
Abstract
Background:
Health-related Quality of Life (HRQoL) is a concept covering social, physical, psychological, and environmental factors. This study aimed to evaluate the HRQoL of medical students in Mogadishu, Somalia, using the WHOQOL-BREF instrument.
Methods:
This is a cross-sectional study design to assess QOL among medical students in Mogadishu, Somalia, between August and November, 2024 at selected public and private universities offering undergraduate medical programs. Data were collected using a structured self-administered questionnaire comprising socio-demographic variables (Gender, Age, Residence, Marital Status, Academic Year, and GPA). The WHOQOL-BREF instrument consists of 26 items grouped into 4 domains: physical, psychological, social, and environmental. Data were analyzed using descriptive statistics, ANOVA, and Regression with p < 0.05 were statistically significant.
Results:
The majority of students (57%) reported their overall QOL as “good,” while 22% reported it as “very good.” A significant association was found between age and psychological health (p = 0.011), with students above 25 scoring highest (76.82 ± 13.88) compared to those aged 21–24 (69.41 ± 15.27) and 18–20 (71.51 ± 15.90). Academic year showed a significant association with social health (p = 0.026), highest in years 3–4 (73.48 ± 20.72), followed by years 1–2 (71.46 ± 21.06), and lowest in years 5–6 (65.85 ± 27.29). In multivariate Age 21–24 years had association with the Psychological domain (β = –0.858, 95% CI: –1.672, –0.045).
Conclusions:
The study demonstrates that medical students in Mogadishu generally report a good QOL; however, it underscores the necessity for interventions aimed at improving psychological resilience and social support systems.
Introduction
According to the WHO, Quality of Life reflects a person’s subjective evaluation of their life situation, shaped by cultural norms, personal values, and individual objectives, expectations, and worries. 1 Since the 1970s, Quality of Life (QoL) has become a prominent focus in social research.2,3 “QoL” is a comprehensive concept that is influenced by various interconnected factors, including an individual’s physical health, mental well-being, degree of independence, social connections, personal values, and how they relate to key aspects of their surrounding environment.4–6
Medical students tend to experience a lower quality of life compared to the young people in the general population. 5 This reduced QoL has been linked to various long-term negative issues, such as the adoption of unhealthy lifestyles, the occurrence of psychological issues, poor academic performance, and other adverse effects that can hinder their overall professional growth and development.6–9 Medical students frequently experience significant personal distress throughout their undergraduate education. 8 Multiple studies, have shown that medical education and training can adversely impact students’ physical and mental health, leading to a decline in their overall quality of life.10–13
A lot of the contributing factors are related to either individual circumstances or institutional conditions. Conflict-affected countries, common risk factors that increase the vulnerability of medical students to this public health issue include a challenging learning environment, financial strain from educational debt, heavy academic workload, and disruptions in sleep patterns.14,15 Furthermore, medical students shows a high prevalence and severity of psychosocial distress and mental health conditions, including depression, anxiety, burnout syndrome, suicidal thoughts and attempts, sleep disturbances, as well as alcohol and substance use and abuse.13,16–19 Depression is a major mental health concern in Somalia, driven by prolonged conflict, displacement, poverty, and limited healthcare access, with a study among medical students at selected public and private universities in Mogadishu reporting a high prevalence rate of 58.6%. 14
The evaluation of QOL has been extensively studied in Western countries; however, there is a notable lack of research on this topic in developing nations,20,21 with particularly limited evidence from African contexts. 22 In Somalia, there is a clear lack of studies focusing on the QoL of medical students. Although one study conducted in Mogadishu examined health science students—specifically nursing students—it highlighted several challenges faced during clinical internships. These included ineffective communication, inadequate preparation, and strong emotional responses within the clinical learning environment.6,23
Therefore, the objective of this study is to assess the QOL of medical students in Mogadishu, Somalia using the WHOQOL-BREF instrument. Its hypothesized that Guided by these aims, the study hypothesizes that medical students in Mogadishu experience domain-specific variations in their QoL, and that both demographic and academic characteristics significantly influence these variations. It is hypothesized that the majority of medical students attending universities in Mogadishu experience a poor overall Quality of Life (QoL).
