
Abstract
Objective:
The aim of this systematic review was to investigate, identify, and summarize the existing literature on the levels of proinflammatory cytokines and chemokines present in gingival crevicular fluid (GCF) of primary teeth restored with stainless steel crowns (SSC) versus control teeth.
Materials and methods:
The systematic review was registered in the Open Science Framework (ID): 10.17605/OSF.IO/39U4D. In addition, it was prepared following the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA). Five electronic databases were used to identify studies for this systematic review: PubMed, Scopus, ScienceDirect, Web of Science, and Google Scholar, from January 10, 1999, to September 15, 2024. The risk of bias in the included studies was assessed using Joanna Briggs Institute (cross-sectional studies) and the Cochrane Risk of Bias for Randomized Trials (RoB 2.0) in randomized clinical trials.
Results:
The review includes four studies (two cross-sectional and two randomized clinical trials). A total of 75 children aged 3 to 10 years were studied. GCF samples were taken from 98 upper and lower molars rehabilitated with SSC and control teeth (without SSC). ELISA analyzed all samples. This way, the levels of four proinflammatory cytokines and chemokines, IL-1β, IL-6, MIP-1α, and MIP-1β, were determined. The studies reported significant differences between both study groups: IL-1β: 27.30 versus 23.56 p < 0.05; MIP-1α: 682.55 versus 197.60 p < 0.05; and MIP-1β: 884.35 versus 287.85, p < 0.05.
Conclusions:
This systematic review provides a comprehensive and current overview of the concentrations of proinflammatory cytokines and chemokines present in GCF, providing new insights into the pathogenesis of gingival inflammation in children with SSC. IL-1β, MIP-1α, and MIP-1β levels increased in the GCF of upper and lower molars rehabilitated with stainless steel crowns compared to control primary teeth.
Introduction
Oral health in children is a determining factor of general well-being. According to the latest WHO report, the global prevalence of early childhood caries ranges from 60% to 90% in developing countries, highlighting an urgent need for effective restorative strategies. 1 Not only are caries lesions a reason for the rehabilitation of deciduous teeth, but developmental disorders of the dental organ, fractures, and other conditions such as hypoplastic lesions are the most common diagnoses that require tooth rehabilitation.2,3 These conditions in primary teeth cause sensitivity and pain in children and affect their quality of life and that of their caregivers.4,5
Primary teeth are essential for aesthetics, chewing, speech, and the proper development of occlusion in the permanent dentition. 6 A significant challenge for primary teeth treatment is that the younger the age, the lower the survival rate of restorations. The effective restoration of primary teeth is influenced by several factors, such as the child’s cooperation, the operator’s behavioral and technical skills, and the characteristics of the selected restorative biomaterial. 7
While resin-bonded composite strip crowns are commonly preferred for primary anterior teeth due to their esthetics, zirconia crowns offer superior durability and biocompatibility, making them a viable alternative, particularly in cases with high caries risk or parental preference for metal-free options. 8 Although amalgam was traditionally favored for its durability and affordability, its use has declined due to environmental and health concerns related to mercury. Alternatives such as high-viscosity glass ionomer cement (GIC) and resin-modified glass ionomer cement are increasingly preferred, particularly in atraumatic restorative treatment protocols. 9 Stainless steel crowns (SSC) remain preferred for posterior primary teeth due to their high fracture resistance, minimal technique sensitivity, and superior longevity compared to direct restorations. However, their esthetic limitations and potential impact on gingival health necessitate careful case selection. 10
Furthermore, the use of SSC in pediatric dentistry includes the restoration of teeth affected by extensive carious lesions, post-pulpotomy/pulpectomy, dental development disorders, fractures, and hypoplasic lesions, surpassing other materials such as GIC and compomers, among others, especially in those children with a high risk of caries. It has been reported that the main drawback of SSC is its metallic appearance, but its success rate is as high as 97.2%.9,10 In addition, the design modifications that have taken place over the years since their first use in 1950 have improved both the morphology and the placement procedure, which must be quickly given that we are dealing with pediatric patients. 11
Although the main objective is to restore the tooth’s functionality in the mouth, it is important to consider all aspects that restore oral health, including periodontal tissues. The marginal adaptation of the SSC is an important factor in maintaining gingival health since it has been described that the health of the gingival tissue is correlated with the dental biofilm around these crowns. 12
Alterations in the typical oral biofilm due to plaque accumulation result in poor periodontal health in children. The presence of an altered biofilm leads to the activation of immune system cells, which release cytokines and chemokines that act as signaling molecules that coordinate and direct the host’s defense. The persistence of the presence of these mediators triggers a chronic inflammatory response. In pathological conditions, these cytokines control bone resorption, potentially leading to bone and tooth loss. 9
It has been described that in individuals with periodontal inflammation, concentrations of proinflammatory cytokines are elevated in gingival crevicular fluid (GCF) and may contribute to a systemic hyperinflammatory state.13,14
Despite advancements in pediatric restorative materials, there remains a need to assess the biochemical effects of stainless steel crowns on gingival health. This systematic review aims to evaluate the impact of SSC placement on biochemical markers in GCF, providing insights into their potential role in periodontal inflammation and long-term oral health outcomes.
Materials and methods
Project registration
The study was registered in the Open Science Framework (OSF) platform, which is available at 10.17605/OSF.IO/39U4D.
Protocol format
The protocol for this systematic review and meta-analysis was prepared using the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) guidelines (Supplemental Material). 15
Research question construction
The PECOS items were used to construct the research question:
P (Participants) → GCF samples collected from primary teeth in systemically healthy children.
E (Exposure) → Primary teeth with SSC.
C (Control) → Primary teeth without SSC.
O (Outcomes) → Differences in levels of proinflammatory cytokines and chemokines in GCF.
S (Studies) → Cross-sectional studies and randomized clinical trials.
Based on the above, the following research question was formulated: Are there differences in the levels of proinflammatory cytokines and chemokines in the GCF of primary teeth restored with SSC versus control teeth?
