
Abstract
Background:
Stunting is a condition of impaired growth and development that affects children worldwide. It impacts not only physical growth but also cognitive development and learning capacity. This study aimed to identify factors associated with stunting among families with children aged 5 years.
Design and methods:
A cross-sectional study was conducted from January to May 2023. Secondary data from the National Population and Family Planning Board. This study involved 2,014,369 children under 5 years old. The endogenous variables were poor housing condition and stunting, while the exogenous ones lacked access to clean water supply, inadequate toilet, maternal age, short birth intervals, high parity, and lower education. The data were analyzed using path analysis with IBM SPSS AMOS 22.
Result:
The path model showed goodness of fit with CMIN = 0.98, NFI = 0.99, CFI = 1.00, and RMSEA = 0.00. Poor housing conditions had a direct and statistically significant effect on stunting (b = 0.45; p < 0.001). High parity (b = −1.46; p = 0.002), no clean water supply (b = 0.49; p = 0.032), lower education (b = 0.74; p < 0.001), and short birth interval (b = 11.90; p < 0.001) exerted an indirect effect on stunting.
Conclusions:
Poor housing conditions, maternal age, and lower education had a direct effect on stunting. High parity, lack of access to clean water supply, lower education, and short birth intervals had an indirect effect on stunting.
Introduction
Stunting is a significant indicator of poor human capital quality and can reduce a nation’s long-term productivity. Its adverse effects on children result in irreversible impairments in both physical and cognitive development. A child is considered stunted if his or her height falls more than two standard deviations below the World Health Organization (WHO) 1 growth reference standard. Stunted children are more likely to grow into adults with lower levels of educational attainment, a higher risk of poverty, poorer health outcomes, and an increased likelihood of developing noncommunicable diseases. 2
The global prevalence of stunting is estimated at 165 million children under the age of 5 who experience physical growth issues, with Africa and Asia accounting for 90% of cases. The global target for fighting stunting is a 40% decrease by 2025. The government focuses on lowering the stunting rate because it has a significant impact not only on the growth and development of children but also the Indonesian economy in the future. 3
It will create a burden for the government in the future, especially in terms of increased healthcare expenditures. Stunting conditions can have short- and long-term effects on children’s health. The short-term health effect of stunting is an increase in child morbidity and mortality rates. In addition, it can negatively affect the cognitive, motor, and language development of children. In terms of the economy, it increases spending due to child health issues. Meanwhile, the long-term health effects on stunted children are increasing cases of obesity, obesity-related disorders, reducing reproductive health, and decreasing work capacity and productivity in the future. 4
Stunting is caused by a complex combination of factors, including multifaceted parenting practices, particularly exclusive nursing due to low parental education levels, poor housing, and limited access to sanitation and clean water, healthcare access, maternal health, and the family’s economic situation. The low income and education levels of parents, particularly mothers. 5 Mothers play an essential role in caring for and providing resources for their children. If a mother has a low level of education and awareness about stunting prevention methods, she will be unable to utilize a variety of appropriate and effective stunting protection and prevention methods for her child. Mothers who are well-educated will have access to knowledge and understanding about nutrition and child nutrition fulfillment, as well as knowledge about providing a safe and clean environment for their children at home. 6 This condition is related to child malnutrition, which is the most common cause of stunting. Malnutrition in the early childhood period might cause inflammation and abnormal metabolism of several hormones, such as leptin and glucocorticoids. These conditions can influence the epigenetic changes that result in neurogenesis alterations, brain development disorders, and synaptic dysfunction that ultimately affect the cognitive, memory function and motoric skills. 7
Environmental factors can also contribute to stunting in children. Environmental health refers to the surroundings’ condition that promotes an ideal state of health. Environmental health encompasses convenient housing conditions, access to sanitation facilities, clean water availability, proper rubbish disposal, wastewater management, and hygiene practices. Infectious disorders, such as diarrhea and respiratory infections can result in stunting due to environmental condition and poor hygiene practices. 8 Sanitation is considered adequate if it complies with health standards, such as having properly constructed latrines with a septic tank that is regularly maintained and emptied. Poor sanitation and hygiene can cause digestive issues that impede growth and affect the body’s resistance to diseases, increasing the likelihood of stunting in children. 9
According to UNICEF, stunting is caused by three causes: immediate, underlying, and basic. The immediate causes of stunting included inadequate dietary intake and disease. Underlying causes include household food insecurity, which is associated with limited access to a healthy diet among the poorest, bad dietary habits, lifestyle, and lack of nutritional awareness. 10 Underlying causes also consist of inadequate care and support to children where mothers not being able to optimize breastfeeding practices and early introduction of formula-based formula to the babies. Underlying causes stated that house, environment, and health services also affect children’s stunting. The basic causes of stunting included inadequate access to services, inadequate financial and human resources, and a sociocultural, economic, and political context. 11
Several stunting factors can be identified based on the information provided above. However, as they arise from various aspects of human life, the range of factors that can lead to stunted growth is broad. Therefore, further research on factors associated with stunted growth in children is required to identify more specific and effective indicators of stunting. Therefore, individuals interested in stunting preventive measures can focus on their efforts on using methods for preventing and treating growth failure in children.