Methodology
Study design & population
This is a cross-sectional descriptive study design to evaluate the Quality of Life (QoL) among undergraduate medical students in Mogadishu, Somalia from August to November 2024. The reporting of this study conforms to the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology), 24 and the completed STROBE checklist is provided as a Supplemental File.
The study was conducted in selected public and private universities located in Mogadishu, Somalia, which offer undergraduate medical programs. These institutions were chosen based on accessibility, cooperation from administration, and student population size. The study population included all undergraduate medical students enrolled in the selected universities during the study period. This included students from first year to sixth year of medical training. The diverse inclusion across academic levels was intended to find variations in QoL throughout the course of medical education. Full-time medical students from selected universities were eligible if they provided informed consent. Exclusion criteria included : (1) completion of 6 years of medical school and (2) submission of an incomplete or largely invalid WHOQOL-BREF questionnaire.
Sample size determination
The sample size was calculated using the single-mean formula: (n = (Z1−α/2 × σ/d)²) to estimate the mean WHOQOL-BREF score. At a 95% confidence level, and based on a standard deviation of 0.95 for the overall QoL score reported in a previous study among medical students in Saudi Arabia. 6 After accounting for a 10% non-response rate, the final calculated sample size was 347. However, a total of 343 students were agreed to participate.
Sampling technique
A total of 343 medical students were selected using a convenience sampling method. Students were recruited over the course of 1 month, typically after their class breaks, by randomly inviting them to participate in the survey. The inclusion criteria were: students who were currently active, had not yet completed 6 years of medical school, and were willing to participate in the study. Students who declined to provide informed consent or submitted incomplete or invalid responses were excluded from the study
Data collection
Data were collected using a structured, self-administered questionnaire consisting of two parts: Section 1: Socio-Demographic Information Collected data on: Age, gender, academic year and self-reported GPA (Grade Point Average). Section 2: The WHOQOL-BREF instrument consisting of 26 items grouped into 4 domains: Physical, Social relationships, Environmental and psychological health to assess Quality of Life.
25
The instrument used a
Participants were given clear instructions and completed the forms anonymously. Completed questionnaires were collected in sealed envelopes to maintain confidentiality. To maintain the accuracy of the study, participants were instructed to fill out the questionnaire thoughtfully and independently. Sufficient time was provided to allow for careful consideration and review of their responses.
Study instruments, validation, and reliability
The WHOQOL-BREF instrument is a validated and widely used tool for assessing Quality of Life. 25 It consisting of 26 items designed to assess the four major quality of life domains defined by the WHO: physical health, psychological health, social relationships, and environment. Each item is rated on a five-point Likert scale, with response options ranging from 1 (very poor/very dissatisfied/none/never) to 5 (very good/very satisfied/extremely/always). Scores from the four domains are summed and then transformed positively, so that higher scores indicate better quality of life. Previous studies have evaluated the reliability and validity of the WHOQOL-BREF and confirmed its appropriateness as a tool for assessing quality of life.26,27 In this study, the English version of the instrument was administered, as the target population (medical student) were proficient in English.
Data analysis
Data were coded and entered into IBM SPSS version 27.0 for analysis. Descriptive statistics (means, frequencies, standard deviations) were used to summarize participants’ characteristics and QoL domain scores. One-way ANOVA and linear regression were used to examine differences in QoL scores across gender, academic year, and GPA categories. Data visualization included a pie graph for students’ self-reported overall QoL. A p-value < 0.05 was considered statistically significant.
Ethics consideration
Ethical approval for this study was obtained from the Research Ethics Committee of Jamhuriya University of Science and Technology (Ref: JUREC/0136/FMHS/052024). All participants signed an informed consent form prior to their involvement in the study. They were assured of the confidentiality of their responses and that all collected data would be used solely for the purposes of this research.
