
Abstract
Introduction:
Cervical cancer is a major public health problem, particularly in low- and middle-income countries. Persistent human papillomavirus (HPV) infection is the primary cause of cervical cancer and constitutes an increased risk for women living with HIV (WLHIV). The aim of this study was to identify factors associated with cervical cancer screening among women with HIV followed at Bonassama District Hospital, Cameroon, in order to improve the coverage and quality of prevention programs.
Methodology:
The study was conducted in the Bonassama health district over a period of 9 months from November 2023 to July 2024 with a collection period of 4 months. A quantitative, cross-sectional, and analytical approach was adopted, targeting 283 women living with HIV aged 21 and over. Data were collected using a structured questionnaire. Data analysis was performed using R software version 4.4.2 and included both descriptive and multivariate analyses to identify factors associated with screening.
Results:
Screening uptake was low, with 18.7% of participants reporting previous cervical cancer screening. The screening was significantly associated with being divorced (AOR = 8.82, p = 0.024), having received a screening prescription at the HIV Management Unit (AOR = 6.79, p < 0.001), having consulted a gynecologist for another reason (AOR = 2.79, p = 0.015), knowing the symptoms of cancer (AOR = 2.86, p = 0.009) and having received advice from a healthcare professional (AOR = 14.70, p < 0.001).
Conclusion:
This study highlights the low coverage of cervical cancer screening among women living with HIV in Cameroon. The results highlight the importance of information and support from healthcare professionals to encourage screening. It is crucial to integrate cervical cancer screening into HIV follow-up programs and to improve access to healthcare services for this vulnerable population.
Introduction
Cervical cancer is a major public health problem, particularly in low- and middle-income countries 1 In 99% of cases, it is caused by persistent infection with the human papillomavirus (HPV), a widespread sexually transmitted infection. Other risk factors, such as smoking and human immunodeficiency virus (HIV) infection, can weaken the immune system and increase the persistence of HPV. 2 A weakened immune system not only increases the risk of acquiring new infections but also increases the likelihood that an HPV infection will progress to persistent precancerous lesions. 3 Women living with HIV (WHIV) are therefore particularly at risk of cervical cancer, as precancerous lesions, in the absence of regular screening and early treatment, may progress more rapidly to invasive cancer. 4
Worldwide, more than 600,000 new cases of cervical cancer are diagnosed each year, and around 340,000 deaths are recorded, mainly in developing countries where access to preventive services is limited. 1 This makes cervical cancer the fourth leading cause of cancer in women worldwide, after breast, lung, and colon cancer. 3 In 2022, 662,301 new cases were reported worldwide, representing 69% of cancer cases, resulting in 348,874 deaths, representing 8.1% of all cancer-related deaths in women. 5 The highest incidence and mortality rates are observed in sub-Saharan Africa, Central America, and South-East Asia. 1
In Africa, cervical cancer is the second most common cancer in women after breast cancer, with an estimated incidence of 125,699 cases, representing approximately 10.6% of global cervical cancer cases, with 80,614 deaths attributable to this cancer. 5 Sub-Saharan Africa has the highest incidence and mortality rates, due to limited access to screening, low levels of awareness, and structural weaknesses in healthcare systems. 6 Cameroon is not an exception, with an estimated incidence of 2525 new cases in 2022 and nearly 1837 deaths. 5 In Douala, the situation is particularly worrying in peri-urban areas, where health services are often overcrowded and inaccessible. HIV infection is also a well-documented aggravating factor: HIV-positive individuals are at increased risk of HPV persistence and progression to cervical cancer. 7 This makes screening in this population a priority.
Despite efforts by the Cameroonian government and its technical partners to integrate cervical cancer screening into HIV care services, particularly through one-off campaigns and screening using acetic acid visualization (VIA), 4 coverage remains very low. A study carried out in Yaoundé in 2017 revealed that only 12.8% of women had ever been screened for cervical cancer 8 ; while in 2021, only 5.0% of women aged between 30 and 49 in Cameroon had been screened in the last 5 years. 9 At Bonassama District Hospital, a referral center for monitoring people living with HIV in the Douala IV subdivision, internal data also show low uptake of screening, despite the availability of services. This situation raises questions about the behavioral, organizational, and socio-cultural determinants that influence the uptake of screening by people living with HIV.
