
Abstract
Introduction:
The technique of sealing is a widely accepted procedure for prevention of caries. The aim of our in vitro study was to compare the effect of two different curing units (traditional LED source and innovative laser diode lamp) on the integrity of fissure sealant material and its interface with tooth enamel.
Materials and methods:
Sixty healthy third molars were randomly assigned to two groups. In group A were teeth intended for polymerization by LED B lamp, and group B comprised teeth to be polymerized by an innovative laser diode. Both groups were treated with the traditional sealing technique, subjected to a metallization process, and analyzed by scanning electron microscope.
Results:
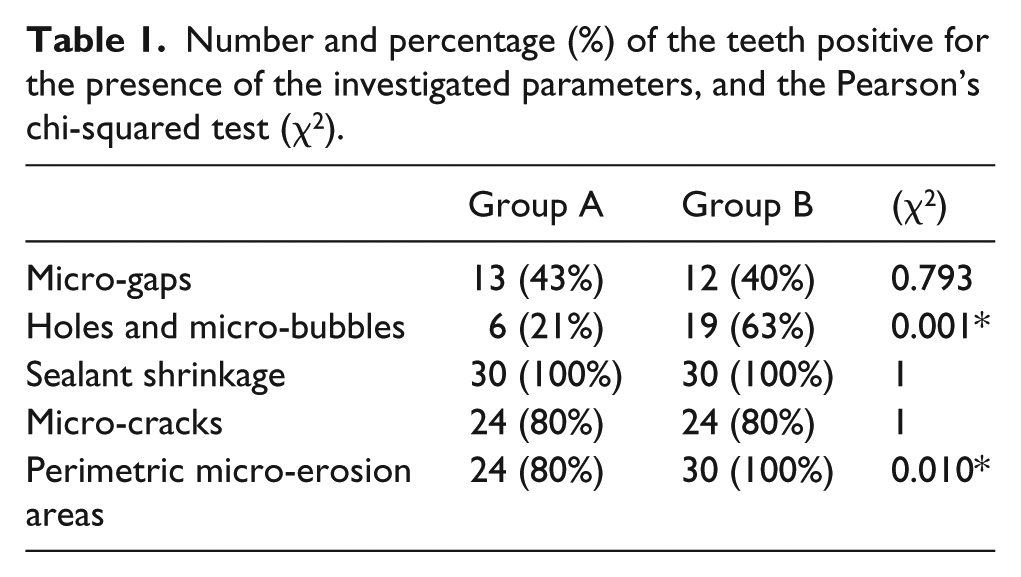
Micro-gaps between the sealant and the enamel were found in specimens in both A (43%) and B (40%) groups (p=0.793), and sealant shrinkage was seen. Significant differences between the groups emerged in the percentage of perimetric micro-erosion sites (80% vs. 100%, p=0.010) and the presence of holes and micro-bubbles on the sealant surface (21% vs. 63%, p=0.001).
Conclusions:
Although macroscopic clinical polymerization occurred with both instruments, the microscopic evaluation showed significant differences between the studied groups in terms of perimetric micro-erosion sites and micro-bubbles, which were higher in laser-cured samples.
Introduction
Dental caries is, still today, one of the most common diseases worldwide.1-3 A great deal of attention has been directed to preventing the development of carious injuries in occlusal pits and fissures by using seals which, through a composite resin application, can fill pits and fissures and remain intact and bonded to enamel.4-6 Sealing techniques include the use of resins that can prevent caries through both mechanical and chemical actions. The mechanical function consists of the filling of enamel micro-cavities, and it is associated with the chemical action, carried out by the release of substances capable of counteracting the onset of caries.7,8 The sealant resins adhere to the tooth enamel after a first stage of surface etching with 37% phosphoric acid. Once applied to the tooth surface, the resins are subjected to polymerization by different light sources. High-intensity light-emitting diode (LED) curing units are well established and commonly used for curing the sealants. 9 New high-intensity light via laser units could provide polymerization of the sealant composite materials faster than conventional lights. 10 However, according to some studies in the literature, the shortened curing times and the use of high-power sources remain controversial regarding the final outcome. 11
The purpose of this study was to evaluate in vitro the effects of two different light curing units, the innovative laser diode (LD) lamp and the traditional LED B, on sealant resin polymerization.