Results
Socio-demographic characteristics of participants
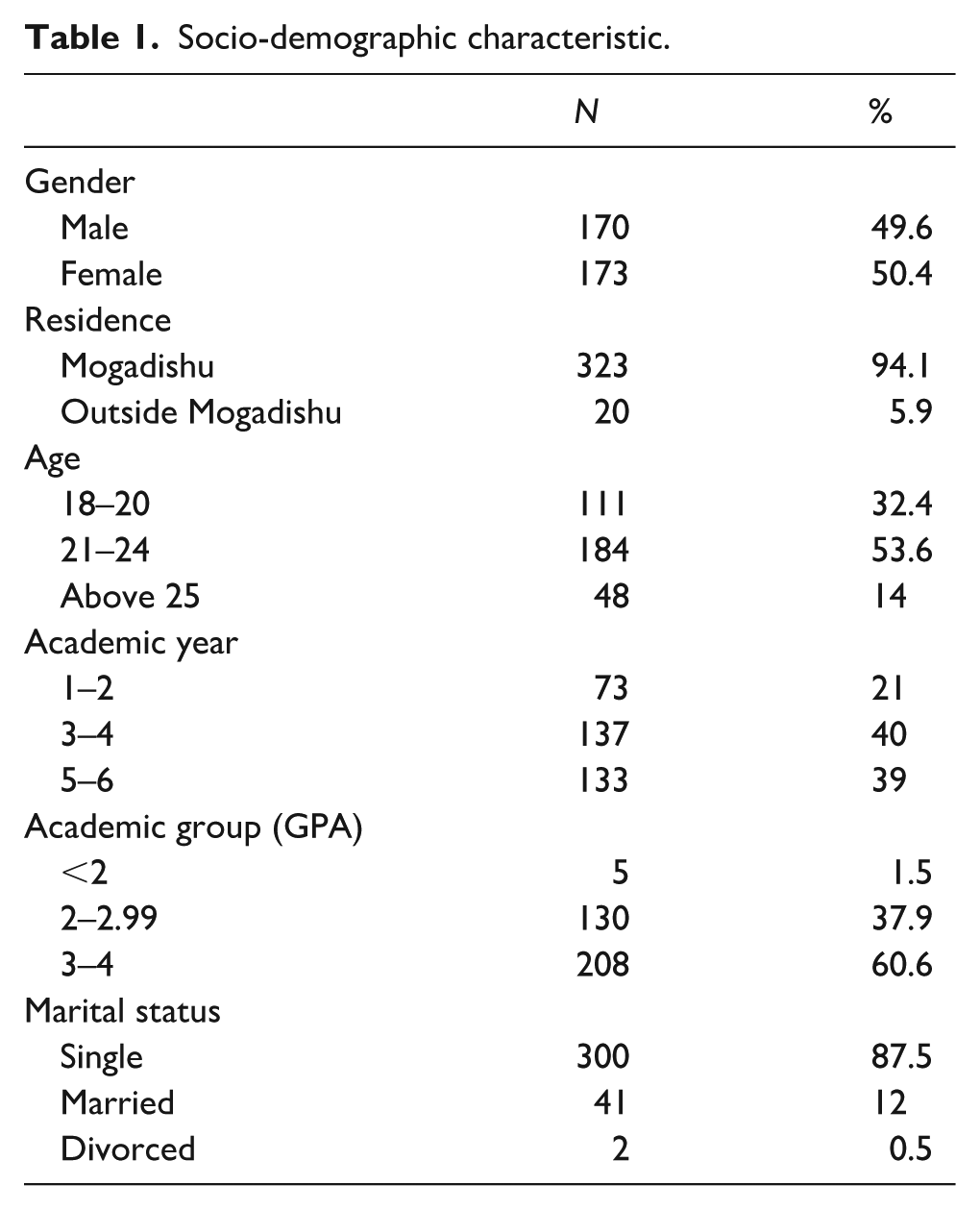
A total of 343 medical students participated in the study, with an almost equal gender distribution (49.6% male and 50.4% female). The vast majority of participants resided in Mogadishu (94.1%), while only 5.9% were from outside the capital. More than half (53.6%) were aged 21–24 years, 32.4% were 18–20 years, and 14% were 25 years or older. Regarding academic year, 21% were in their first or second year, 40% in years 3–4, and 39% in years 5–6. Most students reported a GPA between 3–4 (60.6%), followed by 2–2.99 (37.9%), while only 1.5% had a GPA below 2. In terms of marital status, the majority were single (87.5%), 12% married, and 0.5% divorced (Table 1).
Socio-demographic characteristic.
Overall quality of life
The majority of students (57%) reported their overall quality of life (QoL) as “good,” while 22% reported it as “very good.” About 16.16% reported their QoL as “neither poor nor good.” Only 3% and 2% of students reported their QoL as “poor” and “very poor,” respectively as shows in Figure 1.

Students’ self-reported overall QoL.