The socio-economic and cultural context of the city of Douala, marked by inequalities in access to healthcare, cultural beliefs that are sometimes incompatible with biomedical recommendations, and high levels of economic insecurity, is a major obstacle to the effective implementation of prevention strategies. 10 Added to this is the stigma attached to HIV, the fear of being diagnosed with cancer, and a lack of awareness of the benefits of early screening. 11 In addition, some women may perceive the services offered as unsuited to their needs, or face logistical barriers (cost, distance, waiting times). These factors combine to make it necessary to gain a detailed understanding of the determinants associated with screening uptake.
The main objective of this study is therefore to identify the factors associated with cervical cancer screening among women living with HIV attending Bonassama district hospital. The aim of this research is to gain a better understanding of the levers and obstacles to participation in screening in an urban context with limited resources. The results obtained could be used to strengthen prevention programs integrated with HIV care, in order to improve the coverage and quality of preventive care for this vulnerable population.
Methodology
Setting and study period
The study was conducted over a period of 9 months, from November 2023 to July 2024, at Bonassama District Hospital. Bonassama District Hospital is located in the Bonassama neighborhood, chief town of the 4e arrondissement of Douala, Wouri department, Littoral region - Cameroon. It covers an area of one and a half hectares. It is bounded to the north by the Douala IV town hall, to the south by the Wouri River, to the east by the sub-prefect’s residence, and to the west by the CAMITOYOTA company. The hospital has a number of departments, including general medicine, laboratory, blood bank, surgery, operating theater, imaging, pediatrics, and neonatology, as well as a high-standard ward and a gynecology department offering prenatal consultation and family planning. This health facility was chosen for this study because of its optimal accessibility to information and adequate infrastructure for screening and clinical follow-up. Collaboration with local medical staff provided valuable information on the obstacles encountered by patients, thus guaranteeing the feasibility of the study. 12
Study design and study population
The study was quantitative, cross-sectional, and analytical, targeting HIV-positive women attending Bonassama District Hospital. The study population consisted of women aged 21 and over, diagnosed HIV-positive within the last year, followed up at Bonassama District Hospital, and who had given informed consent to participate in the study. Exclusion criteria included women who had given consent at baseline and wished to withdraw from the study at some point. The non-inclusion criteria included HIV-uninfected women, HIV-positive women under 21 years of age, and women who refused to consent to the study.
Sample size and sampling procedure
The sample size was determined according to Lorentz’s formula: n = p (1−p) × z2α/2 ̸̸d2. Where p is the expected prevalence, p 23.3% from a study conducted in Ethiopia 13 ; the degree of precision (5%), zα/2 is the critical value on the reduced centered normal distribution for a risk of error α (for α = 5%, zα/2 = 1.96). After calculation, the minimum sample size was estimated at 276 women. Taking into account potential non-responses, the final number was set at 283 participants recruited using non-probability convenience sampling.
Data collection technique and tools
Data were collected by means of a hospital-based survey using a semi-structured questionnaire with three headings: socio-demographic characteristics, clinical and reproductive characteristics, and knowledge of cervical cancer and lifestyle. The questionnaire was pre-tested with 25 participants, after which the comprehension of the questions, clarity, and length of the interview were noted. Based on this pre-test, several adjustments were made: ambiguous questions were reworded, the order of sections was rearranged for better flow, and the number of open-ended questions was reduced. Most questions were closed with predefined modalities, while open-ended questions (e.g. occupation, type of STI, advice received) were further coded into standard categories.
Definition and operationalization of variables
The dependent variable in this study was cervical cancer screening, measured by a binary indicator: women living with HIV are classified into two categories according to whether or not they have been screened in the last 5 years.
Data collection procedure
After obtaining the necessary research authorizations, we requested a meeting with the head of the HIV department, who granted us permission to contact the patients. Once in contact with the patients, the investigator introduced himself and explained the reasons for his presence as well as the objectives and activities of the study through the information leaflet, and answered any questions the patients might have for a better understanding. When patients agreed to take part in the study, they were given the informed consent form to sign, after which a questionnaire was administered face-to-face, and those who refused were considered non-respondents. The anonymity and confidentiality of participants were ensured by assigning a unique code to each one.
