
Abstract
Background:
Breast cancer represents a significant public health concern in Jordan. Female schoolteachers, as an often underserved demographic, possess the potential to significantly influence community health behaviors. This study aims to assess the knowledge, attitudes, and practices (KAP) regarding breast self-examination (BSE) among female schoolteachers in Irbid, Jordan.
Design and Methods:
A cross-sectional study of 518 female schoolteachers aged 23–41 in Irbid’s public schools used a self-administered questionnaire to evaluate their socio-demographic characteristics, knowledge, practices, and attitudes toward breast self-examination (BSE).
Results:
The study found that the average age of participants was 32.77 years, with 64.1% holding a baccalaureate degree. Most participants (55%) had been employed for 1–5 years, and 60.4% resided in the city of Irbid. Regarding reproductive history, 44.6% had their first child between the ages of 23–25 years, and 46.5% had 1–3 children. Breastfeeding was practiced by 62.7% of the participants, with 44.8% breastfeeding for a duration of 1–12 months. Additionally, 58.3% of the participants demonstrated knowledge of breast self-examination (BSE), and positive attitudes toward BSE were widely observed. Factors influencing knowledge and practices included age, breastfeeding practices, and the age at first childbirth. Meanwhile, attitudes were significantly impacted by marital status, breastfeeding practices, employment period, and breastfeeding duration.
Conclusion:
The study revealed that although a majority of women in Irbid demonstrated knowledge of breast self-examination (BSE), their actual practices were insufficient. Given the significance of BSE in resource-limited settings, the findings underscore the necessity for enhanced awareness campaigns and educational initiatives aimed at improving BSE practices and promoting breast cancer prevention.
Keywords
Introduction
Breast self-examination (BSE) is a method of physical examination in which women evaluate their own breasts and surrounding tissues, typically in private settings. It is widely promoted as a simple, non-invasive, cost-effective, and empowering technique for women to monitor changes in their breast health. While BSE is often recommended for women of all ages, it is considered particularly appropriate for younger women. 1
Knowledge in this context refers to the systematic acquisition, organization, and dissemination of information about the procedure, encouraging a culture of continuous learning. 2 Attitudes refer to the cognitive and emotional evaluations that predispose individuals to engage in specific behaviors. 3 Practice is defined as the consistent performance of activities that lead to desired outcomes, which can be adapted to improve both efficiency and effectiveness. 4 Breast cancer remains the most common cancer among women worldwide, and the American Cancer Society has long advocated for BSE education. 5 Although breast cancer is rare among adolescents, BSE education targeted at younger women is seen as beneficial, potentially helping them develop lifelong breast health habits. 6 In June 2003, the American Cancer Society updated its guidelines to recommend that BSE be an option for women starting in their 20s. 7 Studies indicate that women who perform BSE more frequently tend to be those who are married, have higher educational attainment, are pre-menopausal, have a family history of breast cancer, or have experienced benign breast disease. No significant associations have been found between BSE frequency and factors such as religion, hormone usage, or body mass index. 8
Early detection of breast cancer allows for timely treatment and has the potential to reduce mortality. 9 While breast cancer incidence is increasing globally, mortality rates have remained relatively stable in several regions, including the United States and many Western and developing countries. 10 The yearly prevalence rate of breast cancer in the United States varies over time and is impacted by a range of demographic variables. Nevertheless, current estimates suggest that approximately one in eight women will be diagnosed with breast cancer at some stage in their lifetimes. More precisely, the American Cancer Society’s data reveals that there were roughly 281,550 incident cases of invasive breast cancer and approximately 49,290 cases of non-invasive (in situ) breast cancer in the year 2021. According to the 2019 report from the Jordan National Cancer Registry, breast cancer is the most prevalent type of cancer in Jordan, accounting for 20.3% of all cancer cases.
Particularly among female individuals, it exhibits a greater prevalence, accounting for 38.5% of all cancer diagnoses, with a reported total of 1524 cases. In contrast, breast cancer does not rank among the top five cancer types for male individuals, thus indicating a significant gender disparity in its occurrence. Other frequently observed cancers in females encompass colorectal cancer (9.7%) and thyroid cancer (6.2%); however, breast cancer undoubtedly maintains its position as the foremost type of cancer.
