
Abstract
Teeth with molar-incisor hypomineralization (MIH) present demarcated opacities, which are structural alterations in the enamel, making them more porous and often resulting in dentin hypersensitivity (DH). New technologies have been developed for the management of MIH-affected teeth, including bioactive silicon materials, which could form new silicon-enriched hydroxyapatite crystals, reinforcing the structure, and acting as an obliterating agent. The aim of this study was to evaluate the formation of a mineral layer and changes in the demarcated opacities’ color employing an intraoral Trios 4 scanner after using a new silicon-based bioactive clinical system plus calcium in 11 children with MIH. DH was assessed with the VAS and SCASS scales at baseline, 15, and 30 days. Intraoral scanning revealed the formation of a mineral layer after 30 days, and significant DH reduction was observed (mean reductions: VAS 65% at 15 days and 83% at 30 days; SCASS 76% at 15 days and 94% at 30 days). Moreover, Cox regression analysis identified baseline pain severity as an independent predictor of a faster reduction in DH (adjusted HR = 0.06, p < 0.05). Color analysis suggested a lightening of the demarcated opacities. These results indicate that the new silicon-based bioactive clinical system plus calcium may effectively reduce DH and modify both enamel structure and opacity coloration in MIH-affected teeth. Longitudinal studies with larger samples are needed to assess the long-term effects.
Keywords
Introduction
Molar-incisor hypomineralization (MIH) is defined as a qualitative developmental defect of enamel that affects at least one permanent first molar and may or may not affect incisors. 1 Clinically, MIH is characterized by demarcated opacities that vary from white-cream to yellow-brown and affect teeth asymmetrically.2,3
Due to the presence of lower mineral content and higher organic content in its composition, the affected teeth is fragile, porous, more susceptible to dentin hypersensitivity (DH), and painful in the presence of thermal stimuli, such as cold or hot drinks, or mechanical stimuli, such as brushing,4,5 a condition that can affect patients’ oral health-related quality of life (OHRQoL). 6 This occurs because dentin pain is a subjective condition that has a negative impact on daily habits such as chewing, oral hygiene, physical disposition, and communication ability and can generate fear and anxiety during dental appointments. 3
Given this scenario, there is a need to search for technologies that can assist in the management of DH in patients with MIH. Various dental materials and technologies have been described in the literature as attempts to manage DH,7–10 with a focus on promising bioactive silicon technologies. 11
Among them, the REFIX technology stands out, a bioactive complex of phosphates, silica, and fluoride that, when present in the oral environment, forms a mineral layer containing silicon-enriched hydroxyapatite.12,13 This layer acts as an obliterating agent and assists in the management of DH.14–16 Also, when REFIX is combined with a calcium booster, this system can form an immediate smooth mineral layer similar to enamel,17,18 with positive protection results against DH since first use.16,19
Another in vitro study demonstrated REFIX technology’s ability to form a new mineral layer with a thickness that can vary between 3 and 60 μm20 In this sense, evaluating the formation of the silicon-enriched mineral layer in a clinical setting becomes a challenge because the layer formed is micrometers thick and therefore difficult to visualize and measure. However, intraoral scanners and digital dentistry indicate new possibilities for diagnosis, with tools to evaluate the variation in enamel porosity through the comparison of scans as a result of specific treatments.
The Trios 4 scanner (3Shape, Denmark) is an option because it has an accuracy of 6.9 ± 0.9 μm and is able to perceive small changes between the patient’s intraoral scans through its software’s monitoring tool (App Monitoring, 3Shape, Denmark), which allows for the comparison of scans performed at different times from the superposition of the meshes. The tool also allows for transverse cuts in 3D models to evaluate the dental structure at the times when the scanner was used on the patient. 21 The Trios 4 intraoral scanner (3Shape, Denmark) also allows for the assessment of changes in color perception between scans using the color measurement tool embedded in its software, allowing for the evaluation of potential color alterations before and after treatments. 22
In view of the above, this preliminary study was conducted to evaluate, through the longitudinal comparison of images obtained by intraoral scanning, the possibility of identifying the formation of the layer created by the REFIX technology and to evaluate the alterations in DH.
The primary objective of this preliminary study was to evaluate whether an intraoral scanner is capable of identifying changes in the dental structure’s thickness through cross-sectional cuts of 3D models suggestive of the formation of a silicon-rich mineral layer. Secondary objectives include testing the effectiveness of the REFIX technology implemented in toothpastes for reducing dentin hypersensitivity in children with MIH and comparing the perceived color of demarcated opacities in affected teeth before and after treatment with this technology using intraoral scanner software.
Material and methods
The Research Ethics Committee of the Faculty of Dentistry, University of São Paulo (FO-USP) approved this project under registration CAAE: 79258224.0.0000.0075.