Eligibility criteria
Inclusion criteria
Studies with the following characteristics were included:
Children aged 3 to 10 years.
Periodontally healthy anterior or posterior primary teeth rehabilitated with SSC.
Informed consent signed by the child’s parents and/or guardians.
Studies approved by the ethics committee of the corresponding institution.
Articles written in any language, published after 1999.
Exclusion criteria
Studies that met the following characteristics were excluded:
Primary teeth are rehabilitated with metal-ceramic crowns, zirconia, or any biomaterial other than stainless steel crowns.
Children with periodontal disease (gingivitis and/or periodontitis).
Children who have received pharmacological treatment (antibiotics/anti-inflammatory drugs) in the last 6 months.
Children with mental problems.
Children with pre-existing systemic diseases.
Children with orthodontic treatment.
Studies in animal models or cell lines.
Book chapters, systematic reviews and meta-analyses, editorials, and letters to the editor.
Information sources and search strategy
One investigator conducted an electronic search in five databases: PubMed, Scopus, ScienceDirect, Web of Science, and Google Scholar, from January 10, 1999, to September 15, 2024. Table 1 samples the search strategy employed in the present work. The keywords “Stainless Steel,” “Dental Crowns,” “Primary Teeth,” “Cytokines,” “Chemokines,” and “Gingival Crevicular Fluid” were used, along with the use of Boolean operators “OR” and “AND.” Additionally, to make our search for related articles even more exhaustive, a manual search was performed in the journals: “Pediatric Dentistry,” “Journal of Clinical Pediatric Dentistry,” “BMC Oral Health,” “Journal of Prosthetic Dentistry,” “Journal of Advanced Prosthodontics,” “International Journal of Prosthodontics,” “International Journal of Periodontics & Restorative Dentistry,” and “Journal of Periodontal and Implant Science”.
Results of the complete search strategy employed in the five databases.

Selection process
Two authors independently analyzed the records obtained through the previous search strategy. Subsequently, the investigators carefully examined the titles and abstracts of the studies. Those that did not meet the inclusion criteria, as well as duplicates, were automatically eliminated. Studies that could potentially be selected were subjected to a detailed review. Any discrepancies that arose during the record comparison were resolved by consulting a third investigator, a specialist in the field. EndNote V.9 software was used to manage all records for this process.
Data extraction
Two investigators extracted the following data independently:
First author.
Year of publication.
Country.
Study design.
Ethics.
Gender.
Age.
(n) = Exposure group (primary teeth restored with SSC) and control group (natural contralateral primary teeth free of restoration with SSC).
Total population studied.
Confounding factors
Primary teeth restored.
Brand of SSC.
GCF collection tools.
Type of immunoassay.
Mean values of proinflammatory cytokine and chemokine levels.
Main findings.
Variables extracted from the articles were organized in Word (Microsoft) tables. Quantitative data were presented as mean ± standard deviation, and qualitative data were expressed as frequencies (absolute and relative).
Study risk of bias assessment
Two investigators independently performed the risk of bias assessment in the included studies. The Joanna Briggs Institute tool was used for the cross-sectional studies. 16 This tool examines eight items related to inclusion criteria, a detailed description of the study subjects (EG and CG), identification and management of confounding factors, and formal statistical analysis to facilitate the biological interpretation of the results. Thus, total scores ranged from 0 to 8, with response options such as “Yes,”/“No,”/“Unclear,” and “Not applicable.” Consequently, studies were categorized as high risk with scores from 1 to 3, moderate from 4 to 6, and low risk with scores of seven or more. 17 The Cochrane Risk of Bias for Randomized Trials (RoB 2.0) tool 18 was used for the risk of bias assessment of randomized clinical trials. 18
Results
Study selection
We initially found 1299 articles in five electronic databases, including PubMed (13 records), Scopus (1 record), ScienceDirect (25 records), Web of Science (875 records), and Google Scholar (385 records). No articles of potential interest were identified in the hand search related to the main topic of this research. During the identification phase, duplicates were eliminated (23 records). Then, in the screening phase, based on the title and abstract of each record, 1258 studies were excluded, giving a total of 18 studies. Applying the eligibility criteria, three additional records (literature reviews) were discarded,19–21 resulting in 15 potentially relevant records. After reviewing the full text of the remaining articles, 11 were discarded as unrelated to the topic of interest. The authors evaluated cytokine levels in permanent teeth rehabilitated with metal-ceramic, zirconia, and other biomaterials fixed dental prostheses in five articles.22–26 One study evaluated cytokine expression in mechanically exposed or caries-affected pulp tissue. 27 Finally, in five articles, clinical, radiographic, and microbiological aspects of primary teeth rehabilitated with stainless steel crowns were examined, but not the levels of proinflammatory cytokines and chemokines in GCF.28–32 Therefore, four articles were included for qualitative analysis, three of which were used to perform the meta-analysis. Details of the study selection are presented in Figure 1.