Materials and methods
Sixty healthy fully impacted third molars extracted for orthodontic reasons were included in this in vitro study. The crowns were totally mineralized and free of cracks and caries. The teeth were cleaned from impurities by means of curettes and stored in a sodium chloride (0.9%) and thymol (0.2%) solution. Before use, all the teeth were rinsed and the occlusal areas were brushed with sodium bicarbonate (granulometry 65 µm). After that, the teeth were subjected to a heat cycle of 37°C for 2 days in a ventilated oven in order to guarantee complete dehydration before the metal-graphic analysis with a scanning electron microscope (SEM). After these procedures, the teeth were randomly assigned to two groups and stored in distilled water. Group A consisted of the teeth destined for polymerization by LED B lamp (wavelength: 420–480 nm; power: 5 Watt; optic fiber diameter: 8mm), and group B comprised the teeth to be polymerized by LD (wavelength: 450 nm ± 10 nm; power: 0.1–3.0 Watt; frequency: 0 Hz–20 kHz). Both groups were treated by the same operator, in accordance with the traditional sealing technique, strictly following the clinical recommendations of the manufacturer (Helioseal® F). In particular, the following procedures were performed:
- etching with 37% orthophosphoric acid (Ultra-Etch® /ULTRADENT) for 30 s of the surface portion destined to be sealed;
- thorough rinsing and drying;
- application of the sealant (Helioseal® F) directly on the surface by means of disposable cannula, and waiting for 15 s;
- polymerization with LED B lamp, (420–480 nm at 5 Watt) for 20 s in the direction of the groove, at a distance of about 3 mm of the surface in group A;
or:
- polymerization with LD lamp (450 nm ± 10 at 0.5 Watt) for 3 s in the direction of the groove, at a distance of about 3 mm of the surface in group B;
- afterwards, each tooth was stored in foil paper in order to avoid post-cure polymerization processes and thus artifacts in the results.
At the end of the treatment, all the teeth were subjected to a metallization process in a palladium-silver bath (Figure 1) and were then analyzed with the SEM (Stereoscan 360, Cambridge Instruments) at different magnifications.

Metallization of the teeth in palladium-silver bath.
Then, the following qualitative evaluations were performed in both the groups:
- the presence of micro-gaps between the sealant and the enamel;
- the presence of holes and micro-bubbles on the sealant surface;
- the sealant shrinkage and its direction;
- areas of micro-erosion on the occlusal surface of the teeth.
These parameters were observed under low (10×), medium (250–500×) and high (1000–1500×) magnification.
In particular, the micro-gaps were defined as detachment of the sealant from the enamel, observed under 1000–1500× magnification (Figure 2(a,b)). The holes and micro-bubbles were identified on the sealant under 500× magnification (Figure 3). The sealant shrinkage was considered as the difference between the etched surface completely covered by the sealant material prior to polymerization and the etched enamel surface visible after polymerization (Figure 4(a,b)).