Statistical analysis of the data
The data collected was analyzed using RStudio software version 4.4.2. Microsoft Office Excel 2016 was also used to prepare the tables. Descriptive statistics were calculated for all the variables considered. The analysis of this study took into account one dependent variable (cervical cancer screening) and several independent variables divided into three groups (socio-demographic characteristics, clinical and reproductive characteristics, and knowledge about cervical cancer and lifestyle). The association between the dependent and independent variables was determined using binary logistic regression, and all variables with a p value < 0.05 in the bivariate analysis were candidates for multivariate analysis. The various indicators were estimated with a significance level of α = 0.05, and the associations were considered significant for a p value < 0.05.
Results
At the end of the study, a total of 315 women were approached, 283 of whom agreed to take part, corresponding to a participation rate of 89.8%, while 32 (10.2%) refused, mainly due to fatigue or lack of time. Missing data represented less than 5% of the total data and were treated by deletion from the list during the analysis.
Socio-demographic and cultural characteristics of participants
Table 1 shows the socio-demographic characteristics of the study participants. The most common age group was between 41 and 60 years (56.54%), with an average age of 44.51 ± 11.50 years. In terms of marital status, the majority of participants were single (32.86%). In addition, 49.12% had between 1 and 3 children, and 96.11% were Christian. Furthermore, 46.64% had a secondary education, and most worked in the informal sector (79.51%), earning less than 50,000 francs a month (44.17%).
Socio-demographic characteristics of HIV positive women.

Proportion of HIV-positive women screened for cervical cancer
Figure 1 shows the distribution of participants according to their cervical cancer screening status. The results show that 18.37% of participants had been screened for cervical cancer.

Distribution of cervical cancer screening among women on antiretroviral treatment.
Relationship between socio-demographic characteristics and cervical cancer screening in women on antiretroviral treatment
Table 2 presents the results of bivariate analyses of socio-demographic determinants associated with cervical cancer screening in women on antiretroviral treatment. The data show that being divorced (OR = 5.20; 95% CI: 1.89–30.54; p = 0.046) significantly increased the probability of these women being screened for cervical cancer.
Relationship between sociodemographic characteristics and cervical cancer screening in women receiving antiretroviral treatment.

CI: confidence interval; OR: odds ratio; p-value: significance level.
p< 0.001; **p < 0.01; *p <0.05.
