
Abstract
Objective:
To evaluate the effects of three different curing units on the physical and mechanical features of three different orthodontic adhesive resin materials.
Material and Methods:
45 specimens (5 mm in diameter, and 2 mm in thickness) of each of the three different adhesive composite resin materials (Transbond XT, Grēngloo™ Adhesive and Light Bond Paste) were cured with three different light units (a polywave third generation (Valo), a monowave (DemiUltra), and a second-generation LED (Optima 10)). To quantify degree of conversion (DC), the Attenuated Total Reflectance Fourier Transform Infrared Spectroscopy was used in transmission mode (ALPHA FT-IR Spectrometer, Bruker Optics, Germany). Vickers hardness value was recorded under constant load 100 g for 10 s with a microhardness tester (HMV M-1, Shimadzu Corp., Kyoto, Japan). The data were statistically analyzed using Kruskal-Wallis and chi-square tests. The level of significance was considered p < 0.05.
Results:
The highest DC values were obtained as a result of curing with Optima 10. This rate was followed by Demi Ultra and Valo, respectively. Transbond XT samples showed a lower level of conversion than the samples of Light Bond Paste and Grēngloo™ Adhesive. The top surfaces of each material showed higher hardness values than the bottom surfaces (p < 0.05). The Light Bond Paste showed the highest hardness values both on the top and bottom surfaces among the three materials, followed by Grēngloo™ Adhesive. While the hardness values of the top surfaces of the samples cured with Demi Ultra and Valo light units were similar, higher hardness values are recorded with Valo on the bottom surfaces (Valo; 85.200/75.200 (top/bottom) versus Demi Ultra; 86.100/66.000 (top/bottom)).
Conclusions:
The different DC and the surface hardness properties were recorded for the resin as orthodontic adhesives depending on different light units. Shorter radiation time caused lower DC and surface hardness values.
Introduction
In material science, composites are resin materials made from two or more substances that, when combined, produce a material with characteristics different from the individual components. In early 1960s, the word “composite” had been introduced to the dental nomenclature. 1 Dental composites are types of synthetic resins typically composed of three distinct phases: an organic matrix (polymerizable resin-based oligomer matrix, such as a bisphenol A-glycidyl methacrylate (BISGMA) or urethane dimethacrylate (UDMA)), an inorganic matrix (filler, such as silicon dioxide (silica)), and a coupling agent (such as silane, to enhance the bond between the two other components). 2
An initiator begins either the chemical or light polymerization reaction of the resin phase. The resin phase is composed of monomers that convert to a crosslinked polymer with polymerization reaction. A critical feature of the light curing composites is its polymerization. The degree of polymerization is determined by the proportion of the remaining concentration of the double carbon bonds in a polymerized sample relative to the total number of double carbon bonds in the uncured material. The degree of conversion (DC) directly affects the chemical, physical, and mechanical properties of the composites and higher degree of conversion indicates greater amount of polymerization. 3
The quality of the polymerization of resin composite materials used as orthodontic adhesives has been widely studied and there is a continuous attempt to fabricate new light sources that promise effective conversion of monomers in polymers, so that the material has appropriate clinical performance.4–6 In a paper by Mangat et al. the light sources were classified under five groups according to their evolution; 1st Generation: Ultra-Violet (UV) Light, 2nd Generation: Visible Light Units (halogen curing lights-QHT), 3rd Generation: Plasma Arc Units (PAC), 4th Generation: Light Emitting Diodes (LED), 5th Generation: Lasers. 7
In the early 1980s, the quartz tungsten halogen curing light (QHT) replaced the UV curing light since the latter had longer wavelengths allowing greater penetration and having no harmful effects on the surrounding tissues. Despite their disadvantages such as their limited effective lifetime due to the degradation of the bulb’s components and the necessity of relatively long exposure time (20–40 seconds), the halogen bulbs are still commonly used in dentistry. 8 As a result of the latest advancements in technology, gallium nitride blue light-emitting diodes (LED) curing units have been available on the market and they were promising faster and deeper curing. They presented the advantages of being more lightweight, do not require a fan to cool, and their energy does not decrease over time. 9 Besides the new technologies in the field of light unit technologies, considerable efforts have been made to develop new material systems with different chemical composition that may provide better polymerization properties. 10 Different methods such as pre-heating composite prior to light-curing or using laser beams are some of the promising methods to polymerize the composite materials.11–13 The results of two recent studies showed a very high potential of diode-pumped solid-state lasers to be used in endodontics, orthodontics, and restorative dentistry since similar mechanical properties were obtained compared to the conventional LED-polymerized composite samples.12,13
In orthodontics, light units were used for many years to cure resin-based adhesive composite materials and resin-modified glass ionomers to bond orthodontic attachments to the tooth surface. Regarding all kinds of light-curing systems, QTH lamps have long been predominant in dental practice.9,14 In 1995, Mills was the first to suggest the use of LED in orthodontics. 15 While LED curing is a crucial step forward, refinements are being developed with the goal of faster and more powerful curing.
