
Abstract
Objective:
To assess public awareness of cancer symptoms, risk factors, and available screening programs, and to examine their association with sociodemographic parameters in Georgian population.
Methods:
A cross-sectional study (2023–2024) surveyed 385 adults via random-digit dialing using the Georgian version of the Cancer Awareness Measure (CAM), which comprises 9 symptom and 11 risk factor items. No stratification or demographic weighting was applied. A pilot test (n = 20) was conducted prior to ethical approval. Chi-square and t-tests assessed categorical and continuous variables; multivariate analysis used linear regression, with p < 0.05 considered significant.
Results:
Among the 385 respondents, 57.7% demonstrated low-to-average awareness of cancer symptoms. Women exhibited significantly greater awareness than men (β = 0.19, B = 1.56, 95%CI: 0.7–2.4; p < 0.001), and awareness was positively associated with household income (β = 0.17, B = 0.67, CI: 0.23–1.1; p < 0.001). Only 5.7% of respondents demonstrated high knowledge of cancer risk factors, with urban residents and those with higher incomes showing significantly greater awareness.
Conclusions:
Improving cancer awareness and facilitating earlier diagnosis will require scalable, equity-oriented educational initiatives that account for gender and socioeconomic disparities. Implementing such programs across schools, primary care settings, and mass media, alongside the expansion of cancer screening services, may substantially enhance timely detection and reduce inequities in cancer outcomes.
Keywords
Introduction
Cancer remains the second leading cause of death worldwide, accounting for an estimated 9.7 million deaths and 20 million new cases in 2022. 1 The estimates indicate that approximately 1 in 9 men and 1 in 12 women are expected to die from the disease. 2
Approximately 1/3 of cancer-related deaths are caused by the top five behavioral and dietary risk factors: obesity, insufficient consumption of fruits and vegetables, low physical activity, and excessive tobacco and alcohol consumption. 3
By reducing exposure to risk factors, it is possible to prevent 30%–50% of all cancer cases. 4 The burden of cancer can also be alleviated through early diagnosis, 4 which makes awareness of cancer symptoms, risk factors, and available screening programs essential.
Patient survival largely depends on the stage of the cancer at the time of diagnosis. For example, the 5-year survival rate for breast cancer patients is very close to 100% when the cancer is detected at an early stage, but it is only 25% when the cancer is diagnosed at a late stage. The statistics are similar for other cancers: the 5-year survival rate is 90% for early-stage colorectal cancer, only 10% for late-stage cancer, and 65% and 5% for early-stage and late-stage lung cancer, respectively.5–7 Late-stage diagnosis contributes to preventable deaths from colorectal, 8 breast, 9 and lung cancer 7 in the UK.
Georgia is a small country located in the South Caucasus region, at the crossroads of Eastern Europe and Western Asia. It has a population of around 3.7 million inhabitants, with an ethnically diverse composition: Georgians constitute the majority (86.8%), followed by Azerbaijanis (Azeri, 6.3%), Armenians (4.5%), and other minority groups (approximately 2.3%). Georgia is classified as an upper-middle-income country, and despite recent economic growth and improvements in healthcare infrastructure, the country faces significant public health challenges, including a high burden of non-communicable diseases such as cancer. 10
In 2023, Georgia recorded 11,625 new cancer cases (incidence rate of 312.9 per 100,000 inhabitants). The most common cancer sites were breast, thyroid, colorectum, uterine body, and ovary among women, and prostate, lung, colorectum, urinary bladder, and stomach - among men. 40.2% of new cancer cases were diagnosed at stages III–IV and 37.2%—at stages I–II; staging was unspecified in the remainder. 3 Population-based registry data revealed a strong association between earlier diagnosis and 5-year survival—90% for stage I patients versus 27% for stage IV patients. These trends underscore the survival disadvantage of late-stage detection. 3 Georgia’s 5-year survival rates remain lower than those of high-income countries—for example, breast cancer survival is 79% in Georgia 3 versus 91% in the U.S., 5 and for colorectal cancer, survival rates are 49.5% 3 versus 71% in Australia. 11
Low cancer awareness—encompassing knowledge of symptoms, risk factors, and screening programs—is a key contributor to late-stage diagnosis. 12 Timely detection relies on public recognition of potential symptoms and understanding the importance of seeking care. Awareness of screening programs is equally critical, as screening enables early detection of cancers such as breast, colorectal, and cervical cancer. The example of the Czech Republic’s national colorectal cancer screening program, which started in July 2000, effectively demonstrates the significant benefits of screening in reducing both the incidence of new cases and mortality rates. Between 2000 and 2007, the incidence of new cases decreased by 6%, and colorectal cancer-related mortality decreased by 20.8% between 1995 and 1999 and 2006–2010. 13