Mammography is widely regarded as the most effective method for detecting breast cancer. 11 However, access to mammography and clinical breast examinations is often limited for Jordanian women, particularly those from lower socioeconomic backgrounds, due to cultural discomfort and reluctance to expose their bodies to healthcare providers. 12 Consequently, private screening methods, such as BSE, may play a more significant role in promoting breast health awareness in Jordan. Despite the prevalence of breast cancer among Jordanian women, awareness and practice of BSE remain low, highlighting the need for research into factors influencing women’s adoption of BSE. Unlike other early detection methods, BSE is a personal behavior that can be performed independently of healthcare facilities. To perform accurate breast self-assessments, women must be able to recognize subtle changes in their breast tissue. For BSE to be effective, women must be adequately trained and feel comfortable practicing the technique regularly. This study focuses on female teachers as a target group, as they can serve as influential role models for promoting BSE education, provided they possess sufficient knowledge, positive attitudes, and appropriate practices toward BSE.
This study aims to explore the knowledge, attitudes, and practices of women regarding BSE among female teachers in Irbid, a city in northern Jordan, and to evaluate how personal attributes and socio-demographic factors influence these aspects of BSE.
Methodology
Study design
The objective of this study is to assess the knowledge, attitude, and practice of breast self-examination (BSE) among female schoolteachers. It is a cross-sectional study conducted as a population survey. The cross-sectional design is chosen because it allows for a large number of participants, data collection on numerous variables, and suitability for exploratory research.
Setting
The study took place in Irbid, the third largest city in Jordan in terms of population. With a population of approximately 2,095,700, Irbid Governorate, which includes Irbid and neighboring cities and villages, has the highest population density in the kingdom. Our sampled population consists of schoolteachers from public schools for girls. The sample includes female schoolteachers from all education directorates in Irbid. The public schools in Irbid are divided into three education directorates: first, second, and third.
Study population and sampling technique
The study population comprises all female schoolteachers in Irbid city. Among the three education directorates, there are 3915 female schoolteachers in the first directorate, 1489 in the second directorate, and 576 in the third directorate. The total number of female schoolteachers in public schools for girls is 5980. The sample size is determined using the SPSS program. The specifications entered include the population size (5980), expected frequency of BSE (18%), worst acceptable frequency (15%), and a 95% confidence interval. The calculated sample size is 530 female schoolteachers from all public schools in Irbid city. This sample size represents approximately 10% of the sampled population. Applying this fraction to the three directorates results in sample sizes of 350, 130, and 50 female schoolteachers from the first, second, and third directorates, respectively. The total sample size is 530 schoolteachers. The first school in each directorate is selected using simple random sampling. Systematic random sampling is then employed to select schoolteachers within each school. Every 10th teacher is chosen before moving on to the next school. The list of schools is arranged in descending order, from the one with the highest number of female teachers to the one with the lowest number of female teachers. Out of the 49 schools in the first directorate, 14 schools were visited to complete the required sample of 350 teachers. Similarly, nine schools were visited in the second directorate and five schools in the third directorate, out of a total of 28 and 9 schools, respectively. provides an overview of the population and sample selected.
Data collection
Permission was obtained from each directorate in Irbid to distribute the questionnaire among female schoolteachers. The questionnaires were distributed while the teachers were present in the classroom. Written informed consent, approved by the IRB, was obtained from all from each interviewed schoolteacher prior to their inclusion in the study. The questionnaires were handed out either at the beginning or end of the lesson and were systematically given to all classrooms in the school. Teachers were free to accept or refuse participation in the study. To ensure privacy and confidentiality, no names were written on the questionnaire.
Study tool
In this study, a self-administered questionnaire consisting of three sections was used.
First section
This section collects sociodemographic characteristics such as age, educational level, marital status, number of live children, breastfeeding practice, residency, employment period, age at birth of the last child, and duration of breastfeeding.