The newest high powered (HP) LED curing unit is an updated version that cures material much faster than the QTH lamps and the previous LED curing unit. The new HP LED curing units are promoted to reduce the curing time dramatically, thus reducing the chair time and increasing the patient comfort. Despite the multiple advantages of LEDs, it is important to know exactly the curing potential of these light devices with increasing importance on the market. Some studies have been performed to evaluate the mechanical properties of the resin-based composite materials cured with LEDs. However, very few studies have investigated the degree of conversion (DC) which is determined by the chemical transformation of the polymer and there is need of further scientific research in this field.
In this study, we aimed to evaluate the effect of three different light units on the physical and mechanical features of three different adhesive composite resin materials by using Attenuated Total Reflectance Fourier Transform Infrared Spectroscopy and Vickers surface hardness test.
Material and methods
Specimen preparation
Three different adhesive materials were used in this study. The compositional information about these materials is given in Table 1.
Compositional information about the adhesive materials.

To prepare the specimens, uncured resin materials were poured into polytetrafluoroethylene (Teflon®, PTFE) molds of 5 mm in diameter and 2 mm in thickness. The molds were covered with Mylar Strip and placed between two layers of 1 mm-thick laboratory glasses. The 15 specimens of each material were randomly separated into three groups and cured with three different light units. The manufacturers’ guides were followed to use these light units which are given in Table 2.
LED light units and curing protocols applied in this study.

Subsequent to application of curing protocol, a total of 45 disc-shaped specimens were stored in separate dark containers containing distilled water at room temperature for 24 h prior to testing.
Microstructural characterization by Fourier Transform Infrared Spectroscopy
The Attenuated Total Reflectance (ATR) Fourier Transform Infrared Spectroscopy (FT-IR) was used in transmission mode (ALPHA FT-IR Spectrometer, Bruker Optics, Germany). The spectra were recorded using a germanium crystal, within a wavenumber range of 400–4000 cm−1 with a resolution of 2 cm−1 from 32 scans. The spectra were imported via OPUS (Bruker, Germany) and analyzed with the Origin v8.0 software (OriginLab Corporation, Northampton, Massachusetts, USA).
To quantify DC% we used the intensity of the characteristic absorption peak of the unsaturated aliphatic C=C double bond originated from the methacrylate group at 1636 cm−1 and that of aromatic C=C double bond at 1604 cm−1 with the following equation 16

Peak areas were used to calculate the DC values rather than peak intensity and, in the equation, “ac” and “bc” represent conditions of “after curing” and “before curing.” The given part of the spectrum in this range was fitted multipeaks by using the Gaussian non-linear peak deconvolution function of OriginPro 8.0 software then the area of each corresponding peaks was calculated. Between each set of monomer/polymer spectrum measurements, the crystal plate was cleaned with a soft absorbent paper and ethyl alcohol and dried with an air blower. 17
Mechanical characterization by Vickers hardness test
The surface of the samples was polished using 400, 800, 1000, 1500, 2000, 2500 grit silicon carbide paper. Vickers hardness value was recorded under constant load 100 g for 10 s (Vickers pyramid: diamond right pyramid with a square base and an angle of a = 136°) with a microhardness tester (HMV M-1, Shimadzu Corp., Kyoto, Japan). Measurements were performed five times on the top and bottom surfaces; one in the center and one in every quadrant. The mean value was reported as Vickers Hardness value.
Statistical analysis
The data were statistically analyzed using SPSS 20 software and Kruskal-Wallis, chi-square tests. The level of significance was considered p < 0.05.