However, screening program coverage in Georgia remains low. In 2021, the screening rates for the target populations were 12% for breast cancer, 11% for cervical cancer, and just 2% for colorectal cancer. 14 Importantly, a coverage rate of 70%–75% is considered the benchmark for effective screening programs, as it is linked to significant reductions in cancer-related morbidity and mortality.15,16
Early diagnosis and treatment are key to reducing the cancer burden. Assessing public knowledge, attitudes, behaviors, and barriers to early detection—alongside their sociodemographic determinants—can inform more effective prevention and early detection strategies. We reviewed the published literature to assess cancer awareness in countries neighboring Georgia, including the Black Sea region and the Caucasus. In Bulgaria, knowledge of cancer screening tests is limited and varies by cancer type. 17 In Romania, symptom awareness is low, even among high-risk groups. 18 In Turkey, knowledge of cancer symptoms and risk factors is limited. 19 In Armenia 20 and Azerbaijan, 21 awareness and screening behaviors differ according to age, residence, education, and other sociodemographic factors. To date, no systematic population-based research on cancer awareness has been conducted in Georgia. The only available study, published in 2022, assessed screening awareness among primary healthcare physicians in three regions and reported low levels of knowledge, which may contribute to low public participation in screening programs due to insufficient referrals. 22
Understanding where knowledge deficits lie is a prerequisite for designing effective, equity-minded interventions. We therefore conducted the first systematic population-based assessment of general cancer awareness in Georgia to establish a national baseline before targeting specific cancers. The study aimed to (
Design and methods
Sampling and data collection
We conducted a cross-sectional study between December 2023 and September 2024 to assess awareness of cancer symptoms, risk factors, and screening programs among 385 Georgian adults aged ≥18 years.
The sample size was calculated using the standard formula for descriptive studies: n = (z^2 × (p) ̂ (1–(p)’))/ε^2, z = 1.96, p^ = 0.5, and ε = 0.05 (margin of error − 5%), giving n = 384.16, which was rounded up to 385.
The inclusion criteria were as follows: age ≥ 18 years, knowledge of the Georgian language, and verbal consent to participate.
We applied a random digit dialing (RDD) approach. Telephone numbers were generated via national telecom prefixes and a computer-generated six-digit suffix. Each number was called up to three times on different weekdays and times. Of the 9862 numbers dialed, 4136 were ineligible (disconnected or business lines), and 2944 refused. Among the 782 eligible contacts, 385 completed the interview, yielding a response rate of 49% and a cooperation rate of approximately 12%. No stratification or weighting was applied; implications for representativeness are considered in the Discussion.
The participants were surveyed via the Cancer Research UK Cancer Awareness Measure (CAM) toolkit version 2.1,23,24 an international standardized validated tool used to evaluate public awareness of cancer symptoms and risk factors, as well as barriers to seeking help. CAM is freely available and does not require explicit permission for its use.
We used the full nine-question toolkit covering suspicious cancer symptoms (Q1–2), help-seeking behavior (Q3), barriers to consulting a doctor (Q4), cancer risk factors (Q5–6), cancer and age (Q7), common cancers (Q8), and knowledge of screening programs (Q9).
The questionnaire was translated via the forward‒backward translation method in accordance with the guidelines outlined by Beaton et al. 25 All author recommendations for modifying the questionnaire have been considered. The original 9 questions and 47 items were retained, with an additional item on “financial barrier” added to question 4, reflecting its significance in the Georgian context. The adapted version now includes 48 items. All necessary demographic questions recommended by the authors have been preserved, and an additional question regarding the household’s monthly income has been added. The translated and adapted questionnaire (Supplemental File 1) was tested in a pilot phase with the first 20 respondents to assess clarity and understandability. Afterward, the Biomedical Research Ethics Board at the University of Georgia approved the final version of the questionnaire and study protocol (N11-33877, 20.12.2023).