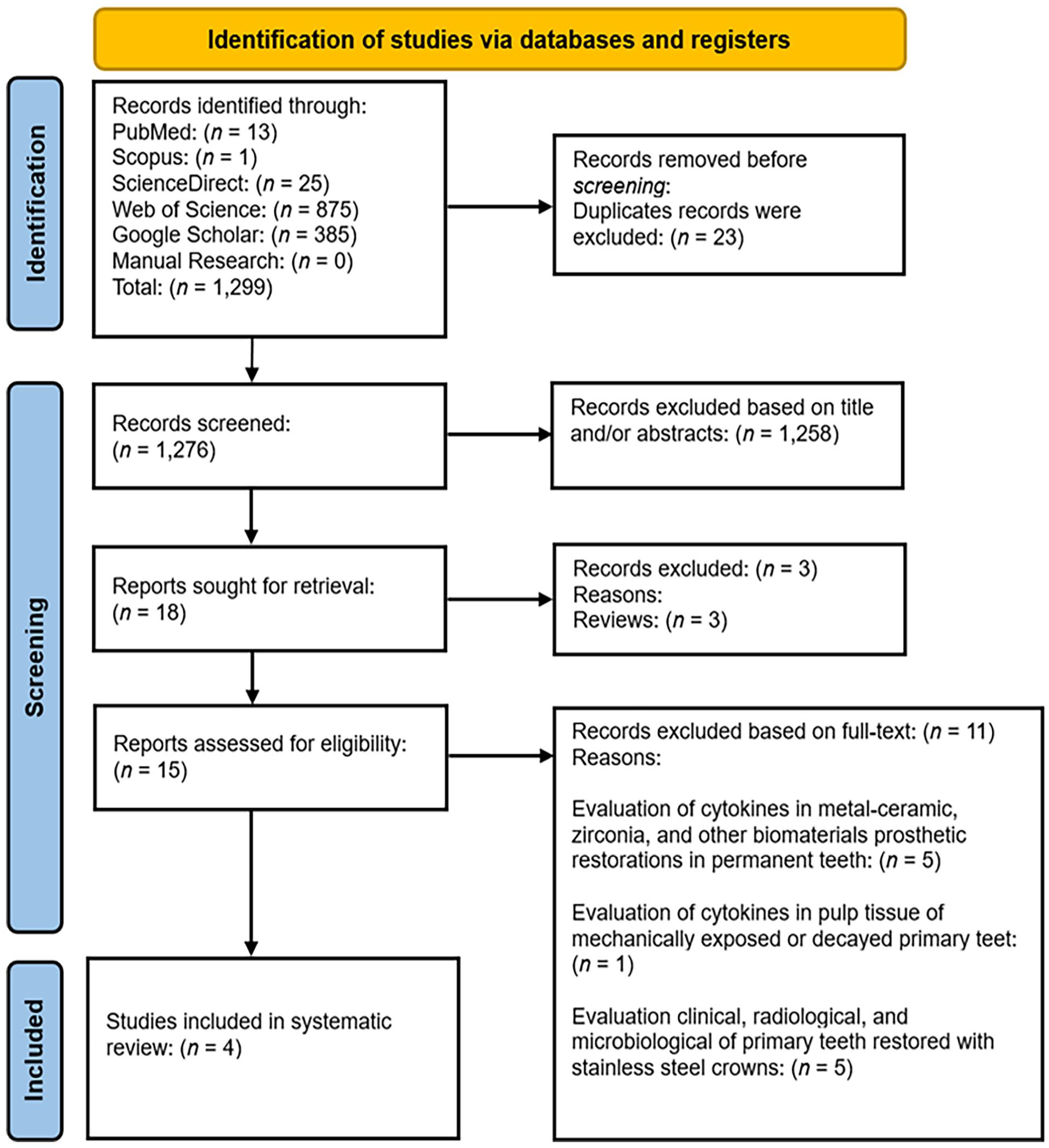
PRISMA flow diagram of the study selection process.
Qualitative analysis: Main outcomes of included studies
In this systematic review and meta-analysis, a total of four articles, two cross-sectional studies,10,13 and two randomized clinical trials12,14 were reviewed.
A total of 75 children were studied in the included papers. Of these, a total of 98 primary teeth were analyzed, of which 55 (56.1%) represented the case group (primary teeth rehabilitated with SSC) and 43 (43.9%) represented the control group (contralateral primary teeth free of SSC). The ages of the children ranged from 3 to 10 years. Gender was not specified in the included studies.10,12–14
The articles were published between 2016 and 2024. All four studies were published in a single country (India)10,12,14 (Table 1).
GCF samples were collected from 46 (46.9%) mandibular primary molars and 52 (53.1%) maxillary primary molars. For their collection, micropipettes were used in 50% of the cases, and periopapers and absorbent paper tips in 20%. The enzyme-linked immunosorbent assay (ELISA) (100%) was the most commonly used immunological method for determining proinflammatory cytokine and chemokine levels.10,12–14 Thus, five proinflammatory cytokines and chemokines were evaluated: IL-1β, 10 IL-6, 14 MIP-1α, and MIP-1β12,13 (Tables 2 and 3).
Characteristics of the included studies.
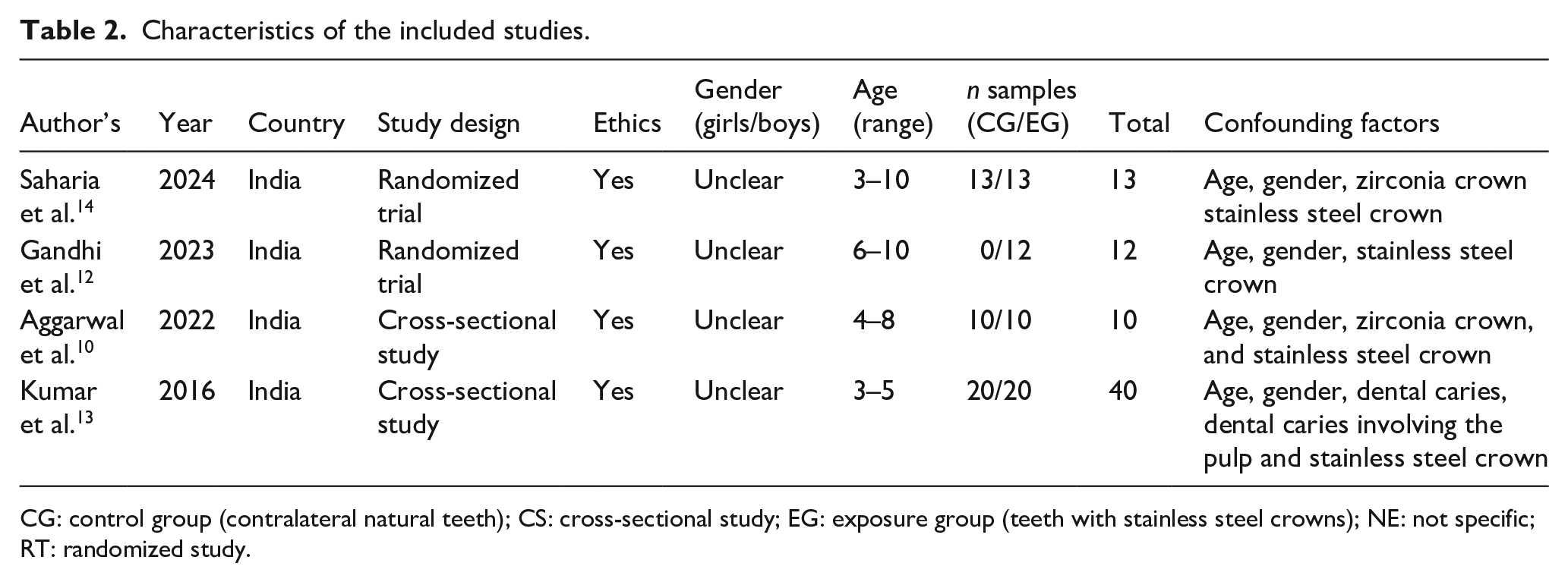
CG: control group (contralateral natural teeth); CS: cross-sectional study; EG: exposure group (teeth with stainless steel crowns); NE: not specific; RT: randomized study.