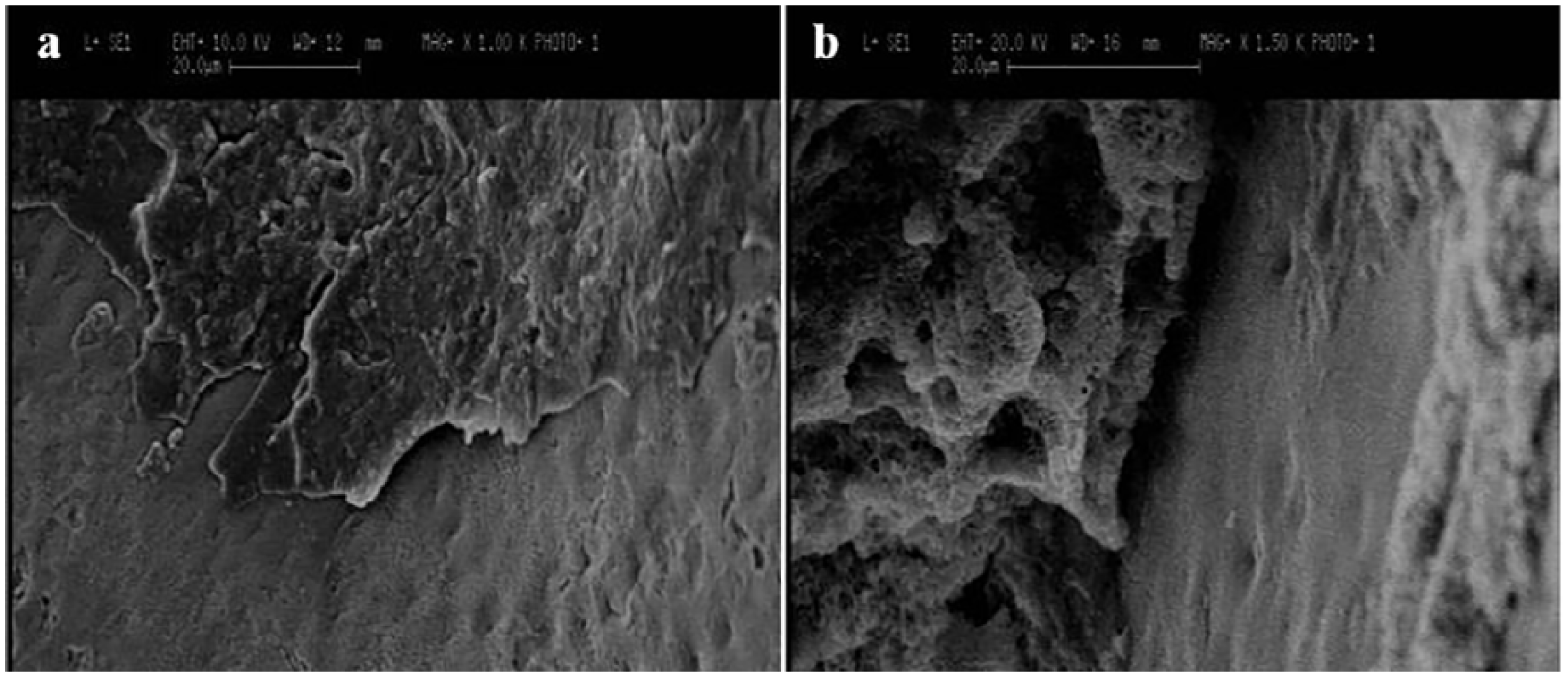
Micro-gaps between sealant and enamel, observed under 1000× (a) and 1500× (b) magnification.
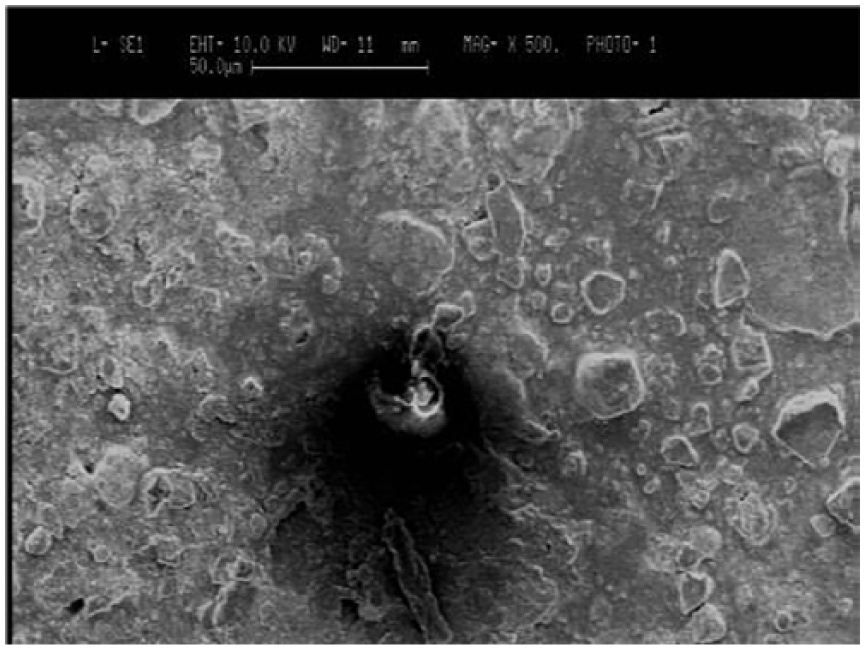
Holes and micro-bubbles identified on the sealant under 500× magnification.
