
Abstract
Background:
Endosalpingiosis is an understudied gynaecological condition with limited knowledge of its prevalence and clinical significance.
Methods:
We report two rare cases of severe endosalpingiosis aged 25 and 30 highlighting their clinical, laparoscopic and histological features, as well as treatment outcomes.
Results:
Both cases presented with severe and intractable chronic pelvic pain (CPP) with a pattern like endometriosis pain. Initially, they received standard medical management for CPP, including hormonal therapy and pain modulators, with limited or no improvement. They were then offered laparoscopy, which revealed widely spread superficial vesicular lesions on ovaries, pelvic peritoneum, uterus and bowel. Wide excision of affected peritoneum was performed, and multiple biopsies were obtained from ovarian lesions. Histology revealed endosalpingiosis in both cases. In case 2, histology also revealed a neuroendocrine tumour, which was likely from a gastrointestinal (GI) primary malignancy. This case was referred to the GI team for further management. In both cases, surgery resulted in 6-month relief of pelvic pain followed by gradual recurrence of severe symptoms.
Conclusion:
These cases highlight the clinical dilemma of severe endosalpingiosis, which appears to be associated with intractable pain that is resistant to all standard hormonal and surgical treatments. Whether the association with the neuroendocrine tumour in the second case was incidental or a true link remains uncertain. Further research is required to identify effective treatment strategies for ES.
Introduction
Endosalpingiosis (ES) refers to the presence of ectopic tubal-type ciliated glandular epithelium outside the fallopian tubes. 1 Histologically, ES can be distinguished from endometriosis (EM) by the presence of ciliated glandular epithelium and the absence of endometrial stromal component. Furthermore, unlike EM, ES is not associated with an inflammatory response. It usually affects ovarian surface, pelvic peritoneum (including pelvic sidewalls, pouch of Douglas and uterovesical fold), and the serosal surfaces of pelvic organs including fallopian tubes, uterus, bowel and bladder. 1
ES is traditionally viewed as an incidental and insignificant finding in histological specimens obtained during endometriosis or other pelvic surgery. This has led to a lack of interest in this condition, which has remained largely understudied. To date, very little is known about its prevalence, epidemiology and clinical significance owing to scarcity of its documentation in the literature.
Ries 2 was the first to recognise peritoneal Müllerian inclusions in 1897. The term ‘endosalpingiosis’ was first introduced by Sampson 3 in 1930 who described the local proliferative and invasive properties of tubal mucosa following surgical interruption.
The pathogenesis of endosalpingiosis remains largely uncertain. Currently, there are three main theories including, shedding of epithelia from the tubes into the pelvic peritoneum, coelomic metaplasia of pelvic peritoneal epithelium and growth of vestigial embryonic Müllerian tissue, misplaced during Müllerian migration during embryogenesis (a process called Müllerianosis). 1 Other possible mechanisms include transplantation of tubal mucosa to peritoneal surfaces during tubal surgery and lymphatic vascular metastasis of tubal mucosal cells. 4
Although both endometriosis and endosalpingiosis are derived from the Müllerian system and are frequently seen together, each condition is considered an independent clinical and pathological entity with different demographics. 5 The clinical presentation and features of ES are controversial. Although many studies reported an association with chronic pelvic pain,4,6–9 few reports found no association.5,8,10 However, it is widely believed that ES is often asymptomatic, and is only painful when associated with endometriosis. 4 Other reported symptoms include infertility, pelvic mass and urinary symptoms.
Like endometriosis, laparoscopy remains the main diagnostic tool that allows visualisation of endosalpingiosis lesions. However, ES is generally not recognisable by gynaecologists at the time of laparoscopy and is often misdiagnosed as endometriosis. The definitive diagnosis is made only by histological examination of surgical biopsies. When visually obvious, ES may appear as multiple white to yellow, translucent to opaque, punctate, fluid-filled cystic lesions.
A key challenge regarding this condition is the difficulty to differentiate it clinically and laparoscopically from endometriosis. Another dilemma encountered with endosalpingiosis is the uncertainty about effective/curative treatment strategy for this condition.
More recently, the presence of ES has been considered more of a concerning finding than previously thought as it could be a possible origin of serous ovarian carcinomas, which are widely believed to originate from tubal or tubal-like serous epithelium. 5 There is emerging evidence supporting a close relationship between ES and the development of serous tumours, especially borderline and low-grade ovarian serous carcinoma.6,7,11–13 Furthermore, Prentice et al. reported that premenopausal women with ES have an increased likelihood of developing a gynaecological malignancy. 5 In addition, ES lesions can undergo massive cystic change resulting in cystic endosalpingiosis, which could mimic serous tumours. There have also been associations between ES and primary papillary peritoneal neoplasia of low malignant potential and less commonly cystadenocarcinomas.14,15
Although several case reports have previously been published, the purpose of this report was to present two challenging cases of extreme endosalpingiosis highlighting their clinical presentation, laparoscopic and histological features in addition to treatment outcomes and prognosis.
