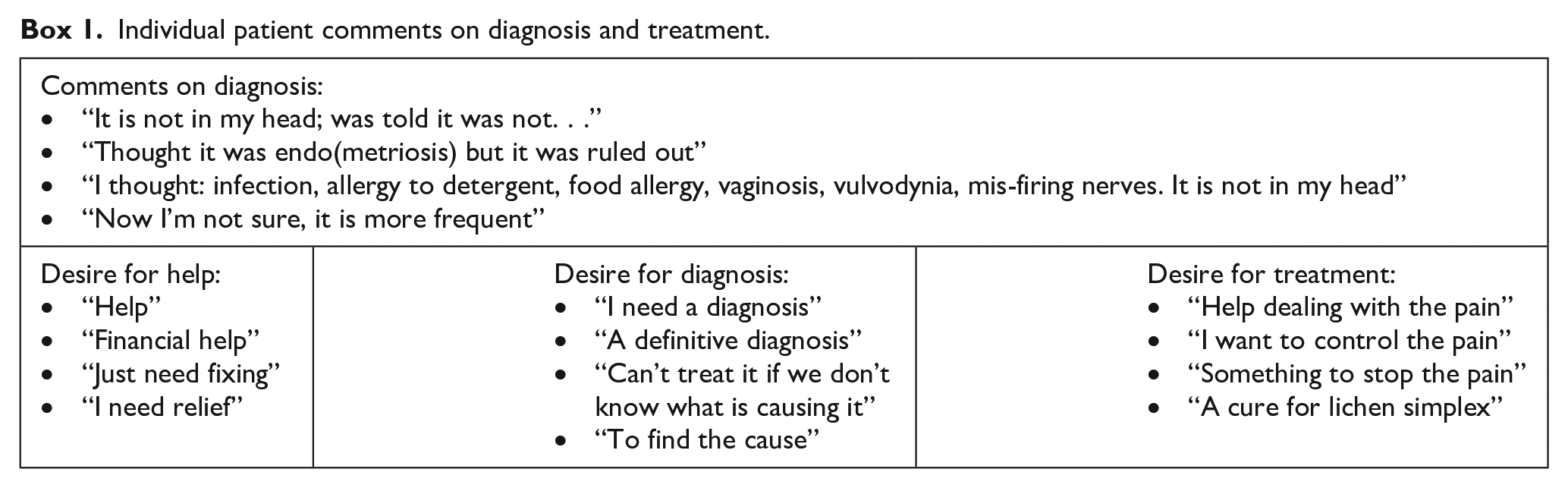
“I don’t know” was the most commonly listed first answer to the question about perceived helpful treatments (n = 45, 30.8%). Individual patient comments on treatment as listed in Box 1.
Individual patient comments on diagnosis and treatment.
Using a biopsychosocial model, 34 comments from 30 individuals (20.5%) included treatments which were considered non-biomedically driven, compared to 116 individuals (79.5%) who felt they required a more biomedical approach. These included: pain management (n = 21), counselling (n = 8), stress management (n = 3), peer support (n = 1), and mindfulness (n = 1). There was no statistical difference between those who identified a biomedical model compared to a biopsychosocial model of their pain with the EQ-5D-5L and PDI results. Similarly, there was no statistical difference between the group who identified a treatment option they felt they needed and the group who did not know what they needed with the results of the EQ-5D-5L or the PDI (p > 0.05).
On average, patients felt that they would need to have a 72% reduction in their pain “to do the things that are most important”, with a range from 0% to 100%. Only one patient thought they needed 0% reduction in their pain, and 23 patients (16.2%) reported needing 100% reduction in their pain to do important things.
Discussion
This study aimed to characterize the expectations and beliefs of patients with chronic pelvic pain about the cause of their pelvic pain and perceived beneficial treatments prior to entering an interdisciplinary chronic pelvic pain program. Entering this program, the average pain duration was 9.5 years and all patients had seen a gynecologist previously. Most women believed they had a gynecologic cause for their pain, specifically endometriosis (29.5% of patients), followed by musculoskeletal causes and other health issues. Twelve percent of women did not know the cause of their pain. Very few women identified psychosocial factors despite a 39% mental health comorbid diagnosis. Many women believed that a rehabilitation program would help treat their pain, followed by medications and pain management. Thirty-one percent of patients reported that they did not know what could help their pain. In keeping with this, a small number of patients (6%) reported wanting further investigations for the cause of their pain because, “can’t treat it if we don’t know what is causing it.” Chronic pain management is based on a biopsychosocial model of pain. Despite this only 20.5% of women felt they needed this approach.
