
Abstract
Background:
Mental illness is a widespread issue that affects millions of people worldwide. Its impact is not only limited to the individuals suffering from it but also extends to their families and communities. Caregivers suffer physically, psychologically, and socially twice than general population related to care giving process.
Methods:
An institutional-based cross-sectional study design was employed from January 21 to February 21, 2024, at public hospitals in Harari Regional State and Dire Dawa City Administrative; 437 primary caregivers were selected via a systematic sampling technique. Data were collected using interview-administered questionnaires. Simple and multiple linear regression analysis were used to assess the contributing factors of quality of life domains among the participants, and the ꞵ-coefficient with a 95% confidence interval was used. Statistical significance was accepted at a P-value < .05.
Results:
A total of 421 respondents participated, for a response rate of 96.3%. The results found that the mean quality of life scores of caregivers of people living with mental illness for each domain (mean ± SD) were 58.05 ± 18.81, 57.29 ± 16.28, 51.19 ± 23.12, and 53.04 ± 16.13, for physical, psychological, social and environmental factors, respectively. Multiple regression analysis revealed that the caregiver’s educational status, depression, perceived stigma, perceived burden and patient’s diagnosis were negatively associated with all domains of quality of life, whereas the caregiver’s resilience and social support were strongly positively associated with all domains of quality of life.
Conclusion:
Caregivers’ quality of life found to be low across the four domains of quality of life, with the lowest score in the social domain. Resilience and social support found to plays a positive role in the quality of life of caregivers. Regular evaluation of risky caregivers, and psycho-support are crucial to address these challenges and improve caregivers’ well-being.
Introduction
A mental illness is a condition that alters a person’s mood, behavior, or thought processes. 1 While emotional, cognitive, and behavioral problems are hallmarks of mental illnesses, mental illnesses also manifest as distress or trouble in completing routine duties at work, at home, or in social settings. Mental illness affects people of all ages, educational levels, income levels, and cultures and has a substantial effect on the family. 2
Quality of life (QOL) is a person’s assessment of their situation in relation to the different social, cultural, and value systems in which they live. QOL encompasses many facets of an individual’s existence, including financial stability, achieving personal objectives and expectations, social and psychological well-being, and physical, mental, and emotional health.3 -7
Primary caregivers refer to any person either a family member or relative who has most frequent contact with the patient and provides unpaid support to the patient financially, socially, psychologically, and physically.8,9
One in every four families has a member who is currently dealing with some form of mental illness and more than 90% of these individuals receive continuous support from their families.10,11 It is also estimated that the cumulative global impact of mental disorders in terms of lost economic output would amount to $16.3 trillion over the coming 20 years. 12
A study has revealed that 72.7% of family caregivers for individuals with severe mental illness reported a poor QOL. 13 In Sub-Saharan Africa as many as 86% of caregivers of mentally ill patients experiences low. Beside this the lack of interventions for counseling, training or supporting them has been exaggerated negative impact on caregivers’ QOL.14 -17 It has been found through a study that a significant proportion of caregivers of patients with mental disorders experience a considerable level of burden, with almost 63.3% of them falling under the moderate to severe level of burden. 18 Perceived stigma among caregivers of people with severe mental illnesses was as high as 75%19,20 and the prevalence of common mental disorders among informal caregivers in Ethiopia accounted for 40.5%. 21 Such social, economic, and psychological changes found to be greatly impact the caregivers’ QOL.22,23
Physical, psychological, and social challenges due to the demands of caregiving process estimated to be double among caregiver of PLWMI compared to general population.11,24 -27 This may lead caregivers to diminished life expectancy, and compromised well-being.25,28 Also, the QOL of caregivers is important in maintaining patients’ aid recovery and stability, the progress, and outcome of the patients.29 -31
Previously conducted research among low- and middle-income countries found that the lowest mean score of caregivers QOL (8.696 ± 2.59 to 18.8) in social domain and the highest mean score of caregivers QOL (21.397 ± 5.59 to 56.3 ± 17.4) in environmental domain of caregivers QOL.32 -36 While research among studies conducted in high- and upper-income countries found that the lowest range of caregivers QOL mean score (11.0 ± 4.7 to 64.42 ± 17.74) in social domain and the highest range of caregivers QOL mean score (12.34 ± 2.25 to 70.45 ± 13.08) in psychological domain of caregivers QOL.28,31,37 The severe impairment associated with mental illness leads to a strong dependence of patients on caregivers. 38 The relationship between the quality of life of caregivers of individuals with mental illness and socio-demographic, clinical, psycho-social, and substance-related factors has been explored in previously conducted studies. 13
In Lower and Middle Income Countries (LMICs), the ratio of patient to mental health professional is low and there is limited availability and adequacy of rehabilitation center which cause limited access to modern mental health care.39,40 This huge treatment gap ultimately affects the QOL of caregivers and their relatives.41,42 Interventional based research found that Caregiver-focused interventions appear to improve the experience of caring, quality of life and reduce psychological distress among caregiver. 43
It is remarkable to note that mental health professionals commonly focus exclusively on the primary patient. 11 Beside this the lack of interventions for counseling, training or supporting caregivers has been exaggerated negative impact on caregivers’ quality of life as well as data showed that even in developed country 10% of caregivers of mentally ill patients get counseling. 44
Despite this diverse and complicated out comes, quality of life of caregivers of PLWMI is not well addressed in developing countries, including Ethiopia.
There was paucity of research in Ethiopia with the previously published paper was conducted in the northern part of Ethiopia which means caregivers from the other corner of the country were not addressed and the previously conducted research didn’t incorporate some crucial factors related with care giving process such as caregiving burden and resilience.
The key findings of this study can significantly inform policymakers in resource-limited settings, including Ethiopia, by highlighting specific needs and providing significant factors to be addressed through different strategies. It also demonstrates the extent of caregiver burden, stigma, and emotional distress, revealing the pressing need for support systems and effective coping strategies by examining the resilience of caregivers. Besides this, studies reveal the significant impact of readily available support groups and brief psychoeducational intervention regarding caregiving challenges. Overall, the finding of the study provides useful information for policymakers regarding the design and implementation of programs that guarantee the consideration of primary caregivers in mental health services and community mental health programs, raising awareness toward the impact of stigma, caregiving burden, social support, and resilience on the overall quality of life of caregivers.
The goal of this study was to assess the status of caregiver QOL among caregivers of PLWMI, to enable healthcare professionals to be capable of identifying caregivers with low QOL and counseling them, will be helpful for healthcare planners and program managers for designing specific and scientifically sound interventions suitable for caregivers in optimizing their social support and resilience to ensuring their QOL.
Therefore, this study aimed to assess the QOL of primary caregivers and identify associated factors with caregivers QOL, with consideration of new variables like perceived burden, and resilience among primary caregivers of patients with mental disorder attending follow-up treatment at public hospitals in Harari regional state and Dire Dawa City Administration.
Conceptual Frame-Work
Taking the broad concept and complexity of caregiving process, stress process model was compatible to establish theoretical frameworks that illuminate the multifaceted nature of caregiver quality of life. 45 Stress process model has three key categories of factors contribute to caregiver’s quality of life. The first category is background factors: these are the individual characteristics and social contexts that shape a person’s experience of stress. They include the demographic variables of caregiver46 -48 and patient.46,47,49 The second category is stressors. According to stress process model, stressors are specific events that create demands on the individual. Stressors include the disease-related characteristics of caregivers and care recipients.14,48,50 -52 The third category is mediator. These are the mechanism that influences how stressors impact an individual’s mental and physical health. This may include social resources, psychological factors and caregiving related mental health as well as psychoactive substance use.7,13,35,36,46,51,53 -56 Overall, stress process model highlights the complexity of the stress experienced by illustrating how background factors shape exposure to stressors and how mediators can exacerbate the effect of those stressors on well-being of individual (Figure 1).