Participants undergoing treatment at the Enamel Defects Clinic of the Pediatric Dentistry Department of FO-USP of both sexes aged between 5 and 18 years with a diagnosis of MIH and complaining of DH in at least one affected tooth were considered for inclusion. A score equal or greater than 1 was required in at least one affected tooth on the VAS and SCASS scales used for HD assessment to be included in the study.
Patients with systemic diseases, with semi-erupted hypomineralized teeth, with carious lesions with pulpal involvement, using orthodontic appliances or bands, or who had used desensitizing toothpastes in the last 3 months were excluded.
MIH diagnosis
Trained and calibrated researchers made the diagnosis of MIH with an intra- and inter-examiner kappa agreement index greater than 0.8, demonstrating satisfactory agreement among the researchers. The diagnosis of MIH was made based on the Ghanim index, 23 and cases were categorized based on the defect’s severity (mild, moderate, and severe). 24 Teeth with demarcated opacities larger than 1 mm and without requiring additional treatments or interventions were considered.
Thickness change assessment
To evaluate thickness changes, the intraoral scanner’s App Monitoring tool (3Shape, Denmark) was used, which allowed for the comparison of scans from the same patient before and 30 days after use of the tested technology. This comparison is performed on sagittal cuts of the obtained 3D models.
DH evaluation and sensitivity to cold-air jet
After the diagnosis of MIH, the presence of DH was assessed. One trained and calibrated specialist determined the diagnosis of HD using the Visual Analog Scale (VAS) and the Schiff Cold Air Sensitivity Scale (SCASS). The affected teeth were dried with an air syringe to determine sensitivity to the stimulus. The air stream was applied for 1 s at a distance of 1 cm and perpendicular to the surface of the affected teeth. Neighboring teeth were protected with cotton rolls.
The SCASS classification 25 was used, which indicates the professional’s perception of the patient’s response to the stimulus—scores range from 0 to 3; higher scores indicate sensitivity to the stimulus—and the VAS scale, 26 which indicates the patient’s perception of the stimulus—scores range from 0 to 10; higher scores indicate greater sensitivity. Only participants with scores equal to or greater than 1 on both scales were included.
Demarcated opacities color perception
The perception of color alteration was measured using the 3Shape intraoral scanner’s tone measurement tool (Color System, Denmark), which allows for the comparison of scans and their color changes. The color is measured automatically during scanning with the aid of the fluorescence tool, combining the color information recorded in 3D images obtained from multiple angles. The final color is translated in the present experiment to the Vita Classic and Vita 3D-Master shade systems, selecting the most corresponding shade. 22
The scanner constantly calibrated the tips (gray scale and color) for proper use of the tools, and the scanning was performed with the reflector lights off to avoid interference in color perception, as indicated by the manufacturer.
Study participants
