
Abstract
Background
Colorectal cancer (CRC) is the first commonest diagnosed cancer in men and the fourth commonest in women in Ethiopia. Awareness of CRC and associated factors is crucial in the prevention of CRC. However, there have not been studies about the awareness of CRC and associated factors among adult patients in Ethiopia. Therefore, the study aimed to assess the awareness of CRC and associated factors among adult patients in Jimma, South-West Ethiopia, 2020.
Methods
This institution-based cross-sectional study design was conducted among 422 adult patients. The study respondents were recruited by a systematic random sampling method. The Cancer Awareness Measure questions were used to measure awareness of CRC of adult patients. Descriptive and logistic regression analyses were conducted.
Results
More than half (57.6%) of respondents had low-level awareness of CRC. Respondents who were females (adjusted odds ratio [AOR] = 1.86; 95% CI: 1.26, 2.75), who are residing in urban areas (AOR = .45; 95% CI: .30, .67), who had a monthly income of 3000 Ethiopian Birr and above (AOR = 4.72; 95% CI: 3.11, 7.15), who heard about CRC (AOR = 4.48; 95% CI: 2.90, 6.93), who get information through social media about CRC (AOR = 2.51; 95% CI: 1.18, 5.37), and who had a family history of CRC (AOR = 3.27; 95% CI: 1.45, 7.36) had a high level of awareness of CRC, while those who cannot read and write (AOR = 2.83; 95% CI: 1.49, 5.37) and learn elementary school (AOR = 2.12; 95% CI: 1.15, 3.93) had a low level of awareness of CRC.
Conclusion
This study indicated that awareness of CRC of adult patients was inadequate. Adult patients’ gender, residency, level of education, monthly income, heard about CRC, sources of information about CRC, and a family history of CRC were found to be independent predictors of the awareness of CRC. Therefore, there is a need for health education and awareness campaigns for promoting awareness of CRC of adult patients, and the government should develop policy on CRC prevention and screening program.
Introduction
Cancer is an important global health problem in a developed and developing country. It is the most important cause of morbidity and mortality which affects the socioeconomic status of the population.1-4 It is expected to have grown to 18.1 million new cases and 9.6 million of the population died globally.2,5 The most commonly identified cancers are colorectal, lung, and breast cancers.6-9 Cancer in sub-Saharan Africa (SSA) is on the rise mainly caused by a lack of awareness about cancer.4,10,11
Colorectal cancer (CRC) is the third commonest confirmed cancer in males and the second commonest in females in the world. It has grown to 1.8 million cases (10.2%) with the biggest figure of deaths (9.2%) in the globe.5,12 The majority of CRC is classified as adenocarcinoma, which mostly begins as a benign tumor, and changed to cancerous, and that may attack normal tissue, which spreads into the distant organ.13-15 In SSA, CRC is the commonest cancer that confirmed case for 5.6% in male and 3.7% in the female.10,16 Previous evidence showed that CRC accounts for 12.2% in males and 4.4% in females in Ethiopia. 17 Currently, CRC in Ethiopia has become the first highest in men (19%) and fourth-highest for women (5%).6,18
Patients with CRC face multifaceted problems arising from the disease due to a lack of awareness about CRC risk factors and symptoms among the population.10,16 Studies have demonstrated that increasing the awareness of the general population about CRC may lead to a decrease in the prevalence and rising willingness to involve in cancer screening, early treatment, and may increase the survival rate.19-21
Awareness of CRC and its associated factors is crucial among the population in the prevention of CRC. Awareness of CRC is recognizing the risk factors and warning signs and symptoms of CRC. The risk factors of CRC include non-modifiable risk factors such as aging, gender, prior colon diseases such as inflammatory bowel disease, type 2 diabetes mellitus (DM-2), family history of the CRC, and polyp,22-25 and modifiable risk factors such as lack of physical activity, smoking, alcohol drinking, obesity, low fiber diet, high red meat, and low fruit and vegetable intake in the diet.13,26-29 The warning signs and symptoms of CRC are bloody stool, unexplained weight loss, change in bowel habit, anemia, lower abdominal lump, rectal bleeding, and chronic abdominal pain.30-33
Nevertheless, increasing the awareness of people about lifestyle modification, predictor identification, and recognizing warning signs and symptoms may be important to reduce CRC morbidity and mortality. Evidence showed that a multitude of factors may be associated with the awareness of CRC among adult patients. These may include gender, age, marital status, educational level, income, family history of CRC, heard about CRC, and source of information were the most predictors of awareness of CRC.34-38 However, there have not been studies about the awareness of CRC and associated factors among adult patients in the study area. Therefore, this study aims to assess the awareness of CRC and associated factors among adult patients in Jimma, South-West Ethiopia.