Quality of life domains by academic performance
When examining QoL domains across academic performance, students with higher GPA generally scored better. Mean psychological health increased with GPA, ranging from 70.0 among students with GPA < 2, to 74.2 among those with GPA 3–4 (Figure 2). A similar trend was observed for physical health, with mean scores rising from 67.9 in the lowest GPA group to 77.0 in the highest (Figure 3). Social health scores showed a non-linear pattern, lowest among students with GPA < 2 (63.3), peaking among those with GPA 2–2.99 (72.8), and then declining slightly in the highest GPA group (68.6; Figure 4). Environmental health improved steadily with GPA, from 50.0 in the lowest group to 59.4 in the highest (Figure 5)

Mean psychological health scores across different GPA categories.
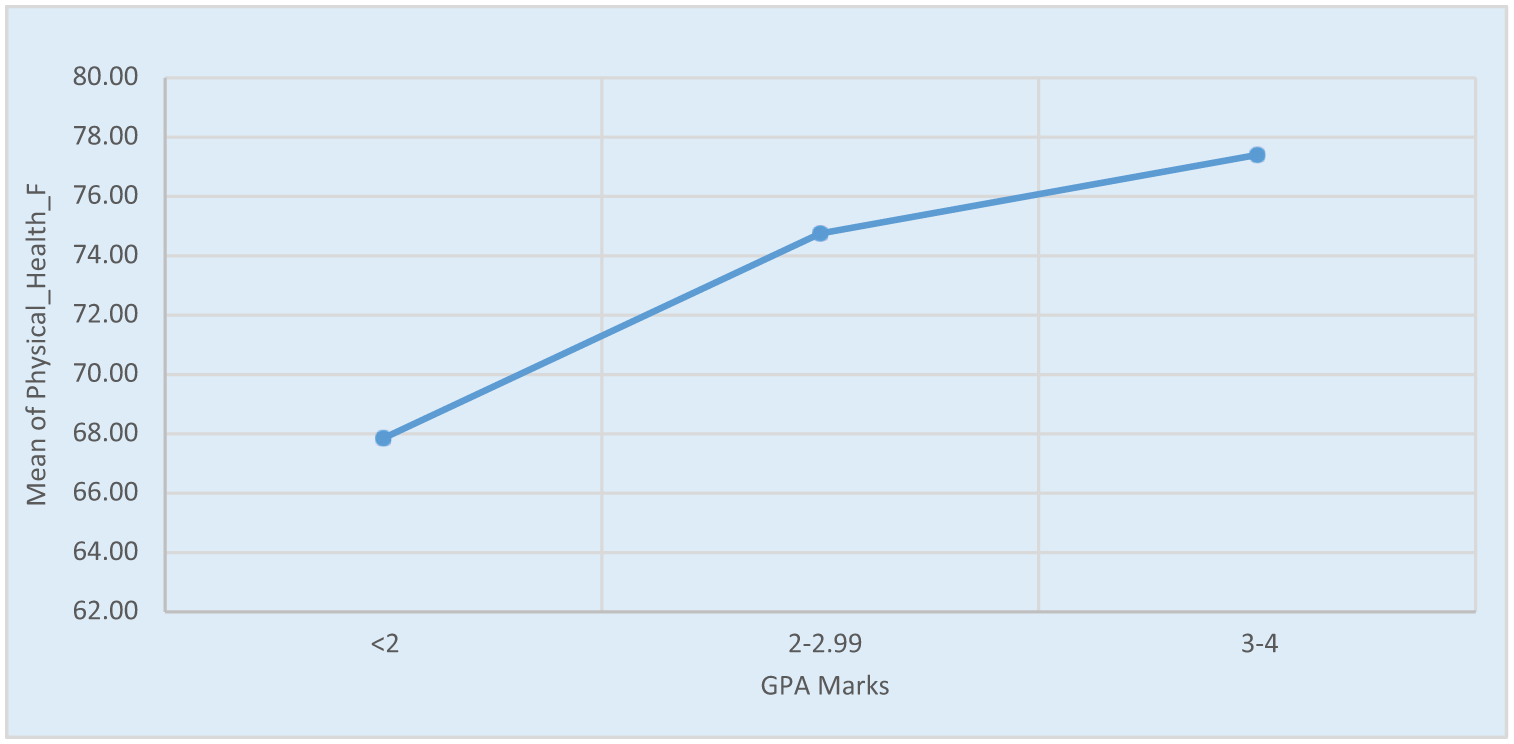
Mean physical health scores by GPA categories.
