
Abstract
Background
Early-stage cervical cancer screening is essential for providing women with a better chance of receiving effective treatment for precancerous and cancer stages. Delay in cervical cancer screening results in late presentation and cancer metastasis. National-level cervical cancer screening in resource-limited countries was scarce and not well studied in Africa based on national data specifically in Kenya, Cameroon, Nambia, and Zimbabwe.
Objective
To determine the prevalence and determinants of cervical cancer screening among eligible women in Kenya, Cameroon, Nambia, and Zimbabwe.
Methods
This study analyzed demographic and health survey data from Kenya, Cameroon, Nambia, and Zimbabwe. The data were extracted and analyzed by STATA version 15 and further analysis was done. Intraclass correlation coefficient, median odds ratio, and proportional change in variance were calculated to check the appropriateness of multilevel analysis. Variables with P-value < .25 were selected for multivariable multilevel logistic regression analysis. Finally, statistical significance between dependent and independent variables was assessed by odds ratios and 95% confidence intervals.
Results
The prevalence of cervical cancer screening in 4 African countries (Nambia, Kenya, Cameroon, and Zimbabwe) was 23.4 [95%CI: 22.8-24.1]. The determinants identified in this study were women of age 41–50 years [AOR = 1.47; 95% CI 1.24, 1.73], rural residence [AOR = .67; 95% CI .55, .81], women who have their own work [AOR = 1.1; 95% CI 1.0, 1.37], smoking status [AOR = 1.89; 95% CI 1.17, 3.0], age at first birth >=35 [AOR = 5.27; 95% CI 1.29-21.52], condom use [AOR = 1.79; 95% CI 1.46,2.19], husbands having worked [AOR = 1.5; 95% CI 1.08,2.11], rich household wealth [AOR = 1.43; 95% CI 1.13,1.8], and having health insurance [AOR = 2.2; 95% CI 1.8,2.7].
Conclusion
The prevalence of cervical cancer screening in Kenya, Cameroon, Nambia, and Zimbabwe was low as compared to World Health Organization (WHO) recommendations. Age, residence, work status, smoking status, women’s age at first birth, condom use, husbands having work, wealth status, and health insurance were the identified determinants of cervical cancer screening. Programme and policy interventions could address younger, rural residence women, poor wealth status women, women without work, and those who never use health insurance for the uptake of cervical cancer screening.
Introduction
Cancer is a public health problem worldwide and it is the threat to all nations.1,2 Cervical cancer is a global public health problem. One of the leading reproductive system infections is cervical cancer, which is caused by the human papilloma virus (HPV). Several studies have reported that sexual activity may increase HPV risk among women, and some medical studies have mentioned that human papilloma virus (HPV) is the primary factor for cervical carcinoma in women.3-5 Worldwide, cervical cancer is the fourth most common cancer with estimated 604,127 new cases in 2020 and 341831 estimated deaths (90% of all cancer deaths from low- and middle-income countries).6-8
Cervical cancer is one of the leading causes of cancer death in women in lower and middle-income countries (LMICs), where 83% of new cases and 85% of related deaths from poor resource countries, poor, vulnerable, and disenfranchised women were primarily affected. 7 Mortality and risk of acquiring cervical cancer are high in low- and middle-income countries.2,9 Cancer-specific mortality of women is leading in Africa and the lifetime risk and death in lower- and middle-income countries being high as 1.6% and .9% ,respectively. 4 The burden of cancer in Africa is underestimated and the ability to screen is low due to many reasons. Change in lifestyle results in an increase in the burden of cancer in sub-Saharan Africa, while in the region, it disproportionately results in poor access to health care and poor quality of screening services. 10 The burden of cervical cancer in sub-Saharan Africa is estimated at 84%. 11
Cervical cancer is the easiest and potentially preventable cancer; it is the cause of maternal morbidity and mortality especially in developing countries. With regular Pap smears and follow up, it is a highly treatable and curable cancer.3,4,12,13 Cervical cytology is a very specific test when the collection is with quality and reporting by well-trained technicians. 5 Human papilloma virus types 16 and 18 cause 70%–75% of the overall cervical cancer. For non-communicable diseases, accurate statistics, high-quality surveillance, and monitoring system are important for designing a fundamental action plan. 14 Therefore, studying the magnitude and determinates of cervical cancer is important to design or reshape the existing policy.