Methods and Materials
Study Design, Area, and Population
This institutional-based cross-sectional study design was employed from March to April 2020 at Jimma University Medical Center (JUMC) placed in Jimma town, located 354 km from the capital Addis Ababa within the South-West Ethiopia. JUMC is one of the largest public institutions giving service for cancer treatment and care in South-West Ethiopia. All volunteer adult patients (18 years and above) who had been attending adult medical and surgical outpatient clinic of JUMC during the data collection period were included, except patients who had a history of CRC, mentally ill, chronically ill, critically sick, visual and hearing disorder, and unable to speak during the data collection period.
The sample size was estimated by employing a single population proportion formula. This sample size yielded with considering marginal error (d) = 5%, 95% confidence level (CI), α = .05, and prevalence of 50%. The final sample size including the non-response rate yielded 422 patients. A systematic random sampling technique was employed to get allocated samples from JUMC. The number of monthly attended adult patients in the outpatient department of JUMC was [N = 14 559] from these, 485 patients were attended daily. For all cases [n = 422], K = N/n = 35 and K was between 1 and 35. First comer patients who registered in the health management information system case registry book took as a first sample and then every 35 intervals until getting the [485/35 = 14] samples with a day at the outpatient department.
Data Collection Tools, Procedures, and Validation
Data were collected using an interviewer-administered structured questionnaire. The data instrument included 2 parts. Part 1: socio-demographic data including information-related factors. Part 2 comprised Cancer Awareness Measure questions which were adapted from the University College London and Cancer Research in the United Kingdom (UK) in 2008 and were intended to examine the general public’s awareness of CRC in the UK with some modifications after serious literature review 39 and using question with “Yes or No” answers where “Yes” indicated for an exact response which scores 1. An accumulative mark of respondents on awareness of CRC ranging from 0 to 20 which was acquired by the accumulation of exact response to the 20-item questionnaire. A total mark of 15 or more (≥75%) was referred to as the respondents were attaining high awareness, whereas respondents who score less than 15 (<75%) were attaining low awareness. Cronbach’s alpha coefficient of the tool was .84.23,39-41 For this study, the instruments on awareness of CRC were interpreted to the Amharic version, then the local language Afan Oromo via a back-to-back translation approach. The instrument was certified before being used in this work as defined in the section. The certification result revealed that there was 96% consent between the Amharic, Afan Oromo, and English instruments. To assure the quality of data, the following measures were taken. A pre-test was conducted on 42 adult patients in Shenen Gibe General Hospital in Jimma Zone 1 week before the actual data collection and the questionnaire had been checked for its clarity, understandability, and simplicity. After the pre-test, the questionnaires were reviewed and reformatted based on the inputs and comments generated by seniors. After this, the internal consistency (Cronbach’s-α) in this study was .90 which can be considered adequate. The data were collected by 8 nurses holding Bachelor of Science degrees under the supervision of 2 professional senior nurses. Both the principal investigator and recruited supervisors had been responsible for supportive supervision on the spot and for reviewing all filled questionnaires on daily basis. Data collectors and supervisors were enrolled in training for 2 days on the objective of the study, instrument, and data collection procedures by the principal investigator. The supervisors were checking the questionnaire for completeness and closely supervise data collectors and presented it to the principal investigators. Moreover, the collected data were coded, cleaned, and explored by the principal investigator before analysis.
Data Entry, Analysis, and Presentation
The collected data were checked for its completeness and consistencies before data entry. Answers in each question were labeled for easiness of data entrance. The coded data were entered into Epi data version 4.6.0 and exported to SPSS version 25 for data analysis. Descriptive analysis, bivariate, and multivariate logistic regression models were carried out. The adjusted odds ratio (AOR) was used to determine the association between the dependent variable and independent variables with a statistically significant level at a 95% confidence interval (CI). Then, significant factors with a P-value < .25 in the bivariate logistic analysis were taken as a candidate for multiple logistic regression analysis. In both simple and multiple logistic regression models, the statistical significance of associations between variables was determined using AOR with 95% CI and P-value < .05. Then, the result of the study was presented in figures and tables.