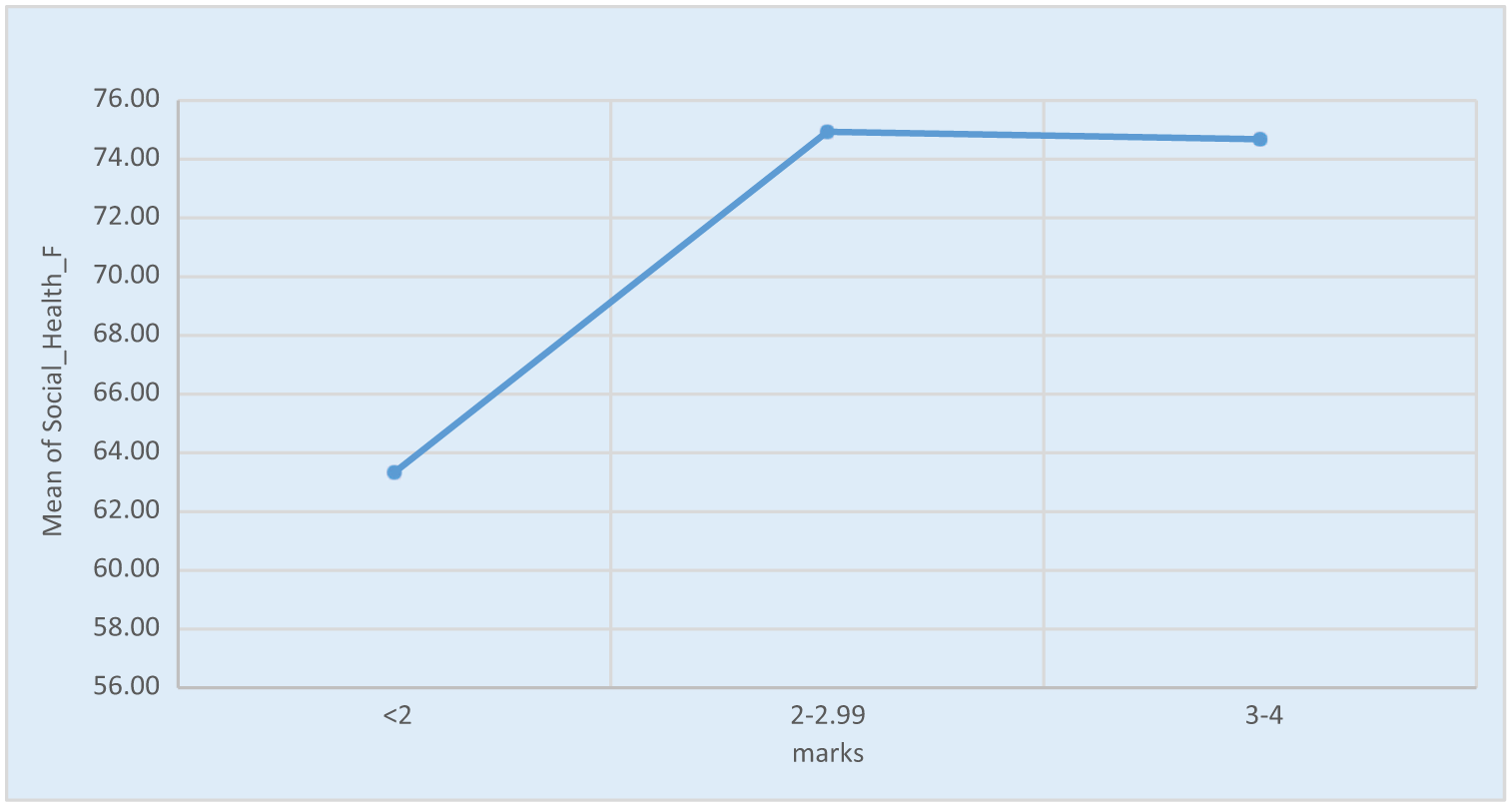
Mean social health scores by GPA categories.