Studies revealed the uptake of cervical cancer screening in sub-Saharan Africa was 12.87%; 15 in Botswana, 72% of the women screened for cervical cancer ever by Pap smear; 16 20.6% of the women in Uganda screened for cervical cancer; 17 in other studies, only 29% screened for cervical cancer; 18 in a study conducted in Kenya, 16.4% of women screened; 19 and in Hara region, Ethiopia, 24.5% screened. 20 Furthermore, the previous study in Kenya showed that 46% screened; 21 in Guraga zone, Ethiopia, only 3.8% screened; 22 in Urban areas, Somali, 32.7% tested; 23 and other national level studies conducted in Kenya indicated that (19.4%) of women screened, 24 and only 5% underwent screening. 25
Determinants identified in previous literature with the uptake of cervical cancer were age,19,26-28 residence,19,29 marital status,28,30 occupation,19,29 educational status,15,19,20 wealth,17,19,30 knowledge on cervical cancer,15,17,25,31 age at first sex,22,28,32 human immune deficiency virus status,15,25,33 and awareness.17,20,22,25-27 Besides, other literature identified awareness on services,23,27 history of STI,27,32-34 multiple sexual partners,20,22,25 contraceptive use,15,18 provider recommendation, frequency of facility visit and history of vaginal examination, 34 binge drinkers, high sugar consumption, and insufficient physical activity. 19
Furthermore, concern about the gender of the health care professional, encouragement by HCPs and perceived quality of CCSS, 18 recommendation by staff was made prior to joining KNH CCC, 21 perceived susceptibility and awareness about screening locations, 15 perceived susceptibility to cervical cancer and no perceived embarrassment of Pap smear test, 24 doctors visit, 35 self-perceived susceptibility, having received community health education from health extension workers, 27 number of women lifetime sexual partners >1, older age at the first pregnancy, higher number of children born, 28 lack of adequate health care facilities, lack of symptoms, not feeling at risk and social stigma, 25 negligence, absence of medical problems, fear, economic reasons, 31 media exposure, had higher household wealth index, employed, insured, and had visited a health facility in 12 months 24 were the identified determinants of cervical cancer screening uptake.
World Health Organization (WHO) set the target for cervical cancer elimination by 2030 by implementing a “90%-70%-90%” target, which means by 2030, 90% of girls should be fully vaccinated with the HPV vaccine, 70% of women should be screened, and 90% of those identified with the cervical disease should receive appropriate treatment. 7 Understanding the status of cervical cancer screening is essential to design a new approach to screening, reshaping, and evaluating the existing methods of screening. To make evidence-based decision techniques, monitoring and understanding the current practice and factor of cervical cancer gives outshining impact to improve maternal health. Therefore, this study aimed to determine the prevalence and determinants of cervical cancer screening in Kenya, Cameroon, Nambia, and Zimbabwe.
Methods and Materials
Design and Study Period
Demographic and health survey was a cross-sectional study conducted every 5 years based on nationally representative areas. This cross-sectional study was conducted in demographic and health surveys of in Kenya, Cameroon, Nambia, and Zimbabwe based on the timeframe of DHS of each country. The demographic and health survey name of each country were as follows: Kenya, KE DHS-2014; Cameroon, CM DHS-2018; Nambia, NM DHS-2013; and Zimbabwe, ZW DHS-2015. The study period for each country was in Kenya from May 7 to October 20, 2014; in Cameroon, from 06/2018–01/2019; in Nambia, from May to September 2013; and in Zimbabwe, from July 6 to December 20, 2015. For detailed information, you can access on demographic health survey database at http://www.dhs
Data Source and Population
Showing the Survey Year and Total Weighted Sample for Each Country.

Study Variables
Data Collection Method
Demographic and health surveys implemented interviewer-based structured questionnaires. All reproductive-age women were interviewed by structured questionnaire with face-to-face interview techniques. Reproductive health-related standard questionnaires (in Woman’s Questionnaire) and several variables like socio-economic and demographic information were collected from women and households. For detailed information on the data collection methods, you can access (http://www.dhs.program.com). Among all reproductive-age women who were interviewed during the survey, 17,432 were included in this specific study. There are 4 model questionnaires in demographic and health surveys: A Household Questionnaire, a Woman’s Questionnaire, a Man’s Questionnaire, and a Biomarker Questionnaire. There are also several standardized Questionnaire Modules for countries with an interest in those topics. 36 For detailed information about the population, sample size, and questionnaire, access the demographic and health survey dataset (http://www.dhs.program.com). Strobe checklist was used for our study to check the content and guiding of the procedures of cross-sectional study. 37 The data which were collected during primary data collection were de-identified of individual profile, and there are no personally identified data in this study.