Conceptual framework for study to assess possible factors associated with quality of life among primary caregivers of people with mental illness constructed from different literature.
Methods and Materials
Study Setting, Study Design, and Period
An institutional-based cross-sectional study design was employed at public hospitals found in the Harari Regional State and Dire Dawa City Administration. Harar is the capital city of the Harari Regional State, which is located 525 km away from Addis Ababa, the capital city of Ethiopia, to Eastern Ethiopia. There are 6 hospitals, 8 health centers, and 22 health posts Harari Regional State. However, there are only two public hospitals known to provide psychiatric services. Namely, Haramaya University Hiwot Fana Comprehensive Specialized Hospital (HU-HFCSH) and Jogula General Hospital (JGH). Dire Dawa is located 526 km away from the capital city of Addis Ababa and 47 km from Harar town. In terms of the distribution of health facilities, the city has two governmental hospitals and 8 health centers. However, only two public hospitals are known to provide psychiatric services. Namely, Dil-Chora Referral Hospital (DCRH) and Sabean General Hospital (SGH). An institutional-based cross-sectional study design was conducted from January 21 to February 21, 2024.
Source Population Study Population and Their Eligibility Criteria
The source population of the study was all primary caregivers of PLWMI on follow-up at HU-HFCSH, JGH, DCRH and SGH. The study population included all selected primary caregivers of patients living with mental illness in HU-HFCSH, JGH, DCRH, and SGH during data collection period. All primary caregiver of people with mental illness whose age ⩾18 and all primary caregivers give care at least for at least 6 months were included in the study. While primary caregivers who were severely ill were not included in the study.
Sample Size Determination
For analysis relies on linear regression; the more appropriate method for justifying the sample size should consider the number of predictors, expected effect size, significance level (α), and desired statistical power (typically .80). accordingly, G*Power 3.1 software was used to calculate minimum sample size with the assumption of medium effect size (.15), α error probability (.05), and number of predictors, 22 which yields a sample size of 163. Beside this we have used single mean population formula with the assumption of 13.82 = standard deviation of the mean quality of life score; from a previously published study in Ethiopia, 35 and with a margin of error of 1.36 units which yield final sample size of 437 with 10% nonresponse rate.
The number of samples required for the study was calculated using single population mean.

Where:
n = Minimum required sample size.
Zα/2 = Standard normal distribution with 95% confidence interval at (α = .05) = 1.96.
δ = Standard deviation (SD) of the overall QOL score (SD = ± 13.82), was taken from previously published study at Dessie Referral Hospital. 35
d = margin of error = 1.36.
Thus, by substituting those value we got a minimum sample size of 437 with 10% non-respondent rate. But due to the sample size determined using the single mean population formula (n = 437) was greater than that of the sample size determined with G*Power 3.1 software (n = 163), we kept the sample size calculated by the single mean population formula.
Sampling Procedures
Systematic random sampling with proportional allocation was employed to select the study participants from each hospital. Initially, the total expected number of caregivers of PLWMI during the study period was calculated from the records of the hospitals. The sampling interval (K) was subsequently determined by dividing the total number of eligible individuals (945) by the sample size to be drawn (437). The lottery method was used to select the first participant between one and K. Then, data were subsequently collected from each study participant with a K interval of “2” until the desired sample size was reached (Figure 2).

Schematic presentation of sampling procedure of study samples from all study areas, Harari Regional State and Dire Daya Administrative City, Ethiopia, 2024.
Data Collection Tool Preparation
The dependent variable was measured using the WHOQOL-BRFE. WHOQOL-BRFE has 26 items. This questionnaire consists of two parts. The first, part evaluates the individual’s overall perceptions of QOL and the person’s overall perception of health. The second part evaluates the four domains: physical health domain, psychological health domain, social relationships domain, and environmental health domain. These four domains scores denote individual’s perception of life in a particular domain. Each of these items was scored as a five-point Likert scale. The tool raw scores were transformed in to a range between 0 and 100 and they are scaled in a positive direction (ie, higher scores related to a better health related QOL and vice versa). This tool was cross-culturally validated instrument to measure the QOL at health care settings with good sensitivity and specificity. It was revealed that WHOQOL-BREF Scale had a high internal consistence reliability coefficient (physical domain = 0.853, psychological domain = 0.832, social domain = 0.880, and environmental domain = 0.79). 57 In this study the Cronbach alpha was α = .88 for physical domain, .81 for social domain, .78 for psychological domain, and .86 for environmental domain. 57
The raw score of each domain was transformed into 0 to 100 scale using the formula shown below 58 :

Where:
Actual raw score: is the values achieved through summation of each domain facet,
Lowest possible raw score: is the lowest possible value that could occur through summation of each domain facet, and
Possible raw score range: is the difference between the maximum possible raw score and the lowest possible raw score of each domain.
Oslo social support scale (OSSS-3): was used to assess support level of study participants. It consists of 3 items with a total score ranging from 3 to 14. A higher score indicates stronger levels of social support, and vice versa. 59 In the current study, the OSSS-3 showed good internal consistency of .82.
The global clinical impression: was used to assess severity of illness among the patients. The CGI score was categorized into three levels (mildly ill = “1-3”, moderately ill = “4”, and severely ill = “5-7”) for both subjective and objective severity assessment. 60
The Patient Health Questionnaire (PHQ-9): was used to assess depression among the study participants. It is a 9-point item questionnaire measured on a 4-point Likert scale ranging from 0 (“not at all”) to 3 (“nearly every day”), generating a complete score ranging from 0 to 27. A cutoff point of 10 and above was used to screen for depression among the study participants. PHQ-9 has been validated in Ethiopia with sensitivity and specificity of 67% and 86% respectively. 61 In the present study, the PHQ-9 showed good internal consistency of .81.
The Generalized Anxiety Disorder Scale (GAD-7): was used to screen anxiety. It is a 7-point item questionnaire measured on a 4-point Likert scale ranging from 0 “not at all” to 3 “nearly every day”, generating a complete score ranging from 0 to 21. A cutoff point of 10 or above on the GAD-7 scale was used to define presence of anxiety. 62 In the current study, the GAD-7 showed good internal consistency of .84.
The Family Interview Schedule (FIS) questionnaire: was used to assess perceived stigma among primary caregivers. It 14 items questionnaire rated on a four-point Likert scale ranging from, “not at all” to “always”. The higher the score is, the greater the perceived stigma. 63 The internal consistency in this study was .91.
The short-form Zarit Burden Interview (ZBI-12): was used to assess the perceived burden among the study participants. This scale has 12 items, and they are defined subjectively. Each item is graded on a 4-point Likert scale ranging from never to almost always present. The total ratings range from 0 to 48. The higher the score is, the greater the perceived caregiver burden. 64 In the current study, the ZBI-12 showed good internal consistency and had a Cronbach’s alpha of .95.
The Brief Resilient Coping Scale (BRCS): was used to assess the resilience level of the study participants. This scale has 4 items with 5 possible answers given a score of 1 to 5, with 1 being “Does not describe me at all” and 5 being “Describes me very well”. The total score is a minimum of 4 and a maximum of 20. The higher the score is, the greater the degree of the coping mechanism. 65 In the current study, the tool has a Cronbach’s alpha of .87.