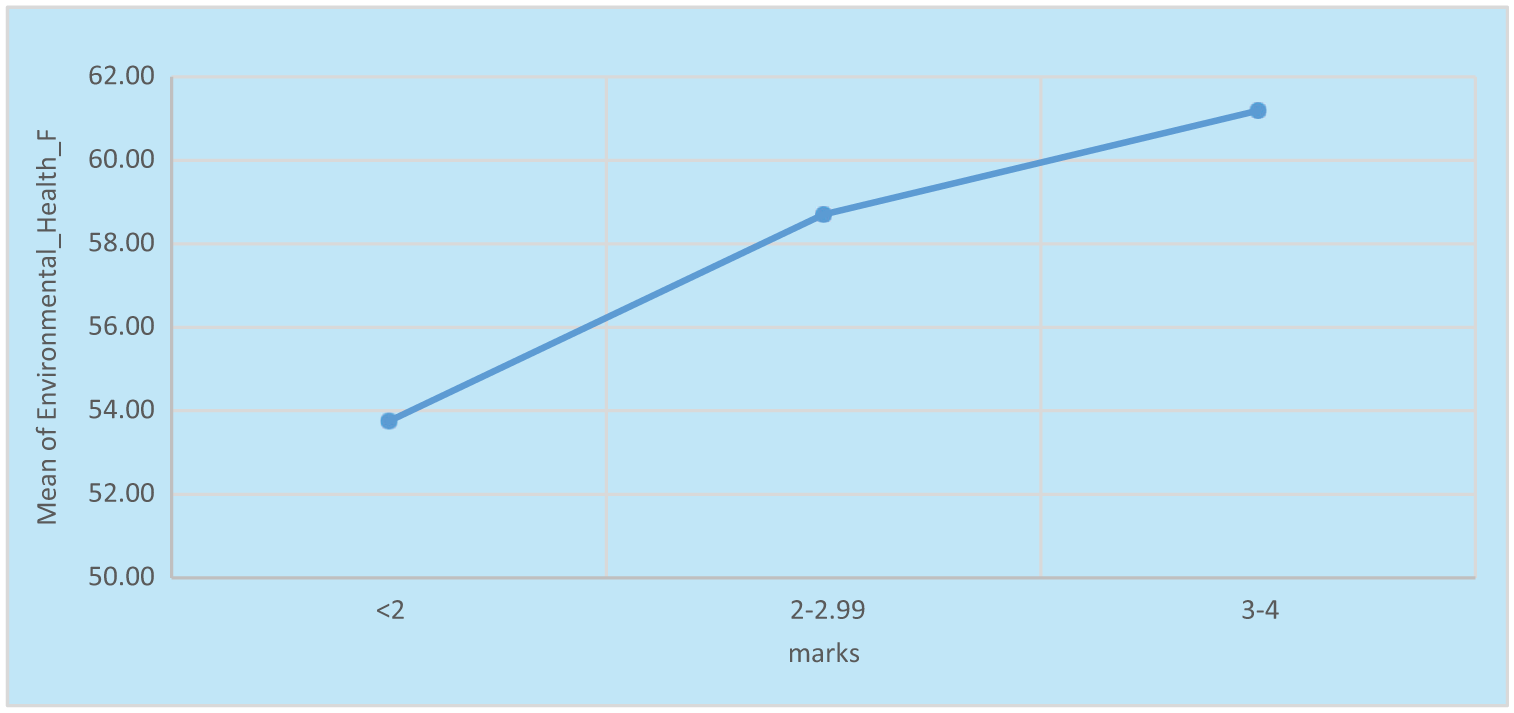
Environmental health scores by GPA categories.
One-way ANOVA across the domains of quality of life (QoL)
Gender, marital status, GPA, and residence were not significantly associated with any QoL domain. However, age and academic year showed meaningful relationships. Students older than 25 years had significantly higher psychological health scores compared to younger groups (p = 0.011, η² = 0.024). Social health also differed significantly by academic year (p = 0.026, η² = 0.020), with students in years 3–4 reporting better scores compared to their junior and senior peers (Table 2).
One-way ANOVA across the domains of quality of life (QoL).

indicate statistically significant at p < 0.05.
Multivariate regression
Multivariable regression analysis further confirmed these associations. After adjustment for potential confounders, being aged 21–24 years was negatively associated with psychological health compared to students aged ≥ 25 years (β = –0.858, 95% CI: –1.672, –0.045). No other socio-demographic or academic predictors were significantly associated with physical, social, or environmental domains. Marital status produced unstable estimates due to the very small number of divorced participants, limiting interpretation (Table 3).