Second section
This section focuses on assessing knowledge and practice related to breast self-examination (BSE). The questionnaire includes targeted questions to evaluate participants’ understanding and reported behaviors, with correct answers provided in Table 1. Practice-specific items, such as ‘How often should BSE be performed?’ (Correct: monthly), ‘When should a woman with regular menstruation do BSE?’ (Correct: post-menstruation), and ‘What should be the position of the body when performing BSE?’ (Correct: standing or lying), alongside knowledge items like ‘Do you know what BSE is?’, are evaluated as ‘true’ or ‘false’ based on criteria from the Turkish National Family Planning Guideline (adapted for this study). Correct responses are scored as 1 and incorrect as 0, with the mean for the knowledge and practice domain converted to a fraction of one to reflect the proportion of correct answers (e.g. a 58.3% correct rate equals 0.583). Attitude items, such as those for Importance of BSE and Fear of Breast Cancer, are measured on a 5-point Likert scale (1 = Strongly Disagree to 5 = Strongly Agree). The self-reported nature of practice data, a common approach in knowledge, attitude, and practice (KAP) studies, may indicate intended rather than actual behavior, a limitation acknowledged for potential future validation with observational methods.
The questions and corresponding answers about knowledge of BSE.

Third section attitudes toward BSE
To assess attitudes toward BSE, a set of 19 statements was utilized. Participants were asked to rate these attitude items on a 5-point Likert scale, ranging from strongly disagree (1) to strongly agree (5). Factor scores were computed by summing the responses for each factor and dividing by the number of items within that factor. As a result, factor scores ranged from 1 to 5. The means were then divided into three categories: high, medium, and low, as follows the below figure:

Classification of means:
1–2.49: low, 2.5–3.49: medium, 3.5–5: high The internal consistency reliability coefficient was determined through a pre and posttest. Subsequently, the questionnaire was piloted with a group of 12 female schoolteachers. They were requested to provide their feedback and suggestions for improvement. Their responses and suggestions were then incorporated to refine the questionnaire.
Reliability (pilot study)
To ensure instrument reliability, a pilot study was conducted with 12 teachers, where test-retest reliability and Cronbach’s alpha were initially computed, yielding correlation coefficients ranging from 0.61 to 0.90. Following reviewer feedback, Cronbach’s alpha was recalculated using the entire sample (n = 518) to ensure robust internal consistency. The updated reliability coefficients, demonstrating acceptable to excellent internal consistency (α ≥ 0.72), are presented in Table 2.
Correlation coefficients on a sample of 12 teachers.
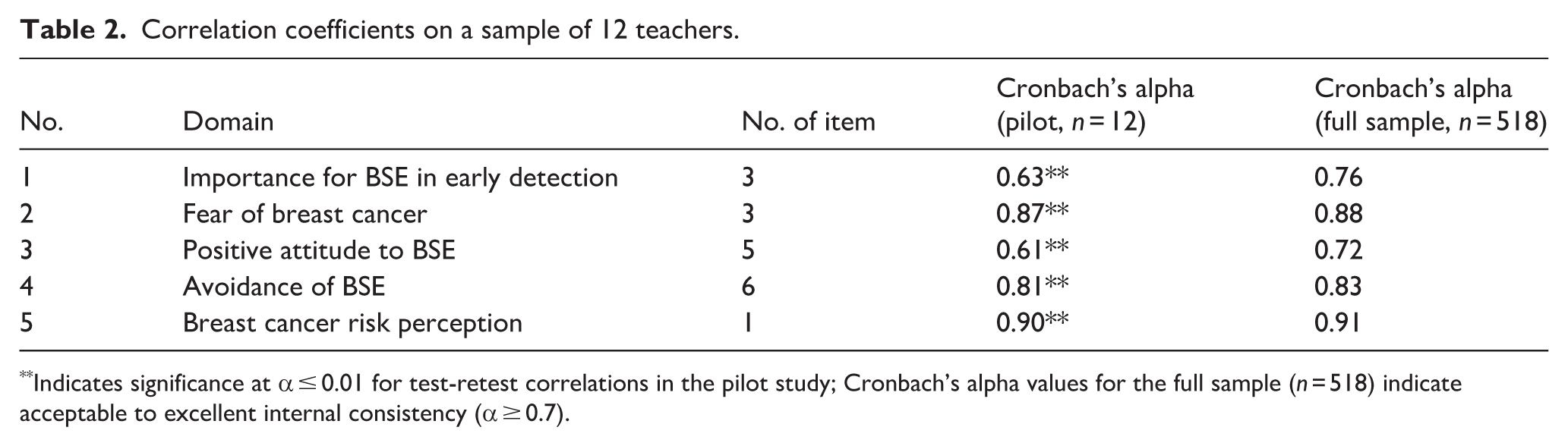
Indicates significance at α ≤ 0.01 for test-retest correlations in the pilot study; Cronbach’s alpha values for the full sample (n = 518) indicate acceptable to excellent internal consistency (α ≥ 0.7).