Case reports
Case 1
This is a 25-year-old nulliparous lady presenting with a long-standing history of severe chronic pelvic pain, which has not been responsive to all forms of pain management or hormonal therapies including combined oral contraceptives (COC), Progestogen only contraceptives (minipill and Mirena coil) and GnRH analogues. Her pain was worsening with recurrent acute exacerbations requiring repeated emergency admissions. She denied any history of sexually transmitted infection (STI) and genital swabs have been reported as negative. An ultrasound scan did not show any abnormality. She was therefore offered a laparoscopy to assess and treat any possible pain associated pelvic pathology such as endometriosis.
Laparoscopy revealed extensive pelvic adhesions involving sigmoid, pelvic sidewalls and both ovaries, which were tethered to ovarian fossae. Both ovaries were extensively covered with 2–3 mm vesicles/nodules. Similar lesions were also present on the pelvic sidewalls bilaterally (Figure 1). Extensive adhesiolysis was performed followed by bilateral ovarian suspension to the ipsilateral round ligaments. This was followed by bilateral ureterolysis with excision of pelvic side wall peritoneum removing all lesions on both sides. Multiple vesicles/nodules were excised from the surfaces of both ovaries, but complete excision of ovarian lesions was not possible.
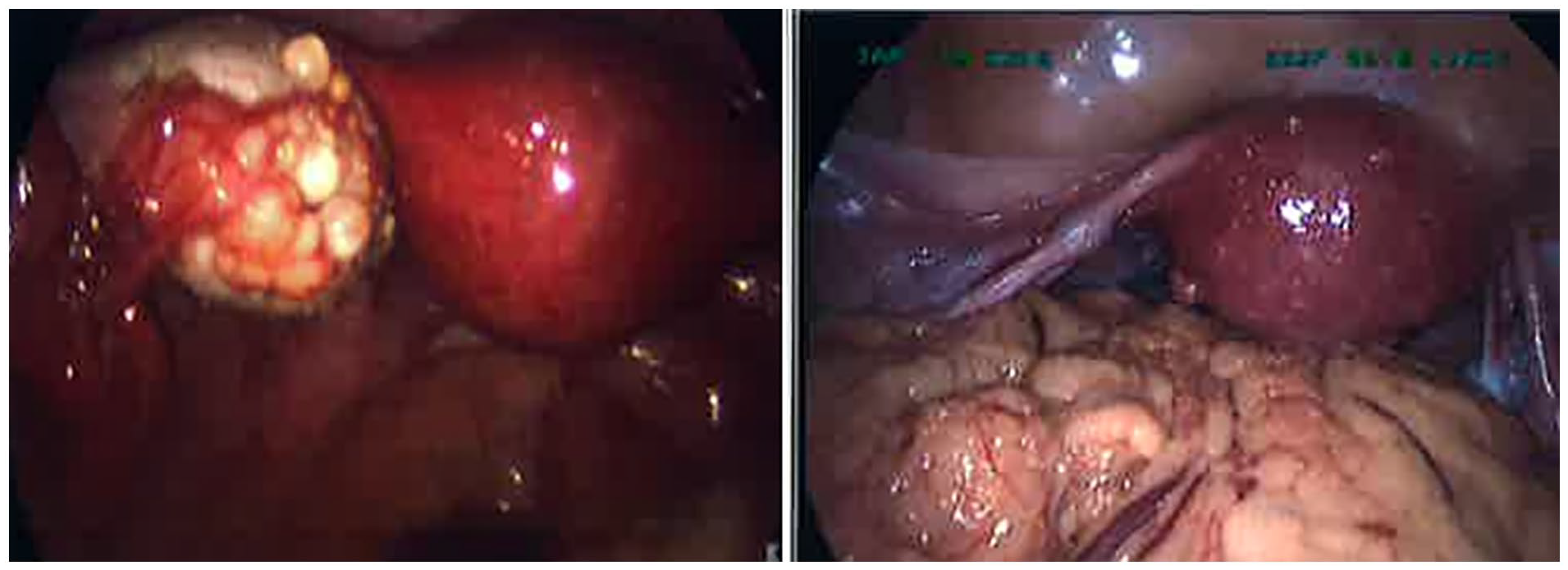
Case 1, laparoscopy appearance of endosalpingiosis showing wide spread vesicles/nodules on left ovary and uterus.