Participation in the study was voluntary, and informed consent was obtained from each respondent prior to completion of the questionnaire. Due to the RDD method, the Biomedical Research Ethics Board at the University of Georgia waived the requirement for written informed consent and approved the use of verbal consent.
The data were anonymized, and the study was conducted in accordance with the Declaration of Helsinki. 26
Three outcome variables were defined: (a) awareness of cancer signs and symptoms, (b) awareness of cancer risk factors, and (c) awareness of available screening tests. The explanatory variables included sex, age group, residence (urban vs rural), marital status, education level, employment status, and monthly household income.
Cancer signs and symptom awareness were scored following the provided coding from 9 to 27, with 9–21 indicating low awareness, 22–24 indicating average awareness, and 25–27 indicating high awareness.
Cancer risk factor awareness was scored as follows: very low (11–21), low (22—32), average (33–43), or high (44–55).
Awareness of screening tests for breast, colorectal, and cervical cancer was assessed based on knowledge of screening programs and the eligible age range, determined by the percentage of people aware versus unaware.
For the household income parameter, the categories were defined with reference to national income distribution data from the National Statistics Office of Georgia (GeoStat). 10 We used the values of the subsistence minimum for a working-age male in Georgia (256 GEL in 2024) to define cut-points for “low,” “medium,” and “high” income brackets.
We anticipated several potential sources of bias. Selection bias may have occurred because households without active phone lines could not be reached through random-digit dialing, potentially underrepresenting lower-income and rural populations. To minimize this, each generated number was called up to three times at different hours and on different days. Social desirability bias was also possible due to the interviewer-administered format; however, standardized questioning procedures were used to reduce interviewer influence.
Analyzes assumed a simple random sample of respondents. No post-stratification weights were applied; thus, findings may overrepresent urban and highly educated participants due to the random digit dialing recruitment method.
There were no missing data for variables included in analyses.
The reporting of this study conforms to the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines for cross-sectional studies. 27 (Supplemental file 2).
Statistical analysis
Data entry, verification, management, and statistical analysis were conducted via IBM SPSS Statistics for Windows (Version 21.0). Quantitative indicators were compared via the SPSS program (IBM Corp., Armonk, NY).
Descriptive statistics (mean, median, standard deviation) were calculated for each variable. The t-test was used to analyze the relationships between categorical and quantitative variables, whereas the chi-square test and odds ratio (OR) with 95%CI were used to assess categorical parameters. Multivariate analysis was performed via linear regression. A p-value < 0.05 was considered significant.
Results
Participant flow and characteristics
A total of 9862 telephone numbers were dialed, 782 eligible adults were reached, and 385 completed the interview (response rate = 49%, cooperation rate = 12%). The mean participant age was 50 (SD = 12.8); 73% were female, and 84% had tertiary education (the sociodemographic characteristics of the study participants are presented in Table 1).
Sociodemographic data of the study participants.

Knowledge of cancer symptoms
The overall average score for cancer symptom awareness was 22.87 (SD = 3.67), which falls within the low awareness range. A total of 222 out of 385 respondents (57.7%) demonstrated a low-to-average level of knowledge of cancer warning signs.
In response to the open-ended question, the most frequently recalled symptoms were a lump (42.1%), weakness (36.9%), weight loss (30.9%), and pain (28.6%), whereas the least frequently mentioned symptoms (<5%) were nausea, vomiting, jaundice, and loss of appetite. The most recognized symptom was a change in mole appearance (88.3%), followed by unexplained weight loss (85%), unexplained lump or swelling (80%), unexplained bleeding (75%). Less recognized symptoms were persistent cough or hoarseness (71%), persistent unexplained pain (69%), persistent difficulty swallowing (66%), persistent change in bowel habits (63%), and the least recognized one was sore that doesn’t heel (30%).
Women’s awareness of cancer symptoms was significantly greater than men’s awareness (mean score 23.3 (SD = 3.4) vs 21.8 (SD = 4.1), p = 0.014), and there was a positive association between cancer symptom awareness and household income (χ2 (8) = 17.907, p = 0.022).
No significant differences were found by education, but knowledge was notably low among students (72% had low to average symptom awareness). Similarly, while residence type showed no significant difference, awareness was lower in rural areas. Additionally, 50% of individuals over 70 years of age had low levels of cancer symptom awareness. The associations of awareness of cancer symptoms with the sociodemographic parameters of the respondents are presented in Table 2.