After the diagnosis of MIH and assessment of DH, 11 participants were included. All participants’ guardians were invited to complete a questionnaire containing socioeconomic, demographic, and environmental factors related to MIH as well as other important information about the patient’s medical-dental history.
The terms of consent and free and informed assent were completed prior to the start of the study. The included participants’ characteristics are shown in Table 1.
Subject’s characteristics.

N/A: not applicable.
The flowchart illustrating the study methodology is presented in Figure 1.
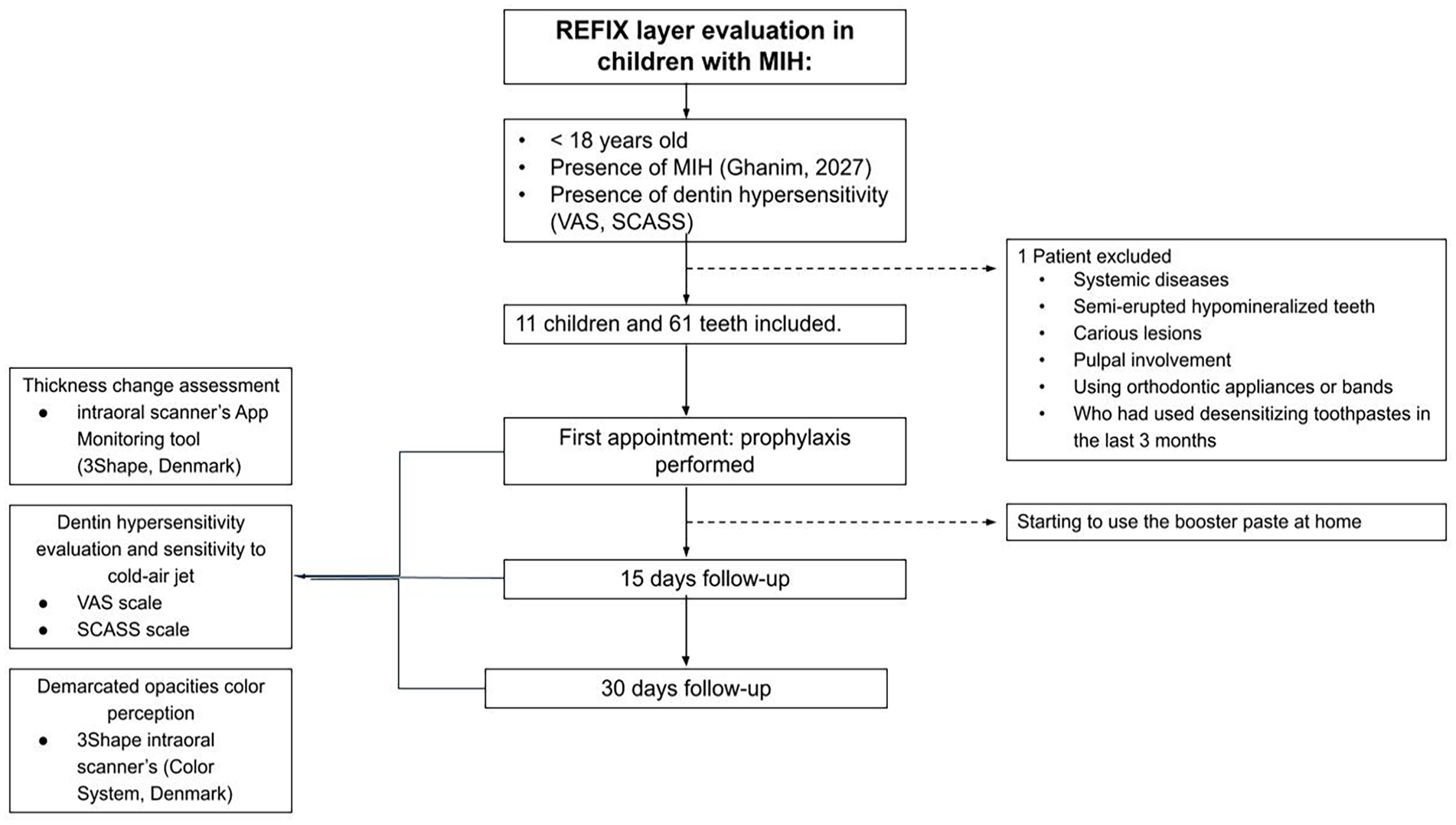
Participants inclusion flowchart.
Interventions and longitudinal evaluation
Baseline
With the patients seated in the dental chair, the initial assessments at baseline were intraoral scanning with the Trios 4 scanner (3Shape, Denmark) and then the assessment of DH with the aid of the air syringe through the SCASS classification and the VAS scale.
Immediately afterward, professional prophylaxis was performed using a new silicon-based bioactive clinical system plus calcium known as the REFIX Booster System (Dentalclean, Brazil; Si-Ca System), which consists of two tubes containing different dental gels: a crystallizer (bioactive silicon dental gel) and an accelerator (calcium dental gel). Following the manufacturer’s instructions, small amounts of each of the gels were placed and mixed in a prophylaxis cup. The application was done with a prophylaxis brush, and after 1 min in contact with all teeth, low-speed activation was performed, maintaining prophylaxis for 1 min on the MIH-affected teeth. After prophylaxis, the participants received a soft children’s toothbrush, the Si-Ca System, and a leaflet with instructions for use.
Participants and their guardians were instructed to continue treatment at home for 1 month by brushing their teeth at least twice a day with the kit brush and the Si-Ca System. The use of the SI-CA System involved the following instructions: a pea-sized amount of the crystallizer dental gel and the same amount of the accelerator dental gel should be placed directly on the toothbrush and left to activate for 1 min. Then, brushing could be performed normally for at least 1 min.
Follow-ups 15 and 30 days after the first intervention
At each follow-up, DH was assessed using the SCASS classification and the VAS scale, followed by a new intervention with the performance of professional prophylaxis with the Si-Ca System as described at baseline.
Intraoral scanning was repeated only at the last follow-up (30 days after the first intervention).
Throughout the study period, patients did not undergo any restorative treatment and only used the gels the researchers indicated to avoid influencing the results.
Data analysis
All data collected was tabulated in an Excel spreadsheet. Descriptive analyses of the sociodemographic and clinical variables of the sample were conducted.
The analysis of the reading of the layer formed was conducted using the 3Shape monitoring application (Denmark, Brazil), which allows for the superposition of the meshes of the two scans (baseline and 30 days) and the performance of cross-sectional cuts in specific teeth to verify superficial alterations. Images of the cross-sections were recorded and compared.