Ethical Consideration
An ethical clearance letter was gained from the institutional Review Board (IRB) of Addis Ababa University College of Health Science (Protocol No. IRB/059/20/SNM). A permission letter was obtained from Addis Ababa University College of Health Sciences School of Nursing and Midwifery to the administrator of the study site. A letter of permission was secured from the administrative bodies of the hospitals. All of the study participants were informed about the purpose of the study; written informed consent was obtained and they are informed that participating in this study was fully voluntary. Besides, the confidentiality of the information was assured. The study was conducted following the Declaration of Helsinki. The IRB office in Addis Ababa University College of Health Sciences School of Nursing and Midwifery approved the consent process.
Results
Socio-Demographic Characteristics of Respondents
Socio-Demographic Characteristics of Respondents in Jimma, South-West Ethiopia, 2020 (n = 422).

Abbreviations: CRC, colorectal cancer; ETB, Ethiopian birr.
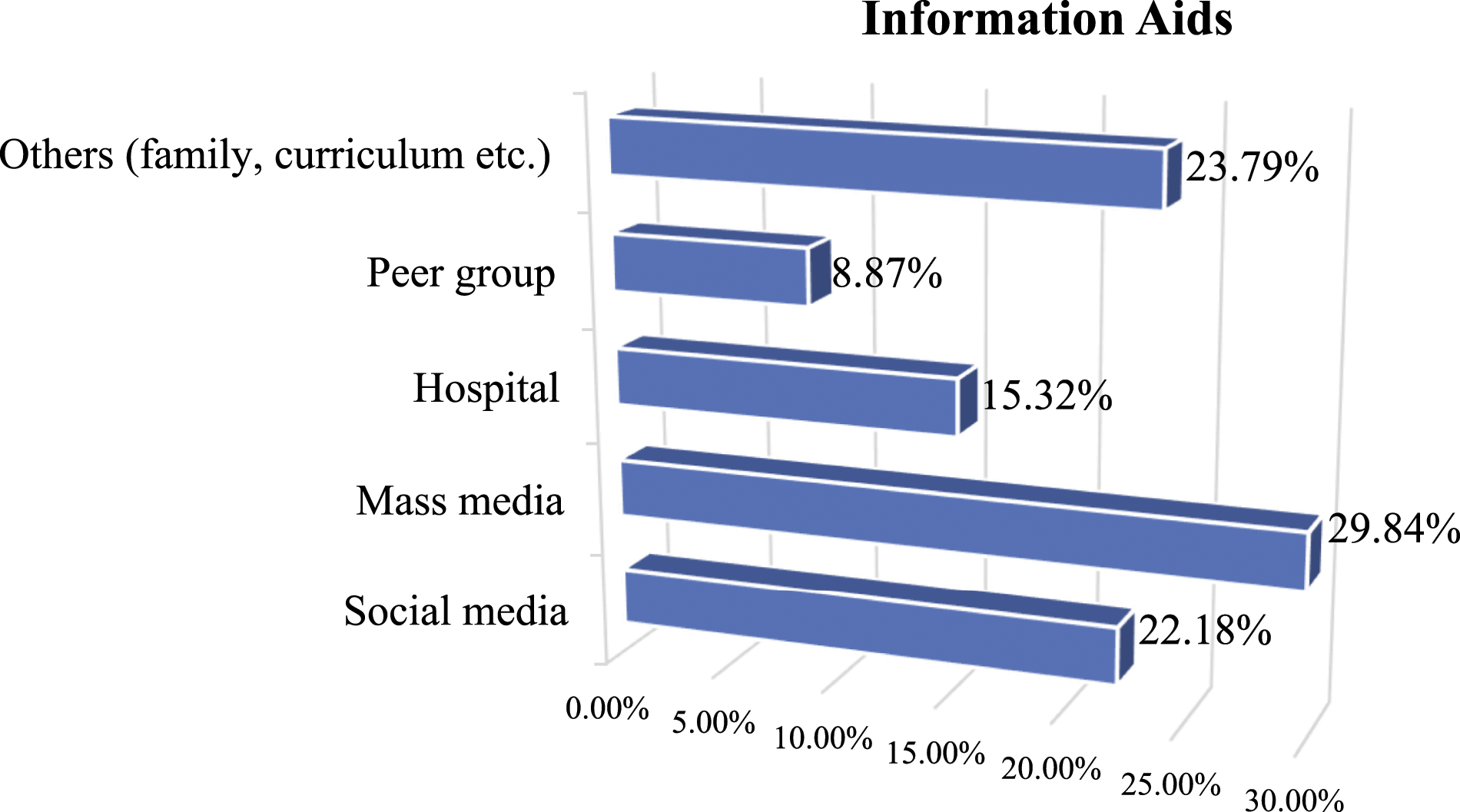
Sources of information about colorectal cancer among patients in Jimma, South-West Ethiopia, 2020 (n = 422).