Despite extensive global and national efforts to reduce stunting, Indonesia continues to face significant challenges, particularly at the sub-national level where disparities remain wide. East Java Province, one of the most populous and socioeconomically diverse regions in Indonesia, still reports high rates of stunting in several districts. While numerous studies have examined individual-level determinants of stunting, research that holistically investigates the structural pathways through which socioeconomic, environmental, and reproductive factors interact to influence child growth outcomes. This study addresses this gap by employing path analysis to explore both direct and indirect effects. Moreover, by leveraging large-scale, district-level data from over 2 million children under 5 years of age, this study provides robust evidence to support more integrated, multi-sectoral public health strategies. These contributions highlight both the urgency and novelty of this study in informing targeted interventions and regional health policy planning.
Methodology
Study area and population
This study utilized secondary data obtained from The National Population and Family Planning Board (BKKBN), which focuses on children aged 5 years. BKKBN conducted a large-scale population-based survey across all 79 cities and districts in East Java Province, Indonesia. The original data collection involved structured interviews with household respondents, conducted by trained enumerators using standardized questionnaires. The questionnaires included information on housing conditions, maternal and child health, water and sanitation, reproductive history, and education. A total of 2,014,369 children under the age of 5 were included in the analysis from the raw dataset. Relevant variables were aggregated at the city and district levels to conduct a macro-level analysis.
The National Population and Family Planning Board (BKKBN) conducts periodic family data collection. Family data collection is an activity of collecting primary data on family development, population, family planning, and family member data carried out by the local community (enumerator cadres) at a predetermined time, every 5 years through house-to-house visits to families. Local cadres conduct family data collection through direct interviews and observations through house visits using the form prepared by BKKBN. Interviews were conducted with the head of the family and his/her spouse who knew the characteristics of all family members well. The data collected by local cadres were then forwarded to systematic stages from local cadres, data supervisors in local areas, and data managers in city and district areas, until they were submitted to the BKKBN central data officer for further processing. A total of 79 cities and districts around East Java Province were selected because they are equal to the total number of cities and districts in Java Province, Indonesia.
Study variables
In this study, the endogenous variables were poor housing conditions and stunting. The exogenous factors were lack of access to clean water supply, maternal age, short birth intervals, high parity, and lower education. Each variable used in this study is defined operationally to ensure conceptual clarity and reproducibility. The variables are outlined as follows: Poor housing conditions (uninhabitable housing) indicate substandard housing types, which are measured by the damaged condition of the house’s roof, floor, and walls, and inadequate sources of electric lighting. Access to clean water is the source of water used by the family for drinking and doing other personal hygiene activities. Inadequate toilet, toilet that does not have a clean latrine that can be used personally by the family members. Maternal Age means the mother’s age when giving birth for the first time, where the maternal age condition that is not ideal is indicated if the mother gives birth for the first time at the age of less than 19 years and/or at the age of more than 35 years. Short Birth Intervals: means the birth interval of children born to the mother that occurs less than a 2-year span. High Parities, means that the number of children born to the mother is more than three children. Lower Education: The mother’s education level is lower than junior high school. These variables were measured by direct observation of enumerator cadres and respondents’ answers to the data interview conducted by enumerator cadres.
Data analysis
Path analysis was performed using IBM SPSS AMOS 22 for analyzing the data.
Ethical considerations
This study adhered to ethical principles for research involving human subjects. Although secondary data were used, ethical clearance was obtained to ensure compliance with institutional and national research standards. This study was approved by the Ethics Committee of Universitas Islam Al-Azhar (UNIZAR), with reference number 108/EC-04/FK-06/UNIZAR/I/2023. The data were anonymized and publicly accessible to authorized researchers, no direct informed consent from participants was required for this analysis. Nonetheless, the original data collection by BKKBN followed ethical procedures, including obtaining informed consent from respondents and ensuring confidentiality.
Results
Characteristics of the participants
Table 1 shows that the dominant age involved in the study is 0–23 months (33.9%). The dominant couples who filled out the questionnaire were those in reproductive age (98.9%). The highest percentage of families with economic status is prosperous (88.1%). Most mothers in this study were over 35 years old and gave birth at an older age (74.3%). Additionally, 58.8% of their education is under junior high school.
Demographic characteristics of children aged 0–59 months in East Java, Indonesia.

Model specification
Figure 1 shows the initial model in path analysis.
