
Abstract
Aim:
The aim of the study was to investigate the shear bond strength (SBS) and compressive strength (CS) of Er Cr YSGG laser (ECL) treated, re-bonded lithium disilicate (LD) ceramic in comparison to standard conventional conditioning (hydrofluoric acid (HFA) and silane).
Methods:
One hundred LD ceramic disks were divided equally for SBS and CS testing. Eighty samples were conventionally surface treated and bonded to resin cement followed by de-bonding of the cement build-up. All de-bonded specimens were divided into four groups based on re-bonding surface treatments (HFA, primer, adhesive, and ECL). Resin cement build-ups were performed in 40 specimens for SBS testing (universal testing machine); however, the remaining 40 specimens were tested for CS. Ten specimens each were used as controls (surface treatment was performed once and no primary resin cement bonding) for SBS and CS assessment. Surface topography was assessed using a scanning electron microscope.
Results:
The maximum and minimum SBS values were shown by groups: control (33.42 ± 3.28 megapascals (MPa)); and ECL (17.50 ± 2.22 MPa) respectively. The maximum and minimum CSs were displayed by specimens in the ECL group (439.45 ± 70.68 MPa) and the control group (237.28 ± 19.96 MPa), respectively. For ECL specimens, SBS was significantly lower and CS was significantly higher as compared to control specimens.
Conclusions:
Application of the Er Cr YSGG laser significantly improved the CS of de-bonded ceramic specimens. However, it did not show a positive influence on the bond integrity of re-bonded ceramics in comparison to conventional surface treatment regimes.
Introduction
Ceramics have revolutionized esthetic dentistry and modern veneers made from ceramics are a major tool in smile reconstructions. In esthetic dentistry, creating a life like smile is a continuous challenge which is dependent on factors including, tooth substrate, ceramic type, luting cement, shade matching, and technical expertise.1–3 Providing a satisfying smile appearance with an acceptable shade is susceptible to error as it depends on operator experience in shade matching and patients’ perception of tooth color. 4 ) It further becomes a difficult task as high translucent ceramics are adhesively bonded to teeth, in an irreversible way. Tooth veneers of ceramic material, are surface treated to create micro-retentions and are adhesively bonded to the tooth with resin luting cements to enhance its fracture resistance. 5–6 This makes the removal of intact veneer for chipping repairs, shade improvement, and modifications difficult.
Removal of veneers for color mismatch is common, however the methods to reversibly remove veneers are not established. A common technique is the use of dental burs on a high-speed or slow-speed handpiece with copious water irrigation. However, this method presents the potential for irreversible damage and fracture of the veneers. 7 In addition, it also risks thermal damage and physical iatrogenic loss of tooth structure (enamel), which is critically required for predictable adhesive ceramic bonding. 8, 9 A contemporary alternative is the use of erbium lasers used at 2780–2940 nm for two minutes (mins) with continuous motion for de-bonding indirect tooth veneers. 7, 10, 11 It is proposed that the laser wavelength is absorbed in the water content of luting cement resulting in a softening effect on the cement. Thereafter the veneer can be removed mechanically. 7
The Er Cr YSGG laser is increasingly being employed for dental therapeutic applications including, caries removal, cavity preparations, surface treatment of tooth, soft and hard tissue therapies, tooth whitening gel activations, and periodontal disinfection. 12–14 The Er Cr YSGG laser works on the principal of micro explosion during tissue ablation resulting in microscopic and macroscopic irregularities, and softening of luting cement. 15 As an established technique for veneer removal, it avoids the physical contacts with veneers, therefore minimizing fracture risk. In addition, it has shown to be an effective conservative option reducing the damage to tooth structure. 7
Re-bonding of de-bonded ceramic includes cleaning and removal of existing resin (heat treatment) followed by ceramic conditioning and primer application prior to re-cementation. 16 The commonly used conditioners include hydrofluoric acid (HFA) etching and silane coupling agent. 5, 6 The Er Cr YSGG laser is also a potential conditioning therapy for conditioning of ceramics prior to re-bonding. It has been reported that the conditioning of ceramics for longer duration significantly compromises the bond strength of ceramics to resin. 17, 18 As lasers generate ceramic structural changes, a similar effect of the Er Cr YSGG laser on the ceramic surface bond integrity and strength prior to re-bonding may occur. Therefore, it is hypothesized that ceramic surface treatment with the Er Cr YSGG laser for re-bonding of ceramics will significantly influence its bond integrity and compressive strength (CS). The aim of the study was to investigate the shear bond strength (SBS) and CS of Er Cr YSGG laser treated, re-bonded lithium disilicate ceramic in comparison to standard conventional conditioning (HFA and silane) techniques.