Awareness of Respondents Toward CRC
Awareness of CRC Risk Factors and Symptoms of Respondents in Jimma, South-West Ethiopia, 2020 (n = 422).
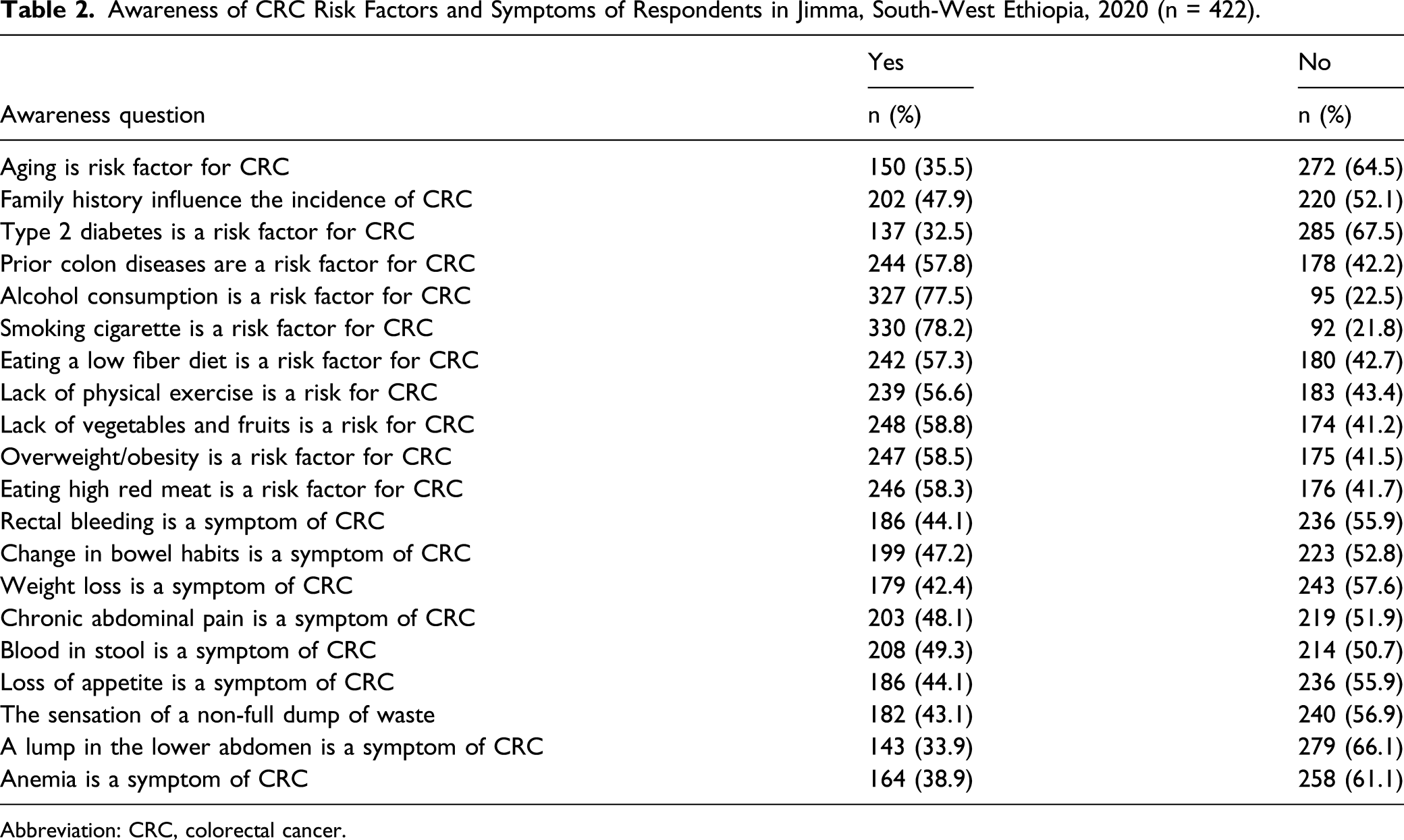
Abbreviation: CRC, colorectal cancer.