Operational Definitions
Primary caregiver: A family member/relative/any person who has most frequent contact with the patient, provides unpaid support to the patient financially, socially, psychologically, and physically, and has mostly been collateral in the patient’s treatment visit. 66
Quality of life: Scores range from 0 to 100 on WHO-BREF with high score close to 100 indicates higher QOL and low score closer to 0 indicates lower QOL. 67
Physical health domain: it is subscale of WHOQOL-BREF containing 7 items on energy, pain, sleep, mobility, rest and daily working capacity with raw score range from 7 to 35. 58
Psychological health domain: it is subscale of WHOQOL-BREF containing 6 items covers self-image, self-esteem and attitudes, memory, concentration, learning ability, and mental status with raw score range from 6 to 30. 58
Social health domain: it is subscale of WHOQOL-BREF containing 3 items measures personal relationship, sex life, and social support with raw score range from 3 to 15. 58
Environmental health domain: it is subscale of WHOQOL-BREF containing 8 items measures issues related to safety, health and social services, living physical environment, opportunities to acquire new skill and knowledge, financial resources, recreation, and transportation with raw score range from 8 to 40. 58
Social support: any physical and psychological comfort provided by other people as measured by the OSSS-3. Higher score of the tool indicates higher level of social support. 59
Severity of illness: participants with CGI score 1 to 3 were considered as mildly ill, while those with score of 4 and 5 to 7 were considered as moderately ill and severely ill, respectively. 60
Anxiety: study participant who scored 10 and above on GAD-7 scale considered as having probable case of anxiety, while those with less than 10 considered as possible case of anxiety. 62
Depression: study participant who scored 10 and above on PHQ-9 scale considered as having probable case of depression, while those with less than 10 considered as possible case of depression. 61
Perceived stigma: the degree to which caregivers dealt with negative attitudes from others because of their relatives’ illness measured by the FIS questionnaire higher value of the scale indicating stigma in the total score. 63
Substance use: participants those used substance during life time were considered as ever substance users, while those used substance since the last 3 months considered as current substance users. 68
Caregiver burden: any negative or unwanted consequence to the family members caused by providing care for mentally ill relatives measured by the ZBI-12. The higher score of the ZBI-12 indicate higher level of caregiving burden. 64
Resilience: The cognitive, emotional, and behavioral methods of dealing with problems as measured by the BRCS-4. Higher scores of the tool indicate higher levels of coping. 65
Data Quality Assurance
The questionnaire was prepared first in English then translated into to local language Afan Oromo, Amharic, and Somali language. Then it was back translated to English to insure the consistency of the tools. Pre-test study was conducted on 5% (n = 22) of the sample population 1 week before the actual data collection at Bisidimo Hospital to check for the consistency of the tool. Data collectors and supervisors were trained for 1 day. Throughout the data collection supervision was made by the supervisor to keep the quality of data to its maximum. The collected data were checked for completeness of each questionnaire at the end of the data collection.
Study Variables
Outcome Variable
Quality of life domains (physical, psychological, social, and environmental domain)
Independent Variables
Socio-demographic factors of caregiver and patient: Age of caregiver and patient, Sex of caregiver and patient, Residence, Educational Status of caregiver and patient, Occupational Status, Marital Status of caregiver and patient, and Kinship with the patient.
Clinical related factors of caregiver and patient: Chronic medical illness in caregiver and patient, caregiver depression, and Anxiety, history of mental illness among caregivers, and history of mental illness among other family members.
Psycho-social factors: Social support, perceived stigma, perceived burden, resilience, daily caregiving hours, and caregiving duration.
Substance-related factors: life time and current caregivers Alcohol, Khat, Tobacco, cannabis or/and others use.
Data Management and Analysis
The collected data were checked, coded, entered into Epi-data version 3.1, and then exported to STATA version 14 for analysis. The assumption of linear regression was checked prior to analysis. The normality of the residuals was checked by skewness and kurtosis tests for normality. The range value between −1 and +1 of skewness was considered as normal distribution of residuals. No heteroscedasticity was detected by the Breusch-Pagan-Cook-Weisberg test (P-value > .05). There were no potential outliers, as checked by Cook distance. Accordingly, the absolute value of cook distance <±1 was taken as the cutoff point, and there were no observed influential outliers. The multicollinearity among the independent variables was checked by variance inflation factor (VIF). A VIF cutoff point <10 was used to declare multicollinearity, and there was no issue of multicollinearity. After fitting the regression model, residual plot was checked in which the residual plot shows even distribution of residuals. Lastly, goodness-of-fit model was evaluated with adjusted R2. Accordingly, the adjusted R2 of the final model was 75.12% in the physical domain, 60.89% in the psychological domain, 67.45% in the social domain, and 70.23% in the environmental domain of caregiver QOL. In simple linear regression analysis, variables with P-value < .25 were considered candidates for multiple linear regressions to establish the variables that independently predict QOL through forward selection. One strength of forward variable selection is its ability to identify strong predictor variables that enhance the explanatory power of the regression model. It also helps distinguish predictors that contribute significantly to the variance in caregiver QOL. Variables with a P-value of less than .05 in the multiple linear regression were considered statistically significant, and an unstandardized β coefficient was used for interpretation. Descriptive statistics such as the means, standard deviations, medians, interquartile ranges (IQRs), proportions, frequencies, and percentages were used to describe the outcomes and independent variables in the study. Finally, the results of the study were summarized by using tables, graphs, and narrative descriptions (Supplementary File 3).
Ethics Approval and Consent to Participate
Ethical clearance was obtained from the Institutional Health Research Ethics Review Committee (IHRERC) of Haramaya University College of Health and Medical Sciences. Informed, voluntary, written and signed consent was obtained prior to data collection from each participant after a brief explanation about the purpose and objectives of the study and for participants was provided. For participants who were unable to read and write, fingerprints were taken. The participants were informed that they had the right to withdraw from the interview at any time they wished. The collected data were kept confidential and used only for the purpose of the study. All the necessary methods were carried out in accordance with the institutional guidelines and the Declaration of Helsinki. Furthermore, to minimize social desirability effect of sensitive issues the data collectors provided guarantee for participant privacy, in which the interviews were took place in an isolated area, a place where others were not present in the waiting room.
Results
Socio-Demographic Characteristics of Caregivers
A total of 421 primary caregivers of PLWMI participated in this study, resulting in a response rate of 96.3%. The median age of study participant was 30 years. There was an almost equal distribution of gender among participants, with a modest majority being female (52.97%). More than half of the study participants 239 (54.39%) were married. Majority of respondents (53.44%) lived in rural areas, and 31.12% were engaged in farming. Low educational attainment (33.73%) was notable among the study participants (Table 1).
Socio-Demographic Characteristics of Caregivers of People Living with Mental Illness at Harari Regional State and Dire Dawa Administrative City Public Hospitals, Ethiopia, 2024 (N = 421).

Catholic, Waqefata, Johva witness.
Gurage, Tigre, Wolayita.
Daily laborer, unemployed, retired.
Aunt, uncle, grandmother/father.
Socio-Demographic Characteristics of People Living with Mental Illness
More than half 250 (59.38%) of the patient were male and the median age of the patients was 30 years, with an IQR of 19 20 years (median꓿30; IQR꓿ 25-45). Regarding marital status 223 (52.97%) of the patients were married and regarding to their educational status about one third of the patients were attend primary school (Table 2).
Socio-Demographic Characteristics of People Living with Mental Illness at Harari Regional State and Dire Dawa Administrative City Public Hospitals, Ethiopia, 2024 (N = 421).