Results
Microstructural characterization by Fourier Transform Infrared Spectroscopy
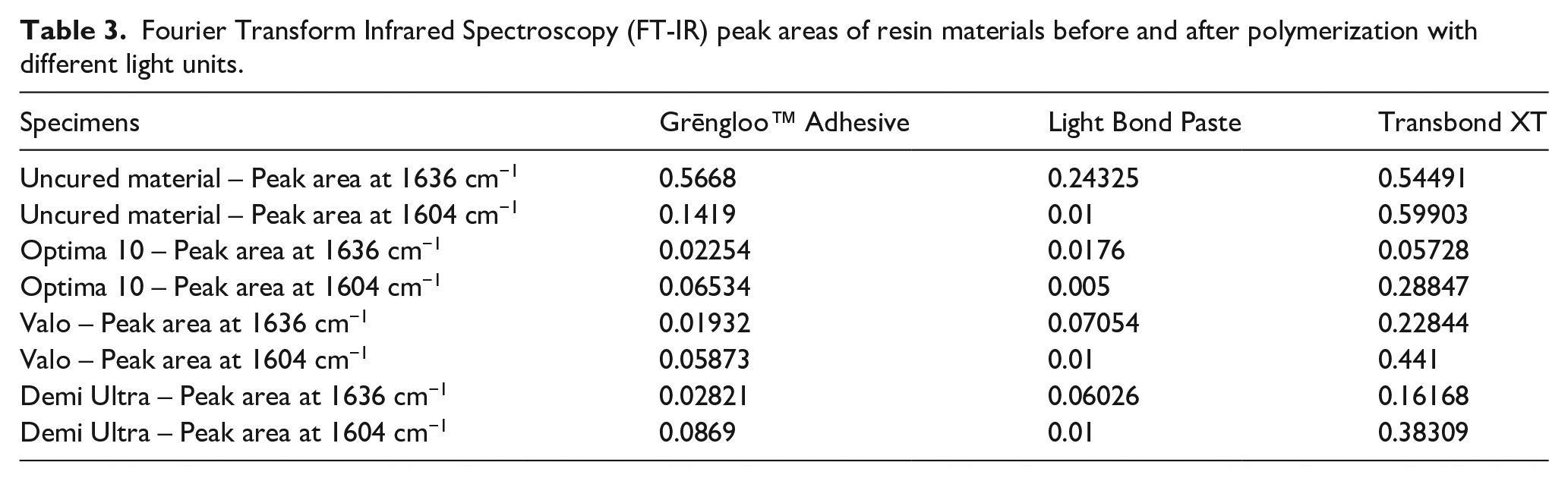
The FT-IR spectra of uncured resin specimens cured with the Optima 10, Valo, and Demi Ultra light units within a narrow range of wavenumber (1575–1800 cm−1) are given in Figures 1(a) to (c). The FT-IR peak areas at 1636 and 1604 cm−1 of the materials before and after polymerization are listed in Table 3. It was found that the DC values of the samples changed with different light units (Table 4). The highest DC values were obtained as a result of curing with Optima 10. This rate was followed by Demi Ultra and Valo respectively. In addition, Transbond XT samples showed a lower level of conversion than the samples of Light Bond Paste and Grēngloo™ Adhesive, when we compared the DC values.

Representative Fourier Transform Infrared Spectroscopy (FT-IR) spectra of Grēngloo™ Adhesive before (—) and after (– – –) irradiation by light sources respectively (a) Optima 10, (b) Valo, (c) Demi Ultra.
Fourier Transform Infrared Spectroscopy (FT-IR) peak areas of resin materials before and after polymerization with different light units.
Degree of conversion (DC%) values of samples.

Mechanical characterization by Vickers hardness test
The comparison of the top and bottom surfaces’ hardness values of each material depending on the curing unit is presented in Table 5. As it might be expected, the top surfaces of each material showed higher hardness values than the bottom surfaces. Statistically significant difference was found among the top and bottom surfaces’ mean hardness values of these adhesive resin materials (p < 0.05). The Light Bond Paste showed the highest hardness values both on the top and bottom surfaces among the three materials, followed by Grēngloo™ Adhesive. In addition, the top and bottom surfaces hardness values of Light Bond Paste cured with different light units showed significant differences (p < 0.001). The highest hardness measurements for Light Bond Paste were obtained with Optima 10 on both upper and lower surfaces. While the hardness values of the top surfaces of the samples cured with Demi Ultra and Valo light units were similar, higher relative hardness values are recorded with Valo on the bottom surfaces (Light Bond paste Valo; 75.200/85.200 (bottom/top) versus Demi Ultra; 66.000/86.100 (bottom/top)). The Grēngloo™ Adhesive samples cured with Valo and the Light Bond Paste samples cures with Demi Ultra-light units did not provide the bottom/top ratio ⩾80% criteria. 18
Intragroup comparison of the top and bottom surfaces’ hardness values depending on the curing unit.

The top surfaces of Transbond XT and Grēngloo™ Adhesive samples cured with different light units showed no intra group statistically significant difference; however, significant difference was found for the bottom surfaces. Higher values on the bottom surface were recorded with the samples cured with Optima 10 for both Grēngloo™ Adhesive and Transbond XT.