Clinical and immunological characteristics of the studies assessed.
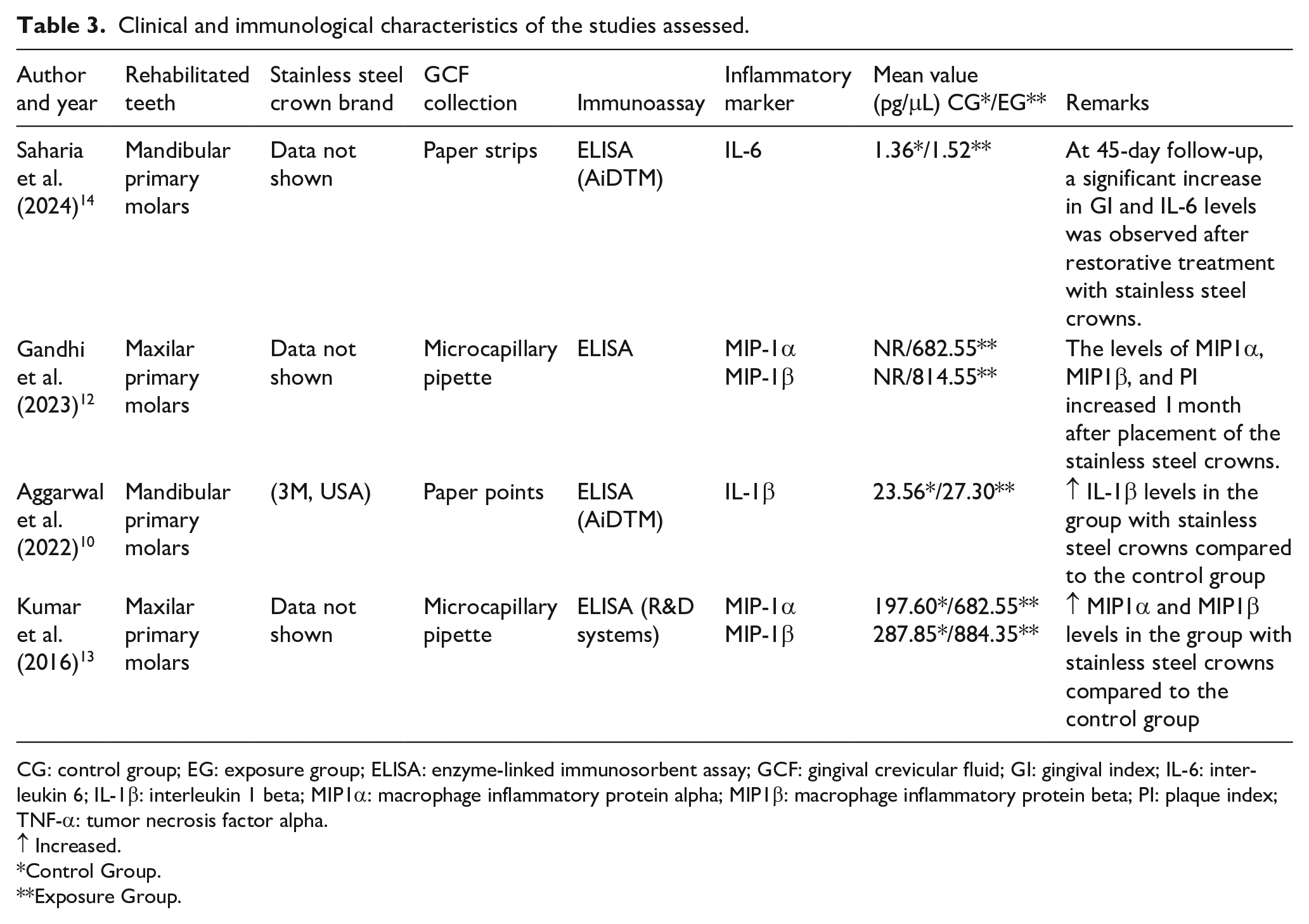
CG: control group; EG: exposure group; ELISA: enzyme-linked immunosorbent assay; GCF: gingival crevicular fluid; GI: gingival index; IL-6: interleukin 6; IL-1β: interleukin 1 beta; MIP1α: macrophage inflammatory protein alpha; MIP1β: macrophage inflammatory protein beta; PI: plaque index; TNF-α: tumor necrosis factor alpha.
Increased.
Control Group.
Exposure Group.
IL-6, MIP1-α, MIP1-β, and IL-1β levels in GCF of primary teeth with stainless steel crowns
The IL-1β, MIP1α, and MIP1β levels in GCF increased in teeth restored with SSC compared to natural teeth. In addition, IL-6, MIP1α, and MIP1β levels were found to increase in GCF between the first 30 to 45 days after placement of SSC.10,12–14
Risk of bias in studies
Cross-sectional studies (50%)10,13 had a moderate risk of bias. They were deficient in identifying and managing confounding factors. In general, randomized clinical studies12,14 showed a low risk of bias, identifying their primary deficiencies in the first two domains about the randomization process (the allocation sequence was not concealed) and the process of bias due to deviations in the interventions, where the participants/guardians of the children, as well as the scientific staff involved, knew the intervention that had been assigned to them (Figures 2 and 3).