Clinical Characteristics of Caregivers of People Living with Mental Illness
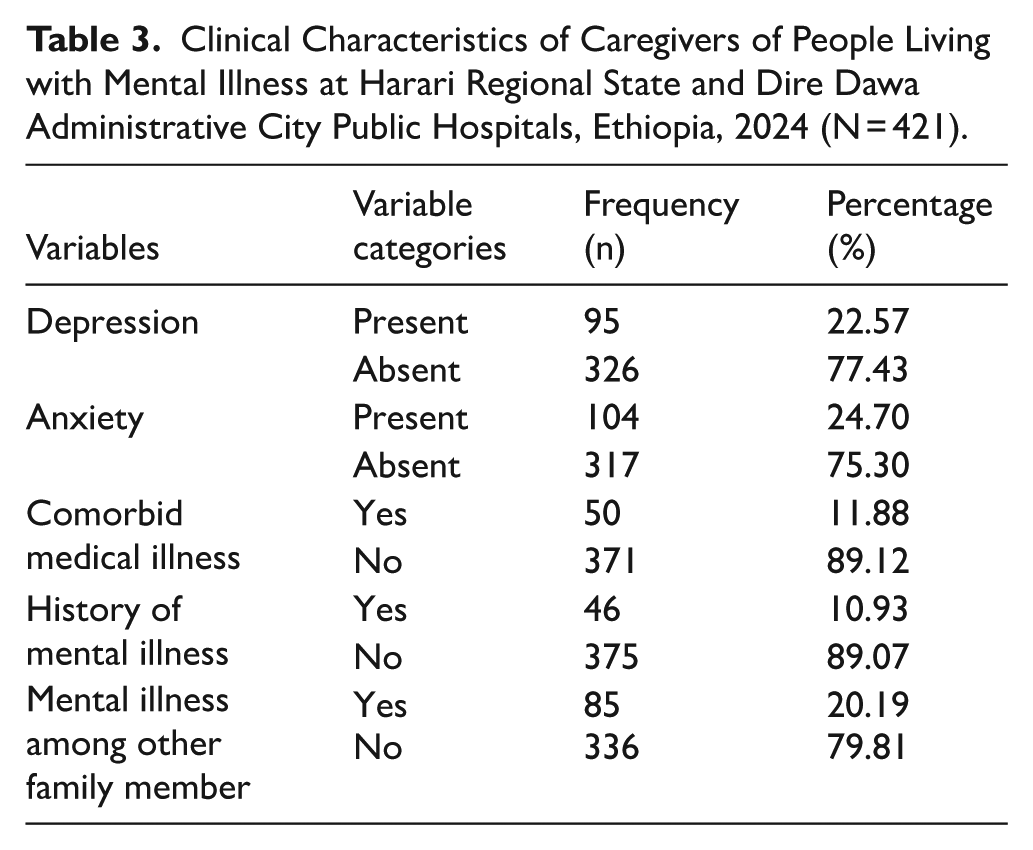
Among the 421 caregivers of PLWMI, 95 (22.57%) were found to have depression and nearly one fourth (24.70%) experienced anxiety, indicating a notable burden of mental health issues within this group (Table 3).
Clinical Characteristics of Caregivers of People Living with Mental Illness at Harari Regional State and Dire Dawa Administrative City Public Hospitals, Ethiopia, 2024 (N = 421).
Clinical Characteristics of People Living with Mental Illness
Psychosis was diagnosed in 154 patients (36.58%). Regarding the severity of their current illness, 229 patients (54.39%) were classified as mildly ill (Table 4).
Clinical Characteristics of People Living with Mental Illness at Harari Regional State and Dire Dawa Administrative City Public Hospitals, Ethiopia, 2024 (N = 421).

Anxiety disorders, minor psychiatry disorders, post traumatic stress disorder.
Psychosocial Characteristics of Caregivers of People Living with Mental Illness
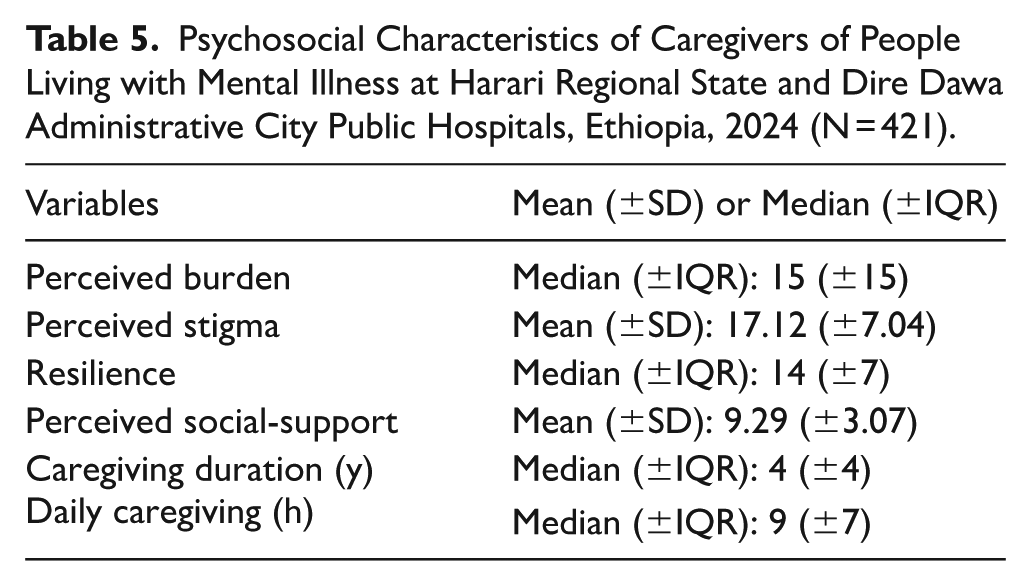
The report of caregivers of people living with mental illness showed that a median score of perceived burden was (median: 15 ± 15) and resilience was (median: 14 ± 7), alongside a perceived social support mean score was (mean: 9.29 ± 3.07). They also experienced notable perceived stigma (mean: 17.12 ± 7.04). The median caregiving duration was 4 years, with a daily caregiving commitment of approximately 9 hours, highlighting the substantial and sustained demands placed on these caregivers (Table 5).
Psychosocial Characteristics of Caregivers of People Living with Mental Illness at Harari Regional State and Dire Dawa Administrative City Public Hospitals, Ethiopia, 2024 (N = 421).
Distribution of Mean Score of QOL with Socio-Demographic Characteristics of Caregivers of Patients Living with Mental Illness
Caregivers who were younger, male, government employment, Higher educational attainment, and residing in urban areas reported higher QOL scores across physical, psychological, social, and environmental domains. Single individuals also showed better QOL compared to those who were married, divorced, or widowed. In contrast, close family members particularly children and spouses of people living with mental illness reported lower QOL scores than more distant relatives or non-family caregivers. Additionally, those with lower education levels and informal jobs, such as farmers or housewives, experienced the poorest QOL across all measured domains (Supplementary File 1).
Distribution of Mean Score of QOL with Socio-Demographic Characteristics of Patients Living with Mental Illness
This study found that mean score of QOL was higher scores across all domains among patients who were younger age (18-37 years), female, single, and primary education. Single patient showed the highest QOL scores, particularly in the social and environmental domains, while widowed patients had the lowest score across all domains. Similarly, participants with no formal education had lower QOL scores compared to those with primary or secondary education (Supplementary File 2).
Substance Use Characteristics of the Study Participants
Among the 421 caregivers of PLWMI, 62.47% had used Tobacco, Khat, or Alcohol in their lifetime, and 53.44% had used these substances in the past 3 months (Figure 3).

The frequency distribution of current substance use among caregivers of peoples living with mental illness at Harari Region and Dire Dawa City Administration Public Hospitals, Eastern Ethiopia, 2024 (n = 225).
Mean Score of Quality of Life in Each Domain of the WHOQOL-BREF Among Primary Caregivers of PLWML
The overall mean WHOQOL-BREF score among caregivers was 82.93 (±17.48), indicating a moderate quality of life. Among the domains, the physical (58.05 ± 18.81) and psychological (57.29 ± 16.28) domains had relatively higher mean scores. The social domain had the lowest mean score at (51.19 ± 23.12), suggesting caregivers experienced the most challenges in social relationships. Environmental quality of life was also modest, with a mean score of 53.04 ± 16.13 (Table 6).