The variation in dentin hypersensitivity was evaluated through descriptive analysis of the means and standard deviations of the values obtained using the SCASS classification (Schiff Cold Air Sensitivity Scale) and the VAS scale (Visual Analog Scale) at three time points: baseline, after 15 days, and after 30 days. Percentage reductions were calculated for each evaluation point.
To investigate the association between categorical variables—age (⩽12 years or > 12 years), gender (male or female), pain severity (mild, moderate, or severe), and tooth group (incisors or molars)—and the outcomes at different time points (baseline, 15 days, and 30 days), the chi-square test was used. The VAS scale was categorized as mild (score 0–2), moderate (score 3–7), and severe (score 8–10) to facilitate the interpretation of results.
Descriptive analyses of sociodemographic and clinical variables were expressed in absolute and relative frequencies. The change in category on the VAS and SCASS scales over time was analyzed, highlighting the percentage of pain reduction at each time point. To investigate factors associated with the time to categorical pain reduction according to the VAS scale on the 30th day, Cox proportional hazards models were used. The model included only children with a baseline VAS score greater than 0, considering gender, pain severity, age, and tooth group as independent variables. The analyses were conducted using both univariable and multivariable approaches. All statistical analyses considered two-tailed p-values < 0.05 as statistically significant and were performed using Stata software version 15.1 (StataCorp, College Station, TX, USA). 27 The dataset was created in Microsoft Excel version 16.8.
Results
Images obtained from the scan
In Figures 2 and 3, it is possible to compare the images of the teeth’s enamel contours in the initial scans (baseline—blue line) and final scans (after 30 days of treatment—yellow line) by making sagittal cuts of the 3D models obtained using the App Monitoring tool (3Shape, Denmark).

(a and b) Perception of thickness change in the superficial layer of affected incisors. X: Points where no change in thickness was detected, Y: Points where the final thickness was greater, Z: Points where the final thickness was smaller.

(a and b) Perception of thickness change in the superficial layer of affected molars. X: Points where no change in thickness was detected, Y: Points where the final thickness was greater, Z: Points where the final thickness was smaller.
In some regions of all teeth, an overlap of the yellow line over the blue line (X) was observed, demonstrating that there was no difference between the enamel contour at baseline (blue) and the enamel contour after 30 days of treatment (yellow).
However, in other images, a clear difference is noticeable between the baseline image (blue) and the image after 30 days of treatment (yellow), in which the yellow line shows an increase in the tooth contour in relation to the blue line (Y), which indicates an increase in enamel thickness in the final scan, suggestive of the formation of the silicon-enriched layer in these regions (Figures 2 and 3).
There were also points where the yellow line (30 days after treatment) shows a decrease in the tooth contour compared to the blue line (Z); that is, the tooth appears to have a smaller thickness than in the initial scan, which may indicate a possible post-eruptive structure loss, a frequent characteristic of teeth with MIH (Figures 2 and 3).
Although the scanner had the capacity and precision to detect micrometer changes in the dental surface, it was not possible to measure the difference in thickness between the scans because appropriate tools were not found for this function in the software of the intraoral scanner used.
Dentin hypersensitivity evaluation
Descriptive analysis of the variation in dentin hypersensitivity (patient as the unit of analysis)
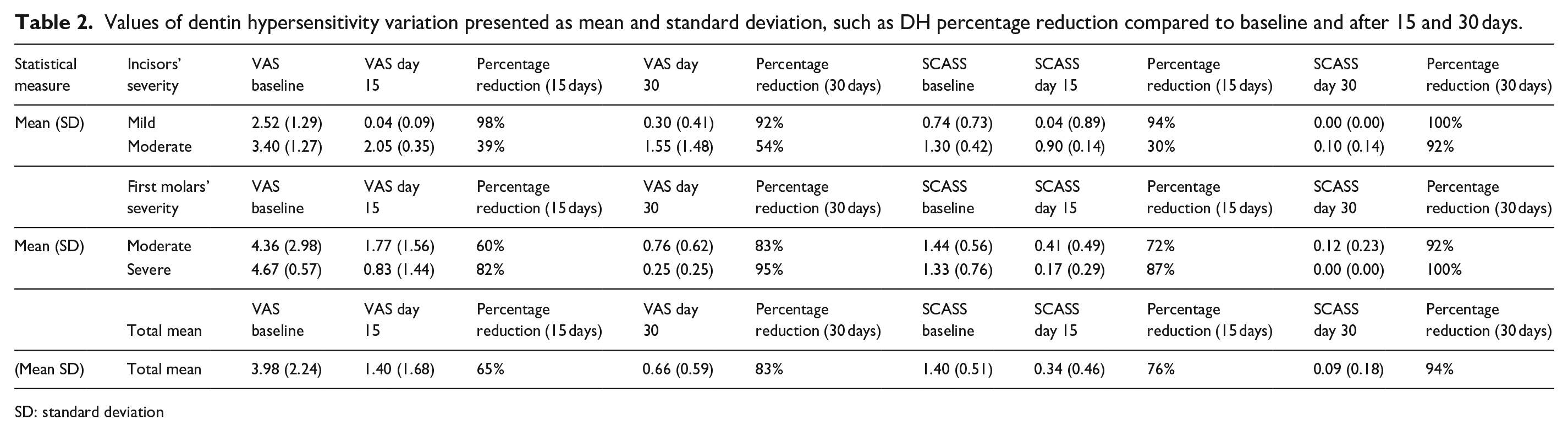
The DH data were tabulated, and the values are presented as mean and standard deviation in a descriptive manner for each of the returns and the outcome measures used. For better analysis, the data were divided based on the condition’s severity and the group of affected teeth (Table 2). The individual mean DH values for each patient on the VAS and SCASS scales are presented in Figures 4 and 5.