Association between awareness of cancer symptoms and risk factors and the sociodemographic characteristics of the respondents.

df: degrees of freedom.
p-value is significant (<0.05).
Help-seeking intentions and barriers
The response to symptoms potentially indicating cancer suggested that individuals would wait an average of 10 days (SD = 15) before consulting a doctor. A total of 19.5% of the respondents would delay seeing a doctor for more than a month, and 3% would never seek medical attention. The most common factors contributing to delays in seeking medical advice are financial aspects (45.2%), worries about what the doctor might find (42.9%) and fears (37.4%). Women reported being more afraid to visit a doctor than men were (χ2 (3) = 7.593, p = 0.055), although the result was marginally nonsignificant. In contrast, men were significantly more likely than women were to report difficulty discussing their symptoms with a doctor (χ2 (3) = 8.774, p = 0.032). Individuals aged 18–29 and 30–49 years (χ2 (9) = 18.188, p = 0.033), as well as students and employed individuals (χ2 (12) = 20.294, p = 0.062), reported being too busy to visit the doctor. A significant association was found between delaying doctor visits due to financial barriers and household income (χ2 (12) = 33.297, p < 0.001).
Risk factor knowledge
The overall average score for cancer risk factor awareness was 34.91 (SD = 5.762), which is close to the lower limit of the average awareness range.
Only 5.7% of the respondents had high knowledge of cancer risk factors, while 63.6% had average knowledge, and 30.7% had low or very low knowledge.
In response to the open-ended questions, the most frequently recalled risk factors for cancer were tobacco use (39.5%), unhealthy diet (39.0%), air pollution (28.3%), genetics (28.1%), a polluted environment (27.0%), and stress (26.5%).
The most recognized risk factors were smoking (76.9%), HPV (63.1%), family history (62.9%), and passive smoking (61.1%). Less frequently identified factors included poor diet, sunburn, alcohol use, red meat consumption, obesity, and age.
Knowledge of cancer risk factors was significantly associated with age (χ2 (9) = 18.854, p = 0.026), with mean scores of 35.1 (SD = 5.0), 36.0 (SD = 5.98), 34.3 (SD = 5.68), and 33.5 (SD = 5.23) for the 18–29, 30–49, 50–69, and >70 age groups, respectively, indicating lower awareness in older age groups. Individuals residing in urban areas demonstrated significantly greater knowledge of cancer risk factors than those living in rural areas did (χ2 (12) = 24.103, p = 0.02). Sixty-one percent of the respondents thought that cancer development was not age dependent.
The associations of awareness of cancer risk factors with the sociodemographic parameters of the respondents are presented in Table 2.
Awareness of the most common cancers and national screening programs
The respondents were asked to list the three most common cancers in women and men. For women, the three most common cancers listed by participants were breast cancer (74%), cervical cancer (63.4%), and bowel cancer (15.8%). For men, most respondents indicated prostate cancer (56.4%), lung cancer (29.6%), or bowel cancer (17.1%).
With respect to the available screening programs, 92.2% of the respondents were aware of breast cancer screening, but only 63% correctly identified the eligible age range (40–70 years). While 79% were aware of cervical cancer screening, only 13% accurately reported the eligible age range (25–60 years). Similarly, 53.8% knew about colorectal cancer screening, but only 47.4% correctly identified the target age range (50–70 years).
Women were significantly more aware of all three screening programs than men were. Awareness also varied significantly by age, with the lowest levels in the 18–29 age group and the highest in those over 70 years of age. Individuals with tertiary education were more knowledgeable than were students or those with only secondary education. Breast cancer screening awareness was greater among employed/self-employed individuals than among unemployed individuals and students (p = 0.01) and lower in rural areas than in urban areas (p = 0.062), although the latter difference was not statistically significant. The associations between awareness of screening programs and sociodemographic parameters are shown in Table 3.
Association of screening programs’ awareness with sociodemographic parameters.

df: degrees of freedom.
p-value is significant (<0.05).