Relationship between factors related to sexual activity and cervical cancer screening in women on antiretroviral treatment
Table 3 presents the results of the bivariate analysis of sexual activity-related factors associated with cervical cancer screening in women on antiretroviral treatment. The data revealed that the absence of sexual activity (OR = 5.41; 95% CI: 1.56–25.34; p = 0.014), the absence of a sexual partner for some time (OR = 2.25; 95% CI: 1.10–4.53; p = 0.023), as well as non-use of oral contraceptives (OR = 6.71; 95% CI: 1.34–122.21; p = 0.046), significantly increased the probability of these women being screened for cervical cancer
Relationship between factors related to sexual activity and cervical cancer screening in women on antiretroviral treatment.

CI: confidence interval; OR: odds ratio; p-value: significance level.
p< 0.001; **p < 0.01; *p <0.05.
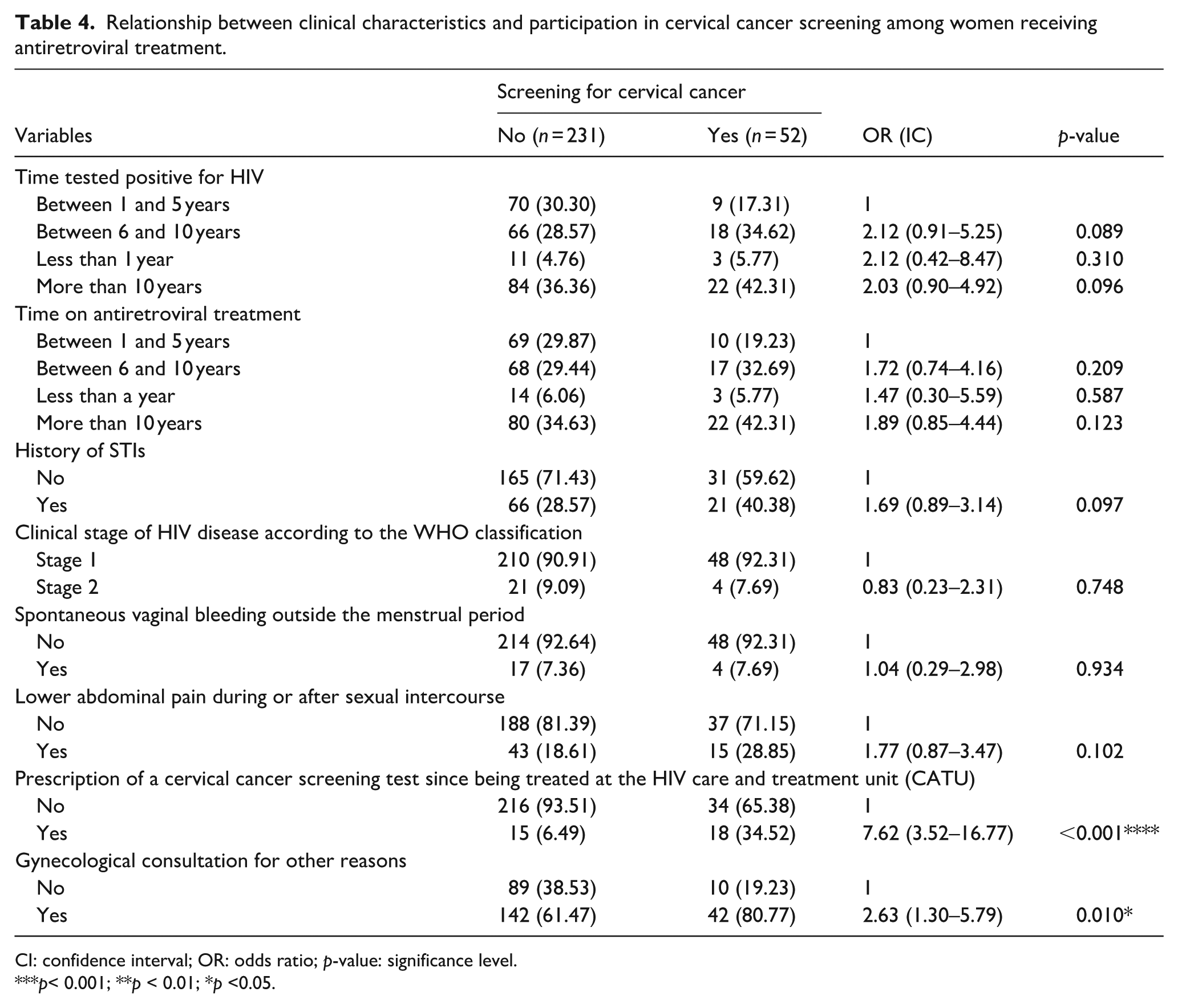
Relationship between clinical characteristics and participation in cervical cancer screening among women on antiretroviral treatment
Table 4 presents the results of the bivariate analysis of clinical characteristics associated with cervical cancer screening in women on antiretroviral treatment. The table shows that prescribing a cervical cancer screening examination since admission to the HIV unit (OR = 7.62; 95% CI: 3.52–16.77; p < 0.001), as well as having consulted a gynecologist for another reason (OR = 2.63; 95% CI: 1.30–5.79; p = 0.010), were significantly associated with cervical cancer screening in these women.
Relationship between clinical characteristics and participation in cervical cancer screening among women receiving antiretroviral treatment.
CI: confidence interval; OR: odds ratio; p-value: significance level.
p< 0.001; **p < 0.01; *p <0.05.
Relationship between participants’ knowledge of cervical cancer and participation in screening among women receiving antiretroviral treatment
Table 5 presents the results of the bivariate analysis of participants’ knowledge of cervical cancer associated with screening in women on antiretroviral therapy. The results show that knowing that abnormal vaginal bleeding or unusual vaginal discharge are symptoms of cervical cancer (OR = 3.26; 95% CI: 1.76–6.12; p < 0.001), knowing that regular use of tobacco, alcohol or electronic cigarettes can lead to cervical cancer (OR = 2.64; 95% CI: 1.42–5.10; p = 0.002), as well as having been screened early for this cancer, thereby increasing the chances of treatment (OR = 5.56; 95% CI: 2.55–13.98; p < 0.001), were significantly associated with cervical cancer screening in these women.
Relationship between participants’ knowledge of cervical cancer and participation in screening among women on antiretroviral treatment.

CI: confidence interval; OR: odds ratio; p-value: significance level.
p< 0.001; **p < 0.01; *p <0.05.