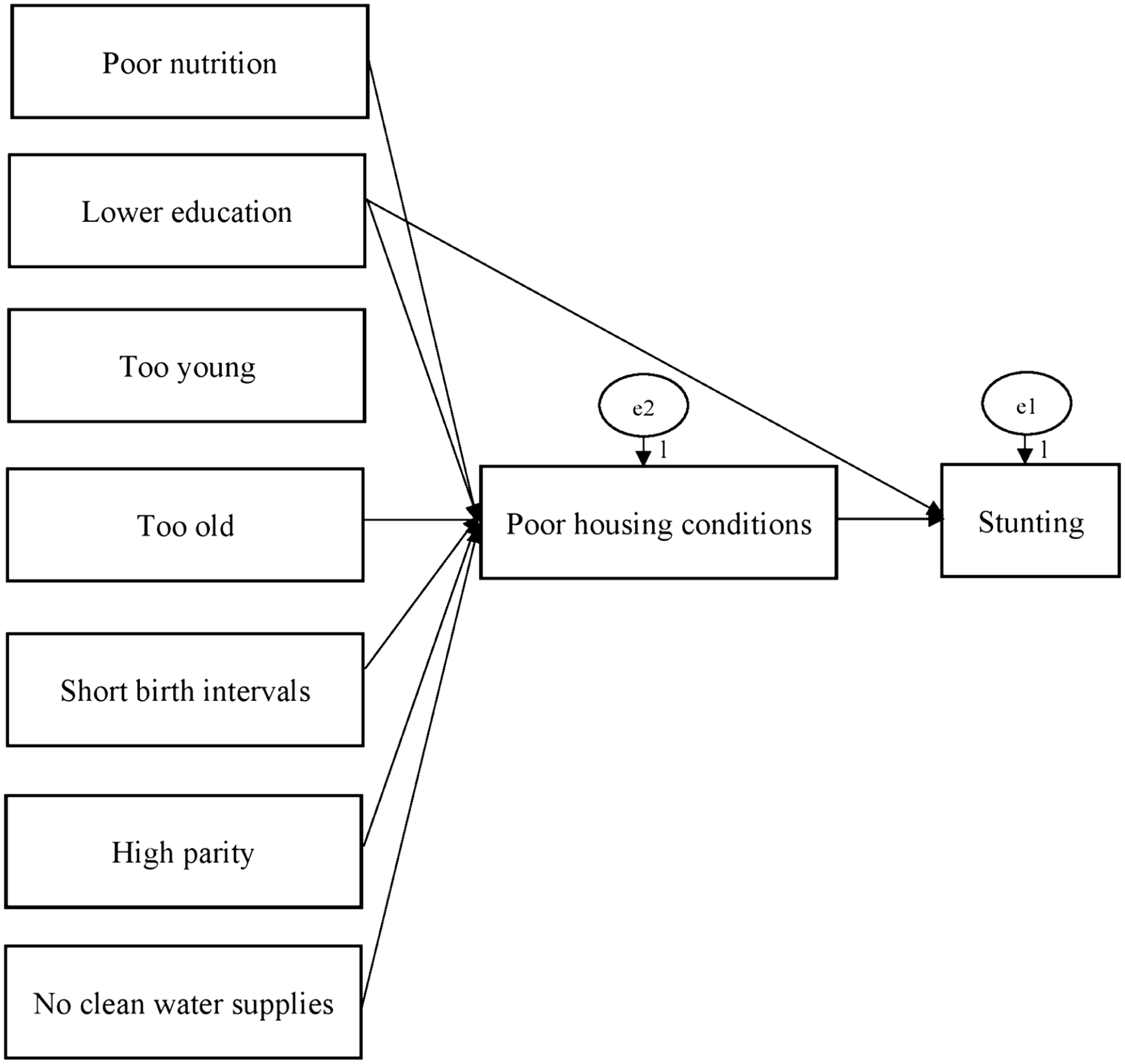
Structural model of path analysis.
Model identification
The study included 8 measurement variables, 2 endogenous variables, 6 exogenous variables, and 17 parameters. The degree of freedom (df) was 6, indicating an overidentified model that allowed path analysis to be conducted.