Multivariable associations
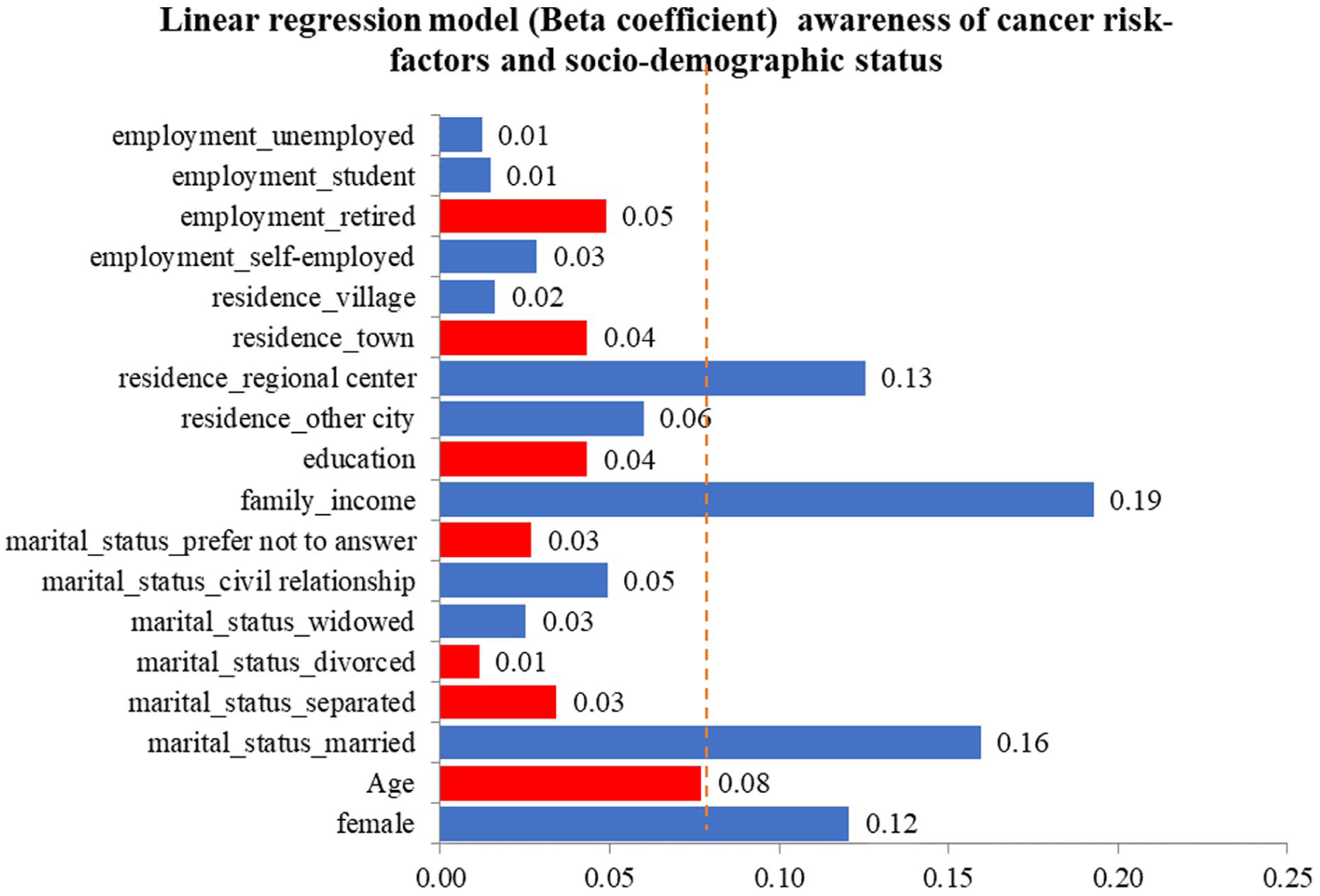
According to the fully adjusted models (Figures 1–3), women scored higher than men did in terms of knowledge of symptoms (β = 0.19, B = 1.56, 95%CI: 0.7–2.4; p < 0.001, adjusted R2 = 0.04), risk factors (β = 0.12, B = 1.56, 95%CI: 0.2–2.9; p = 0.02, adjusted R2 = 0.07), and were more likely to be aware of screening programs for breast cancer (β = 0.16, B = 0.18, 95%CI: 0.06–0.3; p < 0.001, adjusted R2 = 0.08), cervical cancer (β = 0.23, B = 0.41, 95%CI: 0.21–0.61; p < 0.001, adjusted R2 = 0.1), and colorectal cancer (β = 0.2, B = 0.44, 95%CI: 0.22–0.66; p < 0.001, adjusted R2 = 0.06).