Values of dentin hypersensitivity variation presented as mean and standard deviation, such as DH percentage reduction compared to baseline and after 15 and 30 days.
SD: standard deviation

(a and b) Individual DH mean values for each patient on the VAS scale after 15 and 30 days for incisors (a) and molars (b).

(a and b) Individual DH mean values for each patient on the SCASS scale after 15 and 30 days for incisors (a) and molars (b).
A reduction in DH was observed in the patient’s perception (VAS) and in the operator’s vision (SCASS).
In teeth that presented mild severity (incisors), in the participants’ subjective perception (VAS), there was an increase in DH at the 30-day follow-up compared to the 15-day follow-up. On the other hand, these values remained lower than the baseline values, still showing a reduction in DH compared to the beginning of the study. On the SCASS scale, there was a gradual reduction in DH values at each follow-up, being zeroed at the 30-day follow-up.
In teeth that presented moderate (incisors and molars) and severe (molars) severity, there was a gradual reduction in DH values at each follow-up, decreasing for both scales. In the group of severely affected molars, the values on the SCASS scale were zeroed at the last follow-up.
Sample characteristics (tooth as the unit of analysis)
According to Table 3, the sample consisted of 61 teeth, with 31.2% of patients being male and 68.8% female. The majority of participants (73.8%) were 12 years old or younger, while 26.2% were older than 12 years. Regarding the dental group, 39.3% were incisors and 60.7% were molars. In terms of dentin hypersensitivity severity, 6.6% of cases were classified as mild, 26.2% as moderate, and 67.2% as severe. Baseline dental pain or sensitivity was reported as absent in 6.6% of cases, mild in 32.8%, moderate in 50.8%, and intense in 9.8%.
Sample characteristics (tooth as the unit of analysis) N = 61.

Descriptive analysis of the variation in dentin hypersensitivity (tooth as the unit of analysis)
According to Table 4, the descriptive analysis of the VAS and SCASS scales revealed a progressive reduction in pain over the follow-ups. At 15 days, 77.2% of participants showed a decrease in VAS scores, increasing to 89.5% at the end of 30 days. Regarding the SCASS scale, 84% demonstrated a reduction at 15 days, with 100% of participants showing decreased dentin hypersensitivity by the 30-day follow-up. Among the teeth that did not present a zero score at baseline, 31 reached the minimum score by the end of 30 days. These results reflect a consistent trend of pain reduction over time, as evidenced by both scales used. Table 4 presents the pain reduction observed throughout the follow-ups:
Pain reduction.

Statistical analysis of pain reduction: Chi-square and Cox regression
Association between variables and pain reduction
According to Table 5, the association between categorical variables and pain reduction, as measured by the VAS scale, was analyzed. No statistically significant associations were found for gender (p = 0.584), age (p = 0.992), or tooth group (p = 0.404). However, a significant association was observed between pain severity and pain reduction (p < 0.001), indicating that participants with severe baseline pain were more likely to experience a reduction in pain scores. Among the group with pain reduction, 88.1% of teeth were classified as having severe pain, while only 11.9% had moderate pain. Conversely, in the group without pain reduction, 57.8% of teeth were classified as moderate, and 21.1% as mild, reinforcing the relationship between initial pain severity and the likelihood of pain reduction over time.
Distribution of pain reduction according to clinical variables (VAS).

Bold values indicates statistically significant.