Discussion
In the present study, we evaluated the effect of three different light units on the physical and mechanical features of different composite resin materials which are used as adhesives in the field of orthodontic dentistry.
Usually, the light output required for polymerization varies between 360 to 500 nm and more specifically for camphorquinone, which is the most often used photo-initiator in resin composites, the optimum absorption occurs near the wavelength of 470 nm. 19 Therefore, in the present study we preferred three different light units having wavelength range covering the absorbance wavelength of camphorquinone.
Knowing the physical structure and the chemical features of a resin material makes it possible to explain their mechanical behavior. The quality of polymerization is of great importance since it is one of the factors promising the optimum clinical performance of the resin material. The DC is a critical feature in evaluating the polymerization performance since it is determined by the proportion of the double carbon bonds in a polymerized material relative to the total number of double carbon bonds in the uncured sample.
There are several methods to determine the DC of light curing materials. FT-IR is one of these methods and has been proven to be powerful and reliable.16,20 Although the polymerization of the light curing orthodontic composite adhesives has been studied using FT-IR analysis in a few studies, the effect of brand-new high-power light units on the polymerization is not well known. In the present study, the unsaturated aliphatic C=C double bond related to the methacrylate group at 1636 cm−1 and that of the aromatic C=C double bond at 1604 cm−1 was used to determine the degree of conversion (DC%) as previously described in the literature. 16
In the literature, the photopolymerization process is related to the type of the photoinitiator, viscosity, exposure duration, and the energy absorbed by the resin. 21 The total emitted energy by the curing unit is calculated by the multiplication of the light intensity by the time of exposure. 22 A radiant exposure within the 16–24 J/cm2 range is reported to be necessary in order to obtain adequate cure with a 2 mm increment resin-based composite material.21,23,24 In our study, the highest DC values were obtained as a result of curing with Optima 10 followed by Demi Ultra and Valo. Considering the total energy concept, higher DC is expected to occur with Optima 10 (1200 mW/cm2 × 20 s). However, the lower DC recorded with Valo (3200 mW/cm2× 6 s) compared to Demi Ultra (1300 mW/cm2 × 10 s) can be associated with the time variable rather than the total energy concept (18 J/cm2 versus 13 J/cm2). These results support the previous studies, suggesting that there is a minimum efficient curing time for the polymerization of composite materials. Mavropoulos et al. tested the concept of total energy and they demonstrated that this hypothesis indeed does not hold for orthodontic light-curing bracket bonding materials. 25 In a recent study, Masood et al. evaluated the DC for Transbond XT using variable curing durations with 1600 mW/cm2 light intensity and aimed to determine the effect of the tested curing durations on shear bond strength of the material with ceramic brackets. 26 They found that 6- and 9-seconds curing showed significantly higher shear bond values and better DC when compared to the 3 seconds curing, whereas no significant difference was recorded between the 6- and 9-seconds curing. In this study, the authors concluded that in actual fact, while bonding the ceramic brackets, the irradiation should at least last 6 seconds instead of 3, as advised by the manufacturer. The closest beam device used in our study was Demi Ultra (1300 mW/cm2 × 10 s) and we recorded only 53.6% DC for the Transbond XT. On the other hand, Masood et al. (1600 mW/cm2 × 9 s) recorded up to 80% DC for the same material. The difference between these results might be related to the fact that we analyzed samples of 2 mm thickness and Masood et al. evaluated a much thinner material, expected to cure better, bonded on a ceramic bracket mesh surface.
A study by Selig et al. evaluated the validity of exposure reciprocity using real-time degree of conversion and they demonstrated the principle of exposure reciprocity is not supported for light units providing power above 1.5 W/cm2. 27 They recommend being cautious when using irradiance levels above 1.5 W/cm2 with correspondingly shorter exposure times since it provides lesser DC compared to the same irradiance provided with longer exposures.
Although the DC is closely associated with the physical properties of the materials, no acceptable limit of DC is determined in the literature to provide acceptable clinical properties for orthodontic adhesive resin materials, even though the expected minimum shear bond strength (5.9–7.8 MPa) for brackets is documented. 28 Moreover, the contents of various adhesive materials differ, and the kinetics assessed by irradiance measurements demonstrate higher variability. 29 In studies evaluating the mechanical properties such as the shear bond strength, there is generally no information about the degree of polymerization of the materials. Even though they are polymerized under the same conditions, different branded materials can exhibit different polymerization degrees and therefore can manifest different clinical behaviors. This argument is particularly emphasized by Musanje and Darvell who suggest that manufacturers ought to supply a graph indicating the minimum acceptable exposure for each product for specified curing lamps since the calculations based on total energy delivered to guide irradiation protocols are not valid for resin-based composites. 30
In the present study, the Transbond XT showed a lower DC values than the Light Bond Paste and Grēngloo™ Adhesive. These findings are in harmony with the Vickers surface hardness test findings. The Light Bond Paste showed the higher hardness values, followed by Grēngloo™ Adhesive and Transbond XT for both top and bottom surfaces.