Variables Measurement
Measurement and Description of Dependent and Independent Variables in the Study.

Statistical Analysis
Data were extracted based on the previous literature and the availability of the variable in the demographic and health survey database. After the data were cleaned, categorized, coded, and weighted, the authors explored the descriptive statistics by using the frequencies and percentages of data and presented by using tables. Before running a multilevel analysis, appropriateness was checked. The appropriateness of multilevel logistic regression was checked by calculating intraclass correlation coefficient (ICC), a proportional change in variance (PCV), and median odds ratio (MOR). The value of ICC greater than 5% to consider a variety of cervical cancer magnitude across the cluster indicated that significant clustering was found, therefore, multilevel logistic regression was a more appropriate method of analysis for the data. The first model was built only with dependent variable, and then the AIC, ICC, and BIC were checked. The second model was built on dependent and community-level factors. The third model was built on dependent variable and individual-level variables. The final model was built with on dependent variable and both community and individual-level variables. The potential correlation was checked between independent variables. The proportional change in variance increased from the null model to the full model (final model), which indicates the variation of cervical cancer screening across the clusters. Four models were built; the null model, (model 1) only dependent variable; model 2, dependent variable and community-level factors; model 3, dependent variable and individual-level variable; and the final model (model 4) was a dependent variable and both the community-level and individual-level factors. The best model was selected by comparing the Akaike information criteria (AIC) level, and the model with the smallest Akaike information criteria (AIC) is the best-fitted model. Therefore, a model with the smallest Akaike information criteria (AIC) value was selected and all interpretations and inferences were made based on this model. After selecting the best-fitted model, bivariable and multivariable multilevel logistic regression was done to determine the uptake and determinants of cervical cancer screening in 4 African countries based on recent demographic and health survey