Fit model and estimation parameters
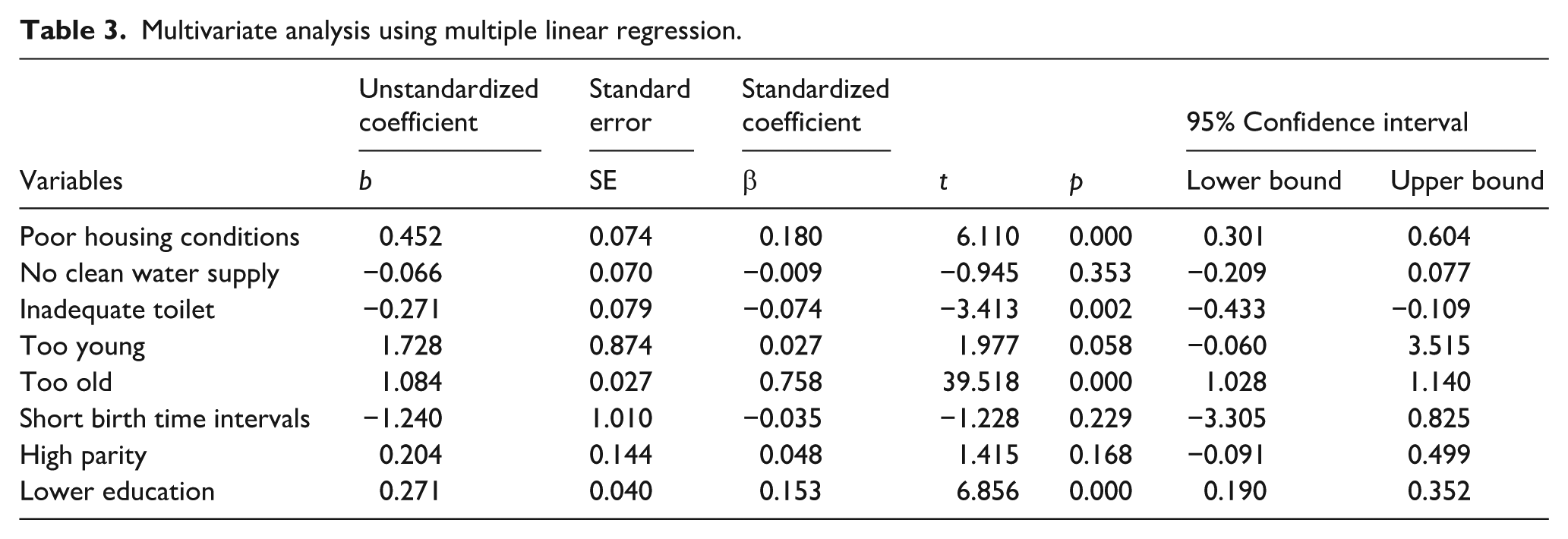
The suitability of the path analysis model was checked using the best variable correlation model (SPSS) called the saturation model based on the collected sample data. Figure 2 shows the structural model after estimation using IBM SPSS AMOS 22. Table 2 shows the indicators that show the suitability of the path analysis model. The chi-square test was used to assess the goodness of fit of the final model and the goodness of fit indices, such as the Root Mean Square Error of Approximation (RMSEA), goodness-of-fit index (GFI), adjusted goodness-of-fit index (AGFI), normed fit index (NFI), relative fit index (RFI), incremental fit index (IFI), Tacker Lewis index (TLI), and comparative fit index (CFI). The GFI, AGFI, NFI, RFI, IFI, TLI, and CFI values range from 0 to 1, with recommending values greater than 0.90 indicating a good fit. Conventionally, there is a good fit if the RMSEA is under 0.05, and there is an adequate fit if the RMSEA is less than 0.08. It shows that the Goodness of Fit Measure finds the CMIN fit index by 0.98 with p = 0.435 (>0.05); NFI = 0.99 (>0.90); CFI = 1.00 (>0.90); and RMSEA = 0.00 (≤0.08), which means that the empirical model meets the criteria specified and is equivalent to the empirical data. The non-standardized path coefficient demonstrates the correlation between the exogenous and endogenous variables in the original unit of measurement. Table 3 shows the calculation results obtained using IBM SPSS AMOS 22 computer software program.
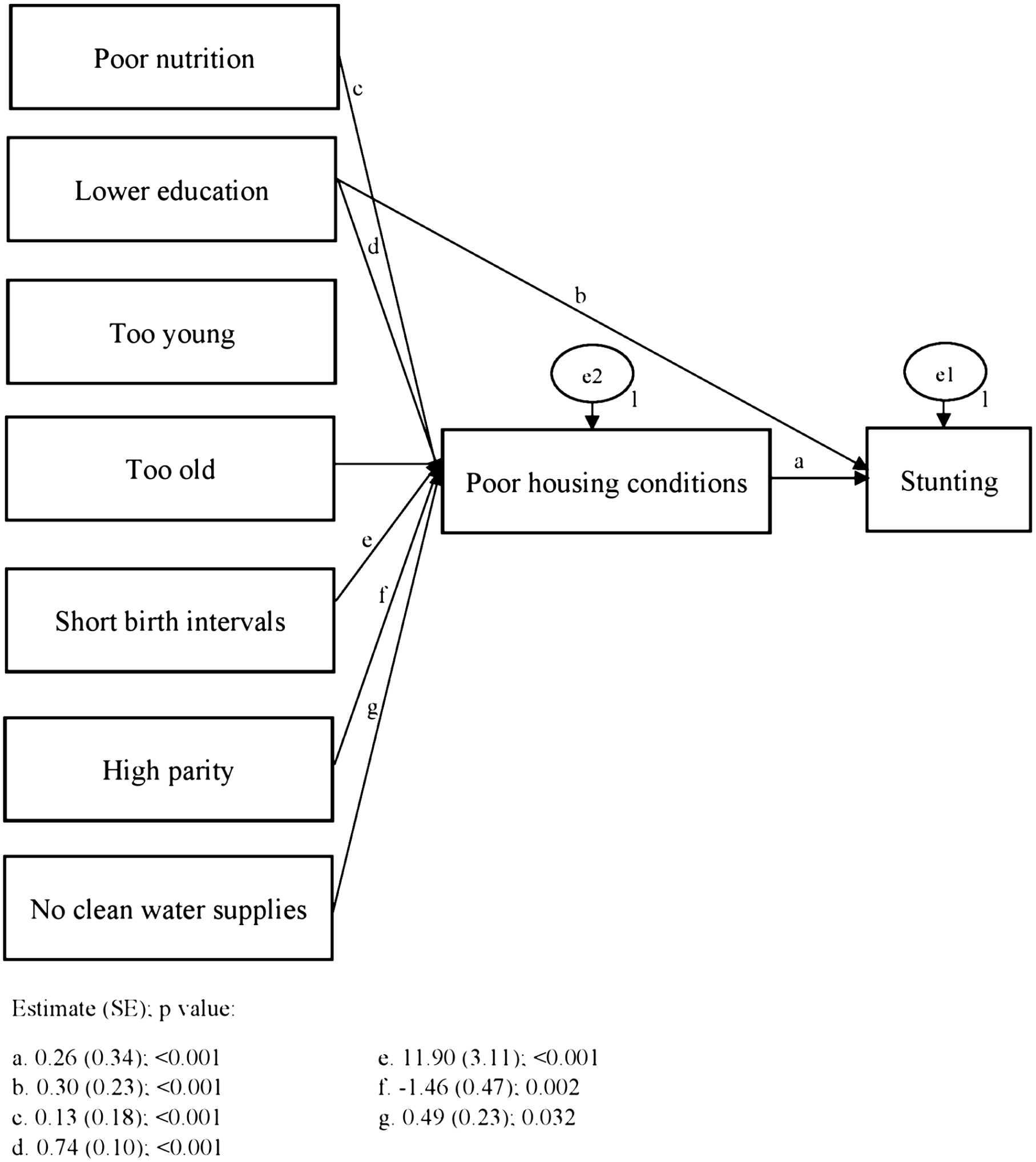
Structural model of path analysis using unstandardized solution.
Path analysis results.

Multivariate analysis using multiple linear regression.
Model re-specification
The model in this study corresponds with the sample data as indicated by the saturation model and the path coefficient, which is more than zero and statistically significant; thus, the path analysis model cannot be recreated.
Figure 2 illustrates the structural model developed through path analysis, which captures both direct and indirect relationships between sociodemographic, environmental, and reproductive factors and childhood stunting. The diagram highlights poor housing conditions as a central mediating variable that connects multiple exogenous predictors to the stunting outcome variable. The model demonstrates that maternal age (particularly being too old), lower education, and poor housing conditions have significant direct effects on stunting. Specifically, older maternal age (b = 1.14) exerted the strongest direct impact, followed by lower maternal education (b = 0.30) and poor housing conditions (b = 0.26). These findings suggest that biological and socioeconomic vulnerabilities directly influence child growth outcomes. In addition, the model identifies several significant indirect effects mediated by poor housing conditions. Short birth intervals (b = 11.90), lower education (b = 0.74), lack of access to clean water (b = 0.49), and high parity (b = –1.46) significantly affect housing quality, which in turn influences stunting risk. These pathways emphasize the cumulative effect of reproductive behavior, maternal disadvantage, and environmental deprivation on the child nutritional status of children.