In studies of chronic non-pelvic pain, most patients (15%–32.5%) had no expectations of their visit to a pain clinic prior to attending.8,9 Some of these participants indicated that they could not define their expectations of the pain clinic as they did not know what was offered. 10 However, many patients expected an explanation of their pain, 8 with 18% requesting a diagnosis and 24% wanting some explanation for their condition.9,10 Allcock et al. 8 found that relief of pain was the most significant expectation, and other researchers identified that between 5.2% and 17% of patients were expecting to learn ways of managing their pain.9,10 In a study by Calpin et al., 10 70% of patients expected the formulation of a management plan at the first visit, followed by an assessment of the cause of pain by 50% of respondents. These results are all comparable to our findings in this pelvic pain population. Considering this, it is crucial that health care professionals take time to address patients’ perceptions and understanding of the cause of their pain. Patients may believe their pain has a pathologically serious cause and without clear dialogue between patient and health care professional this can be perpetuated, leaving the patient dissatisfied. 20 Other studies have shown that there are worse outcomes when the patient’s beliefs around their pain have not been addressed, or they feel dismissed.6,7
Sixty-one patients (42%) felt they had multiple causes for their pain, and most reported a combination of gynecologic and MSK conditions as the potential cause for their pain. In keeping with this, 68% of patients believed rehabilitation-type therapies such as physiotherapy, exercise, and lifestyle changes would manage their pain. These therapies are not typically associated with treatment of gynecologic conditions, which are more commonly managed with medications or surgery. Although it may appear incongruent that women felt their cause of pain was mainly gynecological and yet felt that a rehabilitation approach was what they needed, Stratton et al. 21 showed that 94% of women with endometriosis also demonstrated myofascial trigger points, and 87% had central sensitization. Between 50% and 90% of patients attending specialized chronic pelvic pain centers have pain originating from MSK structures. 22 Knowing this, a focus on rehabilitation therapies within the biopsychosocial approach to pain management is congruent with patient expectations of treatment. This reflects the importance of addressing a patient’s beliefs about the cause and treatment of their pain. 23
The theme of uncertainty was recurrent in our findings, as 12% of women were unsure of their diagnosis despite the many treatment modalities and years of pain they had endured. Similarly, 31% of women did not identify a treatment they felt they would benefit from (responded “I don’t know”); this was the most common first answer. Despite uncertainty about the diagnosis and treatment options, 95% of patients were taking pain medications indicating that even with uncertainty they were seeking treatment options. Only 10% considered the psychosocial aspect of their lives as being relevant to their pain, and only 20% of individuals entering this tertiary level, interdisciplinary pelvic pain program identified psychosocial factors as important in their care despite 39% self-reporting mental health conditions. As success in the biopsychosocial approach to chronic pain management hinges on the engagement of the individual, this underscores the importance of education prior to embarking on a treatment pathway. 24
Patients with chronic pain tend to have higher rates of co-morbid mental health conditions.25–29 In this study mental health conditions were the most reported co-morbid condition (39% of patients), yet only 11% of patients felt that any mental health services would be beneficial, and no patients explicitly reported mental health as a cause of their pain. Within the biopsychosocial model, which is well suited to address the complexity of chronic pain, modalities such as cognitive behavioral therapy and mindfulness are established treatment options to address the psychosocial components. 30 Clinicians must be respectful when approaching the impact of mental health with patients. Within our population, two patients explicitly stated, “it is not in my head” when asked about the cause of their pain. Many studies have reported on patient frustration about not being believed or being made to feel “crazy” by health care professionals.31–34 Validating a patient’s symptoms while acknowledging the impact of the psychosocial component of pain perception and its role in wholistic pain management is critical.31,32
This study provides a foundation for a program of future research, particularly looking at the connection between patient beliefs at intake and their outcomes at the end of an interdisciplinary pain program. Of interest would be to examine patient-specific priorities and outcomes, with a focus on how to individualize treatment based on patient diagnosis and beliefs about the cause and treatment for their pelvic pain. Exploring the patient perspective behind the uncertainty between cause of pain and necessary treatment could help close the gap between “ideal” and “realistic” goals for a chronic pain program. This study highlights the importance of patient education about how to manage their pain given the number of patients who did not know what could help them, and about the role of mental health in managing chronic pain conditions.
One of the limitations of this study is a lack of comparator group. This precludes drawing any significant conclusions about this population as it differs from patients with other chronic pain conditions, or from the general population. However, to our understanding it represents one of the largest sample of patients attending an interdisciplinary pelvic pain program to date. Further, this study only assesses these topics at intake into the program without any information about perceptions or outcomes during or after completing treatment within the program. We anticipate building on these results to draw more robust conclusions and further characterize this understudied population. Additionally, all patients were seen by a gynecologist prior to referral and as such, they would have had assessment and management of formally diagnosed gynecologic causes of pain. Only if their pain had persisted would they be referred to the pain center. This could explain the discrepancy between a rehabilitation-focus for treatment which is not commonly associated with gynecologic conditions, as they would have already been offered medications or surgery as first line treatment. This may limit the applicability of this data to patients who are directly referred to pelvic pain programs without first being seen by a gynecologist, and skew the population studied towards those who have not found benefit with traditional therapy for gynecologic conditions. Finally, the ranking for diagnosis and treatment was not standardized and so we have assumed patients wrote their answers in order of importance when they may have just listed them in random fashion.
Conclusion
In this study, most women who present to an interdisciplinary chronic pelvic pain program can identify a perceived cause for their pain, and 74% believed their pain was gynecologic in origin while 12.5 % did not know. In contrast, there was high levels of uncertainty about what treatments would help their pain with 31% responding “I don’t know.” Few women identified a biopsychosocial approach to their pain management. This highlights the importance of establishing a patient-provider relationship to address these beliefs, ensure the patients feel involved and respected in their care, and provide education about the biopsychosocial approach to pain management. Engaging patients and understanding their perspectives on the cause and treatment for their pain will ideally lead to improved function and quality of life.
Footnotes
Data availability statement
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.