Statistical analysis
Statistical analyses were conducted to explore the relationships between socio-demographic factors and knowledge, practices, and attitudes toward breast self-examination (BSE). The independent variables included age (grouped as 23–25, 26–35, 36–40, and 41+ years), educational level (Diploma, Baccalaureate, Graduate Studies), marital status (Single, Married, Divorced), number of live children (0, 1–3, 4–5, 6–10), breastfeeding status (Yes, No), age at birth of first child (≤20, 21–25, 26–30, 31–35, 36+ years), and breastfeeding period (1–12, 13–24, 25–32, 33+ months). The dependent variables comprised the domains of knowledge and practices, importance of BSE for early detection, fear of breast cancer, positive attitudes toward BSE, avoidance of BSE, and breast cancer risk perception.
Analysis of Variance (ANOVA) was employed to assess differences in mean scores across multiple groups for age, educational level, marital status, and number of live children. Independent t-tests were used to compare means between breastfeeding groups (Yes vs No). All tests were conducted using SPSS software (version 26), with a significance level set at p < 0.05. Statistically significant p-values included:
Age: Knowledge and Practices (p = 0.01), Breast Cancer Risk Perception (p = 0.001)
Educational Level: Importance of BSE for Early Detection (p = 0.01), Breast Cancer Risk Perception (p = 0.001)
Marital Status: Importance of BSE for Early Detection (p = 0.001), Avoidance of BSE (p = 0.01)
Number of Children: Knowledge and Practices (p = 0.01), Positive Attitudes toward BSE (p = 0.001)
Breastfeeding: Knowledge and Practices (p = 0.001), Fear of Breast Cancer (p = 0.001), Avoidance of BSE (p = 0.001)
Age at Birth of First Child: Knowledge and Practices (p = 0.001), Fear of Breast Cancer (p = 0.001), Breast Cancer Risk Perception (p = 0.001)
Breastfeeding Period: Importance of BSE for Early Detection (p = 0.001), Fear of Breast Cancer (p = 0.001), Positive Attitudes toward BSE (p = 0.02), Breast Cancer Risk Perception (p = 0.001). These results are detailed in Tables 6–12 in the Results section.
Results
Demographic variables
Table 3 presents a summary of the socio-demographic characteristics of the study population. The mean age of the female participants was 32.77 years (standard deviation: 7.35), with nearly half (approximately 50%) of the women aged between 26 and 35 years. In terms of marital status, 73.2% of the participants were married, 20.7% were single, 3.7% were divorced, and 2.5% were widowed. Furthermore, approximately 64.1% of the women had attained a Baccalaureate degree.
Demographics characteristics of the sample.

Regarding residential area, 60.4% of the female schoolteachers resided in urban environments, while 39.6% lived in rural areas. The distribution of employment duration indicated that 54.6% had between 1 and 5 years of work experience, whereas only 5.6% reported having between 16 and 20 years of experience.
Concerning the age at first delivery, 44.6% of the participants had their first child between the ages of 21 and 25, whereas a mere 0.6% were 36 years or older at the time of their first delivery. Additionally, the majority (46.5%) of participants reported having between 1 and 3 living children, and approximately 62.7% selected breastfeeding as their method of infant feeding.
The study aimed to assess general knowledge and practices regarding breast self-examination (BSE; Table 4). The findings revealed that 58.3% of participants were aware of BSE. Additionally, 69.5% of the sample believed that early detection of cancers, in general, is possible, with 83% specifically recognizing the importance of early detection for breast cancer. Only 26.4% of participants provided the correct response regarding BSE for both males and females. Furthermore, approximately 66.8% of participants were not aware of the recommended age to commence BSE. However, 71.2% correctly indicated that BSE should be performed on a monthly basis. The results also indicated that 62.4% of participants did not perceive any correlation between regular and irregular menstruation and BSE. Conversely, 70.5% of the sample accurately responded to when a woman with regular menstruation should conduct BSE. Finally, 26.8% of participants correctly identified the appropriate body position for performing BSE. Table 4 provides a visual representation of the frequency and percentage of correct responses.
Knowledge and practices of breast self-examination.

Attitudes toward breast self-examination
Descriptive statistics were employed to calculate the mean and standard deviation of attitudes toward breast self-examination (Table 5).