Methods
The present in-vitro study was approved by the College of Dentistry Research Center at King Saud University. The study followed the Checklist for Reporting In-vitro Studies guidelines.
Specimen preparations and de-bonding
One hundred lithium disilicate (LD) (Emax, Ivocalr Vivadent, Schaan, Liechtenstein) ceramic disks (5 mm × 2 mm) were fabricated using the hot press technique. Ceramic surfaces were cleaned in an ultrasonic bath with distilled water for 10 mins. The specimens were embedded in orthodontic clear acrylic resin (Caulk, Dentsply, York, Pennsylvania) within polyvinyl chloride (PVC) pipe sections with exposed flat surfaces. The specimens were polished and finished with 1000-grit silicon carbide paper. The specimens were washed with a high-pressure steam gun for 30 seconds (secs) (3.5 Bar pressure, Steam Cleaner, Reliable, 5000CD). Twenty specimens were used as controls. The bonding surface of 80 embedded specimens was exposed to 5% HFA etch (5%) (IPS® Ceramic Etching Gel-Ivoclar Vivadent, Schaan, Liechtenstein) for 20 secs followed by washing for 2 mins and drying for 20 secs. The specimen surfaces were treated with ceramic primer (Rely X ceramic primer-3M ESPE, StPaul, MN, USA) with a microbrush and allowed to dry. Two coats of adhesive (Adper Single Bond Plus adhesive) were applied and dried gently for 10 secs and light cured (Bluephase, Ivoclar Vivadent, Schaan, Liechtenstein) for 10 secs. A build-up of resin cement, Variolink Esthetic (Ivocalr Vivadent, Schaan, Liechtenstein) (3 × 3 mm) using a putty mold was performed with a plugger and plastic instrument on ceramic specimens. The build-up was light cured (Bluephase, Ivoclar Vivadent, Schaan, Liechtenstein) for 40 secs from the top and 40 secs from four directions after mold removal. All 80 specimens received build-ups with a same procedure. All specimens were placed in a universal testing machine (Instron 5965 Material Testing System) with the adhesive interface perpendicular to the floor. An increasing load was applied with a chisel (0.5 mm/min cross-head speed) on the cement close to the interface until failure.
SBS testing and study groups
All (80) de-bonded ceramic specimens were warmed in an oven at 100°C (1 min) and resin tags were removed using an excavator. The specimens were further cleaned in an ultrasonic bath for 5 min in distilled water. Forty de-bonded specimens were divided into four groups (N = 10) based on the re-bonding regime (Groups 2S–5S), while 10 specimens (out of 20 control specimens that did not undergo previously mentioned bonding and de-bonding procedures) served as a control group (Group 1S) with the following bonding regime:
Group 1S (control): Untreated ceramic specimens, were etched with HFA (5%) 20 secs (washed (2 mins) and dried (20 secs)), ceramic primer application (Rely X ceramic primer-3M ESPE, St Paul, MN, USA), two coats of adhesive (Adper Single Bond Plus adhesive) followed by light curing (10 secs) and build-up of resin cement Variolink Esthetic (Ivocalr Vivadent, Schaan, Liechtenstein) (3 × 3 mm) using a putty mold and photo-polymerization (Bluephase, Ivoclar Vivadent, Schaan, Liechtenstein). The bonding procedure for the specimens of the control group was the same as for 80 specimens that undergo bonding and de-bonding procedures.