This study reports both unstandardized path coefficients (b) and standardized path coefficients (β) to provide a comprehensive interpretation of the relationships between variables. Unstandardized coefficients (b) indicate the raw change in the dependent variable for each unit increase in the independent variable, whereas standardized coefficients (β) express the strength of the relationship in standard deviation units, allowing comparison across variables with different measurement scales. Direct effects of three key variables on stunting were observed. First, maternal age was significantly positively associated with stunting (b = 1.14, SE = 0.11, p < 0.001; β = 0.79). This implies that the stunting score increases by 1.14 units for each one-unit increase in the maternal age score (indicating advanced maternal age), with a strong standardized effect. Second, poor housing conditions were also positively associated with stunting (b = 0.26, SE = 0.34, p < 0.001; β = 0.10), indicating that a deterioration in housing quality contributes to an increase in stunting, although with a relatively modest effect size. Lower maternal education was found to significantly predict higher levels of stunting (b = 0.30, SE = 0.23, p < 0.001; β = 0.17), suggesting that limited educational attainment among mothers moderately increases the likelihood of stunted growth in children. The indirect effects were primarily channeled through poor housing conditions. High parity was negatively associated with poor housing conditions (b = –1.46, SE = 0.47, p = 0.002; β = –0.87), a result that may warrant further contextual exploration as it appears counterintuitive. Lack of access to clean water supply was positively associated with poor housing conditions (b = 0.49, SE = 0.23, p = 0.032; β = 0.17), indicating that poor water infrastructure tends to coexist with substandard housing, thereby indirectly influencing stunting risk.
Lower maternal education also had a strong indirect effect on stunting through poor housing conditions (b = 0.74, SE = 0.10, p < 0.001; β = 1.05). This finding underscores the broader socioeconomic mechanisms by which educational disadvantage translates into environmental health risk factors. Furthermore, the short birth interval demonstrated a substantial indirect effect on stunting via poor housing conditions (b = 11.90, SE = 3.11, p < 0.001; β = 0.85). Although the unstandardized coefficient appears to be disproportionately high, the standardized value confirms a strong indirect association. This relationship may reflect the cumulative socioeconomic burden experienced by households with closely spaced births, which compromises their capacity to maintain adequate living conditions.