Mean Distribution of the QOL of Primary Caregivers of PLWML at Harari Regional State and Dire Dawa Administrative City Public Hospitals, Ethiopia, 2024 (N = 421).

Abbreviations: SD, standard deviation; SE, standard error.
Self-Rated Quality of Life and Self-Reported Health Satisfaction of Caregivers of PLWML
On the basis of their perceived QOL, 162 (38.57%) of the study participants reported that their perceived QOL was neither poor nor good, followed by 107 (25.42%) who reported being poor. Regarding study participants self-perceived health satisfaction, 145 (34.44%) reported that they were neither dissatisfied nor satisfied, whereas 109 (25.89%) participants were dissatisfied (Table 7).
Self Rated Quality of Life and Self-Reported Health Satisfaction of Caregivers of People Living with Mental Illness at Harari Regional State and Dire Dawa Administrative City Public Hospitals, Ethiopia, 2024 (N = 421).

Factors Associated with the Physical, Psychological, Social, and Environmental Domains of Quality of Life Among Primary Caregivers of PLWML
Before running multiple linear regression analysis each independent factor was fitted for simple linear regression for the four domains of QOL to determine factors candidate for multiple linear regression analysis. According factors significantly associate at simple linear regression with P-value < .25 passed to multiple linear regression analysis. Variables fitted for multiple linear regression analysis explain 75.65 % of the variance in the physical domain, 58.8 % of the variance in the psychological domain, 69.64 % of the variance in the social domain, and 72.41% of the variance in the environmental domain of QOL of caregiver of PLWMI, respectively (Table 5).
Factors Associated with the Physical Domain
Adjusting for the effects of other variables, the score of the physical domain of QOL was 8.2 (β = −8.2 95% CI: (−11.83, −4.47) and 5.31 (β = −6.15, 95% CI: (−8.75, −1.86) point lower among caregivers who were unable to read and write and who were attending primary school as compared to those who were attended college and above, respectively.
Adjusting for the effects of other variables, the physical domain QOL score was 4.57 (β = 4.57, 95% CI: (−7.48, −1.66) point lower among caregivers who had probable cases of depression as compared to their counterparts.
A one unit increase in the stigma score, the physical domain QOL of caregivers decreased by a unit of −0.80 (β = −0.83, 95% CI: (−0.99, −0.62), adjusting for the effects of other variables.
A one-unit increase in the burden score, the physical domain QOL of caregivers decreased by a unit of 0.59 (β = −0.59, 95% CI: (−0.72, −0.45) adjusting for the effects of other variables.
A one unit increase in the Oslo social support score, the physical domain QOL of caregivers increased by a unit of 0.95 (β = 0.95, 95% CI: (0.57, 1.33), adjusting for the effects of other variables.
A one unit increase in the resilience score, the physical domain QOL of caregivers increased by a unit of 0.31 (β = 0.31, 95% CI: (0.03, 0.59) adjusting for the effects of other variables.
Keeping the effects of other variables constant, the physical domain QOL of caregiver who give care for patient living with other types of mental illnesses was 4.63 (β = 4.63, 95% CI: (1.43, 7.83) points higher as compared to caregiver who give care for patient living with psychosis (Table 8).
Linear Regression Analyses of Factors Associated with the Physical Domains of Quality of Life Among Primary Caregivers of People Living with Mental Illness at Harari Regional State and Dire Dawa Administrative City Public Hospitals, Ethiopia, 2024 (N = 421).

Abbreviations: MLR, multiple linear regression; Ref, reference group; SLR, simple linear regression.
Daily laborer, unemployed, retired.
Aunt, uncle, grandmother/father.
Anxiety disorders, minor psychiatry disorders, post traumatic stress disorder.
Significant at *P < .05, **P < .01, and ***P < .001.
Factors Associated with the Psychological Domain
Adjusting for the effects of other variables, the score of the psychological domain of QOL was 4.22 (β = −4.22, 95% CI: (−7.71, −0.74) points lower among caregivers who were unable to read and write as compared to those who were attending college and above.
Adjusting for the effects of other variables constant the score of the psychological domain QOL was 3.04 (β = −3.04, 95% CI: (−5.79, −0.29) points lower among caregiver who had probable case of depression as compared to their counterpart.
A one unit increase in the stigma score, the psychological domain QOL of caregiver decreased by a unit of −0.51 (β = −0.51, 95% CI: (−0.68, −0.33), adjusting for the effects of other variables.
A one unit increase in the burden score, the psychological domain QOL of caregiver decreased by a unit of −0.24 (β = −0.24, 95% CI: (−0.36, −0.11), adjusting for the effect of other variables.
A one unit increase in the Oslo social support score, the psychological domain QOL of caregiver increased by a unit of 0.85 (β = 0.85, 95% CI: 0.49, 1.21), adjusting for the effect of other variables.
A one unit increase in the resilience score, the psychological domain quality life of caregiver increased by a unit of 0.38 (β = 0.35, 95% CI: (0.12, 0.65), adjusting for the effects of other variables.
The psychological domain QOL of the study participant who care for patients living with other type of mental illnesses was 5.9 (β = 5.9, 95% CI: (2.95, 8.94) points higher as compared to caregivers who care for patients living with psychosis by keeping the effects of other variables constant (Table 9).
Linear Regression Analyses of Factors Associated with Psychological Domains of Quality of Life Among Primary Caregivers of People Living with Mental Illness at Harari Regional State and Dire Dawa Administrative City Public Hospitals, Ethiopia, 2024 (N = 421).

Abbreviations: MLR, multiple linear regression; Ref, reference group; SLR, simple linear regression.
Daily laborer, unemployed, retired.
Aunt, uncle, grandmother/father.
Anxiety disorders, minor psychiatry disorders, post traumatic stress disorder.
Significant at *P < .05, **P < .01, and ***P < .001.
