
Abstract
Background:
The COVID-19 pandemic has emphasized the critical role of public knowledge, attitudes, and practices (KAP) in disease containment. Understanding these aspects can guide health promotion initiatives and policy decisions.
Design and methods:
This cross-sectional study examined the KAP concerning COVID-19 prevention in Vietnam. Participants’ sociodemographic data, along with KAP toward COVID-19, were collected in a survey utilizing a standardized questionnaire. Uni- and multivariable logistic regression were used to identify factors associated with poor level of KAP.
Results:
Of 335 participants, 97 (28.9%) had poor knowledge, 52 (15.5%) poor attitude, and 48 (14.3%) poor practices. Older age (OR = 2.23; p = 0.024), minority non-Kinh ethnicity (OR = 3.05; p = 0.03), education below high school (OR = 8.80; p < 0.001), limited social media access (OR = 2.86; p = 0.002), and limited mobile phone usage (OR = 3.08; p = 0.001) increased poor knowledge risks. Non-Kinh ethnicity (OR = 5.00; p = 0.005) and lower education (OR = 14.79; p < 0.001) were linked to poor attitude. Older age (OR = 2.26; p = 0.035), lower education (OR = 5.74; p = 0.003), and poor knowledge (OR = 3.33; p = 0.005) were associated with poor practices.
Conclusions:
Elderly individuals, those with low education, and limited media access had elevated risks of poor KAP. Emphasizing public health media and targeted education, especially for underserved groups, is vital for effective epidemic management and future strategy planning.
Keywords
Introduction
The new coronavirus SARS-CoV-2 that triggered the COVID-19 pandemic, with its first case emerging in December 2019, has had an extensive impact on people’s health and well-being across the globe. 1 The World Health Organization (WHO) proclaimed COVID-19 a global pandemic on March 11, 2020, and since then, the virus has spread rapidly, affecting millions of people and resulting in millions of deaths. As of March 2023, the global tally shows more than 452 million confirmed cases of COVID-19 worldwide and over 6.1 million deaths. 2 Similar to numerous other nations, Vietnam, has faced significant impact from the COVID-19 pandemic. The initial COVID-19 case in Vietnam was reported in January 2020, and since then, the virus has continued to spread across the country, affecting people from all walks of life. As of March 2023, Vietnam has reported over 11 million confirmed COVID-19 cases and over 43,000 deaths.3,4
COVID-19 primarily spreads through respiratory droplets released during talking, coughing, or sneezing by an infected person. These droplets can enter people’s lungs through their mouths or noses. The virus can spread through touching a virus-infected surface and via fomites. The Vietnamese government has implemented several measures to control the spread of the virus, such as social distancing, wearing masks, and limiting mass gatherings. 5 These efforts have proven effective in reducing the number of COVID-19 cases in the country. However, the success of these measures relies heavily on the knowledge, attitude, and preventive practices of individuals. Insights into citizens’ understanding, attitudes, and practices regarding COVID-19 prevention measures have been gained from prior research in the urban area, which was used to implement changes in preventive measures and policies to better fit with population characteristics.6,7 However, there is little to no study that considers these problems in low socioeconomic regions such as the rural or suburban areas in Vietnam.8 –10
In addition, rural and suburban areas in Vietnam are particularly vulnerable to the spread of COVID-19 due to multiple factors including limited access to healthcare facilities, lower levels of health literacy among residents, low socioeconomic status, high rate of treatment non-adherence, high rate of practicing unconventional medicine due to low health literacy. Therefore, this research paper aims to examine the COVID-19 knowledge, attitude, and preventive measures among outpatients at a rural hospital in Vietnam, as well as the associated factors that may impact these behaviors. Knowing these factors will help in the development of planned public health initiatives and approaches to improve adherence to preventive measures, promote early identification of potential cases, and, in the end, reduce the spread of the virus in rural areas.
Significance for public health
This research spotlights gaps in COVID-19 knowledge and preventive behaviors among marginalized rural populations in Vietnam. The findings demonstrate the need to target communication and outreach to vulnerable groups including older adults, those with limited education, and ethnic minorities to improve adherence to preventive guidance. Specific health messaging via appropriate media channels should be complemented by addressing structural barriers around health literacy and service access. The analysis makes clear that a multifaceted approach is required spanning infrastructure, technology, cultural competency, and community partnership-building to enhance epidemic preparedness and response. Moreover, the disparities observed likely pervade management of other chronic diseases, emphasizing the opportunity to advance health equity through carefully designed promotion programs. This study provides an evidence base for policymakers to allocate resources and target interventions toward supporting at-risk groups. As a snapshot of the current situation, ongoing monitoring of knowledge and practices is warranted to continuously inform and enhance Vietnam’s public health strategy against COVID-19 and beyond.