Group 2S: De-bonded ceramic specimens were treated with ceramic primer and adhesive followed by resin cement build-up.
Group 3S: De-bonded ceramic specimens were treated with adhesive followed by resin cement build-up.
Group 4S: De-bonded ceramic specimens were retreated with HFA (5%), ceramic primer, and adhesive followed by resin cement build-up.
Group 5S: De-bonded ceramic specimens were retreated with Er Cr YSGG laser (ECL) (Biolase, Waterlase I-Plus laser (Biolase, Irvine, CA, USA) frequency 50 Hz and 4.5W) ceramic primer and adhesive followed by resin cement build-up. All specimens were stored in distilled water at 37°C for 24 hours.
All specimens were placed in a universal testing machine (Instron 5965 Material Testing System) with the adhesive interface perpendicular to the ground. An increasing load was applied with a chisel (0.5 mm/min cross-head speed) on the cement close to the interface until failure. The failure load (N) was recorded, and the SBS (σ, megapascals (MPa)) was calculated as: σ = L/A, where L is the load recorded and A is the bonding area (mm2).
CS assessment
Forty de-bonded (cleaned) and dried specimens were divided into four groups (N = 10) on the basis of surface treatments for re-bonding (Groups 2C–5C), while 10 specimens, (out of 20 control specimens) serving as a control group (Group 1C), have been treated as follows:
Group 1C (control): Untreated ceramic specimens, were etched with HFA (5%) 20 secs (washed (2 mins) and dried (20 secs)), ceramic primer application (Rely X ceramic primer-3M ESPE, StPaul, MN, USA), and two coats of adhesive (Adper Single Bond Plus adhesive) followed by light curing (40 secs).
Group 2C: De-bonded ceramic specimens were treated with ceramic primer and adhesive followed by light curing (40 secs).
Group 3C: De-bonded ceramic specimens were treated with adhesive followed by light curing (40 secs).
Group 4C: De-bonded ceramic specimens were retreated with HFA (5%), ceramic primer, and adhesive (light cured).
Group 5C: De-bonded ceramic specimens were retreated with ECL (Biolase, Waterlase I-Plus laser (Biolase, Irvine, CA, USA) frequency 50 Hz and 3.5W) ceramic primer, and adhesive (light cured).
Specimens were tested for maximum failure loads before fracture after 1 hour (stored at room temperature in Memert Universal Oven – 25°C), employing a universal testing machine (Instron 5965 Material Testing System) at a cross-head speed of 0.5 cm/min. The applied loads were in the center of disk specimens with a conical round-ended metal probe creating stresses in the middle. CS was calculated using the formula UCS = 4f/πd2. Where f was the load in Newton (N), and d the diameter of the cylindrical specimen in millimeters.
Failure analysis was performed using a digital microscope (Hirox-KH-7700) and scanning electron microscopy (SEM) for all specimens. Failures were classified into adhesive (at the ceramic–resin interface), cohesive (failure in the resin cement), and admixed failures (partly in resin cement and partly at the ceramic–resin interface). Four LD ceramic specimens for each surface treatment were fabricated and assessed for surface topography using SEM (JEOL JSM-6360 LV Scanning Electron Microscopy, JEOL USA, Inc.). Specimens were mounted on acrylic stubs after gold coating (JFC – 1100 fine coat ion sputter) and were assessed by a single operator. All data were compiled using the Statistical Package for the Social Sciences (SPSS-Version 20, Chicago, IL, USA) software, and data were assessed using two-way analysis of variance (ANOVA) and post hoc multiple comparisons.