Factors Associated with the Social Domain
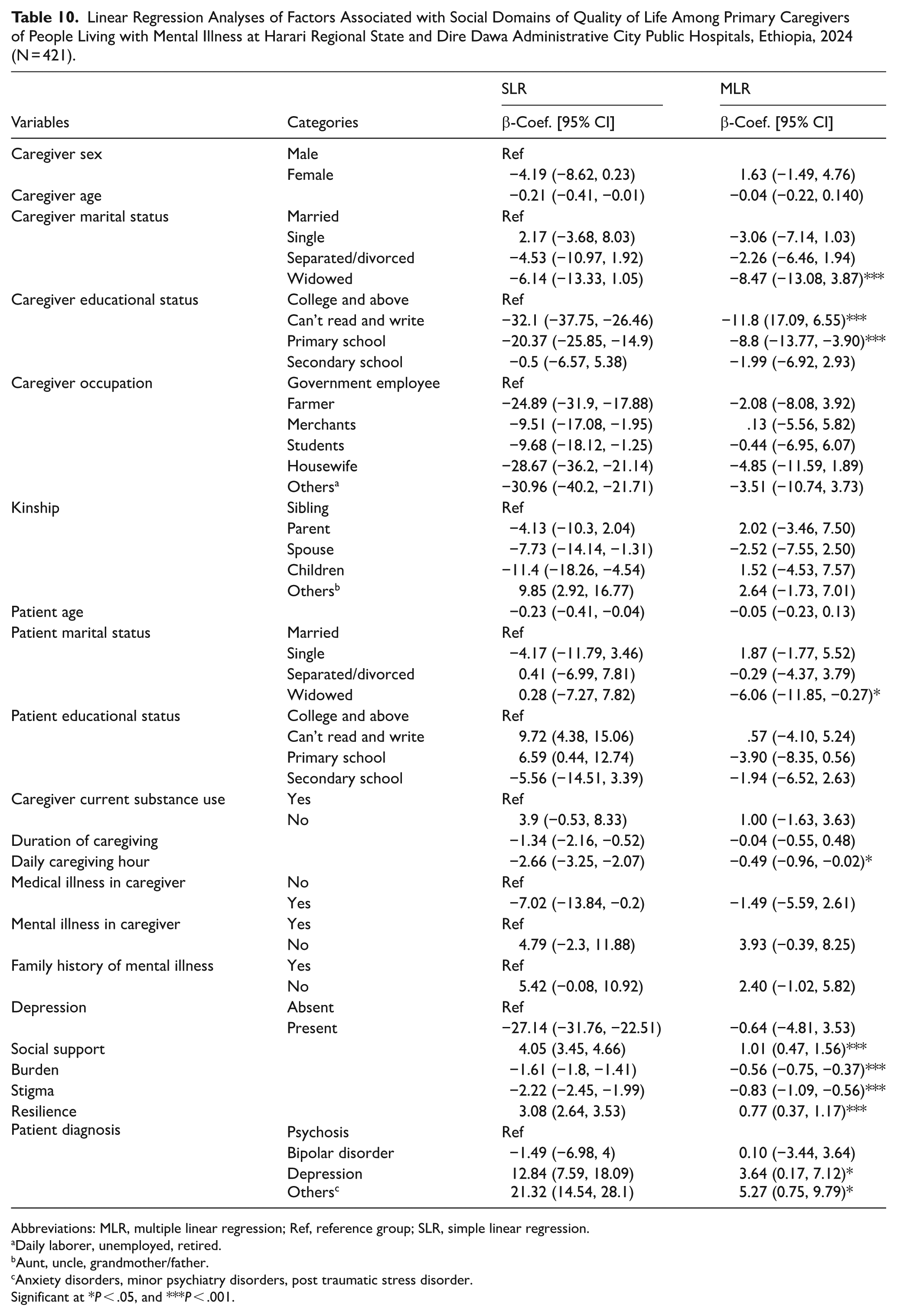
The score of, social domain of QOL was 8.47 (β = −8.54, 95% CI: (−13.08, 3.87) points lower among widowed caregiver than among those who were married, keeping the effects of other variables constant.
Adjusting for the effects of other variables, the scores of the social domain of QOL were 11.8 (β = −11.8, 95% CI: (17.09, 6.55) and 8.8 (β = −8.8, 95% CI: (−13.77, −3.90) points lower among caregiver who were unable to read and write and who were attending primary school as compared to those who were attending college and above, respectively.
The score of the social domain of QOL was 6.06 (β = −6.06, 95% CI: (−11.85, −0.27) points lower among caregiver of widowed patient as compared to caregiver of married patient, keeping the effects of other variables constant.
A one hour increase in the daily care-giving hour, the social domain QOL of caregivers decreased by a unit of 0.49 (β = −0.49, 95% CI: (−0.96, −0.02), adjusting for the effects of other variables.
A one unit increase in the stigma score, the social domain QOL of caregivers decreased by a unit of 0.83 (β = −0.83, 95% CI: (−1.09, −0.56), adjusting for the effects of other variables.
A one unit increase in the burden score, the social domain QOL of caregivers decreased by a unit of 0.56 (β = −0.56, 95% CI: (−0.75, −0.37), adjusting for the effects of other variables.
A one unit increase in the Oslo social support score, the social domain QOL of caregivers increased by a unit of 1.01 (β = 1.01, 95% CI: (0.47, 1.56), adjusting for the effects of other variables.
A one unit increase in the resilience score, the social domain QOL of caregivers increased by a unit of 0.77 (β = 0.77, 95% CI: (0.37, 1.17), adjusting for the effects of other variables.
The social domain QOL of the study participant who give care for patient living with other type of mental illnesses and depression was 5.27 (β = 5.27, 95% CI: (0.75, 9.79) and 3.64 (β = 3.64, 95% CI: (0.17, 7.12) points higher as compared to caregivers who care for patient living with psychosis by keeping the effects of other variables constant, respectively (Table 10).
Linear Regression Analyses of Factors Associated with Social Domains of Quality of Life Among Primary Caregivers of People Living with Mental Illness at Harari Regional State and Dire Dawa Administrative City Public Hospitals, Ethiopia, 2024 (N = 421).
Abbreviations: MLR, multiple linear regression; Ref, reference group; SLR, simple linear regression.
Daily laborer, unemployed, retired.
Aunt, uncle, grandmother/father.
Anxiety disorders, minor psychiatry disorders, post traumatic stress disorder.
Significant at *P < .05, and ***P < .001.
Factors Associated with the Environmental Domain
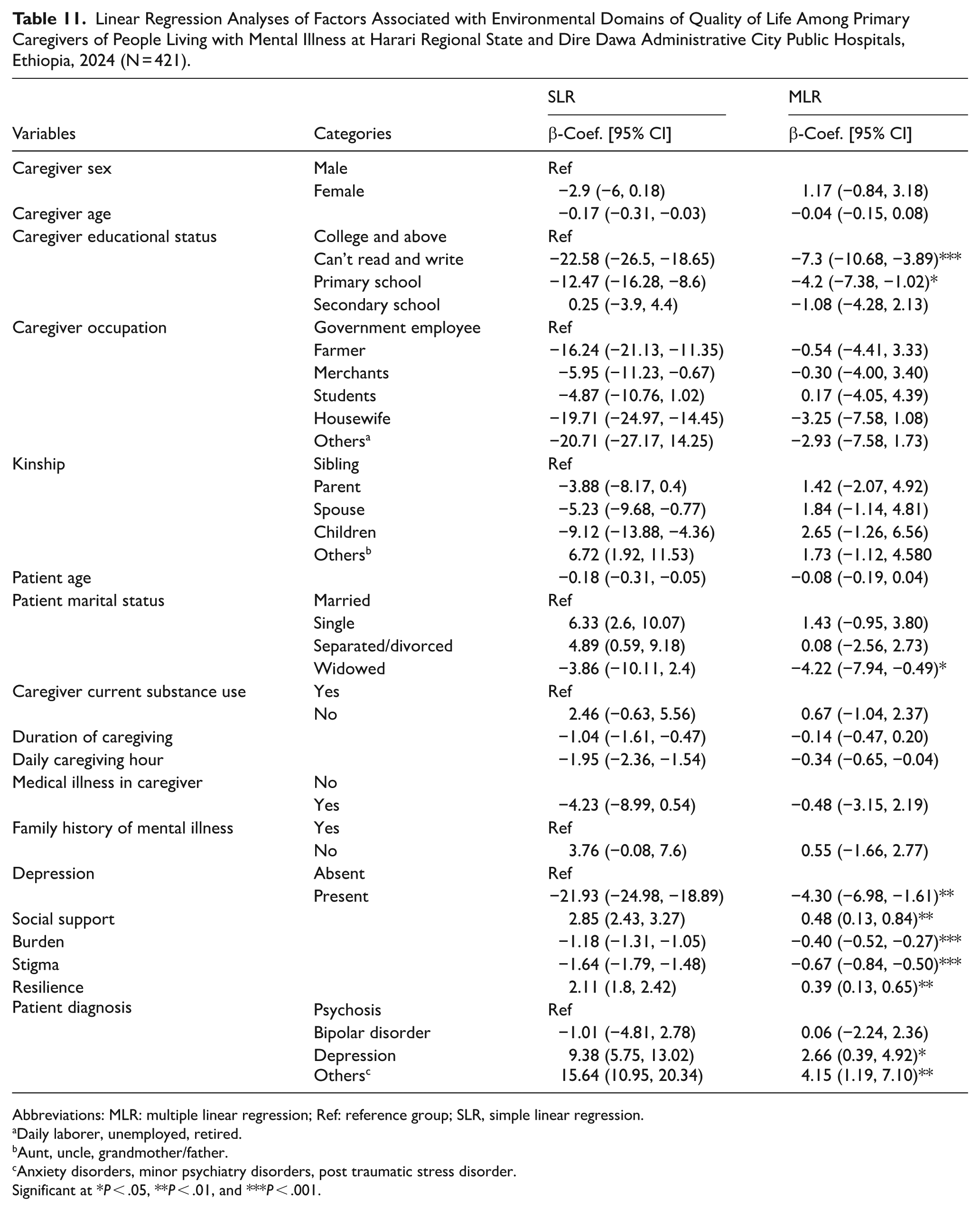
Adjusting for the effects of other variables, the scores of environmental domain QOL was 7.3 (β = −7.3, 95% CI: (−10.68, −3.89) and 4.2 (β = −4.2, 95% CI: (−7.38, −1.02) points lower among caregivers who were unable to read and write and who attended primary school as compared to those who were attended college and above, respectively.