Histological examination of the pelvic sidewall peritoneal lesions showed endosalpingiosis characterised by the presence of glands lined by tubal type ciliated epithelial cells (Figure 2). Ovarian biopsies showed three pathological lesions including endosalpingiosis, serous cystadenofibroma and serous inclusion cysts. There were no atypical or malignant features in any of the biopsies.
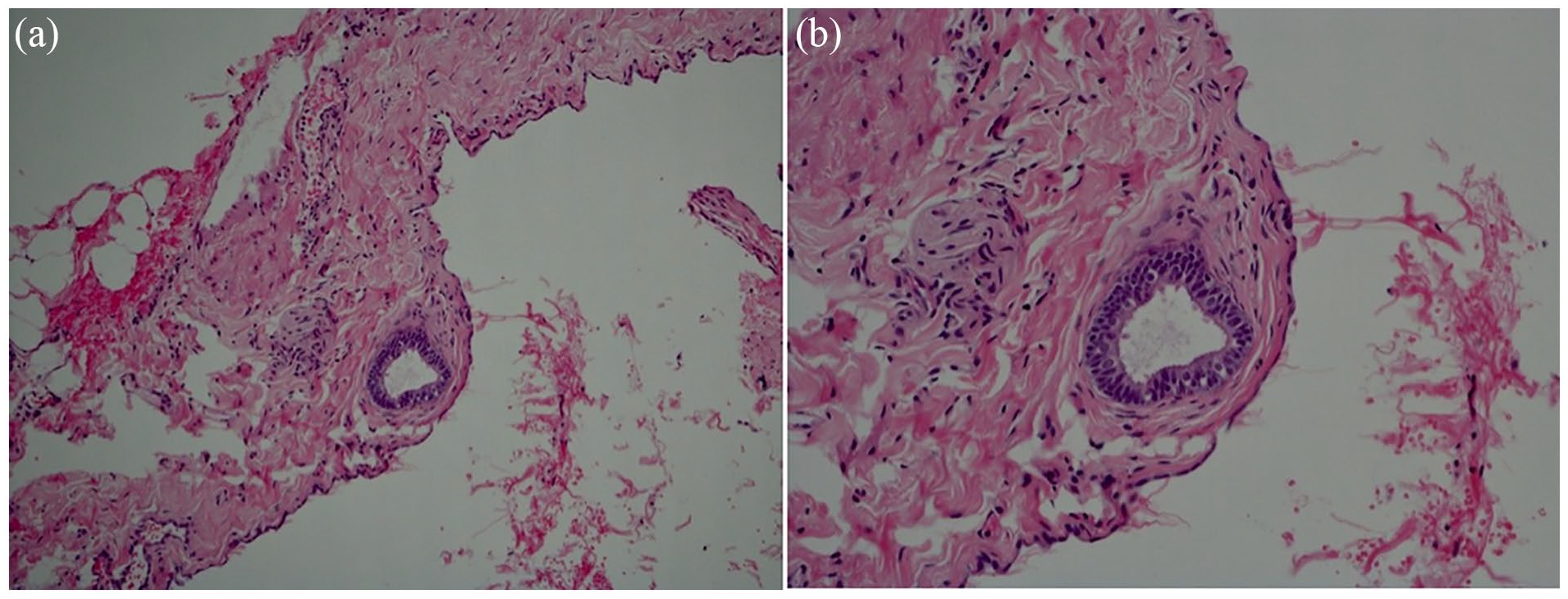
Case 1, histological appearance of peritoneal endosalpingiosis showing a gland lined by tubal type ciliated epithelial cells: (a) low magnification and (b) high magnification.
Following surgery, the patient reported marked improvement of her pelvic pain, which lasted for about 6 months. She then gradually started to experience recurrence of worsening pelvic pain leading to severe flare-ups requiring repeated hospital admissions for pain management. Unfortunately, all hormonal and non-hormonal therapies described above failed to alleviate her intractable pains.
Eventually, she underwent a second laparoscopy 15 months after her first procedure. As her worst pain was focused on the right iliac fossa and the right ovary was known to have worst disease from the first laparoscopy, she was counselled for excision of the right ovary. She had already decided not to have any children long before her suffering and this decision was not related to her symptoms. Laparoscopy revealed similar findings to the first laparoscopy, with more extensive vesicles/nodules on the right ovary with marked periovarian adhesions. Adhesiolysis was performed with complete mobilisation of ovaries followed by right salpingo-oophorectomy and excision of pelvic sidewall peritoneal disease.