Multivariate analysis.

indicate statistically significant at p < 0.05.
Discussion
This study aimed to explore the relationship between quality of life (QoL) domains—physical, psychological, social, and environmental health—and various demographic and academic variables among university students.
Somalia’s medical and health education system has long been hindered by prolonged conflict, instability, and resource constraints.28,29 Nevertheless, notable progress has been made in recent years with the reestablishment of the health sector through institutions. 14 Despite these improvements, challenges remain most notably the absence of a unified curriculum, a limited number of qualified instructors, and insufficient access to up-to-date teaching facilities. 14
In this study, students’ self-reported of their quality of life (QoL) showed that 22% rated it as “very good” and 57% as “good,” with a total of 79% reporting a favorable perception of their QoL. This percentage is slightly higher than the 73% reported in a similar study conducted in Saudi Arabia. 6 One possible explanation for the higher rate in Somalia could be that students may have lower baseline expectations or greater resilience due to adapting to challenging social and economic conditions, which can influence their perception of well-being.
The present study found that Psychological health was significantly linked to age, with students aged over 25 years reported better psychological health scores compared to their younger counterparts. In contrast a study conducted in UK highlighted that younger students, particularly those in their early years of medical education, often experience better psychological health compared to their seniors. 30 Another study also showed a significant association between psychological wellbeing and age, highlighting that while wellbeing tends to follow a U-shaped pattern in high-income countries, it often declines with age in regions such as Eastern Europe, sub-Saharan Africa, and Latin America, indicating that the relationship varies by cultural and regional context. 31 The latter may be due to increased academic pressure, career uncertainty, or life responsibilities experienced by older students. Possibly due to increasing academic pressure and reduced time for social interaction.
The current study also identified a statistically significant relationship between academic year and the Social Health domain. Which consistent with earlier researches from Australia and Sweden, which found that academic year significantly influences medical students’ quality of life.32,33 A possible justification could be that advancing through academic years exposes students to greater stress and workload, leaving them with less time and energy to maintain social relationships and support networks. University students, because of their academic environment and the unique challenges of this stage of life, may be prone to negative psychological conditions and behaviors, including anxiety and depression. 34
None of the remaining demographic variables gender, marital status, residence, and GPA, showed a statistically significant association with Quality of Life in this sample. Contrary to our findings, a 2012 study reported that female medical students in Pakistan experienced higher anxiety levels, which were linked to emotional sensitivity and cultural restrictions on women’s education. 35 Likewise, a systematic review of 40 studies indicated that female medical students in the US and Canada faced greater levels of personal distress. 36
In contrast to our result, study conducted in Saudi Arabia found Students with lower GPAs had a better psychological and social wellbeing compared to those with higher GPA. 6 One possible explanation is that high-achieving students often face intense pressure to maintain and enhance their academic performance. Furthermore, a study reported that living in a small town improves environmental, psychological, and social aspects of quality of life, which contrasts with the findings of our study. 37
Furthermore, unlike our study, previous research found a significant association between marital status and quality of life, with single men reporting significantly lower QoL scores compared to married men. 38 Due to ongoing socioeconomic challenges and instability in the region particularly in Somalia, marriage may not necessarily guarantee improved living conditions or psychological well-being.
To the best of our knowledge, this is the first study to assess quality of life among medical students in Mogadishu, Somalia. However, the study had certain limitations. Including academic performance was based on self-reported GPA, which was not independently verified. Lastly, although the WHOQOL-BREF questionnaire provided useful quantitative insights, employing more in-depth qualitative methods could offer a deeper and more accurate understanding of students’ quality of life and related experiences.
The quality of life of medical students is not only a personal well-being issue but also a critical public health concern, as it directly affects their academic performance, professional development, and future role in the healthcare workforce. In Somalia’s fragile health system, where human resources for health are already limited, ensuring medical students maintain good psychological and social well-being is essential for workforce retention and effectiveness.
In multivariate analysis, our study, students aged 21–24 years reported significantly lower psychological health compared to those aged above 24 years. This contrasts with broader population-based research indicating that psychological well-being tends to improve with age. 39 A possible explanation for this discrepancy is that medical students in early adulthood are often exposed to high levels of academic stress, financial pressures, and uncertainty about their professional future, which may undermine their psychological resilience.