Results
In order to evaluate the influence of ceramic re-bonding surface treatments on its SBS to resin cement, five study groups were investigated. SBS values are presented in Table 1. The control group (Group 1S) showed significantly higher SBS values compared to all experimental groups (p < 0.05). The maximum and minimum SBS values were shown by Groups 1S (control) (33.42 ± 3.28 MPa) and 5S (ECL) (17.50 ± 2.22 MPa), respectively. Ceramic groups’ specimens among Groups 2S (prime and adhesive) (25.08 ± 2.49 MPa), 3S (adhesive only) (23.50 ± 4.39 MPa), and 4S (HFA) (23.73 ± 4.78 MPa) showed comparable outcomes (p > 0.05). Specimens exposed to ECL treatment for re-bonding showed significantly lower SBS (17.50 ± 2.22 MPa) in comparison to all study groups (p < 0.05). Overall, SBS among the study groups showed a statistically significant difference (p < 0.05), indicating a significant influence of the re-bonding ceramic surface treatment regimes.
Means and standard deviations (SDs) of shear bond strength among study groups.

Notes: * comparison of groups using analysis of variance. Groups with similar superscript letters are comparable (Tukey post hoc test).
For assessing the influence of the re-bonding regime on the CS of the treated ceramics, five groups were compared. The maximum and minimum CSs were displayed by specimens in Groups 5C (ECL) (439.45 ± 70.68 MPa) and 1C (control) (237.28 ± 19.96 MPa), respectively (Table 2). CS for the control group specimens was comparable to experimental Groups, 2C, 3C, and 4C (p > 0.05). CSs among the specimens treated with primer and adhesive (Group 2C) (273.61 ± 24.64 MPa), adhesive alone (Group 3C) (245.51 ± 25.03 MPa), and HFA (Group 4C) (280.77 ± 33.14 MPa) were also statistically comparable (p > 0.05). Specimens among Group 5C (ECL) showed significantly higher CSs in comparison to all study groups (p < 0.05). The overall comparison among all study groups for CS showed statistically significant difference (p < 0.05: ANOVA), suggesting a significant influence of re-bonding surface treatments on the strength of LD ceramic specimens.
Means and standard deviations (SDs) of compressive strength among study groups.

Notes: * comparison of groups using analysis of variance. Dissimilar superscript letters denote significant difference (Tukey post hoc test).
The SEM analysis showed the influence of different surface treatment on the ceramic surface. Treatment with HFA revealed micro and macro irregularities in the form of exposed LD crystals (Figure 1). Specimens treated with Er Cr YSGG laser showed localized superficially sintered spots with unaffected areas throughout the treated specimen surface (Figure 2). Overall, HFA treated samples showed a high energy, irregular and favorable bonding surface compared to laser treated specimens showing localized modifications only.

Micro surface and macro surface irregularities in the form of exposed lithium disilicate crystals (scanning electron microscopy).
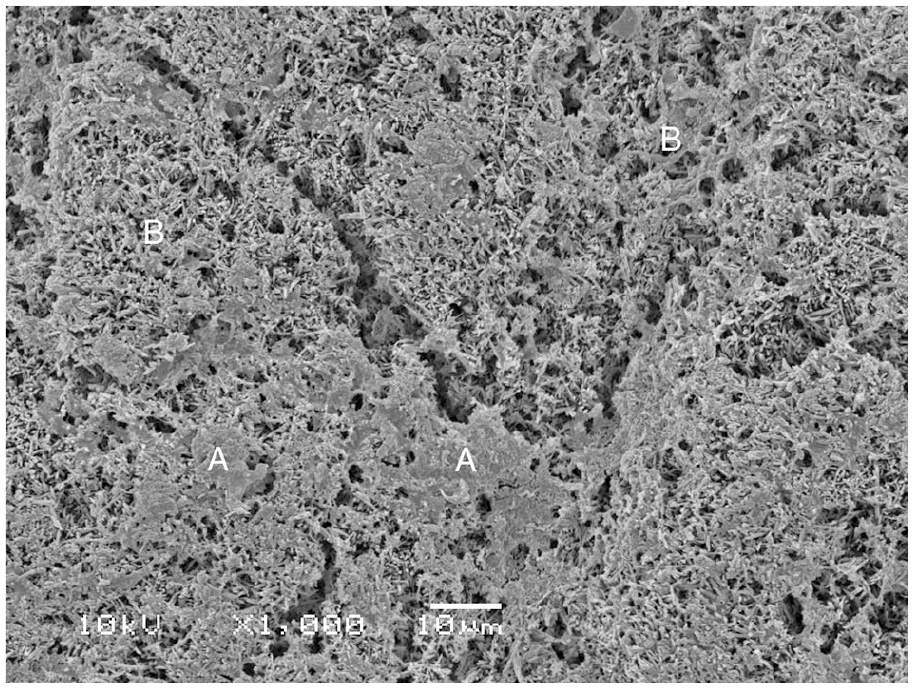
Localized superficially sintered spots: (A) with unaffected areas; and (B) throughout the treated specimen surface (scanning electron microscopy).