Association between awareness of cancer symptoms and sociodemographic status.
Association between awareness of cancer risk factors and sociodemographic status.

Association between awareness of breast cancer screening and sociodemographic status.
Higher household income predicted greater knowledge of symptoms (β = 0.17, B = 0.67, CI: 0.23–1.1; p < 0.001, adjusted R2 = 0.04) and risk factors (β = 0.19, B = 1.17, 95%CI: 0.51–1.83, p < 0.001, adjusted R2 = 0.07). Rural residence was independently associated with lower risk factor knowledge (β = 0.13, B = 3.1, 95%CI: 0.5–5.7, p = 0.02, adjusted R2 = 0.07).
Higher education was positively associated with improved knowledge of all screening programs: breast cancer (β = 0.15, B = 0.1, 95%CI: 0.02–0.18, p = 0.01, adjusted R2 = 0.08), cervical cancer (β = 0.10, B = 0.11, 95%CI: 0–0.23, p = 0.07, adjusted R2 = 0.1), and colorectal cancer (β = 0.14, B = 0.19, 95%CI: 0.04–0.34, p = 0.01, adjusted R2 = 0.06).
Discussion
Our findings predominantly reflect educated urban populations, as most participants were women (73%), urban residents (84%), and had tertiary education (84%). Study revealed that 60% of interviewed people have low-to-average cancer symptom knowledge. Women exhibited significantly greater awareness than men did, and symptom knowledge was positively associated with family income. Financial barriers, fear, and concerns about potential diagnoses delay medical help-seeking.
Knowledge of cancer risk factors was low, with only 5.7% of respondents showing high awareness. This awareness declined with age and was greater in urban residents. Tobacco use and air pollution are frequently recognized as risk factors, whereas stress is overestimated. Many respondents held misconceptions about true risk factors, including the roles of fruit/vegetable intake, alcohol, red meat, obesity, and age.
Respondents correctly identified breast cancer as the most common cancer in Georgian women but misidentified the second and third most common cancers, listing cervical and colorectal instead of thyroid and colorectal. 3 For men, prostate, lung, and colorectal cancers were accurately identified by the respondents as the three most common cancers, which is in line with national statistics. 3
The awareness of screening programs was greater among women, individuals with higher education, and urban residents. However, knowledge of the specific age ranges for eligible screening was often inaccurate.
Comparison with previous work
Our finding that women have greater cancer awareness than men aligns with studies from both developed contexts, such as UK 28 and (Japan) 29 and lower-income regions - Gaza Strip 30 and Jordan, 31 indicating that this gender disparity persists across economic settings. This highlights the need for gender-sensitive education. The association between cancer awareness and education level, consistent with studies in Poland, 32 Hong Kong, 33 and Japan, 29 underscores the importance of incorporating cancer education into school and university curricula. Additionally, our study revealed lower awareness of cancer symptoms and risk factors in older age groups, a finding also reported in UK, 28 Poland 32 and Ethiopia, 34 emphasizing the need for targeted cancer awareness programs for older adults. All of these studies employed adapted versions of the CAM tool.
The pronounced urban–rural gap aligns with the digital access disparities documented in the Caucasus Barometer 35 and underscores the need for non-internet channels in health promotion.
Low literacy around screening eligibility likely contributes to Georgia’s suboptimal program uptake (12% for breast, 11% for cervical, and 2% for colorectal). 12 Evidence from Lithuania 36 and Croatia 37 shows that mailed personalized invitations coupled with nurse-led community outreach can triple screening attendance within 2 years. Adapting such multimodal strategies—SMS and postal reminders, school-based curriculum modules, and primary-care brief counseling—could yield rapid gains. Income-related gradients point to financial and informational barriers. Campaigns should therefore integrate cost-neutral messaging (“all screenings free at state facilities”) and transport vouchers for rural villages.