Following surgery, her right sided pain has completely disappeared and the overall pelvic pain has significantly improved. Unfortunately, several months later, the severe pelvic pain recurred, but her right sided pain remained very mild. She was referred to the pain clinic for further management.
Case 2
This is a 30-year-old nulliparous lady who presented with a long-standing history of chronic pelvic pain with a pattern highly suggestive of endometriosis. Her pains included dysmenorrhoea, dyspareunia and non-cyclical pelvic pain. She has also been troubled with menorrhagia. She denied any past history of STI, and her genital swaps were clear of any infection. She had a background medical history of fibromyalgia, asthma and rheumatoid arthritis.
An ultrasound scan was unremarkable, apart from a 5 mm well defined echogenic area on the right ovary suggestive of endometriosis. Like case number 1, she was initially managed with all standard pain modulators and hormonal treatments, which are usually offered to women with presumed endometriosis as mentioned above. None of these was effective in relieving her pains. Although she initially responded to GnRH analogue injections, the pain later recurred. She was therefore offered a laparoscopy to assess for and treat possible endometriosis.
Laparoscopic examination of the pelvis revealed widely spread clusters of 2–3 mm nodules/vesicles on the uterus, bladder, ovaries, pelvic peritoneum and bowels in addition to a small right ovarian cyst (Figure 3). Right ovarian cystectomy was performed followed by bilateral ureterolysis with wide excision of pelvic side wall peritoneum removing all lesions on both sides. Multiple vesicles/nodules were excised from the surfaces of both ovaries, but complete excision of ovarian lesions was not possible.
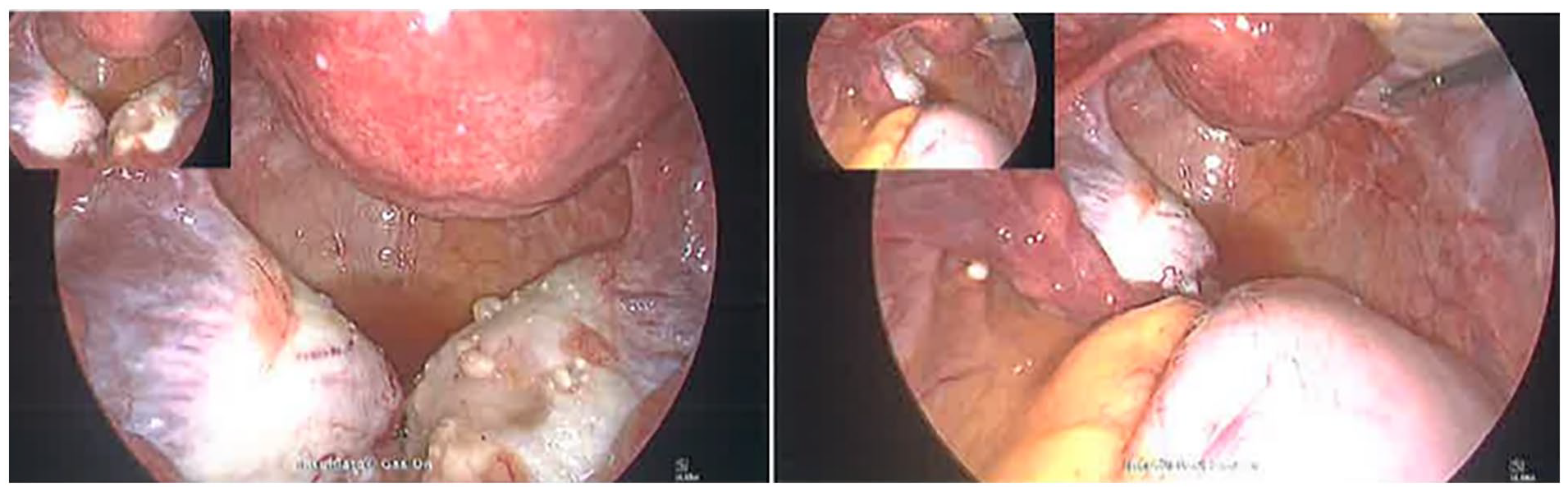
Case 2, laparoscopic appearance of endosalpingiosis showing wide spread vesicles/nodules on ovaries and uterus.
Histological examination of the specimens removed during surgery revealed four pathological entities including: (1) Endosalpingiosis in all peritoneal biopsies from pelvic sidewalls, pouch of Douglas, and utero-vesical fold, (2) metastatic well-differentiated grade 1 neuroendocrine tumour (likely of gastrointestinal (GI) primary) in all peritoneal biopsies, (3) right para-ovarian benign serous cystadenoma with a small deposit of a well-differentiated neuroendocrine tumour and (4) subserosal leiomyoma from the surface of the uterus.