In addition, participants who had received advice on cervical cancer screening from a healthcare professional (OR = 22.74; 95% CI: 10.85–51.87; p < 0.001), those who were aware of treatment options such as surgery, radiotherapy or chemotherapy as a means of treating cervical cancer (OR = 3.43; 95% CI: 1.49–8.52; p < 0.005), as well as those who had known someone with cervical cancer (OR = 2.12; 95% CI: 1.05–4.14; p = 0.030) were significantly more likely to have been screened for cervical cancer.
Multivariate analysis of factors associated with cervical cancer screening in women on antiretroviral treatment
Table 6 presents the results of the multivariate analyses performed on the previously significant variables, in order to control for confounding factors and identify independent predictors of cervical cancer screening in women on antiretroviral treatment. The results showed that being divorced (AOR = 8.82; 95% CI: 1.27–62.80; p = 0.024), having been prescribed a cervical cancer screening test since being treated at
Multivariate analysis of factors associated with cervical cancer screening in women on antiretroviral treatment.

AOR: adjusted odds ratio; CI: confidence interval; p-value: significance level.
p< 0.001; **p < 0.01; *p <0.05.
Discussion
The aim of this study was to analyze the factors associated with cervical cancer screening in HIV-infected women attending Bonassama district hospital. The results showed that several factors are associated with cervical cancer screening in this district.
In the present study, cervical cancer screening (CC) among women on antiretroviral treatment was 18.37%. This is a relatively low rate, but higher than the 6.9% found by Kouakou et al. 14 in their Abidjan study of UCC screening in HIV-infected women and the 9% found by Belglaiaa et al. 15 in Morocco. However, other studies have found higher rates of UCC screening among women living with HIV. In this study, Daniel et al. 13 found that 23.5% of HIV-infected women attending a clinic in northwest Ethiopia had already been screened for CC. Similarly, Emru et al. 16 found a 25.5% screening rate for CC among these women in their study in Addis Ababa, Ethiopia. However, Tesfaye et al., 17 in their study in eastern Ethiopia, showed that 57.5% of women living with HIV were screened for CC. Moreover, this rate was 82.0% in Ghana. 19
The low rate of screening among women on antiretroviral treatment in our study can be explained by several factors. The integration of cervical cancer screening (CC) into HIV care programs is often inadequate, limiting opportunities for screening. In addition, patient awareness and education about the importance of screening remain low, leading to a lack of motivation to participate in these examinations. Socio-cultural barriers, such as HIV-related stigma and fear of diagnosis, also discourage women from undergoing screening. Practical barriers, such as the cost of tests, distance from health facilities, and lack of time due to family responsibilities, also contribute to the low uptake of screening. In addition, the differences observed between the various studies are thought to be due to differences in socio-cultural and economic characteristics, variations in methodology, limited accessibility to screening services, and a priority given to HIV management to the detriment of co-morbidities.
Multivariate analysis revealed that several factors were significantly associated with cervical cancer screening among women on antiretroviral treatment. Firstly, our study found a significant association between divorced status and the use of cervical cancer screening. This result contrasts with those of Seydou et al. 18 in Bamako and Ebu and Ogah 19 in Ghana, where marital status was not a significant determinant of intention to screen. This difference could reflect distinct social and cultural contexts, but in our case, it should be considered an exploratory avenue rather than a firm conclusion. It is possible that some divorced women, feeling more independent in managing their health or faced with a heightened perception of vulnerability, are more likely to use screening. Nevertheless, this result needs to be confirmed by studies including a larger and more representative sample.
Secondly, having received a prescription for screening at
In addition, having consulted a gynecologist for another reason was found to be significantly associated with cervical cancer screening. This result contrasts with that of Garson, 20 who, in a qualitative study, concluded that the frequency of medical consultations, whether regular or occasional, had no significant effect on women’s participation in screening or on their level of knowledge of cervical cancer. This discrepancy could be explained by differences in context or methodology. The association observed in our study suggests that CC screening is often offered opportunistically, that is, during consultations for other gynecological reasons. This shows the importance of the role of healthcare professionals in initiating screening, even outside a systematic framework.
Knowing that abnormal vaginal discharge is a symptom of cervical cancer also increased the chances of screening. This result corroborates that of Faye et al., 21 where knowledge of CC symptoms was significantly associated with screening. This finding is similar to that of Antaon et al. 22 in Brazzaville, who found that the lack of general knowledge about cervical cancer was a reason for the low screening rate. These results and similarities highlight the importance of health education in promoting screening, showing that the better-informed women are about the early signs of the disease, the more likely they are to undergo screening.