The score of the environmental domain of QOL was 4.42 (β = −4.42, 95% CI: (−7.94, −0.49) points lower among caregivers of widowed patients as compared to caregivers of married patients, keeping the effects of other variables constant.
Adjusting for the effects of other variables constant, the score of the environmental domain QOL was 4.30 (β = −4.30, 95% CI: (−6.98, −1.61) points lower among caregivers who had probable case of depression as compared to their counterparts.
A one unit increase in the stigma score, the social domain QOL of caregivers decreased by a unit of 0.69 (β = −0.69, 95% CI: (−0.84, −0.50), adjusting for the effects of other variables.
A one unit increase in the burden score, the social domain QOL of caregivers decreased by a unit of 0.40 (β = −0.40, 95% CI: (−0.52, −0.27) adjusting for the effects of other variables.
A one unit increase in the Oslo social support score, the social domain QOL of caregivers was increased by a unit of 0.48 (β = 0.48, 95% CI: (0.13, 0.84) adjusting for the effects of other variables.
A one unit increase in the resilience score, the social domain QOL of caregivers was increased by a unit of 0.39 (β = 0.39, 95% CI: (0.13, 0.65), adjusting for the effects of other variables.
The environmental domain of QOL of the study participants who give care for patients living with other type of mental illnesses and depression was 4.15 (β = 4.15, 95% CI: (1.19, 7.10), and 2.66 (β = 2.66, 95% CI: (0.39, 4.92) points higher as compared to caregivers who care for patients living with psychosis by keeping the effects of other variables constant (Table 11).
Linear Regression Analyses of Factors Associated with Environmental Domains of Quality of Life Among Primary Caregivers of People Living with Mental Illness at Harari Regional State and Dire Dawa Administrative City Public Hospitals, Ethiopia, 2024 (N = 421).
Abbreviations: MLR: multiple linear regression; Ref: reference group; SLR, simple linear regression.
Daily laborer, unemployed, retired.
Aunt, uncle, grandmother/father.
Anxiety disorders, minor psychiatry disorders, post traumatic stress disorder.
Significant at *P < .05, **P < .01, and ***P < .001.
Discussion
This study found that, caregivers of PLWMI had highest and lowest score on the physical and social domain of WHOQOL-BREF, respectively. The highest score of physical domains implied that our study participants had good activities of daily living, adequate energy and mobility, less pain and discomfort, sufficient sleep and rest, and good work capacity. While the lowest score of social domains implied that our study participants had poor personal relationship, sex life, and social support. This finding is in line with studies conducted in Malaysia, Australia, India, Spain, Hong Kong, India, and Spain.9,28,31,52,69,70
The result of this study was lower than study conducted in South Africa, Malaysian, China, and Brazil in all dimension of QOL.33,37 This discrepancy might be attributed to difference in methodological variation in which the former studies included caregivers above 20 years old, and who live with the patient, 28 sampling size differences, differences in the study participants profile in which the previous research only include caregivers of schizophrenia, 31 caregivers of OCD, 71 and only married women as study participant. 37
The result of this study was higher than study conducted in Uganda in all dimension of QOL, 32 and another study in Ethiopian regarding to psychological, social and environmental domains, 35 in China and Spain in aspect of physical, psychological and environmental domain.28,31 This difference might be due to the variations in socio-demographic factors of study participant, inclusion criteria in which the former studies included caregivers at inpatient services. But the current study includes PLWMI at outpatient department. Additionally, the cultural and economic variations in study population, sample size (ie, larger sample size of the current study) might be accounted for the observed differences.
The result from this study indicates that there was significant negative relationships between social domain of QOL and marital status of caregivers being widowed. This finding was supported by studies conducted in Kenya, South Africa, and India.14,50,51 The possible explanation for the lower QOL among caregivers who were widowed might be that divorce cause lack of emotional support from loved one, lead to feelings of burnout and decreased mental health. 72
The result from this study indicates that there was significant negative association between social and environmental domain of QOL and marital status of patient being widowed. This finding was supported by studies conducted in Kenya and Ethiopia.36,51 The possible reason might be widowed patients may require more intensive care and attention, leading to higher levels of caregiver burden as well divorce can also lead to financial strain for the caregiver. 16
This study revealed that there was significant negative association between the four domains of QOL and lower educational level of caregivers. This finding was supported by studies conducted in China, Jordan, Indonesia, and Ethiopia.35,36,46,47,52,53 The possible reason for the lower QOL among caregivers with lower educational level might be lower education level among caregivers is often related to lower socioeconomic status, educational attainment may influence the acquisition of knowledge about appropriate health practices, and lower education might impair access to health education, adoption of healthy behavior.36,72
This study revealed that there was significant negative relationship between caregivers having depression and the physical, psychological, and environmental domain of QOL. This result is supported with the studies conducted in Ethiopia, South Korea, Sweden, and Ghana.34,36,48,73 This might be due to depression causes a person to lose interest in everyday activities and exhibit vegetative symptoms, which significantly affects functioning in general. Additionally, depression raises the risk of physical illness since it weakens the body’s defenses against illness.74,75
The finding of this study revealed that social support was positively significantly associated with all domain of QOL. This finding was supported by studies conducted in Ethiopia, Indonesia, and China.13,35,36,54 The most likely reason could be that higher perceived social support is generally linked to better interpersonal functioning, less burden, a stronger sense of usefulness, and a more valued sense of self.54,76 Providing and exploring possible ways to strengthen social interaction and social support for caregivers with different strategies, like the creation of respite involving community volunteers and caregiver support groups, can create a sense of accomplishment among caregivers which might improve their social QOL. Leveraging existing community resources, such as religious organizations or local NGOs, can help provide support without significant financial investment. These entities can offer emotional support, and or even practical assistance.
This study revealed that perceived stigma was inversely significantly associated with four domains of QOL. This finding was supported by studies conducted in Ethiopia, Singapore, Jordan.7,35,36,46 The possible reason for the lower QOL among caregivers with high perceived stigma might be attributed to that stigma leads to emotional disturbances and psychological distress, a feeling of shame, embarrassment, and guilt which affect both the physical and mental health of caregivers.36,77 Furthermore, caregivers may hesitate to seek help or support due to fear of judgment or discrimination, leading to delays in getting the assistance they need to cope with the challenges of caregiving. 78 Launching public health campaigns to decrease stigma related to mental illness, which often extends to caregivers, leading to social isolation and reluctance to seek help, can increase the awareness of mental illness and foster community understanding as well as acceptance. This might help the overall well-being of caregivers and care provided for the patient.