Some authors report that the color of the resin-based composite material affects the degree of polymerization. Koupis et al. investigated the relative curing degree of several polyacid-modified composites as a function of shade and found that the shade A2 provides greater curing degree values compared to shade A4. 31 Jafari et al. evaluated the surface hardness of different colored compomers cured with light units. They found the highest hardness with light (silver), and the least hardness with dark (blue) colored compomers. Jafari et al. explained this phenomenon with the fact that the pigments in darker colors absorb more light, thereby decreasing the depth of penetration of the light into the resin. 32 On the other hand, other studies reported better polymerization with darker materials compared to lighter counterparts.33–35 The Grēngloo™ Adhesive is a green paste with a color-change property that changes its color to a translucent color when the adhesive increases to warmer body temperatures. This feature allows easier removal of excess adhesive flash during bracket bonding before curing and facilitates cleanup of the adhesive remnants after debonding once the adhesive is cooled with air or water. 36 The highest DC and surface hardness values were recorded with Light Bond Paste and the lowest with Transbond XT, while the green pigmented Grēngloo™ Adhesive provided average values. The materials used in our study are not different colored materials belonging to the same brand but the adhesives of different brands. Therefore, the results are not comparable.
A previous study with similar methodology was performed to evaluate the physical properties of three different colored compomers cured with three different LED units. 37 The authors reported significantly lower hardness values for the top surface of the silver-colored specimens and for the bottom measurements of the gold-colored specimens, both cured with the Valo unit. The same light units were used in our study. Similarly, the lowest hardness values were obtained with Valo-cured-samples and only two of the materials cured with different light units did not provide the expected polymerization homogeneity considering the bottom/top ratio ⩾80% criteria (Grēngloo™ Adhesive samples cured with Valo and Light Bond Paste samples cured with Demi Ultra). On the other hand, in our study, higher Vickers values were measured for the orthodontic adhesives compared to those reported by Bakkal et al. for the colored compomers. As it is known, compomers have two main constituents: dimethacrylate monomers and a filler part that is similar to the glass present in glass ionomer cements. Thus, they provide the combined benefits of composites and glass ionomers. Lower mechanical characteristic values such as compressive strength and surface hardness values have previously been reported for compomers compared to composites.38,39 Lower hardness values of the compomer have been related to the low volume fraction filler and the incomplete silanization of the filler. 40
The Transbond XT has been the subject of many studies evaluating mechanical properties and it is perceived as one of the golden standard adhesive systems in orthodontics because of its ideal consistency and high clinical performance.41,42 Considering the well-known features of this material and the fact that it provided the lowest DC and lowest surface hardness values, we can assume that the shear bond strength is not dependent on the DC. This assumption is supported by Ekhlassi et al.’s study aiming to compare the shear bond strengths of two color-change adhesives (Grēngloo™ Adhesive and Transbond Plus) with the commonly used Transbond XT, and to evaluate any changes in shear bond strengths over time. 36 The samples were tested at 24 hours following polymerization; Transbond XT showed higher shear bond strength compared to Grēngloo™ Adhesive (13.7 mPA versus 11.3 mPA). In our study, the samples were also tested following 24 hours of incubation in distilled water. The lower DC resulting in lower surface hardness may be helpful in absorbing some mechanical stress. Despite the lower DC and surface hardness values, the material can still provide good clinical performance. In light of these results, we can propose that the acceptable DC level to provide the optimum clinical performance of each material should be provided within the manufacturer’s instructions. Additionally, the mechanical tests evaluating the shear bond should provide information about the DC to make it possible to compare the results more precisely.
Conclusion
In this study, the DC and the surface hardness properties of different resin composite materials which are used as orthodontic adhesives were quantified depending on different light units. Shorter radiation time caused lower DC and surface hardness values.
Footnotes
Acknowledgements
We would like to thank Dr. Zehra DURMUŞ for her assistance and guidance in this research.
Contributorship
BSY and MB researched literature and conceived the study. Both BSY and MB were involved in protocol development, writing the financial project. All the authors BSY, MB, and TZK were involved in data collection and data analysis. BSY wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript
Guarantor
BSY.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.