Furthermore, having received advice on CC screening from a health professional was significantly associated with screening. This result corroborates that of Emru et al. 16 in Ethiopia, who found that having heard about cervical cancer screening was associated with screening; and that of Lukorito et al. 23 in Kenya, who showed that good awareness of cervical cancer and its screening was significantly associated with the use of screening among women living with HIV. This result shows that the direct intervention of healthcare professionals, through advice or recommendations on screening, plays a decisive role in women’s decision to undergo screening, which argues in favor of the systematic use of educational messages during consultations, even outside the context of screening.
Limits of the study
There are several limitations to this study that should be highlighted. Firstly, the sample was restricted to a single institution, which may limit the generalizability of the results to other contexts or regions of Cameroon. In addition, the use of convenience sampling may have introduced a selection bias, reducing the representativeness of the participants, who may not reflect all women living with HIV in the region. The use of self-reported data also exposes participants to memory and social desirability biases, particularly concerning sensitive aspects such as testing history, HIV status, or sexual health, which may affect the reliability of the information collected. In addition, cultural beliefs and stigma associated with HIV and cancer may have influenced the sincerity of responses, impacting the validity of results. Certain associations, such as those observed among divorced women, must be interpreted with caution, given the small size of this subgroup, the wide confidence intervals, and the risk of unmeasured confounding factors. Finally, the cross-sectional nature of the study makes it impossible to establish causal relationships between the factors identified and cervical cancer screening practices, thus limiting understanding of the underlying mechanisms. Larger multicenter studies would be needed to strengthen external validity and deepen knowledge.
Conclusion
This study highlights the low coverage of cervical cancer screening among women living with HIV at Bonassama District Hospital, Cameroon, with only 18.37% of participants screened despite their increased risk. Several factors, such as marital status, prescription of screening by a health professional, and knowledge of cancer symptoms, were significantly associated with participation. These results underline the importance of strengthening health education and awareness programs, as well as systematically integrating cervical cancer screening into HIV follow-up services. At the clinical level, they highlight the need for healthcare providers to actively identify women at risk, counsel them, and systematically prescribe screening, while reinforcing caregiver training and standardizing clinical procedures. In terms of public health, these results underline the importance of targeted awareness campaigns, improved access to care, and the active involvement of policy-makers and healthcare providers to ensure effective integration of screening into existing HIV programs. Finally, larger, multicenter studies would be needed to improve the generalizability of the results, while helping to reduce cervical cancer incidence and mortality in this vulnerable population.
Footnotes
Acknowledgements
We would like to thank the Institut Supérieur des Sciences Appliquées à la Santé (ISSAS) for its institutional support throughout this training course. We would also like to thank the management of Bonassama District Hospital for making this study possible. We express our deep gratitude to the 283 participants who agreed to take part in this research. Their willingness to share their experiences was essential to the success of this work. Thanks to their collaboration, we were able to gain a better understanding of the issues involved in cervical cancer screening for women living with HIV.
Ethical considerations
The study complied with all current ethical standards. Ethical clearance was obtained from the Ethics Committee of the University of Douala (N°4363CE-Udo/06/2024/M), as well as research authorization from the Délégué Régional de la Santé Publique du Littoral (N°0333/ACR/MINSANTE/DRSPL/BCASS). Participants were informed of the objectives of the study and of their right to confidentiality. Informed consent was obtained, guaranteeing their voluntary participation. Confidentiality and anonymity were maintained during data collection.
Consent to Participate
All participants provided informed consent prior to their involvement in the study. They were fully informed about the purpose of the research, the procedures involved, and their right to withdraw at any time without any consequence. Efforts were made to ensure transparency and understanding, allowing participants to ask questions before providing their consent.
Consent for publication
All respondents gave their consent to the publication of anonymized information.
Author contributions
P.J.M.T. designed the study, collected the data and drafted the manuscript. A.K. carried out the data analysis and critically reviewed the content. V.C.K.N. contributed to the methodology and supervised the study, while J.R.M.T. carried out the statistical analysis and interpreted the results. K.C.F.T. reviewed the literature and drafted certain sections, and G.R.P.D. coordinated the research team and carried out the final revision of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.