The model fit indices (RMSEA = 0.00, CFI = 1.00) are exceptionally high. While such near-perfect fit values suggest that the model adequately represents the data, they are relatively rare in empirical research and may indicate potential model overfitting or the presence of a saturated model. The authors acknowledge this and attribute the strong fit to the large sample size and the use of aggregated secondary data, which may reduce variability and enhance model convergence. The model was developed based on theoretically supported pathways, which may contribute to the observed fit. However, slightly overfitting or model saturation cannot be entirely ruled out. Therefore, the results should be interpreted with caution, and future studies should validate the model using independent datasets to ensure generalizability and robustness.
Discussion
The study’s findings show that a variety of characteristics, including low levels of education, limited access to clean water, frequent pregnancies, and high numbers of children, are all associated with poor living conditions. In contrast, inadequate housing, being too old, and a lack of education are all associated with stunting. The cognitive function and development of stunted children are impacted, resulting in suboptimal cognitive potential. Furthermore, stunting leads affected children to be shorter in stature than other children of the same age. Stunting occurs during the first 1000 days of life and is influenced by a variety of factors.
According to Chilinda et al., 12 factors that lead to stunting include poor nutrition, recurring conditions, insufficient psychosocial stimulation, low socioeconomic status, nutritional deficiencies in the mother, unbalanced nutrition, and suboptimal sanitation and environmental conditions. Environmental and living conditions, low birth weight, nursing duration, low hemoglobin levels in the blood, maternal age and education, number of children, and maternal physical condition, such as height and weight, all influence stunting. 13 The complicated dynamics underlying the various causes of increased stunting risk in children.
According to UNICEF’s conceptual framework, stunting can be categorized into three levels: immediate, underlying, and basic causes. Immediate causes include inadequate dietary intake and infectious diseases, both of which directly impair a child’s nutritional status and growth. 14 The underlying causes include household food insecurity, poor feeding practices, inadequate maternal and child care, unhealthy living environments, and limited access to health services. At the most fundamental level, basic causes refer to broader systemic issues such as insufficient access to resources, low maternal education, poverty, and sociocultural and political constraints. 15 Although we acknowledge the importance of nutritional intake, particularly protein and infection-related factors, as direct causes of stunting, this study did not explore these biological mechanisms in detail due to data limitations. Instead, this study focuses on maternal and environmental determinants, which are considered key underlying and basic causes in the UNICEF framework. This focus is also contextually relevant to the study area. Specifically, maternal age (too young or too old at first birth), short birth intervals, high parity, and low maternal education. Poor housing conditions, lack of access to clean water, and inadequate toilet facilities were the environmental factors examined. These variables serve as structural determinants that directly or indirectly influence child growth and are strongly associated with stunting persistence in the studied region. This discussion has been added to the revised manuscript to clarify the scope and rationale of the study focus while acknowledging the broader framework of stunting determinants.
Lower education affects stunting through poor housing conditions
This study reveals that lower maternal education has an indirect effect on stunting through poor housing conditions. Mothers with low educational attainment often lack the knowledge, financial capacity, and empowerment required to ensure optimal living environments for their children. These findings are consistent with those of previous studies, such as those by Yani et al. 16 and Goudet et al., 17 which indicate that maternal education is strongly associated with stunting. According to research conducted by Azizah et al., 18 the educational background of the mother is an indirect factor that contributes to stunting in children.
This study found that mothers with low levels of education have a 3.01% probability of having stunted children because low-education parents experience difficulties in providing optimal home settings for their children’s growth and development. Inadequately educated parents, particularly children, frequently struggle to provide for or avoid stunting in their families, particularly children. 19 Education can assist parents in understanding, adopting, and maintaining ideal efforts to prevent childhood stunting. Mothers with low levels of education confront additional obstacles in addressing their households’ needs, which include shelter, food, water, and adequate facilities for their children. 20 A mother’s capacity and empowerment to offer an optimal environment and sanitation for promoting children’s development might be hampered by a lack of education, both in terms of knowledge and finances. Furthermore, educated mothers are more likely to grasp preventive measures for stunting and to be financially self-sufficient, allowing them to offer acceptable living conditions for their children. 21
Educated mothers are more likely to be able to implement child safety parenting practices during the growth and development period, such as providing and ensuring that the child’s living environment is appropriate and clean, protecting them from disease-causing bacteria and viruses. Educated mothers are also more likely to have adequate household resources, particularly those related to the viability of their home. 20 Consequently, stunting can be prevented in children. On the contrary, a lack of education results in moms having limited information, making it harder for them to seek suitable environmental cleanliness and sanitation. Poor environmental and living conditions may cause stunting in children. 16 As a result, the quality of an individual’s education can be said to have favourable impact on their living situations. The state of a house can have a negative impact on stunting. 22 A child is at greater risk of stunting if they are constantly exposed to a deteriorating home environment. Inadequate housing circumstances, such as low-quality materials, unsanitary conditions, and unclean floors, can increase the risk of stunting in children. 23 Azizah discovered that inadequate living conditions and poor sanitation directly impact stunting. As a result, poor sanitation, inadequate living circumstances, and an unhealthy environment might worsen stunting. 20 Inadequate housing and environmental conditions expose children to a variety of infections or illnesses, thereby increasing their risk of stunting in children. 24
This structural pathway underscores the need for multi-sectoral public health interventions, in which lower maternal education leads to poor housing conditions that subsequently increase the risk of stunting. It supports the Indonesian government’s national strategy to accelerate stunting prevention, which advocates integrated approaches that address not only health and nutrition but also environmental determinants and maternal empowerment. By demonstrating how educational disadvantage translates into environmental deprivation, this study offers novel evidence for targeting housing improvements as part of stunting prevention programs, especially in high-burden provinces like East Java.