Factors Associated With the Awareness of CRC
The multivariate logistic regression showed that awareness of CRC showed a statistically significant association with gender, monthly income, residency, level of education, heard about CRC, information sources of CRC, and family history of CRC of adult patients. Respondents who were females had 1.86 times more likely to have a high level of awareness of CRC (AOR = 1.86; 95% CI: 1.26, 2.75) compared to males. Respondents who are residing in urban areas were 55% less likely to have a low level of awareness of CRC (AOR = .45; 95% CI: .30, .67) compared to those respondents residing in rural areas. Respondents who earn a monthly income of 3000 Ethiopian Birr (ETB) and above were 4.7 times more likely to have a high level of awareness of CRC (AOR = 4.72; 95% CI: 3.11, 7.15) compared to those respondents who earn below 3000 ETB.
Factors Associated With Awareness of CRC Among Respondents in Jimma, South-West Ethiopia, 2020 (n = 422).

Abbreviations: AOR, adjusted odds ratio; CI: confidence interval; COR, crude odds ratio; CRC, colorectal cancer; ETB, Ethiopian birr.
∗Statistically significant at P-value < .05.
Discussion
This study explored the awareness of CRC and associated factors among adult patients in Jimma, South-West Ethiopia, and found that about 42.4% of adult patients in Jimma had a high level of awareness of CRC. The finding of this study was lower than the findings of other studies conducted in the Kingdom of Bahrain (56%) and Pakistan (66.6%).22,42 This might be related to the fact that there is a difference in the socioeconomic status of the respondents, the study population, organizational policies, and access to the information related to CRC and its risk factors, which might be explained by the difference in the level of awareness of CRC. For instance, the study respondents in this study were adult patients, while respondents in the Pakistan study were included only young university students and might be getting awareness through the educational curriculum. Thus, increasing awareness of CRC of adult patients is a cornerstone for better prevention, early detection, and care of patients with CRC and cancer-related complications through health education and awareness campaign interventions.
Our study identified that gender, residency, level of education, monthly income, heard about CRC, information sources of CRC, and had a family history of CRC have an association with awareness of CRC of adult patients. This study revealed that respondents who were females had a high level of awareness of CRC compared to males. This finding is similar to other studies done in other settings that found female respondents had a high level of awareness of CRC.22,35,43-45 This discrepancy between genders might be due to females having more exposure to cancer-related health education or information connected to their reproductive health and females give attention to their health and have desired discussion. Therefore, male respondents need special emphasis when designing interventions aimed at improving the awareness of CRC.
This study shows that the respondents who were residing in urban areas had a high level of awareness of CRC compare to those who were from rural areas. This study finding is consistent with the study done in Malaysia. 46 The probable reason for this might be related to the fact that respondents residing in urban areas might have frequently got information through mass media (television and radio), social media, and they developed better awareness in using these types of information sources. Therefore, giving special attention to the respondents residing in rural areas is essential. This is done by bringing community-based health education to their dwelling places and encouraging them to get information through mass media.
Our study shows that respondents who cannot read and write, can read and write, and learn elementary school had a low level of awareness of CRC compared to those who had college and above educational level. This result is consistent with the study done in Bahrain. 22 The possible justification for this might be that patients with joined college and university might get information through curriculum and work experience about CRC, this might increase awareness of CRC toward risk factors and symptoms. Thus, special emphasis should be given to those respondents with lower-level education when designing health educational interventions.
This study shows that respondents who had a monthly income of 3000 ETB and above had a high level of awareness of CRC compared with those who had a monthly income below 3000 ETB. This result is supported by the study done in Malaysia. 34 This might be related to the fact that respondents who earn better monthly income were more satisfied by their income to initiated in gathering information with different information system like joining in different social media like the internet at home, Facebook, YouTube, and Telegram and using mass media like television and radio. Therefore, respondents with lower monthly income need special emphasis when designing and implementing interventions aimed at improving the awareness of CRC of this population group. This may involve the provision of economic support and giving them access to CRC-related community-based health education.