Conclusion
This study is the first to assess the Quality of Life (QoL) among medical students in Mogadishu, Somalia, using the WHOQOL-BREF instrument. Most students reported good or very good QoL, yet psychological well-being was significantly influenced by age, while social health was shaped by academic year. These findings highlight the need for universities and policymakers to develop targeted support systems, such as mental health services for younger students and stronger social support networks for those in advanced academic years. Addressing these needs can improve student well-being, strengthen resilience, and ultimately contribute to building a more effective and sustainable healthcare workforce in Somalia.
Strengths and limitations of this study
This is first study to assess the quality of life assessment among medical students in Mogadishu, Somalia, addressing a significant gap in literature about healthcare education in fragile states.
Utilization of the validated WHOQOL-BREF instrument enables reliable, multidimensional quality of life assessment comparable with international studies.
Reliance on self-reported GPA and quality of life measures may introduce response bias, potentially affecting data accuracy regarding academic performance and subjective wellbeing.
One limitation of this study is the relatively small sample size, which may affect the generalizability of the findings to the broader population of medical students in Mogadishu.
Significance for public health
This study underscores the critical need to prioritize medical students’ quality of life in conflict-affected Somalia, as their well-being directly impacts future healthcare workforce resilience, mental health outcomes, and ultimately, national health system recovery.
Supplemental Material
sj-docx-2-phj-10.1177_22799036251407366 – Supplemental material for Quality of life (QoL) among medical students in Mogadishu, Somalia: A study using the WHOQOL-BREF instrument
Supplemental material, sj-docx-2-phj-10.1177_22799036251407366 for Quality of life (QoL) among medical students in Mogadishu, Somalia: A study using the WHOQOL-BREF instrument by Nur Rashid Ahmed, Ahmed Mohamed Dirie, Shafie Abdirahman Dirie, Sumayo Ali Shidane, Amiro Hussain Ibrahim, Sowda Nur Abdullahi, Hussein Abdullahi Hassan and Osman Abubakar H. M. Fiidow in Journal of Public Health Research
Supplemental Material
sj-pdf-1-phj-10.1177_22799036251407366 – Supplemental material for Quality of life (QoL) among medical students in Mogadishu, Somalia: A study using the WHOQOL-BREF instrument
Supplemental material, sj-pdf-1-phj-10.1177_22799036251407366 for Quality of life (QoL) among medical students in Mogadishu, Somalia: A study using the WHOQOL-BREF instrument by Nur Rashid Ahmed, Ahmed Mohamed Dirie, Shafie Abdirahman Dirie, Sumayo Ali Shidane, Amiro Hussain Ibrahim, Sowda Nur Abdullahi, Hussein Abdullahi Hassan and Osman Abubakar H. M. Fiidow in Journal of Public Health Research
Footnotes
Acknowledgements
The authors express their sincere appreciation to the Faculty of Medicine and Health Sciences at Jamhuriya University of Science and Technology and the Faculty of Health Science at Salaam University for their invaluable assistance and partnership throughout this study. Special thanks are also extended to the participants and data collectors, whose involvement was crucial to the completion of this research.
Ethical considerations
Ethical clearance for the study was granted by the Research Ethics Committee of Jamhuriya University of Science and Technology (Ref: JUREC/0136/FMHS/052024).
Consent to Participate
Written informed consent was obtained from all participants, who were assured of the confidentiality of their responses and informed that the data would be used strictly for research purposes.
Author contributions
Nur Rashid Ahmed, Ahmed Mohamed Dirie, and Shafie Abdirahman Dirie conceptualized and designed the study. Sumayo Ali Shidane, Amiro Hussain Ibrahim, and Sowda Nur Abdullahi contributed to data collection and data entry. Osman Abubakar H.M.Fiidow, Hussein Abdullahi Hassan assisted with data analysis and interpretation. All authors contributed to drafting and revising the manuscript, approved the final version, and agree to be accountable for all aspects of the work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data supporting this study are available from the corresponding author upon reasonable request.
Open practices
This article is distributed under the terms of the Creative Commons license, allowing unrestricted use, distribution, and reproduction, provided the original work is properly cited.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.