Limited access to clean water affects stunting
According to the study’s findings, the variable of limited access to clean water has an indirect effect on stunting through poor housing conditions. The findings of this study agree with the research conducted by Titaley et al., 13 who discovered that a lack of clean water increased the likelihood of stunting in children. Inadequate access to clean water can have an impact on the house and living environment, increasing the risk of stunting in children. Previous research has indicated that poor living circumstances, which are influenced by the availability of safe drinking water, might worsen stunting in children. Poor housing conditions, including substandard housing types, floor types, and access to clean water and household electricity, also contribute to the risk of stunting in children. The unsuitable condition of the house and living environment is a social determinant of health, which comes from non-medical elements but can affect health. 16
According to Gizaw et al., children’s stunting is linked to poor hygiene, environmental contamination, and inadequate sanitation conditions in their living environment. Environmental contamination can cause bacterial translocation, diarrhea, systemic inflammation, metabolic abnormalities, and nutritional malabsorption in children, all of which are linked to stunting. 25 Children may be exposed to bacterial and microorganism contamination in the food and drink they consume, increasing their risk of developing stunted diseases. Multiple negative exposures caused by poor housing conditions can significantly increase the risk of vitamin and mineral deficiencies in children, which induces. 26
Short birth intervals affect stunting
Pregnancies with a short interval between them have an indirect effect on stunting due to inadequate housing conditions. These findings align with those of Sultana et al., 27 who discovered that children born to mothers with 24-month interpregnancy intervals had a 36% greater risk of stunting. Similarly, Chungkham et al. 28 found that children born at 24-month intervals had a 46% increase in stunting. Furthermore, a study in India found that if a child was born to a mother with a short pregnancy interval, notably less than 3 years, the probability of stunting increased substantially. 29
Mothers who have multiple children in a short time may have difficulty finding acceptable housing. 27 Stunting is more likely in infants born with birth intervals of 12 months or between 12 and 23 months than in infants born with birth intervals of 24–35 months. 28 Having several children in a short time can impair a mother’s ability to provide the finest care and support for her child’s growth and development. Mothers with short birth intervals may not have fully healed after giving birth and may lack the time and attention required to provide their child with the best possible environment. A study on children under the age of 5 in Peru discovered that mothers with birth intervals of more than 24 months were a protective factor in lowering the incidence of stunting in their children. 29 In contrast, children born to mothers who had children during the preceding 24 months are more likely to suffer stunting within the first 60 months of life. In addition, Islam et al. 30 discovered that children born to mothers with short birth spacing intervals (33 months) are 30% more likely to be stunted. Bliznashka and Jeong’s research also confirmed this, stating that 42% of children born from short birth intervals were stunted. Mothers can display behavior that does not support the implementation of optimizing efforts related to domestic conditions and resources as stunting prevention, for example housing conditions, sanitation, and the environment around where they live. 31
Mothers who have a high focus and burden of care tend to be less able to strive for and facilitate cleanliness and adequacy of homes and living conditions, where children are more susceptible to stunting in the presence of poor housing conditions. Children are exposed to various diseases and recurring infections due to pollution in their living environment, which may cause stunted development. According to Sahiledengle et al. and the team, inadequate living circumstances in terms of toilets, access to clean water, house floor, and child stool disposal contributed to the occurrence of stunting in children. Children who live in homes with inadequate and unclean flooring are more likely to suffer from stunting than children who live in suitable and hygienic homes. Poor living conditions are a risk factor for several population-based diseases caused by viruses and bacteria, such as typhoid, hepatitis, and diarrhea. This condition puts children at a greater risk of stunting. 32
High parity affects stunting
Our results showed that poor housing conditions have an indirect impact on stunting in many children. The findings agree with those reported by Lewa in 2020 that mothers with multiple children have a greater burden of caring for and fulfilling home resources than those with fewer children. Another study conducted by Vaivada et al. 2 found that the number of children and the condition of the house had an effect on stunting in children under the age of 5. Stunting in children can be influenced by mothers who have a large number of children. 20 Mothers with this condition face a various obstacles in performing parenting and home functions. 30 One of these issues is assuring the availability of a house and an appropriate living environment to assist their children’s growth and development. Mothers with many children face additional challenges in terms of parenting functions, resource allocation, and access to resources and the environment in the home.13,17 Mothers who have a large number of children are more likely to devote their time to fundamental child care duties rather than working on issues such as sanitation, environmental cleanliness, and sufficient housing. According to the research of Putri et al., mothers who have many children are more likely to have stunted children aged 6–24 months. Mothers with a large number of children have a 30.40 times increased risk of their children being stunted than moms with fewer children. 33
Children’s health might be influenced by their living conditions. Tusting’s found that good living conditions reduced the likelihood of a child developing stunting by up to 12%. 34 According to Tusting, inadequate housing conditions include factors that prevent access to clean and sufficient water, insufficient house building materials, poor sanitation, pollution in and around the home, and overcrowded housing. These various circumstances cause children to encounter a range of health issues, including impediments to healthy growth and development, one of which is stunting.