Following surgery and on receipt of the histology report, the patient was given an urgent appointment to explain the results. She was then referred to the Gynae-oncology MDT for further management in liaison with oncology and gastroenterology teams. Computed Tomography of thorax, abdomen and pelvis with contrast revealed a 3 cm enhancing mass arising from the appendix, which was highly suspicious of primary neuroendocrine tumour. There were also prominent right subpectoral nodes of uncertain significance. She was referred to the GI team with the relevant expertise in managing Neuroendocrine tumour. After full clinical assessment, she underwent total colectomy. She later returned to gynaecology clinic and was still experiencing significant pelvic pain. This has been treated with progestogen only contraceptive pill and she still awaits a follow up appointment for further management.
Discussion
In this report, we present two cases of relatively severe ES presenting with severe endometriosis-like manifestations. Laparoscopically, ES was widely spread in the pelvic area covering almost all organs. The main laparoscopic lesions included small superficial vesicular and nodular lesions affecting the pelvic peritoneum as well as the surfaces of almost all organs especially the ovaries. Whilst wide excision of the affected peritoneum was possible, it was not feasible to excise the lesions completely from the surfaces of the ovaries, uterus or bowel.
Histologically, ES was the main pathology in both cases with no associated endometriosis that could contribute to the extreme pelvic pain. It is therefore possible to conclude that ES was the sole cause for the severe pelvic pain in these women.
Endosalpingiosis and chronic pelvic pain
Although, the association between ES and pelvic pain has been the subject of much debate in the literature as detailed in the introduction, our first case demonstrates clearly that severe ES was the only pathology that could explain the pelvic pain. It is therefore possible to hypothesise that whilst the incidentally found mild ES may not cause pain, severe ES seems to be associated with extreme and intractable pelvic pain. However, in the absence of any inflammation associated with ES, the mechanism of ES-associated pain remains uncertain. Furthermore, our second case also had neuroendocrine tumour concomitant with the ES, which may also be a possible cause for her pain. However, her pain continued after surgical eradication of the tumour.
It was also notable that the severe ES-associated pain did not respond to all forms of hormonal therapeutics used in endometriosis including first line (contraceptive pills) or the second line (Norethisterone or GnRHa). It is not clear as to why ES related pain in these cases did not respond to hormonal suppressive therapy although it is well established that tubal glandular epithelium is responsive to oestrogen and progesterone. 16 This is similar to some cases of endometriosis, which are refractory to hormonal suppressive therapy with no clear explanation. It is possible that the main cause of the pain in our cases was the extensive adhesions, which may not be responsive to hormones. Further research is needed to investigate the underlying pain mechanisms and efficacy of hormonal therapy in ES. Laparoscopic surgery seems to provide a temporary relief that could last for about 6 months. The main limitation of surgery is the inability to achieve a complete excision of the widely spread ES lesions as explained above. Therefore, there is a need for further research to identify more effective treatment for supressing or eradicating ES with effective relieve of its associated pelvic pain.
Endosalpingiosis and malignancy
Our second case was associated with neuroendocrine carcinoma with the bowel being the possible primary source. This finding supports the notion that ES is associated with various types of malignancy. This is consistent with several literature case reports and case series. A 5-year retrospective study by Prentice et al. 5 including 110 ES cases (72 with no concomitant endometriosis) showed that premenopausal women with ES were 10 times more likely to develop gynaecological malignancy when compared with women without ES. Another larger retrospective study by Esselen et al. 12 including 838 ES cases reported concurrent gynaecological malignancy in the histological specimens of 42% of cases. The types of malignancies were cervical (3.8%), uterine (17.7%) and ovarian, tubal or peritoneal (21%). It is therefore important to consider these potential associations when counselling patients with ES diagnosed at the time of Gynaecological surgery. It may be recommended that these women should have some sort of surveillance. Further studies are required to identify possible histological features that are associated with increased risk of malignancy in women with a histological diagnosis of ES.
Conclusion
Our two reported cases raise the awareness of endosalpingiosis as an independent pathological entity both clinically and pathologically. Severe ES seems to be associated with severe endometriosis-like symptoms with intractable pelvic pain. The common laparoscopic lesions are small vesicles or nodules that are widely spread on serosal and peritoneal surfaces. The second case highlighted the significant risk of malignancy in women with ES that should be carefully considered when counselling these women. Further research is needed to identify effective treatment strategies for ES.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.