Mean score of attitudes toward breast self-examination.

Mean score of knowledge, practices and attitudes toward BSE versus

The data demonstrates a robust positive attitude toward breast self-examination (BSE), as evidenced by a remarkably high mean score of 3.9 in the ‘Importance of BSE for Early Detection’ domain. Respondents consistently concur that BSE is an effective method of identifying lumps and enhancing the likelihood of survival. Notably, there is a considerable level of apprehension regarding breast cancer, as indicated by a mean score of 3.69, underscoring the significant concern felt by individuals. However, this fear does not translate into a high inclination to avoid BSE. Despite encountering moderate levels of discomfort or experiencing a lack of knowledge regarding BSE (e.g. a mean score of 2.79 for finding BSE disturbing), the tendency to avoid BSE remains low, with a mean score of 2.49. Moreover, the respondents display a heightened perception of the risk of developing breast cancer, as reflected by a mean score of 3.97, indicating their awareness of the potential threat and reinforcing the crucial role of regularly engaging in BSE.
The relationship between socio-demographic factors and knowledge, practices and attitudes toward BSE
Personal attributes comprise various factors, including age, educational attainment, marital status, number of live children, breastfeeding practices, residency, employment history, age at first childbirth, and duration of breastfeeding.
Age
Analysis of Variance (ANOVA) Applied to Age and its Impact on Knowledge, Practices, and Attitudes Toward BSE. The mean values of knowledge and practices are calculated for each unit of age.
Both older and younger age groups demonstrate a higher level of knowledge regarding BSE, with a statistically significant difference observed. Regarding attitudes, there is a significant difference among different age groups in relation to breast cancer risk perception, favoring older schoolteachers.
Educational level
There is no significant disparity in the understanding and application of breast self-examination (BSE) among individuals with varying levels of education. Similarly, attitudes toward BSE do not demonstrate substantial variation, with the exception of attitudes concerning the importance of BSE in the timely detection of breast cancer and perceptions of breast cancer risk. These particular attitudes reveal notable discrepancies based on educational attainment (Table 7).
Mean score of knowledge, practices and attitudes toward BSE versus educational level.

There are no significant results regarding the relationship between marital status and knowledge and practices of BSE. This suggests that the variation among marital statuses is not significant. Marital status does not have an effect on knowledge and practices of BSE. However, there are significant results regarding the relationship between the first and fourth items of attitudes and marital status. Single women exhibit higher attitudes than others regarding the importance of BSE in the early detection of breast cancer (Table 8).
Mean score of knowledge, practices and attitudes toward BSE versus Marital status.

Number of life children
The relationship between the number of live children and knowledge of BSE was assessed, as depicted in Table 9. The findings indicate a statistically significant relationship between the number of live children and knowledge of BSE. Moreover, the results did not reveal statistical significance between the number of live children and all attitude measures, except for positive attitudes toward BSE, which demonstrated a statistically significant association. Schoolteachers with a higher number of live children exhibited more positive attitudes.
Mean score of knowledge, practices and attitudes toward BSE versus life children.

Breastfeeding
T-tests were utilized to examine the relationship between the variable of breast-feeding and the knowledge and practice domain of breast self-examination (BSE). The findings indicate a statistically significant difference between breast-feeding and the knowledge and practice domain of BSE. Specifically, schoolteachers who breastfeed their babies demonstrate a higher level of knowledge regarding BSE compared to those who do not breastfeed. Additionally, significant associations were observed between attitudes (specifically, fear of breast cancer and avoidance of BSE) and breastfeeding. Individuals who do not breastfeed their babies exhibit greater levels of fear of breast cancer and avoidance of BSE (Table 10).
Mean score of knowledge, practices and attitudes toward BSE versus breastfeeding.

Age at birth of first child
There are significant findings regarding the relationship between the age at which one gives birth to their first child and their knowledge and practices of breast self-examination (BSE). Specifically, individuals in the extreme age groups (20 years and younger, and 36 years and older) demonstrate higher levels of knowledge and engagement in BSE compared to those in the middle age groups. Additionally, there are significant differences in attitudes toward BSE between individuals based on the age at which they had their first child. Notably, schoolteachers who gave birth to their first child in their twenties exhibit higher levels of fear of breast cancer and perceptions of breast cancer risk compared to other age groups (Table 11).