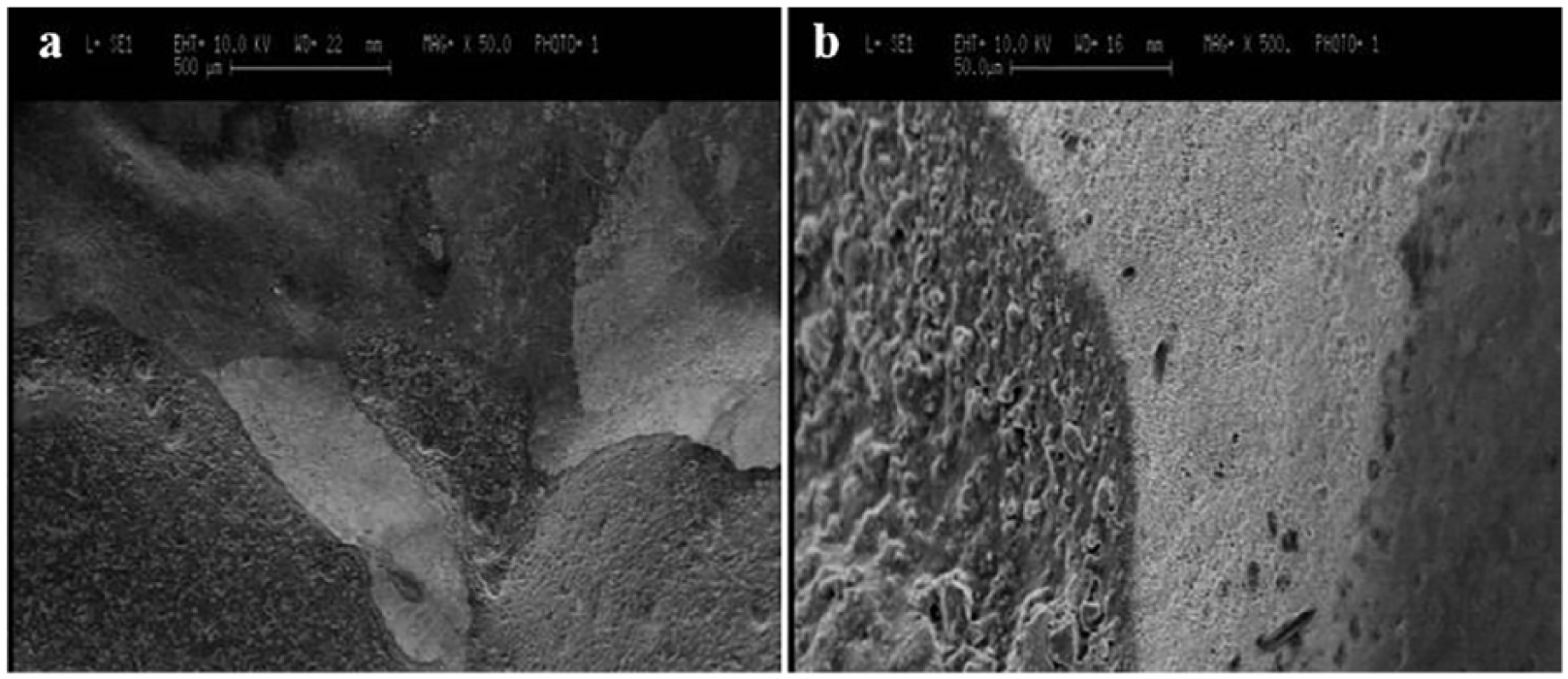
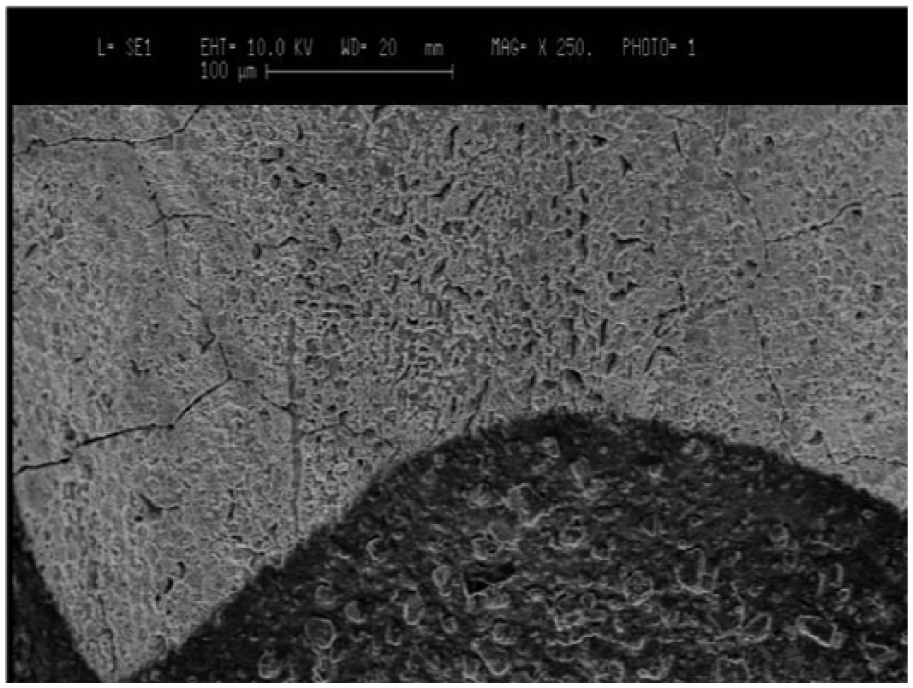
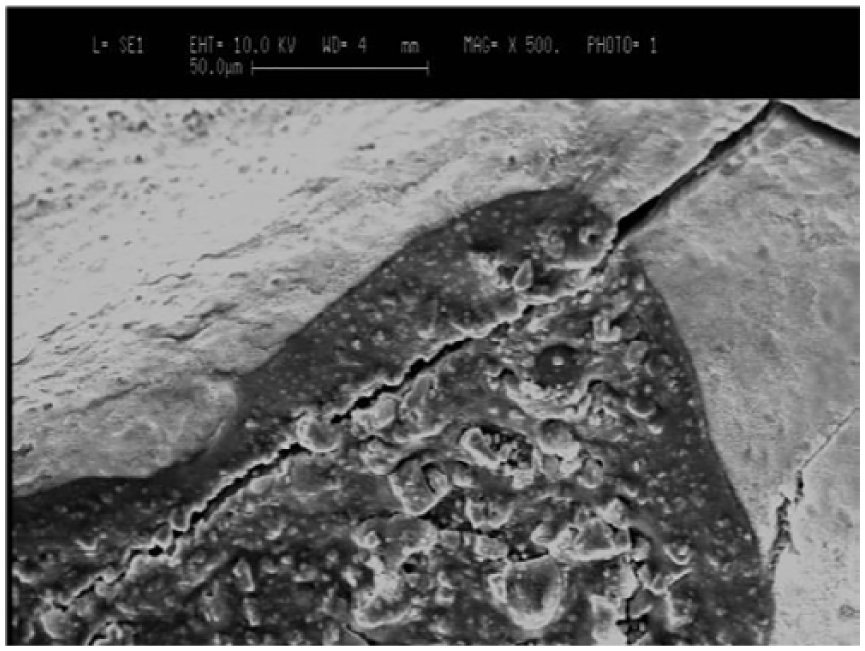
Light areas of enamel surface caused by the etching and subsequent shrinkage of the sealant; (a) at 50× magnification; (b) the interface between the sealant material (dark), etched enamel (very light) and not-etched enamel (gray and homogeneous) 500× magnification.
Micro-erosions of the enamel were identified with the light areas surrounding the sealing material on the surface of the teeth at 1500× magnification (Figure 5). In addition to the evaluation of their presence, an assessment of their perimetric or partial distribution was performed. Only perimetrically distributed micro-erosions were considered for comparison purposes.