Table 6 presents the results of the univariable and multivariable Cox regression models, which investigated factors associated with the time to categorical pain reduction according to the VAS scale. In the univariable analysis, none of the variables—gender, age, and tooth group—showed a statistically significant association with pain reduction. However, pain severity demonstrated a significant association, with severe pain at baseline being linked to a greater likelihood of faster pain reduction (HR = 0.075; 95% CI: 0.02–0.34; p < 0.05).
Univariable and multivariable analyses of factors associated with pain reduction.

p < 0.05.
In the multivariable model, this association remained significant (aHR = 0.06; 95% CI: 0.05–0.70; p < 0.05), reinforcing that higher pain severity at baseline was an independent predictor of a quicker reduction in pain scores. Other variables, including gender (aHR = 1.33; 95% CI: 0.37–4.83), age (aHR = 1.28; 95% CI: 0.10–16.0), and tooth group (aHR = 0.60; 95% CI: 0.13–2.93), did not show statistically significant associations.
Demarcated opacities color change
The Trios 4 intraoral scanner (3Shape, Denmark) was also able to perceive a color change in the teeth with demarcated opacities before and after treatment with the toothpastes with REFIX technology. For example, in case IX, the participant and the guardians reported the color change after observing that the affected teeth were lighter. Comparison of the scans at baseline and after 30 days showed this color change, as shown in Figures 6 and 7.
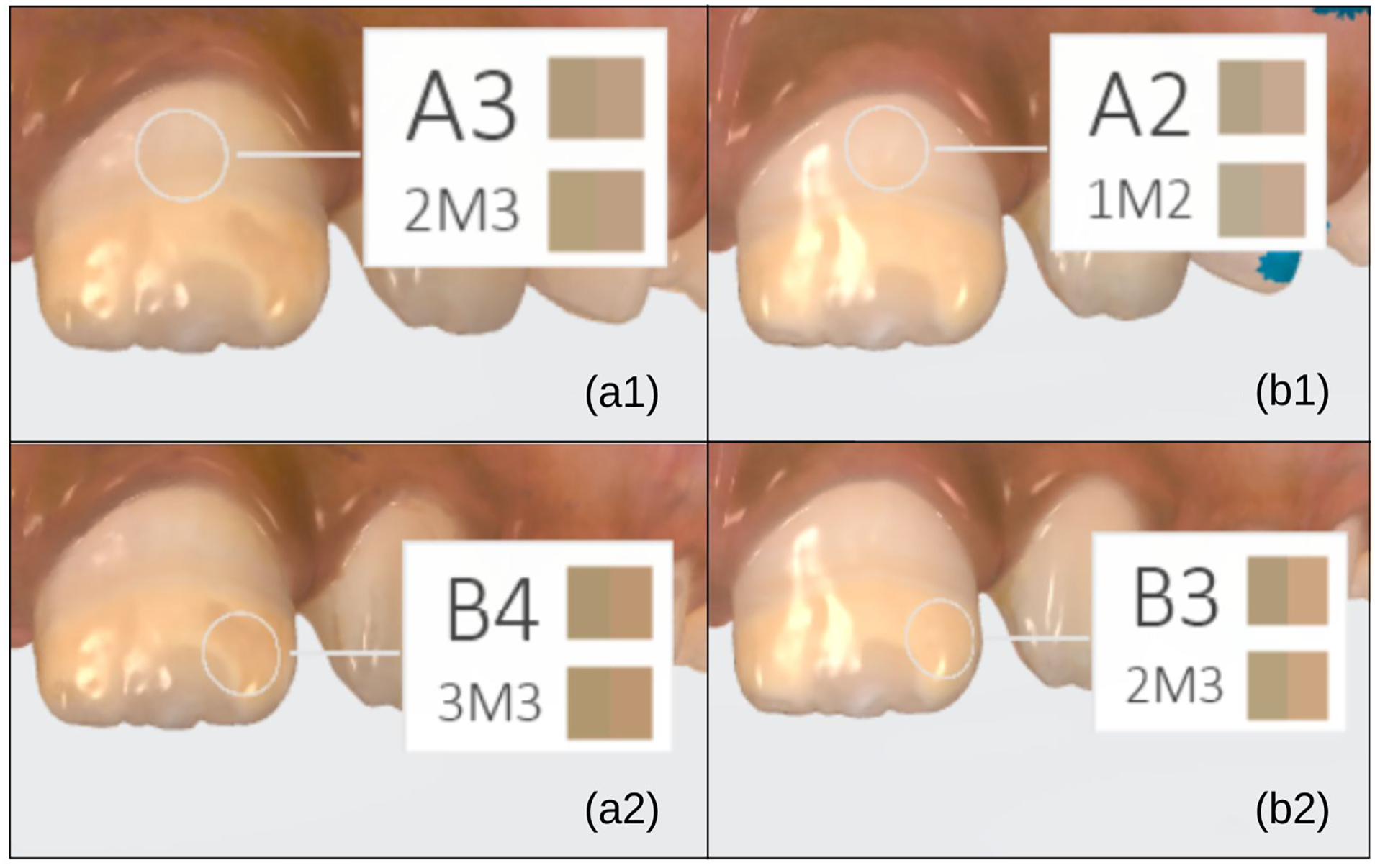
(a and b) Representative color change of incisors (healthy and opacity regions) observed by comparing the initial (a) and final (b) scans.