Poor housing conditions directly affect stunting
The majority of sanitation findings in Indonesian rural areas, including ownership and type of latrine, the absence of a septic tank, cleanliness of latrines, and the practice of open defecation and disposal of children’s feces outside of latrines, are associated with an increased risk of stunting in children under 5 years of age. Children who grow up in contaminated environments with poor sanitation are 40% more likely to suffer from stunting, and the risk is much higher in rural and suburban settings than in urban areas. According to one study, children in rural areas are at the greatest risk of stunting because most individuals still use open defecation. Open defecation has been associated with a higher prevalence of stunting in children under the age of 5. This behavior pollutes the environment by spreading pathogenic bacteria through feces. Intestinal illnesses, such as diarrhea and Environmental Enteric Dysfunction (EED), can have a negative impact on children’s nutritional status by lowering appetite and interfering with nutrient absorption, resulting in malnutrition and growth issues. The use of latrines that do not meet health requirements, open defecation, and the disposal of children’s feces in places other than latrines expose children to environmental pollution, facilitating the transmission of pathogens originating from feces and increasing the incidence of stunting in children under the age of 5. 23
A Peruvian study found that improper toddler feces disposal and poor usage of latrines by children due to a high risk of falling increases the prevalence of diarrhea, intestinal worms, and the incidence of stunting in children under the age of 5. Proper household sanitation can help reduce the prevalence of stunting and severe stunting in Indonesian children aged 5 years. Stunting can be reduced in children aged 0–23 months if proper restroom facilities are available. 35 Efforts to reduce stunting in children under the age of 5 in Indonesia require sensitive nutrition interventions such as improving environmental sanitation, constructing latrines that meet health requirements, and promoting health education to raise public awareness and discourage open defecation behavior. Furthermore, feces, even toddler feces, must be appropriately disposed of in latrines to prevent fecal transmission as a disease vector in humans and the surrounding environment. 8 These activities attempt to break the chain of disease transmission, such as diarrhea, EED, and intestinal worms, and ultimately reduce the prevalence of stunting in Indonesian toddlers.
Maternal age directly affects stunting
The mother’s age is an important factor that can influence stunting in children. 29 If a woman who is not ready to marry is compelled into doing so, she may not take proper of her pregnancy, resulting in low birth weight and stunting. Mothers who are too old typically have less stamina and excitement for caring for their pregnancy, which might increase the risk of low-birth-weight rates.36,37 Studies have shown that older mothers have a higher risk of giving birth to low-birth-weight babies compared with mothers aged 20–24 years. Furthermore, pregnant women over the age of 35 years may experience a decrease in nutritional absorption, resulting in an imbalance in food consumption. Furthermore, their immune system may deteriorate, increasing the mother’s risk of numerous ailments. 38
Conclusion
Stunting is affected by several complex variables. Poor housing conditions, maternal age, lower education levels, having many children, lack of clean water supply, and short birth intervals were identified as variables that contribute to stunting. Poor housing conditions, maternal age, and lower education level directly affect stunting. On the other hand, having many children, a lack of clean water supply, lower education level, and short birth intervals indirectly affect stunting through poor housing conditions in East Java.
Suggestion
Based on our findings, this study recommends some intervention programs by relevant institutions to address poor housing conditions, mother’s age at childbirth, mother’s education, couples’ preference for children, clean water supply, and birth intervals to prevent stunting. The interventions are expected to initially target teenagers and prospective brides, couples of childbearing ages, pregnant women, breastfeeding mothers, and mothers of children aged 5 years.
Footnotes
Acknowledgements
We would like to acknowledge the Universitas Indonesia for awarding the 2022-2023 PUTI research grant (Number: NKB-425/UN2.RST/HKP.05.00/202).
Ethical considerations
The study was approved by Ethics committee with No. 108/EC-04/FK-06/UNIZAR/I/2023.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by grant from Universitas Indonesia (PUTI Q2 Batch 3, 2022-2023).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data presented in this study are available on request from the corresponding author.