data. Both bivariable and multivariable multilevel analyses were done accordingly. Variable in bivariable logistic analysis with P-value < .25 was selected in multivariable multilevel analysis. Variables with a P value <.25 at bivariable analysis were entered into the multivariable multilevel logistic regression model. Finally, the variable with the P-value ≤.05 is used to declare statistical significance with the dependent variable. The odds ratio with a 95% confidence interval was used to declare the statistical association between the dependent and independent variables.
Results
Background Characteristics of the Study Population
Background Characteristics of the Study Population With Uptake of Cervical Cancer Screening in Four African Countries in 2021.

Magnitude of Cervical Cancer Screening
The overall prevalence of cervical cancer screening in 4 African countries was 23.4 [95%CI: 22.8-24.1]. The prevalence of cervical cancer screening in each country is shown in Figure 1. The prevalence of cervical cancer screening of each country in 2021.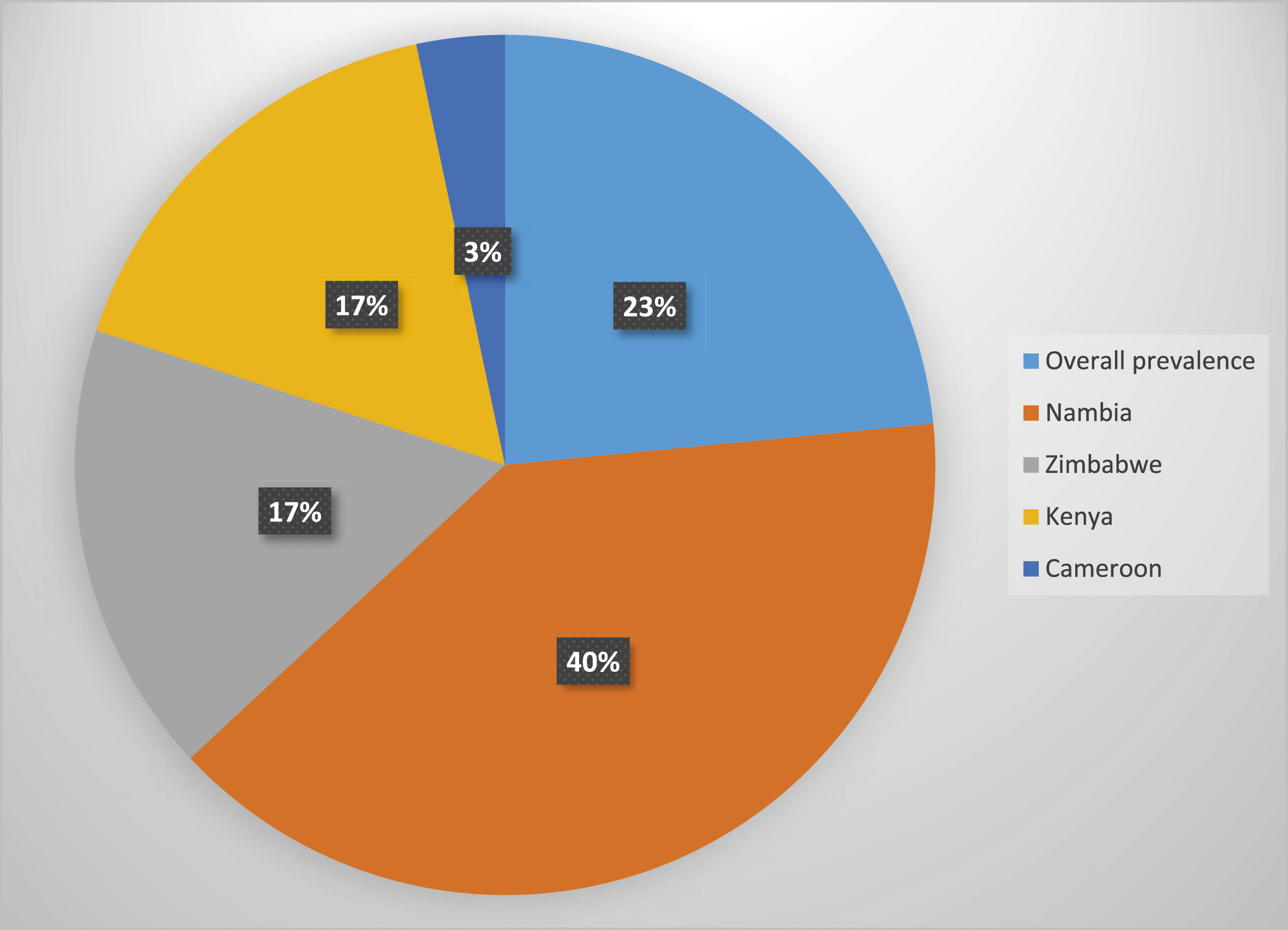
Random Effect Analysis
The hierarchal nature of the data violates the independent assumptions of the standard binary logistic regression model. Therefore, we fitted a multilevel mixed-effects generalized linear model by assuming that individual specific-effect is uncorrelated with the independent variables. Since there is no significant clustering effect at the household level, we were going to use the two levels, which were individual and community-level analyses. We fitted 4 models, which were the null model containing only the outcome variable, models 1 and 2 containing individual and community-level variables, respectively, and model 3, which contains both individual and community-level variables were fitted. Model 0 (empty model) was fitted without explanatory variables to test random variability in the intercept and to estimate the intraclass correlation coefficient (ICC), MOR, and PCV. Model 1 examined the effects of individual-level characteristics, model 2 examined the effect of community-level variables, and model 3 (full model) examined the effects of both individual and community-level characteristics simultaneously.
Model Comparison and Random Effect Analysis Result.

Determinants of Cervical Cancer Screening
Determinants of Cervical Cancer Screening Among Eligible Women in Four African Countries in 2021.

1 = reference.