(a and b) Color change in molars, observed by comparing the initial (a) and final (b) scans.
The color changes the scanner perceived in study participants after 30 days of using the Si-Ca System are presented in Table 7.
Affected teeth’s color perception values before and after treatment.

N/A: not applicable.
Vita Classic (Vita 3D-Master) shade systems.
Color not identified by Classic scale (X).
Color perception of demarcated opacities by the Trios 4 scanner (3Shape, Denmark) can be assessed using the shade measurement tool based on the Vita Classic scale, in which hue, determined by the wavelength of light reflected by the teeth, is represented by the letters A (reddish-brown), B (yellowish-orange), C (greenish-gray), and D (pinkish-gray), and chroma varies from 1 to 4, in increasing order of saturation—the lower the saturation, the paler the color. 28
In these findings, based on comparison of the initial and final scans, some teeth changed to a lower chroma and maintained the same hue, having their color perception altered to a paler and consequently lighter appearance; others changed hue from B to A, altering the wavelength of light reflected by the tooth, and the chroma also decreased, making their perception lighter. Alterations in color perception were observed in demarcated opacity regions and in the healthy regions of affected teeth (Figures 6 and 7). There were also instances in which there was no alteration in the hues the scanner perceived using this system before and after the treatment.
Another system incorporated into the shade measurement tool is the Vita 3D-Master, which allows us to record, besides hue and chroma, the color’s luminosity, determined as a value. 28 Being a more specific system, even in regions where the color was perceived similarly by the Vita Classic system, there was a difference in the color perception by the Vita 3D-Master system, recorded in parentheses in the table. Additionally, there were cases in which a color alteration was perceived by the Classic system but not by the 3D-Master system.
In case IX, the molars’ color was not perceived by the Classic scale at baseline, only by the 3D-Master. In the final scan, after alteration of the color perception by treatment with the Si-Ca System, both scales were able to perceive the shades.
Discussion
In the present study, the increased thickness suggestive of the formation of a silicon-enriched layer by the association of products with REFIX technology in MIH-affected teeth was detected after 30 days; however, this increase in thickness occurs heterogeneously, for it was only perceptible on some faces and surfaces; that is, in the images obtained by scanning, there is no formation of a homogeneous layer covering the entire enamel surface. This result confirms the results of previous in vitro studies that demonstrated that the combination of a fluoride- and silicon-rich toothpaste and a calcium booster was capable of forming a silicon-enriched hydroxyapatite mineral layer similar to the enamel structure and obliterating dentinal tubules with just one application.13,17
According to the literature, the remineralization process can occur through the precipitation and growth of crystals. 29 Boosters are known to increase fluoride’s effectiveness and accelerate dental remineralization through the incorporation of calcium and phosphate into the demineralized structure, resulting in mineral gain. This occurs due to the presence of bioactive ions based on hydroxyapatite and calcium phosphates in its composition.30,31 Small crystal aggregates form until a certain size, called the critical nucleus, is reached. From this nucleus, the growth of this reaction occurs through the deposition of smaller crystals at the expense the substrate’s dissolution. 32
Based on the above, the hypothesis suggested to explain the heterogeneity in the formation of the silicon-enriched layer perceived by the intraoral scanner is that, like any remineralization process, the layer is formed from a critical nucleus and crystallizes around it, which may explain why it is possible to observe only some points with increased thickness and others not. Longitudinal studies with longer follow-up periods should be conducted to determine whether with a longer time of substrate being offered and dissolved it is possible to form a more homogeneous layer along the teeth, covering a larger percentage of the tooth surface.
It was also possible to observe points where the tooth’s enamel contour in the final scan shows a decrease in the tooth contour compared to the initial contour, suggestive of a decrease in thickness. It is suggested that the Trios 4 scanner (3Shape, Denmark), with a precision of 6.9 ± 0.9 µm, would be able to perceive alterations in thickness due to micrometer-level wear of the demarcated opacities due to the hypomineralized enamel’s greater porosity and greater chances of post-eruptive fractures, 4 resulting in points of lower final thickness compared to the initial one in some cases exhibiting yellow-brown opacities.