The current study revealed increased QOL of among caregivers of people live with other types of mental disorder as compared to caregivers of schizophrenia. This finding was supported by studies conducted in India, Indonesia.50,54,79 The possible explanation might be due to the difference of illness process in which affective disorder are by far more episodic at which the patient return to baseline functioning in contrast to that of psychosis. 80 Caregivers illness perception most caregivers perceive caring for patient with psychosis as a stressful event as well as psychotic patients have a long disease duration, progressive exacerbation which makes their caregivers bear an unusually heavy burden of care and physical impairments occurred from long-term uninterrupted care process, which has a significant negative impact on their QOL. 81
This research revealed that resilience was significantly positively associated along the psychological, social, and environmental domains of caregiver’s QOL. This result is supported by study conducted in China, Japan, and Netherlands.49,82,83 The possible explanation for this might be resilience positively influences caregivers’ QoL during caregiving, offering emotional stability, effective resource utilization, and reducing psychological distress. Also, resilient caregivers higher might have a sense of accomplishment, companionship, fulfillment, enjoyment, and improved self-esteem which could mediate the path between coping mechanism and high QOL of caregivers. 84 Enhancing caregivers’ resilience using psychoeducation and skill training on problem-solving, providing counseling, coping mechanisms, and stress management crucially reduces caregivers’ uncertainty and improves their sense of competence, which might result in better patient outcomes as well as caregiver strain management. This may include training sessions or workshops that teach coping strategies, stress management techniques, and problem-solving skills. Such programs can be cost-effective and leverage community resources.
The result of this study revealed that there was inversely significant association between caregiving burden and all domains of caregiver’s QOL. The result of the current study was consistent with study conducted in China, and Indonesia.47,54 The possible reason might be burden result in overwhelmed emotion, stress, and devastating impact of illness on caregivers. The demanding tasks of care giving can lead to physical exhaustion and psychological distress, which are primarily manifested as anxiety and depression.84,85 Routinely screening caregivers for signs of burden as an integral part of the patient health care plan might lead to better care for patients receiving care, reduce health costs, reduce caregiver burnout result in enhanced caregiver QOL.
The current study revealed that daily average care giving hours was inversely significantly associated with the social domain of caregiver’s QOL. This result was consistent with studies conducted in India, and Hong Kong.50,52 The possible explanation for this might be longer caregiving years and longer daily caregiving hours can increase caregiving burden.79,86
Generally, to support caregivers effectively a multifaceted approach is needed. Programs aimed at enhancing resilience through coping strategies, stress management, and problem-solving skills can be implemented using community resources. Addressing caregiver burden is crucial and can involve support groups and respite care services. Strengthening social support networks by connecting caregivers through community organizations and involving volunteers can provide essential emotional and practical help. Policy advocacy is also key in raising awareness and lobbying for funding. Caregiver focused policies can improve their well-being. Utilizing existing resources like religious groups and Non-governmental organizations can offer cost-effective support, while public education campaigns can foster broader understanding of caregivers’ challenges and promote community-wide involvement in supporting them.
Limitations of the Study
Due to its cross-sectional design, this study cannot establish a temporal relationship between the outcome and independent variables. Therefore, future research should consider using a longitudinal design to address this limitation. Comorbid medical conditions in patients were extracted from medical records, while those of caregivers were self-reported, which may have led to under- or overestimation. Additionally, important factors potentially affecting caregiver QOL such as caregiver income, household size, and patient functionality were not included in the current study and warrant further investigation. Due to study constraints, the focus was placed on the caregiver’s individual educational attainment. Nonetheless, exploring the influence of family educational background remains a valuable area for future research. Moreover, the study may be affected by social desirability and recall bias due to the sensitive nature of topics and reliance on self-reported tools. Additionally, some instruments (eg, BRCS, ZBI-12) were not culturally validated for Ethiopia. It is better for future research to consider validated version for these variables.
Conclusions
Caregivers’ QOL found to be low across the four domains of QOL, with the lowest score in the social domain. Caregivers of PLWMI face various challenges that impact their QOL. The key factors associated with QOL include lower educational attainment, patient diagnosis, social support, perceived stigma, caregiver depression, and perceived burden in all domains of caregiver QOL. Resilience and social support found to plays a positive role in of caregiver QOL. It could be essential to implement programs that address the needs of caregivers struggle with caregiving stigma, emotional strain and burden. Providing brief psychoeducation session as well as social integration programs have significant role in improving QOL of caregivers. Providing regular evaluation and screening plans for risky caregivers through integration of mental health into primary health care system, establishment of rehabilitation center for aftercare systems for patients with long-term mental illness and expansion of community-based support services (respite care, support groups, home healthcare) might help for early intervention of caregivers at risk for low QOL. Longitudinal studies should be conducted to reveal the causality between caregiver QOL and associated factors.
Supplemental Material
sj-docx-1-his-10.1177_11786329251374243 – Supplemental material for Quality of Life and Associated Factors Among Primary Caregivers of People Living with Mental Illness in Ethiopia: A Cross-Sectional Study
Supplemental material, sj-docx-1-his-10.1177_11786329251374243 for Quality of Life and Associated Factors Among Primary Caregivers of People Living with Mental Illness in Ethiopia: A Cross-Sectional Study by Abinet Zewudie, Gari Hunduma, Mandaras Tariku, Dawud Wedaje, Hamdi Fekredin Zakaria, Abdi Temesgen, Dawit Abdi, Hirko Assefa and Rudwan Yasin in Health Services Insights
Footnotes
Acknowledgements
The authors would like to acknowledge Haramaya University College of Health and Medical Sciences Department of Psychiatry for providing ethical clearance. The authors would also like to thank; HU-HFCSUH, JGH, DCRH, and SGH psychiatry department staff; and the study participants for providing general information about the study population and the services they provided. Finally, we would also like to thank all parents who participated in this study and their commitment to respond to our questions.
Abbreviations
BRCS: Brief Resilient Coping Scale
CGI: Clinical Global Impression
DCRH: Dil Chora Referral Hopspital
HU-HFCSUH: Haramaya University Hiwot Fana Comprehensive Specialized University Hospital
GAD-7: Generalized Anxiety Disorder-7
IHRERC: Institutional Health Research Ethics Review Committee
FIS: Family Interview Schedule
HMIS: Health Management Information System
JGH: Jogula General Hospital
LMICs: Low- and Medium-Income Country
OSSS: Oslo Social Support Scale
PHQ-9: Patient Health Questionnaire-9
PLWMI: People Live With Mental Illness
QOL: Quality Of Life
SGH: Sabean General Hospital
WHO: World Health Organization
WHOQOL-BREF: World Health Organization Quality of Life-Bref
Author Contributions
Abinet Zewudie: Conceptualization, data curation, formal analysis, methodology, writing – original draft, writing – review and editing. Gari Hunduma: Conceptualization, data curation, formal analysis, methodology, writing – original draft, writing – review and editing. Mandaras Tariku: Conceptualization, data curation, formal analysis, methodology, writing – original draft, writing – review and editing. Dawud Wedaje: Conceptualization, data curation, formal analysis, methodology, writing – original draft, writing – review and editing. Hamdi Fekredin Zakaria: Conceptualization, data curation, formal analysis, methodology, writing – original draft, writing – review and editing. Abdi Temesgen: Conceptualization, data curation, formal analysis, methodology, writing – original draft, writing – review and editing. Dawit Abdi: Conceptualization, data curation, formal analysis, methodology, writing – original draft, writing – review and editing. Hirko Assefa: Conceptualization, data curation, formal analysis, methodology, writing – original draft, writing – review and editing. Rudwan Yasin: Conceptualization, data curation, formal analysis, methodology, writing – original draft, writing – review and editing.
ORCID iDs
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All the data included in the manuscript can’t publicly available to protect the anonymity of the participants. However, upon reasonable request, materials may be obtained from the corresponding author: Abinet Zewudie upon request through the email address of
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.