Discussion
Cervical cancer is a serious and public health issue all over the world. 9 Understanding the status of screening and its determinants is important for early intervention and saving the lives of many women. Therefore, this study aimed to determine the prevalence and determinants of cervical cancer screening among women in 4 African countries based on recent demographic and health survey data. The prevalence of cervical cancer screening in this study was 23.4 [95%CI: 22.8, 24.1]. The current finding is higher than the study conducted in Sub-Saharan Africa, 12.87%; 15 Kenya, 16.4%; 19 Uganda, 20.6%; 17 Mozambique, 3%; 39 Cameroon, 4%; 40 Guraga Zone Ethiopia, 3.8%; 22 and Tigray region Ethiopia, 5%. 25 This could be due to the variation in the study setting and the variation in the access to health facilities across different countries. Specifically, in Sub-Saharan Africa, there was a high burden on health care providers and other contextual factors which may lower the use of cervical cancer screening. Furthermore, the older study period might lower the pooled estimate of cervical cancer screening. In the study conducted in Kenya, there is variation in sample size and it is conducted before the beginning of the sustainable development goal (SDG) which focuses on the reduction of maternal mortality. In the study conducted in Mozambique, the population used was 15–64 years old, which may lower the prevalence of screening uptake since recommended screening services were above 30 years old. Overall, the variation could be due to access to screening services, awareness of the services, availability of the services in health facilities, acceptability of the screening, and perceived risk of the individuals contributing to these variations. Furthermore, variations in behavioral intention to screen for cervical cancer in a different place were different.
However, the current study finding was lower than the study conducted in the urban region, Somali, 32.7%, 23 and Hara region, Ethiopia. 20 This could be due to many African countries applying for free of charge cervical cancer screening services. Another possible reason for this variation is the difference in susceptibility, access to the health facility, and cultural and social support for maternal health services. The other possible reason for this variation could be the availability of different testing methods, access to the services, and availability of well-performed providers. Furthermore, the variation could be due to variations in the sociodemographic characteristics of the study participants and variations in the methodology of the study. Overall, the finding implies that context-specific which is inclusive of the community and the health care aspect is very important to improve the screening status of women. This signifies that there is a need to institutionalize the services in those selected countries. On another side, the current finding was comparable with the study conducted in Debre Markos town, Northwest Ethiopia. 41 This could be due to health care policy and the availability of free pocket services in most African country is applicable.
This study identifies the determinants of cervical cancer screening in those in Kenya, Cameroon, Nambia, and Zimbabwe, based on the final model analysis of maternal age, residence, maternal and husband working status, wealth, smoking status, age at first birth, use of health insurance, and condom use were statistically identified determinants. The odds of cervical cancer screening among women’s age >=41 years were 1.47 times more likely screened as compared to the women’s age of <=40 years old. This finding is comparable with the study conducted in Cameroon, 40 Mozambique, 39 Kenya, 19 Hawassa, Ethiopia, 27 and the study conducted in Rwanda 28 which indicated that with the increased age, the odds of cervical cancer screening were increased. This could be due to the mean age of diagnosis of cervical cancer, where the age was between 35 and 44. The other possible explanation may be due to the symptoms of cervical cancer being presented above 30 years old. This gives an issue for the government which intensifies their intervention on lower age group women. The other possible reasons could be due to many country policies and guidelines recommending cervical cancer screening at higher area due to scarcity of resources. This implies that national and international organizations could emphasize younger women in the ways how to improve their screening services.
The odds of cervical cancer screening among rural residents were 33% less likely to screen for cervical cancer than the women who live in urban areas. Similar finding was observed in a study conducted in Kenya 19 and the rural part of Ethiopia 29 which showed that women living in rural areas were one of the reasons not screened for cervical cancer. In a previous study conducted in Cameroon, women who lived in rural areas were less likely screened for cervical cancer as compared with women who lived in urban. 40 This could be due to fare distance from the health facility and low community support which amplify their service use. In addition, this could be due to lake of awareness of risk and the perception of the women regarding cervical cancer was genetic only, which reduces the perceived susceptibility of the women.42,43 This finding was supported by a systematic review conducted worldwide which showed rural women were more likely to be presented with late-stage cervical cancer. 44 This implies that working with rural area women regarding cervical cancer screening and brief explanation of the risk regarding cervical cancer may improve the screening services. The odds of cervical cancer screening among women who had their own working were 10% higher than their counterparts. This finding was comparable with the study conducted in Rwanda 28 and India, 30 which indicated that women who had their work had higher odds of cervical cancer screening than those who did not work. The possible reason for this could be women who had their own work can get money, which covers the cost of the service and transportation.