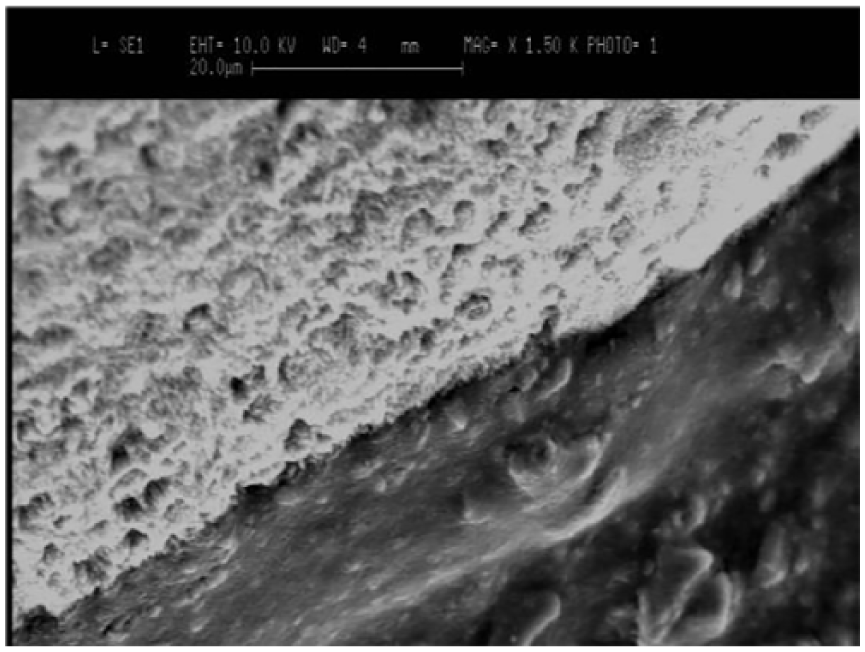
The micro-erosions of the enamel were identified with the light areas surrounding the sealing material on the surface of the teeth at 1500× magnification.
A dichotomic evaluation was used to score the presence or otherwise of the mentioned parameters on the examined surfaces of the teeth, and the results were expressed as a percentage of the comparison of the evaluating parameters in the investigated groups.
Data were analyzed with Pearson’s chi-squared test (χ2).
Results
Table 1 shows the comparison of the evaluated parameters between group A, where the polymerization was performed with LED B lamp, and group B, subject to the LD lamp polymerization.
Number and percentage (%) of the teeth positive for the presence of the investigated parameters, and the Pearson’s chi-squared test (χ2).
A careful evaluation of the morpho-structural data from the observations showed that in both the analyzed groups, all dental elements presented a macroscopic adhesion of the composite material to the dental crown surface. At low magnification (10×) it was possible to identify light-colored areas surrounding the sealing material in a non-uniform manner. These manifestations were caused by variations in the electron signal linked to the chemical composition of the material. The areas were different in size and location in the two analyzed groups. In group A, the light-colored area seemed to completely encircle the sealant material in 80% of the samples, while in group B this conformation was found in 100% of analyzed elements and with a greater extension on the occlusal surface. At a magnification of 250–300× it was possible to observe an adequate interface between the sealant material and the tooth surface in both groups (Figure 6). Increasing the magnification, at 500× deep areas of enamel micro-erosion were observed in both groups. These micro-erosions could be better observed at a greater magnification of 1500×. Comparing the two groups, the micro-erosions surrounding the sealant material were greater and more pronounced in group B compared with group A. Generally, at 1000–1500× magnification, it was possible to evaluate the marked adhesion of the sealing material to the tooth surface on a large part of the perimeter. However, at the same magnification, many gaps and micro-gaps formed between the sealant and the dental surface and were evident with an almost uniform rate of 40–43% in both groups. Conversely, in 21% of group A samples, compared with 63% of group B samples, holes and micro-bubbles were observed within the sealing material. Such defects ranged from a diameter of 1–2 μm to a maximum of 5–6 μm. In both groups, a uniform rate of micro-fractures (80%) was observed; however, they were present only in a small area of the enamel surface (Figure 7). Furthermore, an important shrinkage of the sealing material was observed in all the examined teeth.
An adequate interface between the sealant material and the tooth surface at 250× magnification.
Micro-cracks of the tooth surface and sealant.