JBI for risk of bias assessment of cross-sectional studies.
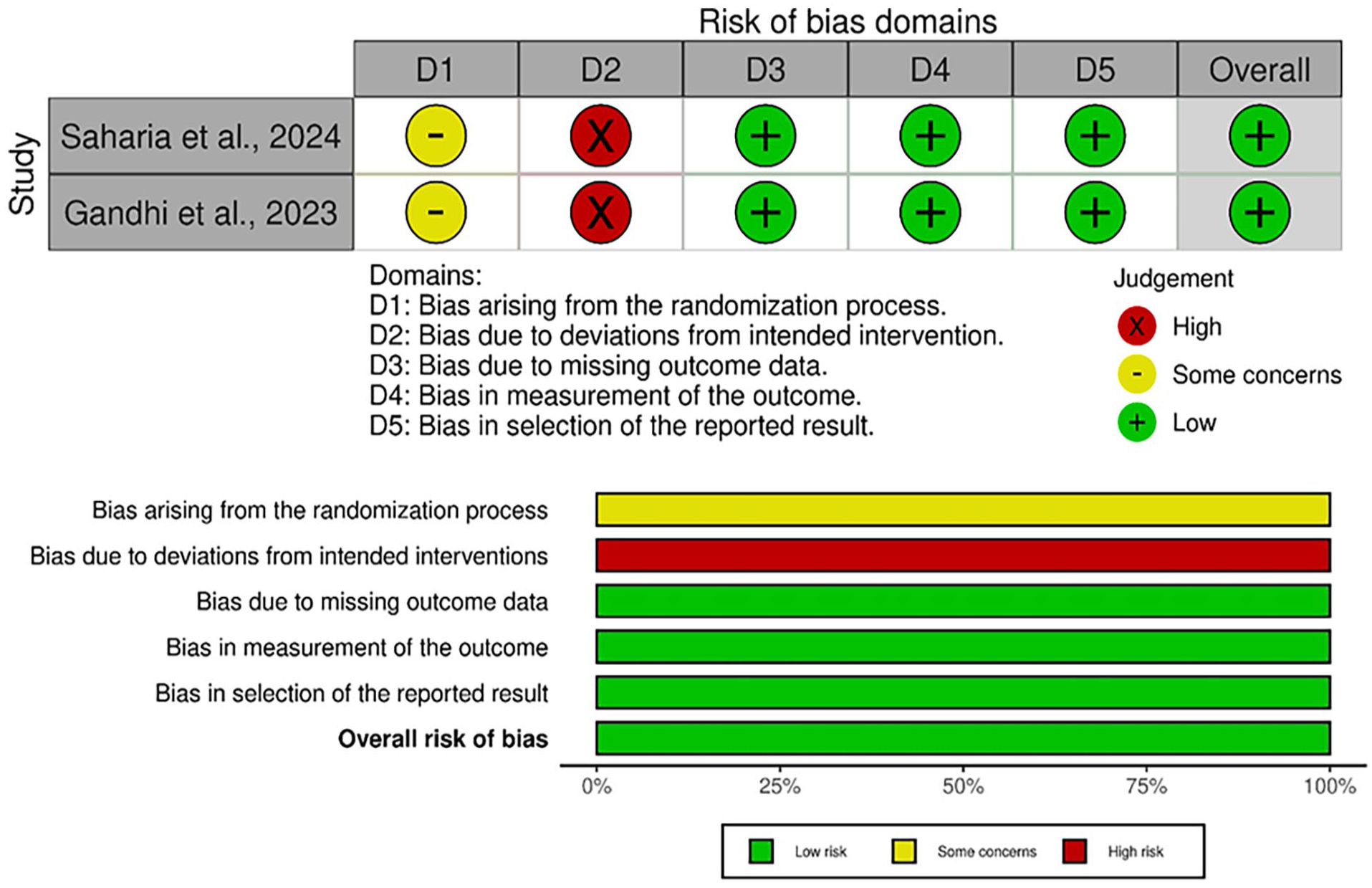
RoB.2 for risk of bias assessment of randomized clinical trial.
Discussion
SSC is the first restorative option for primary teeth due to its high durability, good cervical fit, and affordable cost. However, its involvement in the impact of periodontal health, particularly in plaque accumulation and consequent gingival inflammation, is an area of interest for dentistry.10,12,13
Inadequate marginal adaptation creates space between the restoration and the tooth, contributing to the buildup of dental biofilm.33,34 Inadequate marginal adaptation can present in various ways: Protruding margins, subgingival margins, and deficient margins.10,12–14,35 Protruding margins, where the restoration extends beyond the prepared tooth, create an area where dental biofilm can quickly accumulate.12,35 Conversely, subgingival margins, where the restoration is placed below the gingival margin, can promote inflammation. Placing in this position is usually necessary in specific cases but increases the risk of inflammation due to the complexity of cleaning teeth in that area.10,35 Poor margins, where the restoration does not fit properly to the prepared tooth, can also lead to complications. These margins can create spaces that allow microorganisms to enter and plaque buildup, leading to gingival inflammation.10,35 SSC can be trimmed, contoured, and adapted to the tooth during the cementation procedure; this process allows the dentist to achieve a better marginal adaptation, minimizing the space between the crown and the tooth.10,12,35 Now, it is essential to highlight that optimal marginal adaptation depends on the skill of the dentist and the technique implemented, regardless of the type of restoration selected.
Oral hygiene remains a critical factor in maintaining periodontal health around restorations. Infants with poor oral hygiene often have increased plaque buildup around restorations, which exacerbates gingival inflammation,12,13 On the contrary, adequate and correct oral hygiene helps mitigate the adverse effects of periodontal health. 13 Plaque accumulation is strongly associated with two determining factors: The composition of the restoration material and the surface roughness of the restoration.