The DH results showed a reduction in pain for all patients, regardless of tooth or severity, with a total mean reduction: VAS: 65% after 15 days of treatment and 83% after 30 days, SCASS: 76% after 15 days of treatment and 94% after 30 days. These results align with the literature because existing in vitro and in vivo studies provide evidence that silicon-based technologies can reduce DH and promote enamel-dentin repair.11,33,34 Notably, in the per-tooth analysis, the outcomes were even more striking: by the end of the treatment, 31 teeth that initially exhibited hypersensitivity became completely asymptomatic, underscoring the efficacy of the intervention in achieving substantial and sustained clinical relief.
Also, it was possible to detect an increase in the patient’s perception scale (VAS) values 30 days after treatment compared to 15 days after treatment; however, they remained lower than the values found at baseline. When the SCASS scale was used, however, a continuous reduction was observed over time. A possible explanation could be the more sensitive and fragile emotional state in which MIH patients find themselves.
This study demonstrated a gradual reduction in dentin hypersensitivity (DH) over time, consistent with Bekes et al., 35 who evaluated an 8% arginine and calcium carbonate-based desensitizing agent in MIH-affected molars. Both studies observed progressive DH reduction, though Bekes et al. reported a sustained decrease over 8 weeks, while the present study noted a temporary increase in mild cases at 30 days before stabilization. Additionally, SCASS scores reached zero in severely affected molars, mirroring the complete DH resolution seen in Bekes et al.’s intervention group. Differences in study design, treatment, and follow-up duration should be considered when comparing outcomes. 35
The data analysis revealed that initial pain severity was a significant predictor of faster pain reduction, while variables such as gender, age, and tooth group showed no statistically significant associations. This result may have occurred because studies show that patients with severe MIH tend to experience a more intense DH condition, 36 associated with stronger pain as well as a more significant negative impact on oral health-related quality of life (OHRQoL) compared to patients with moderate severity. 37 This may be related to a heightened perception of pain; therefore, any noticeable improvement ultimately has a greater impact on OHRQoL and the patients’ pain perception (VAS scale).
As for the demarcated opacities’ color alteration, it was possible to perceive through the comparison of scans, in some cases, that MIH-affected teeth were lighter after 30 days compared to the initial scan after the use of dentifrices with REFIX technology. Knowing that teeth with MIH have a characteristic demarcated opacity coloration that varies from white-cream to yellow-brown due to their lower mineral content in their composition and higher organic content 38 and that this technology is capable of forming a silicon-enriched layer and causing remineralization of the tooth surface,12,20 it is possible that with the deposition of new minerals in hypomineralized teeth, the demarcated opacities’ color on affected teeth may be altered.
In a context in which it was possible to perceive alterations in thickness and color through the comparison of 3D models before and after the use of the REFIX Booster system as well as clinical alterations in the picture of DH, it is clear that this technology’s effects are perceptible. It is also pertinent to note that the treatment with the Refix technology did not prevent the loss of structure, even at the micrometric level, in cases of darker opacities over the follow-up period.
However, this preliminary longitudinal study was the first study conducted to clinically evaluate the REFIX Booster System’s effects on teeth with MIH to test the feasibility of broader research by evaluating aspects such as logistics, data collection, measurement tools, and analysis, serving as a pilot study. As a limitation of this study, the small sample size and shorter follow-up period stand out. Nonetheless, its results can serve as a basis for the development of new longitudinal clinical studies with longer follow-up times as well as new laboratory studies to better understand this technology’s durability and mechanisms of action in hypomineralized teeth.
Conclusion
The intraoral scanner Trios 4 (3Shape, Denmark) was able to perceive alterations in micrometer-level thickness between scans. This increase in thickness suggests the formation of a silicon-enriched layer through the REFIX technology.
REFIX technology is effective in reducing DH within a period of 15–30 days, showing itself as a possible alternative for managing this condition in patients with MIH. More longitudinal studies with longer follow-up periods are needed to verify the durability of this technology’s effects in the management of DH.
Color alterations were observed in MIH-affected teeth following the use of dentifrices containing this technology, affecting both the demarcated opacities and the healthy enamel regions. Further research is needed to explore this association and elucidate the underlying mechanisms driving these changes.
Footnotes
ORCID iDs
Ethical considerations
The Research Ethics Committee of the Faculty of Dentistry, University of São Paulo (FO-USP) approved this project under registration CAAE: 79258224.0.0000.0075.
Consent to participate
Informed consent statements were obtained from all subjects involved in the study.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded in part by the Coordenação de Aperfeiçoamento Pessoal de Nível Superior—Brazil (CAPES)—Finance Code 001. The 3Shape Company also funded the intraoral scanner for the development of the research.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The author Vilhena FV is a consultant for Dentalclean.
Data availability statement
All data generated or analyzed during this study are included in this manuscript.