The Pearson’s chi-squared test (χ2) showed significant difference between two groups for the presence of micro-erosion areas (p=0.010) and holes and micro-bubbles (p=0.001). For other parameters no significant difference was detected between group A and B (Table 1).
Discussion
The fissure-sealing procedure was introduced in preventive dentistry more than 50 years ago.12,13 Since then, several studies have been conducted, leading to improvements in the efficacy of sealing materials and procedures.14,15 In order to guarantee effectiveness and durability of the procedure, the integrity of the enamel–sealant interface is fundamental. Many factors are implicated in this challenge, including the chemical characteristics of the materials, the enamel surface treatment, and the operative procedures of sealant application and polymerization.16-18 Various types of curing lights have been introduced for photo-polymerization of the resin composite; among these, the conventional LED B lamp, plasma arc curing light, and LD lamp are the most widely used.19,20
LED combines two different semiconductors (p-n junctions). When voltage is applied, the electrons and holes recombine at the LED’s p-n junctions, leading to the emission of blue light. The spectral output of gallium nitride blue LED falls conveniently within the absorption spectrum of camphorquinone, thus, no filters are required in LED light curing units. 21
The laser’s beam implies stimulated emission of radiation and differs from the conventional light source. It is a single wavelength (monochromatic), collimated (very low divergence), coherent (photons in phase), and intense. 22 Since the 1980s, several studies have been conducted to investigate the use of the argon laser for the photo-polymerization of resin composite restorative materials. 23
In our study, the results of sealant polymerization performed with LD were compared with a traditional LED B polymerization. Even though a good macroscopic adhesion of sealant material to the tooth surface was obtained with both procedures, several defects of material, enamel surface, and sealant–enamel interface emerged at different microscopic magnifications. In particular, the presence of micro-erosion areas and holes and micro-bubbles demonstrated a significantly different (p=0.010 and p=0.001, respectively) quantitative and qualitative distribution in the two investigated groups, suggesting a differing influence of the polymerization mode. Other parameters showed no statistically significant difference between the groups. Among other defects, an important material shrinkage was observed in all the examined teeth. This shrinkage shows that the optimal power and time of sealant polymerization need to be further investigated in order to avoid a procedure that results in a sealing material inefficient for the prevention of caries.
The presence of these defects raises the risk of bacterial colonization and the possibility of developing caries below or in close proximity to the sealing material. 24 Several studies have demonstrated a higher concentration of cariogenic bacteria in plaque adjacent to composite restorations, compared with plaque on the natural surface of the tooth. 25 Another study, analyzing the early stages of plaque formation, revealed that different species of bacteria attached to the composite compared with those adherent to enamel, probably due to different surface characteristics. 26
Thus, the presence of micro-gaps at the sealant–enamel interface may support bacteria, their metabolites, and other compounds from oral fluids, which play a large role in the development of caries. Even though no consensus exists on the role of micro-gaps on the sealant–tooth interface in development of caries, the dimension and the shape of the gap seems to be critical. 27 The results of the most recent studies show that interfacial gaps larger than 60 μm seem to predispose interfacial demineralization, and may thus lead to caries. 28
Application of the sealant, as well as other composite resins, is highly technique sensitive, and polymerization is its fundamental part. Although the clinical recommendations of the manufacturer were strictly followed, the defects of adhesion listed above occurred in the present study.
Based on these findings, further studies are needed to understand if a different material or procedure can improve the results and ensure a more durable and reliable sealing intervention.
Conclusions
From the data obtained in present study, it is possible to state that both LED and laser methods allow good polymerization of the sealant material. Significant differences, however, emerged in the evaluation of the presence of perimetric micro-erosion sites and holes and micro-bubbles, highlighting that in laser-cured specimens the percentage of such defects was significantly higher. Although the clinical significance of such findings is still unclear, it is important to adopt operational techniques that allow maximum reduction of such alterations.
Footnotes
Author contributions
MF: conceived of the presented idea; PI and PE: designed and directed the project; MS: performed the experiments and analyzed the data; ZK: wrote the paper with input from all authors; TG: contributed to the interpretation of the results and performed statistics; CR: provided support for all the SEM procedure, analysis at Politecnico di Milano; GE and LL: supervised the project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The present study was funded by the authors’ own institutions.