For years, SSC has been the most widely used full-coverage restoration for primary dentition in children. However, SSC tends to have a rougher surface than the other materials, which could be attributed to increased plaque accumulation and inflammation identified around restorations. Additionally, stainless steel is a material that can release metal ions, promoting bacterial adhesion. The study conducted by Aggarwal et al. 10 demonstrated that prefabricated zirconia crowns (ZC) presented superior periodontal health due to their smooth surface and low affinity for plaque accumulation compared to SSC. Consequently, ZC can be a relative replacement for SSC in primary molars with an aesthetic advantage. These findings are similar to what was identified by Saharia et al. 14 in which they suggest that ZC are superior to SSC in terms of maintaining periodontal health after cementation; thus, lower growth of bacterial colonies was also harbored on their ZC surfaces, particularly Lactobacillus casei.
The host’s response to restorative materials plays a fundamental role in gingival inflammation. The immune system recognizes foreign materials, such as dental restorations, and triggers an inflammatory response.10,12–14
GCF, a normal transudate, becomes an inflammatory exudate during periodontal disease. It contains several cytokines and inflammatory mediators, including macrophage inflammatory protein beta (MIP-1β), interleukin one beta (IL-1β), and transforming growth factor beta (TGF-β).25,36 Elevated levels of these cytokines in GCF are linked to increased periodontal inflammation and can be used as biomarkers to measure the health of periodontal tissues. 36 Studies have demonstrated that increased levels of IL-1β and TGF-β in GCF are associated with periodontal disease severity and inflammation.37,38
The effect of SSC on the biochemical parameters of proinflammatory cytokines and chemokines in GCF is an important feature of pediatric dentistry, especially when managing primary teeth. SSCs are commonly used to restore primary molars due to their longevity and efficiency in avoiding additional decay. However, their impact on gingival health, notably inflammation, has been investigated.
Studies have revealed that SSC installation can cause various degrees of gingival irritation. For example, Harshitha et al. 39 observed that out of 26 SSC tested, 14 crowns produced mild gingival irritation during follow-ups of 3 to 6 months, showing a significant incidence of inflammatory responses associated with these restorations. Mostafa et al. 40 confirmed this finding, stating that inflammation of the surrounding gingival tissue is usually related to SSC, especially when the crowns are not well-suited.
Furthermore, SSC clinical performance has been connected to crown adaptability and fit. Mulder et al. 41 underlined that the marginal adaptation of SSC is critical because poorly fitted crowns are associated with greater rates of gingival irritation. Al-Dulaimy and Al-Khannaq 42 found that the dimensions and fit of SSC can considerably influence the health of the surrounding gingival tissue. Inadequate adaptation can cause plaque formation, raising proinflammatory cytokines and chemokines levels in GCF and worsening gingival inflammation. 43
In addition to the mechanical factors of crown installation, SSC material qualities influence the inflammatory response. Mostafa et al. 40 found that SSC, while efficient, is usually accompanied by irritation of the surrounding gingival tissue, especially when the crowns are not adequately fitted.
SSC on primary teeth has been linked to inflammatory reactions in the GCF, including elevated levels of proinflammatory cytokines, including IL-1β. IL-1β and tumor necrosis factor-alpha (TNF-α), a critical mediator in the inflammatory process, are widely employed as biomarkers to assess periodontal tissue health around dental restorations. 44 Beldüz Kara and Yılmaz’s 44 study found a considerable correlation between gingivitis and crown fit, highlighting the significance of correct crown placement in reducing inflammatory reactions.
Research suggests SSC can impact IL-1β levels in GCF, a crucial factor in determining gingival tissue inflammation. SSC placement has been linked to higher levels of IL-1β, indicating an inflammatory reaction. This is especially important when the crowns are not adequately fitted, leading to plaque formation and subsequent inflammation. 39 Harshitha et al. 39 found that out of 26 SSC evaluated, 14 caused mild gingival inflammation, suggesting a correlation between SSC placement and increased inflammatory markers in GCF.
Several studies have shown a correlation between IL-1β levels and gingival health. Yaghobee et al. 45 and Gao et al. 46 found considerably higher amounts of IL-1β in the crevicular fluid around implants than in healthy teeth, suggesting a similar process may work around SSC. These results are similar to those found in GCF of teeth with crowns reported by the studies of this systematic review. 10
The inflammatory response in GCF can be influenced by several factors, including the material properties of the crowns and the individual’s oral hygiene practices. Toker et al. 47 highlighted that smoking did not significantly affect IL-1β levels in GCF, suggesting that other factors, such as SSC, maybe more critical in modulating cytokine levels. Furthermore, the adaptation and fit of SSC are critical; poorly fitting crowns can worsen inflammation by increasing plaque buildup, which raises IL-1β levels. 41
On the other hand, interleukin-6 (IL-6) is an important cytokine involved in the inflammatory response. It is frequently measured in GCF to assess periodontal health. The research by Saharia et al. 14 was included in this review, where the levels of IL-6 in GCF were evaluated before and after the placement of stainless steel crowns, and a significant increase in this cytokine was observed, as well as clinical characteristics of gingival inflammation. In addition, research has demonstrated that GCF IL-6 levels can be biomarkers for periodontal inflammation. Kurgan et al., 48 for example, showed that IL-6 levels could be a good indicator of the severity of periodontal disease in patients with chronic periodontitis showing higher concentrations of the protein than healthy controls. This implies that the presence of dental restorations that may irritate gingival tissues may worsen the inflammatory response, as indicated by IL-6 levels.
Harshitha et al. 39 found that stainless steel crowns were linked to mild gingival inflammation, which may eventually cause an increase in IL-6 levels in GCF. Based on changes in cytokine levels in GCF, their study showed that stainless steel crowns contribute to a measurable inflammatory response, even though they may not cause severe inflammation.