The highest (rich) wealth of women was 1.43 times more likely to screen for cervical cancer than the women in the poor wealth category. A similar finding was observed in the study conducted in Rwanda, 28 Cameroon, 40 Maharashtra, and India 30 which indicated that rich women were more likely to get screened. The possible reason could be due to easy access to information and service. This could be due to the easily covered cost of services. Cost is one of the attributes of the low success of cervical cancer screening. This finding supported by a study conducted in South Africa which showed Pap smear use was higher among rich, wealthy status women. 45
Other determinants of cervical cancer screening were husband occupation. The odds of cervical cancer screening among husbands who have occupation have 1.5 times more likely screened than women’s husbands who have no occupation. Household economy and health care practices are intrinsically related. This could be due to the husband’s support in money or the cost that covers the services intake. Women who smoke cigarettes were 1.5 times more likely to get screened for cervical cancer than women who didn’t smoke. Women who smoke are at high risk of progressive cervical cancer. 46 The risk of cervical cancer was increased among smokers as compared with non-smokers. 47 The other prospective cohort study showed that former smokers were more likely to receive screening services than never smokers. 48 This could be due to the health risk and susceptibility of an individual being increased and the health system could give attention to those population groups. While one study conducted in the United States showed that smoking status and cancer screening have no association, 49 the possible reasons for this discrepancy were variations in the method of analysis and variable level of measurement.
The odds of cervical cancer screening among women who give their first birth above 35 years were 5.27 times more likely screened than women aged less than equal to 15 years. The World Health Organization recommend screening for cervical cancer at and above 30 years old and every 5 years after 30 years. The possible reason could be due to maternal ability to use services increased with age, and the risk of the individuals increased so the screening status could be increased. The odds of cervical cancer screening were 1.79 times more likely used among condom users as compared with those who never use a condom for recent sexual activity. The possible explanation for this is that women who used a condom could have an awareness of sexually transmitted diseases which increase the seeking behavior of an individual. Women who used health insurance were 2.2 times more likely to take cervical cancer screening as compared with the women who did not use health insurance. A similar finding was observed in the study conducted in California 50 which showed insurance status is the predictor of cervical cancer screening. Other study conducted in Latin America and Caribbean cities showed women with health insurance having higher odds of cervical cancer screening as compared with women without any health insurance (49). The possible explanation could be due to the service costs covered by health insurance and having health insurance could have some information about health services. The other possible reason could be the women who have health insurance had increased health literacy levels. In some lietratures, the women’s behavior and culture of the community were the factors for cervical cancer screening.51-54 While behavioral factors were not identified as determinant factors in this study, the author recommended researchers and demographic and health survey experts could assess the behavioral factors of the women.
One of the limitations of this study was that the culture, belief, and behavior of women were not assessed. While the current study only considered the status of screening which did not consider the frequency, the type and the indication of screening were considered as the limitation of the study. Some variables like vaginal examination, history of sexually transmitted disease, perceived susceptibility, doctors’ visit, cost of screening, and drinking status were not found in the demographic and health survey. In addition, the sample size for this specific stud was not calculated since we used all participants in the DHS data collection period which was considered a limitation of the study. As the strength of the study, the study considered both the individual and community-level variables with appropriate methods of analysis.
Conclusion
The prevalence of cervical cancer screening among women aged 30–49 years in 4 African countries was 23.4%, which is low compared with the WHO elimination target of more than 70% of eligible women who should be screened. This showed that cervical cancer was still a less prioritized problem in Africa. Government and non-government organizations could understand the real practice of cervical cancer screening and put their relief map on the increment of cervical cancer screening. In the final model, determinants of cervical cancer screening were identified such as maternal age, residence, maternal and husband’s working status, wealth, smoking status, age at first birth, use of health insurance, and condom use. The government and non-governmental organizations should address the screening service in rural areas. National and international interventions could address rural, lower-age, economically poor, and non-health insurance users. Therefore, policy and program interventions should target women who are younger and less than 40 years, who live in rural areas, women who did not have any work, poor household’s wealth, women who give their first birth at less than 15 years, women who never use health insurance, and women who did not use a condom.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
A waiver of written informed consent was secured from Demographic and Health Surveys (DHS) program data archivists to download the dataset for this study. After the data were downloaded from the measure DHS website the research of this study will maintain the confidentiality of the data. Since it was based on secondary data, which was publicly available, ethical approval was not required. However, we accessed the data set from the DHS website (![]() ) through registering or online requesting.
) through registering or online requesting.