Mean score of knowledge, practices and attitudes toward BSE versus Age at birth of first child.

There was no statistically significant relationship between knowledge, practices of Breast Self-Examination (BSE), and the duration of breastfeeding. This implies that the duration of breastfeeding does not have an impact on the knowledge and practices of BSE. However, there were statistically significant relationships between the duration of breastfeeding and all items related to attitudes, except for the item assessing positive attitudes toward BSE and avoidance of BSE. In other words, the more a woman breastfeeds her baby, the more likely she is to develop a positive attitude toward BSE (Table 12).
Mean score of knowledge, practices and attitudes toward BSE versus Breastfeeding period.

Discussion
This study was designed to evaluate the knowledge, practices, and attitudes of female schoolteachers in Irbid, North Jordan, regarding breast self-examination (BSE) and breast cancer awareness. The results provide important insights into how educators’ knowledge and behaviors may influence their student and parent populations, underscoring the potential of this demographic to act as agents of health promotion within their communities.
Knowledge and awareness of breast self-examination
The findings of this study indicate that approximately 50% of the respondents possessed some knowledge of BSE; however, this knowledge was largely superficial and lacked depth. Numerous areas related to general knowledge of breast cancer, including early detection, management options, and the steps involved in performing BSE, demonstrated low knowledge scores of less than 70%. This observation aligns with the results reported by Sarker et al., 13 which highlighted poor baseline awareness among female university students in Bangladesh. Notably, significant improvements were observed in participants’ understanding of breast cancer symptoms, which increased from 2.99 ± 1.05 to 6.35 ± 1.15 (p < 0.001); risk factors from 3.35 ± 1.19 to 7.56 ± 1.04 (p < 0.001); and the process of BSE from 1.57 ± 1.86 to 3.94 ± 0.93 (p < 0.001), after the educational intervention. These findings emphasize that there is a dire need for organized educational programs so that these knowledge gaps are appropriately filled.
Despite the relatively low depth of knowledge, our study revealed that 96.5% of participants reported some awareness of BSE, and 69.8% were aware of the correct timing for performing BSE. However, this knowledge did not translate into practice, as only 31.4% of participants reported regularly performing BSE. This discrepancy between knowledge and practice is corroborated by the findings of Šašková and Pavlišta, 14 who noted that although 58.3% of participants were aware of BSE, only 10.9% practiced it on a monthly basis. Similarly, Alduraibi 15 found that despite having a general understanding of BSE deemed sufficient, the frequency of its practice remained low among female teachers in Saudi Arabia.
Attitudes toward BSE
The findings of this study indicate that, in general, the participants exhibited positive attitudes toward Breast Self-Examination (BSE) and regarded it as an important means of early breast cancer detection. Conversely, misconceptions prevailed, with the majority of participants believing that regular or irregular menstruation is unrelated to the necessity of BSE. This myth underscores the need for targeted educational programs regarding the appropriate timing and frequency of BSE performance. According to Powe and Finnie, 16 greater knowledge about a particular disease is typically associated with more proactive health behaviors, which aligns with our findings.
Worry and fear of breast cancer emerged as significant motivators for performing BSE, as evidenced by their high scores among attitude-related items. This observation is corroborated by Hay et al., who emphasized the correlation between worry and health-related behaviors. However, it contrasts with their assertion that individuals generally do not exhibit significant concern regarding cancer. 17 Similarly, Loescher 18 found that women ‘sometimes’ worried about developing breast cancer, suggesting that worry alone may not consistently drive preventive behaviors. In our study, the low score for avoidance of BSE indicates that, while fear exists, it acts as a motivator rather than a deterrent, thereby serving as a potentially effective lever for promoting engagement with BSE.
Demographic factors influencing knowledge and practice
Our study demonstrated a significant relationship between age and knowledge and practice of BSE, with increased engagement observed among older participants. This finding is consistent with the research conducted by Janda et al., 19 which reported that older women were more likely to engage in BSE. However, conflicting evidence exists within the literature, as Jarvandi et al. 20 noted higher BSE engagement among younger women in certain contexts. These discrepancies suggest that cultural, educational, and regional factors may significantly influence BSE behaviors across various populations.