Furthermore, Menezes et al. 49 discovered that systemic diseases like HIV can alter the amounts of IL-6 in GCF, suggesting that local and systemic factors can influence cytokine expression in periodontal tissues. This emphasizes how complicated the inflammatory response is when dental restorations like stainless steel crowns are present because unique patient characteristics can also influence the amounts of IL-6 in GCF.
Studies show that several factors, including dental restorations, can affect macrophage inflammatory protein alpha (MIP-1α) levels. For example, Duzagac et al. 50 discovered that inflammatory mediators, such as different cytokines and chemokines, are elevated in GCF patients with periodontal disease. This increase in inflammatory markers, such as MIP-1α, could indicate how the body reacts to the foreign substance and the resulting tissue irritation. MIP-1α levels are increased in patients with crowns compared to control subjects, in addition to MIP-1α levels increasing for up to a month after placement.10,12
Furthermore, investigations have demonstrated that both local and systemic circumstances regulate the inflammatory response in GCF. Obesity can lead to elevated levels of proinflammatory cytokines, such as MIP-1α in GCF, complicating the inflammatory response in patients with stainless steel crowns. 51 This association highlights the significance of considering systemic health when assessing the inflammatory condition of periodontal tissues.
Other inflammatory mediators, like TNF-α and IL-6, have been linked to elevated MIP-1α levels in GCF. Fujihara et al. 51 found that TNF-α promotes the production of ligand of the receptor activator of nuclear factor κ B (RANKL) in gingival epithelial cells, which is essential for osteoclast development and bone resorption. 52 This interaction shows that higher levels of MIP-1α in GCF may be part of a broader inflammatory response, including several cytokines and chemokines, contributing to periodontal tissue degradation.
Finally, a chemokine called MIP-1β is important for the inflammatory response in GCF. The type of dental restoration and the inflammatory response that goes along with it can affect the amount of MIP-1β in GCF, which measures the inflammatory status of periodontal tissues. 36 The presence of SSC on central teeth can enhance the inflammatory response, perhaps leading to higher levels of inflammatory mediators in GCF. Stainless steel crowns can cause gingival inflammation, leading to elevated proinflammatory cytokines such as MIP-1β and IL-1β in GCF. 53 In this sense, it is observed that MIP-1β as well as MIP-1α are increased in GCF of teeth with Stainless steel crowns.10,12 Elevated levels of MIP-1β and other inflammatory cytokines in GCF may indicate persistent inflammation and require additional clinical intervention to manage periodontal health successfully. 54 This inflammatory response is critical because it represents the body’s attempt to control the microbiological burden of dental restorations and the surrounding periodontal tissues.55–57
Furthermore, aesthetic considerations and parental satisfaction with SSC against alternative crown materials, such as zirconia, have been established. While zirconia crowns are frequently favored for their aesthetic aspects, SSC remains the gold standard because of their established clinical effectiveness and lower costs. 58 However, the risk of gingival inflammation associated with SSC demands close monitoring of cytokine levels in GCF to guarantee optimal periodontal health in children.
Limitations
This review recognizes some limitations that are highlighted below and should be considered for future studies:
✓ Including only four studies (cross-sectional and randomized clinical trials) with a minimal n (98 primary teeth) makes it difficult to detect significant differences or generalize the results to the broader population. This line of research continues to grow, and it would be important for researchers to carry out good methodological planning to avoid bias.
✓ Due to the limited data availability, it is a quantitative analysis that is impossible to perform.
✓ Differences in sex and age.
✓ Differences in the composition of the sub and supragingival microbiota.
✓ Differences in the type of cement used for the fixation of stainless steel crowns in primary teeth. Could types of cement influence the immunoinflammatory response?
✓ The determination of only four proinflammatory mediators.
✓ Differences in the way GCF is collected and processed.
✓ Differences in the immunoassay techniques and protocols across studies might lead to variability in cytokine measurement, affecting the comparability of results.
✓ The studies included did not specify the duration of follow-up after SSC placement, which was critical for understanding the long-term effects of SSC on inflammatory responses in the GCF.
Future perspectives
Future studies should consider and emphasize the confounding factors that could be influencing their results, as well as how to address them.
All studies were conducted in a single country. More studies need to be done in other parts of the world.
Evaluation of stainless steel crowns placed only in the posterior sector. What about the behavior concerning proinflammatory cytokine and chemokine levels (inflammation dynamics) of stainless steel crowns placed in the anterior sector?
The periodontal condition of children. It would be interesting to compare the levels of these inflammatory mediators in children with gingivitis or in children with more advanced periodontal conditions.
Conclusion
Primary teeth restored with SSC will tend to accumulate more plaque compared to natural primary teeth; this will lead to increased levels of proinflammatory cytokines and chemokines, causing damage to periodontal tissues (Figure 4). In the present study, we found increased levels of IL-1β, MIP-1α, and MIP-1β in GCF of teeth with SSC compared to the control group. Further studies exploring the levels of other inflammatory mediators (IL-17, IL-23, IL-18, and IL-33) related to RANKL/RANK axis activation are needed to understand the dynamics of inflammation in children with SSC.