A summary of failure modes is presented in Table 3. A majority of the failures (50% to 100%) among all groups were adhesive type (Figure 3). Cohesive failures (Figure 4) comprised of less than 5% of overall failures among study groups, that is, 20% each among Groups 4S and 5S respectively. The incidence of admixed type failures (Figure 5) was high among the ECL group (Group 5C) (30%) and Group 4S (40%).
Mode of failure among different experimental groups.


Specimen for Group 1S showing adhesive failure at resin interface (scanning electron microscopy).
Specimen for Group 4S showing cohesive failure in the resin cement (scanning electron microscopy).

Specimen for Group 5S showing admixed failure (parts of interface show adhesive and cohesive type failures) (scanning electron microscopy).
Discussion
The present study was based on the hypothesis that LD ceramic surface treatment with the Er Cr YSGG laser for re-bonding to resin will significantly influence its bond integrity and CS. The hypothesis was accepted as the Er Cr YSGG laser treatment on de-bonded LD ceramics showed a significant reduction in bond strength to resin cement in comparison to the control group. In addition, the CS of the Er Cr YSGG laser treated de-bonded specimens significantly improved as compared to the other experimental groups.
Re-bonding of veneers fabricated with ceramic to tooth dentin is potentially challenging due to the presence of remaining cement on the ceramics and adhesive bond integrity is compromised for re-bonded restorations. 19 In the present study, bond strength of de-bonded specimens with various surface treatments including HFA, silane primer, and/or adhesives were compared to Er Cr YSGG laser conditioned specimens and those from the control group. Interestingly, HFA, silane primer, and adhesive used in various combinations, produced comparable bond strength outcomes. Silane primer is primarily used to improve the surface energy of ceramics for better adhesive and resin penetration; however, the adhesive seals the surface micro-irregularities on ceramics due to its low viscosity along with improving resistance of interface from moisture at a relative humid environment. 20 A possible explanation for these findings may be derived from the fact that the ceramic surface of de-bonded specimens had infiltrations of resin cement from the primary cementation procedure. These resin tags occupied the surface irregularities produced from the primary etching procedure. A heat treatment is recommended in the literature 16 to burn out the resin on the surface of de-bonded ceramic specimens. Although, in the present study the specimens were placed at 100°C for 1 min, this heat treatment may not have been effective in removing the resin tags and achieving a highly wet-able surface topography. In addition, surface etching to re-create a favorable surface topography of de-bonded ceramics was performed with HFA for 20 secs. 5, 21 However, HFA treatment failed to show outcomes similar to control specimens. As duration of HFA etching is known to influence the surface topography and critical bond strength of ceramics, the authors hypothesize that a longer duration of HFA etching for 1 to 2 mins for re-bonding of ceramics may reveal acceptable bond strengths.