Concerning marital status, our study revealed that the practice of BSE was more prevalent among married women compared to their single counterparts, aligning with the findings of Jarvandi et al. 20 No statistically significant differences in knowledge or attitudes were observed based on marital status. This suggests that social support systems inherent in marriage may contribute to healthier behaviors. Furthermore, while higher education levels are often associated with improved health literacy, our findings did not reveal significant differences in knowledge about BSE or its practice in relation to the participants’ educational levels, contradicting studies by Sapountzi-Krepia et al. 21 and Alduraibi. 15
Furthermore, while higher levels of education are often correlated with improved health literacy, our findings did not reveal significant differences in knowledge about BSE or its practice relative to participants’ educational levels, thereby contradicting studies by Sapountzi-Krepia et al. 21 and Alduraibi. 15
Impact of educational interventions
The key finding of this study was the effectiveness of educational interventions in improving knowledge and practice of breast self-examination (BSE). Participants who underwent educational sessions demonstrated significant improvements in both understanding and engagement with the practice. For instance, prior to the intervention, 81.5% of participants did not perform BSE regularly; this figure decreased markedly following the educational intervention. Akarsu and Andsoy 22 reported similar results, indicating that training significantly enhanced knowledge concerning breast cancer risk factors and screening practices among Turkish women.
However, the study’s weaknesses must be considered alongside its strengths as a tool for awareness and early detection. Šašková and Pavlišta 14 noted that routine BSE does not significantly reduce mortality from breast cancer and may result in increased diagnostic procedures, including unnecessary biopsies. Therefore, educational programs should provide balanced information regarding the strengths and limitations of BSE, while also emphasizing complementary screening methods such as clinical breast examination (CBE) and mammography.
Greater implications for breast cancer awareness
This study reaffirms the evidence supporting targeted community-based awareness and education initiatives regarding breast cancer screening practices. Female teachers serve as social trendsetters among influential figures within their community, thereby presenting significant potential for disseminating health awareness information. Integrating breast cancer education into school-based curricula could have a considerable impact on improving knowledge and promoting better preventative behaviors among schoolchildren and their family contacts.
In this context, innovative approaches—such as the use of social media campaigns and other digital resources—may provide additional means of enhancing engagement and access. Tomic et al. 23 discussed how a digital approach can be utilized to improve knowledge, attitudes, and practices related to breast cancer screening among female medical students, suggesting that this strategy could be extended to the broader population.
This study possesses several notable strengths. It specifically examines female schoolteachers, an underrepresented demographic whose role as community educators significantly enhances the potential impact of breast self-examination (BSE) interventions in Jordan. The research employed a representative sample drawn from multiple educational directorates, and the comprehensive questionnaire utilized effectively assessed participants’ knowledge, practices, and attitudes, thereby providing a holistic understanding of BSE behaviors. The reliability of the instrument was confirmed, and ethical standards, including informed consent and anonymity, were rigorously maintained.
Nevertheless, certain limitations warrant consideration. The data were self-reported, which may have introduced bias or led to an overestimation of BSE practices. The pilot study was conducted with a limited sample size, and some of the practice data were hypothetical, thereby constraining the interpretation of findings until complete data collection is achieved. Furthermore, cultural barriers, such as discomfort in discussing breast health, were not thoroughly investigated and may have impacted participants’ practices. Lastly, the focus on schoolteachers within a single city restricts the generalizability of the findings to other populations, although the results provide a foundational basis for broader interventions.
Conclusion
This study has identified critical gaps in knowledge and practice related to BSE among female schoolteachers in Irbid, North Jordan. The high level of awareness regarding BSE is not reflected in consistent practice; hence, comprehensive educational interventions are necessary. The long-term effects of such interventions warrant further investigation, and new effective methods for raising awareness about breast cancer and its early detection should be explored. Therefore, equipping educators with the knowledge and resources to become health advocates is essential for reducing the breast cancer burden and improving health outcomes in various societal settings
Footnotes
Acknowledgements
We would like to acknowledge the participants in our study for their time, effort and insights.
Ethical considerations
The study was approved by the Institutional Review Board research number 44-2009 of Jordan University of Science and Technology (JUST), Jordan.
Author contributions
MH and AQ conceived and designed the study. AQ collected the survey data from the participants. MH and AQ performed the data analysis together. AQ prepared the first draft of the manuscript, and MH critically reviewed and strengthened it. Both authors contributed to subsequent drafts of the manuscript and approved the final version for submission.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
All data in this work are obtainable from the corresponding author upon reasonable request.