This study also shows that respondents who heard about CRC had a high level of awareness of CRC compared to those who never hear about CRC. This finding is consistent with the study done in other settings.37,38 The possible justification for this might be respondents who live in urban areas that may have access to health-related information or they may live nearby cancer awareness campaigns. This might be enhancing awareness about the important disease and increase personal disease preventive practice.
Our study also found that respondents who obtaining information through social media had a high level of awareness of CRC than those who get information through other sources (mass media and pear group). This result is corroborating with the study conducted in Saudi Arabia.37,38 The possible justification might be that information that was required by respondents was available at anytime and anywhere if the internet was available. It might be also that information through social media does not need a fixed period for obtaining information about CRC than others.
In this study, respondents who have a family history of CRC had a high level of awareness of CRC compared to those who did not have a family history of CRC. This might be related to the fact that respondents who had a family history of CRC have information about CRC and had a high level of awareness of CRC when compared to those who did not have a family history of CRC. Thus, respondents who did not have a family history of CRC require close attention to improve their awareness of CRC.
Strengths and Limitation of the Study
This study has a couple of strengths. One, it is the first study on awareness of CRC in Ethiopia. Second, the study had a 100% response rate. Our study also has numerous limitations. First, the use of an interviewer-administered structured questionnaire for data collection. Using this method to identify awareness about CRC and associated factors among adult patients might involve some risk, though qualitative interviews can let participants liberally highlight their concerns and obstacles concerning awareness about CRC. Second, the use of cross-sectional design does not allow inferring causality. Prospective and experimental studies are warranted. Third, the limitation of similar studies conducted in Ethiopia makes the comparison and discussion challenging. Fourth, the study was conducted in a healthcare setting and in 1 geographic area of Ethiopia which all affect the generalizability of the findings. Community-based studies within the different geographical areas of the county are warranted. Finally, the information obtained from study subjects could be subject to recall bias.
Conclusion
This study indicated that awareness of CRC of adult patients was inadequate (42.4%). Adult patients’ gender, residency, level of education, monthly income, heard about CRC, sources of information, and family history of CRC were found to be independent predictors of the awareness of CRC of respondents. Therefore, adult patients with male gender, residing in rural areas, low level of education, small monthly income, those who never hear about CRC, who get information through other sources (mass media and pear group), and those who did not have a family history of CRC could be targeted for awareness of CRC health education and initiating structured awareness campaigns interventions. In addition to this, promoting these activities on mass media and social media will help address information to a wider range of audiences.
Supplemental Material
sj-pdf-1-ccx-10.1177_10732748211033550 – Supplemental Material for Awareness of Colorectal Cancer and Associated Factors Among Adult Patients in Jimma, South-West Ethiopia: An Institution-Based Cross-Sectional Study
Supplemental Material, sj-pdf-1-ccx-10.1177_10732748211033550 for Awareness of Colorectal Cancer and Associated Factors Among Adult Patients in Jimma, South-West Ethiopia: An Institution-Based Cross-Sectional Study by Abdulmenan Hamza, Zeleke Argaw and Debela Gela in Cancer Control
Footnotes
Abbreviations
AOR, adjusted odds ratio; CAM, cancer awareness measure; CI, confidence interval; COD, crude odds ratio; CRC, colorectal cancer; DM-2, type 2 diabetes mellitus; ETB, Ethiopian Birr; HMIS, health management information system; IBD, inflammatory bowel disease; IRB, institutional review board; JUMC, Jimma university medical center; NCD, non-communicable disease; SSA, sub-Saharan Africa; UK, United Kingdom.
Acknowledgments
Our deepest gratitude goes to Addis Ababa University, School of Nursing, and Midwifery for financial support. We would like to extend our sincere gratitude to the data collectors, supervisors, and study participants for being involved in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The cost of the study was covered by Addis Ababa University.
Ethics Approval and Consent to Participate
This study was reviewed and approved by an Institutional Review Board of the College of Health Sciences, Addis Ababa University, Addis Ababa, Ethiopia (Protocol No: IRB/059/20/SNM). All participants provided written informed consent. The study was conducted following the Declaration of Helsinki.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.