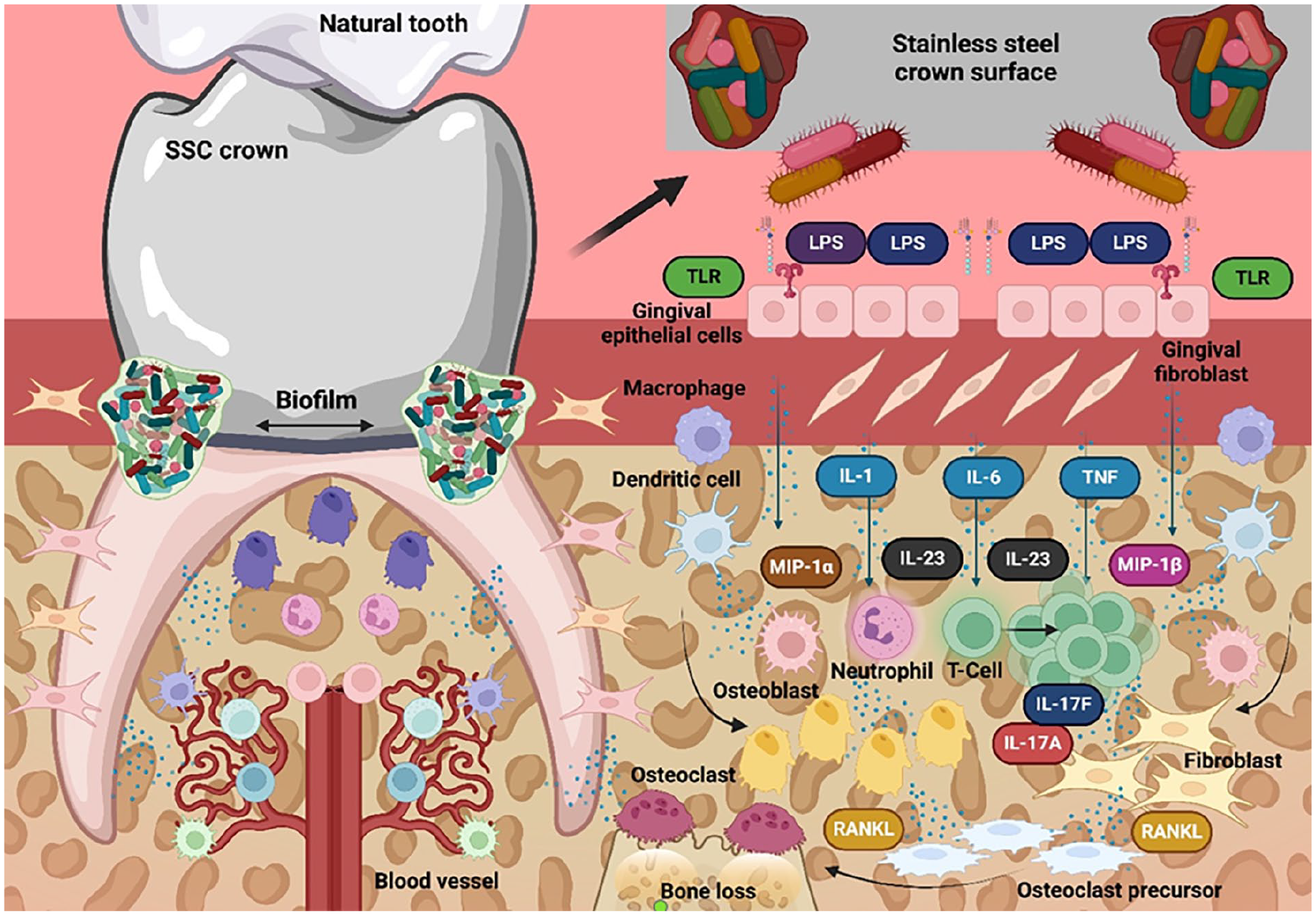
Dynamics of the inflammatory process in teeth restored with stainless steel crowns. The accumulation of bacteria between the surface of the stainless steel crown and the gingival tissue stimulates and activates gingival keratinocytes and fibroblasts. These cells release proinflammatory cytokines and chemokines such as IL-1, IL-6, IL-8, and TNF. Antigen-presenting cells such as macrophages and dendritic cells, in turn, release IL-23, CX3CL1, MIP-1α, and MIP-1β, which, on the one hand, favor clonal expansion of T cells, upregulate IL-17A/F production and attract more neutrophils to the site of inflammation and destruction. IL-17A/F interacts and binds with its receptor, favoring the production of RANKL, which in osteoclast precursors produces osteoclastogenesis and, in turn, bone resorption.
Supplemental Material
sj-pdf-1-jbf-10.1177_22808000251335403 – Supplemental material for The influence of stainless steel crowns placed on primary teeth on biochemical parameters in GCF: A systematic review
Supplemental material, sj-pdf-1-jbf-10.1177_22808000251335403 for The influence of stainless steel crowns placed on primary teeth on biochemical parameters in GCF: A systematic review by Mario Alberto Alarcón-Sánchez, Julieta Sarai Becerra-Ruiz, Ruth Rodríguez-Montaño, Sarah Monserrat Lomelí-Martínez, Luca Fiorillo and Artak Heboyan in Journal of Applied Biomaterials & Functional Materials
Footnotes
Authors’ note
Mario Alberto Alarcón-Sánchez is now affiliated to Doctor of Science in Molecular Biology in Medicine Program, University Center of Health Sciences, University of Guadalajara (CUCS-UdeG), Guadalajara, Jalisco, Mexico and Institute of Research in Dentistry, Department of Integral Dental Clinics, University Center of Health Sciences, University of Guadalajara (CUCS-UdeG), Jalisco, Mexico.
Author contributions
Conceptualization, M.A.A.-S, R.R.-M, J.S.B.R, and S.M.L.M.; methodology, M.A.A.-S. and A.H.; software, M.A.A.-S.; validation, M.A.A.-S, L.F., R.R.-M, J.S.B.R, S.M.L.M, and A.H.; formal analysis, M.A.A.-S, R.R.-M, J.S.B.R, L.F. and S.M.L.M.; investigation, M.A.A.-S, R.R.-M, J.S.B.R, and S.M.L.M.; resources, M.A.A.-S, R.R.-M, J.S.B.R, and S.M.L.M.; data curation, M.A.A.-S.; writing—original draft preparation, M.A.A.-S, R.R.-M, J.S.B.-R, and S.M.L.M, writing—review and editing, M.A.A.-S, R.R.-M, J.S.B.R, S.M.L.M, L.F. and A.H.; visualization, M.A.A.-S, R.R.-M, J.S.B.R, S.M.L.M, L.F.and A.H.; supervision, M.A.A.-S, L.F. R.R.-M, J.S.B.R, S.M.L.M, and A.H.; project administration, M.A.A.-S, and A.H. All authors have read and agreed to the published version of the manuscript.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data supporting this study’s findings are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.