In the present study, the Er Cr YSGG laser failed to show an improvement in bond strength for re-bonded specimens in comparison to conventionally treated or control specimens. The Er Cr YSGG laser has been employed in surface treatment of bonding ceramics with mixed success. 12, 14, 15 It has shown to produce micro ablations resulting in short bursts of temperature hike causing ceramic surface heat vaporization. 22 These laser applications act as localized selective sintering at high power temperatures resulting in macroscopic and microscopic irregularities. 15 It was expected that the micro ablation effect of the laser would be able to eliminate existing resin tags on the ceramic surface in preparation for re-bonding and re-cementation of ceramics. It is pertinent to mention that the ablative effect of the Er Cr YSGG lasers is dependent on multiple laser parameters including, power, wavelength, tip aperture diameter, duration, and number of laser applications. 23 Evidence suggests, LD ceramic specimens treated with 600 to 900 mJ erbium-doped yttrium aluminum garnet lasers showed significantly lower bond strengths as compared to surface treatment with 300 mJ. 24 . In the present study, a single laser (Er Cr YSGG) application (1 min) with a MZ- 6 diameter tip at frequency of 50 Hz and 3.5W power was performed. As laser parameters have been known to influence the precise outcomes of Er Cr YSGG lasers applications, 15 it is suggested that repeated applications with low frequency high power lasers with a wider diameter (MZ-8) tip and longer durations will be more effective in improving the bond integrity of re-bonded ceramic specimens (B, C, and D). Moreover, SEM analysis of lased ceramic specimens showed localized re-sintering of ceramic surface with relatively minor irregularities. Therefore, it is recommended that the Er Cr YSGG laser should be used for resin removal, and the use of HFA may be combined with it to provide a high-energy surface topography, favorable for micro retentive resin tags for re-bonding.
In the present study laser treated specimens showed higher CS as compared to controls. It has been suggested in the literature that surface treated ceramics when bonded using resin cements (BIS-GMA) show significantly higher fracture resistance as compared to cementation using conventional acid-based cements (glass ionomers). 25 Luting resin infiltrates the surface treated ceramics creating resin tags for retention and re-enforces the brittle ceramics in the process, resulting in a robust ceramic restored complex. 26 In the present study re-bonded specimens had infiltrations of resin tags from the primary luting procedure, which was missing in the control specimens. This resin re-enforcement of ceramic surface resulted in the higher CSs of lased specimens. In addition, lased specimens revealed localized spots of sintered surface, as glaze and heat treatments of a ceramic surface are known to influence ceramic surface properties (Figure 2), this is a likely explanation for the improved CS for ceramic specimens. 27
The findings of the present study should be interpreted in light of the study limitations. In modern dentistry, multiple ceramics (LDs, leucites, and zirconia-based) and lasers are employed for treatment procedures – the findings in this study should only be attributed to the LD ceramics and the Er Cr YSGG lasers. In addition, actual CSs observed in the study are not representative of veneer strengths used in clinical dentistry as the thickness of specimens were greater (2 mm) than the clinical veneers (0.7 mm to 1 mm). The surface treatments employed in the study along with heat treatment failed to completely remove the resin from de-bonded ceramics, therefore further studies with treatments at higher temperatures and modified laser parameters are recommended.
Conclusions
Application of the Er Cr YSGG laser significantly improved the CS of de-bonded ceramic specimens. However, it did not show a positive influence on the bond integrity of re-bonded ceramics in comparison to conventional surface treatment regimes.
Footnotes
Contributorship
AMA and RA: Data collection, study design, manuscript writing, and final manuscript approval.
TA and FV: Data collection, study design, manuscript drafting, data analysis, and manuscript approval.
AH and RA: Data collection, manuscript approval, and data interpretation
MA and AA: Data collection, writing, revising, editing, and final manuscript approval
LA and KA: Performed experimental testing, revisions of manuscript, manuscript approval, and data collection.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors are grateful to the Researchers supporting project at King Saud University for funding through Researchers supporting project No. RSP-2019-44.
Guarantor
Tariq Abduljabbar (TA).