Strengths and limitations
Strengths include the first use of a validated cancer-awareness instrument in the study conducted in Georgia and rigorous forward–backward translation. The large sample (N = 385) exceeded the calculated minimum and achieved a 49% response rate. This study has several limitations. First, the RDD approach, without poststratification weights, resulted in oversampling of respondents from urban areas, the capital, and highly educated adults. As a result, awareness in the general population is likely lower than reported. Given the overrepresentation of female respondents, the study’s findings may not fully capture the perspectives or experiences of males, limiting the generalizability of the results to the broader population. Owing to the RDD approach, the sample was unevenly distributed across age groups, with a disproportionate representation of respondents aged 50–69 (51.4%) and relatively fewer participants in the 18–29 (7.3%) and over 70 (6.2%) age groups. Second, 98% of the participants were Georgian, whereas 13% of the Georgian population belonged to other ethnic groups, whose responses could also provide valuable insights. Third, self-reports introduce social desirability bias, although anonymous telephone interviews mitigate this risk. Finally, the cross-sectional design precludes causal inference; longitudinal or experimental studies are needed to assess whether improved awareness translates into earlier diagnosis.
Future research
We recommend a weighted, nationally representative survey to establish baseline metrics for Georgia’s forthcoming 2025–2030 Cancer Control Plan, followed by controlled trials of school-based and primary-care-based awareness interventions that embed screening referral pathways. Qualitative work should explore perceptions among ethnic‒minority communities, which were underrepresented in our sample.
Conclusions
Cancer knowledge among our sample—representing educated, urban Georgians—remains insufficient. Targeted, income-sensitive educational initiatives delivered through schools, community clinics, and mass media, coupled with practical support for rural populations, offer a feasible strategy to enhance screening uptake and promote earlier cancer detection nationwide
Significance for public health
Cancer is a second leading cause of death in Georgia, with nearly half of cases diagnosed at advanced stages, limiting treatment success and survival. Our study highlights low awareness of cancer symptoms, risk factors, and screening programs, particularly among men, rural residents, and low-income groups. Such disparities contribute to delayed diagnosis and extremely low screening coverage, far below the 70%–75% benchmark needed to reduce mortality. By pinpointing the least-informed groups, this research provides critical evidence to guide targeted, equity-focused interventions. Strategies such as gender- and income-sensitive health education, integration of cancer awareness into school curricula, and community-based outreach, along with practical support such as transportation assistance and clear messaging on free screening services, could substantially increase early detection. Improving public knowledge is a cost-effective way to enhance survival, reduce health inequalities, and lessen the overall cancer burden in Georgia.
Supplemental Material
sj-docx-1-phj-10.1177_22799036261423726 – Supplemental material for Cancer awareness in Georgia: A cross-sectional study of knowledge gaps in symptoms, risk factors, and screening programs
Supplemental material, sj-docx-1-phj-10.1177_22799036261423726 for Cancer awareness in Georgia: A cross-sectional study of knowledge gaps in symptoms, risk factors, and screening programs by Ketevan Gachechiladze, Ivane Kiladze, Tina Beruchashvili, Kakhaber Jakeli, Ivane Kechakmadze and Nino Ganugrava in Journal of Public Health Research
Supplemental Material
sj-docx-2-phj-10.1177_22799036261423726 – Supplemental material for Cancer awareness in Georgia: A cross-sectional study of knowledge gaps in symptoms, risk factors, and screening programs
Supplemental material, sj-docx-2-phj-10.1177_22799036261423726 for Cancer awareness in Georgia: A cross-sectional study of knowledge gaps in symptoms, risk factors, and screening programs by Ketevan Gachechiladze, Ivane Kiladze, Tina Beruchashvili, Kakhaber Jakeli, Ivane Kechakmadze and Nino Ganugrava in Journal of Public Health Research
Footnotes
ORCID iDs
Ethical considerations
This study was performed in accordance with the principles of the Declaration of Helsinki. Approval was granted by the Biomedical Research Ethics Board at the University of Georgia (N11-33877, 20.12.2023).
Consent to participate
Informed consent was obtained from all individual participants included in the study.
Author contributions
All the authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by Ketevan Gachechiladze, Nino Ganugrava and Ivane Kechakmadze. The first draft of the manuscript was written by Ketevan Gachechiladze, and all the authors commented on previous versions of the manuscript. All the authors read and approved the final manuscript. All authors agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The dataset of the current study is available from the corresponding author on reasonable request.*
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.