Methods
Study design
This was a cross-sectional study and recruited outpatients who came for the examination from the Endocrinology Hospital in Nghe An Province, Vietnam. The study utilized a pre-designed questionnaire in line with the Checklist for Reporting Of Survey Studies (CROSS) to interview patients about their knowledge, attitudes, and practices toward COVID-19 (Supplemental material). The questionnaire includes sociodemographic, sources of information, and KAP toward COVID-19.
In order to be included in the study, participants had to meet specific criteria. The inclusion criteria comprised individuals who were 18 years old or older, had overall normal health, and possessed the ability to communicate fluently and directly. Individuals without fluent Kinh language were interviewed with the help of a certified interpreter. Furthermore, participants were required to voluntarily and willingly consent to participate in the research. Conversely, certain individuals were excluded from the study, such as those who were behaviorally incompetent or unable to engage in the entire research process.
Sample size
The sample size was estimated using the proportion formula
Using the same formula, based on the proportions of knowledge, attitude, and practice toward COVID-19 in the study by Huynh et al. 5 good knowledge rate was 79.2%, good attitude was 70.7%, and good practice was 76.1%, the respective calculated sample sizes were 254, 319, and 280.
Therefore, to ensure adequate statistical power, a minimum sample size of 319 participants was determined as necessary for the study. Estimating a 5% dropout/refusal rate, the required sample size is 335. The study successfully recruited 335 participants.
Data collection
The study used a convenience sampling method. The outpatient clinic where sampling was conducted operates from Monday to Friday. As such, sampling was only carried out on weekdays. The patients targeted have endocrine disorders and routinely come in for morning blood work before eating. Consequently, interviews could only feasibly be done in the morning hours.
The duration of hospital visits for individual outpatients is unpredictable. Participants were therefore interviewed one-on-one as they became available. Due to COVID-19 precautions limiting contact, only two interviewers were permitted. With interviews estimated to take 20 min each, the interviewers had the capacity for about 30 interviews in the 5-hour morning clinic duration, out of the 400–500 daily patient visits. The final sample of 30 was thus selected randomly from each morning’s patient pool.
Questionnaire development
5K message is measures to prevent COVID-19 issued by the Vietnam government. 5K massage includes mask, distance, disinfection, no gatherings, and health declarations.
Minority non-Kinh ethnicities are ethnic groups other than Kinh ethnic group.
The questionnaire assessing knowledge (35 questions) was answered on correct, incorrect, or unknown. A right answer was given a score of 1, while a wrong or unknown answer received a score of 0, with total knowledge scores varying from 0 to 35. Utilizing Bloom’s cut-off point as a guide, participants’ overall knowledge was classified into three categories: a score of 28–35 points (80%–100%) was considered good, a score ranging from 21 to 27.9 points (60%–79%) was deemed moderate, and a score below 21 points (less than60%) was labeled as poor.
The attitude assessment questionnaire (8 questions) was responded to using agree, disagree, or not sure options. A correct answer was assigned 1 point and an incorrect/not sure answer was assigned 0 point. The overall attitude score ranged from 0 to 8. Based on Bloom’s cut-off point, participants’ attitudes were categorized as follows: good if the score fell within 80%–100% (6.4–8 points), moderate if the score ranged from 60 to 79% (4.8–6.3 points), and poor if the score was below 60% (<4.8 points).
The practice assessment questionnaire (8 questions) was answered to using yes or no options. A correct answer was assigned 1 point and an incorrect answer received 0 point. The total practice score ranged from 0 to 8. Based on Bloom’s cut-off point, participants’ overall practice was categorized as follow: good if the score fell within 80%–100% (6.4–8 points), moderate if the score ranged from 60% to 79% (4.8–6.3 points), and poor if the score was below n 60% (<4.8 points).
Statistical analysis
The data was cleaned during the process of checking the questionnaires. Data entry was done twice by two different people using SPSS 22.0 software. Descriptive statistics were employed for data analysis, and, the results were presented in terms of frequency, percentage, and mean. Univariable and multivariable logistic regression analyses were carried out to discover characteristics related with low KAP. Only variables in univariable with p < 0.2 in the univariable logistic regression analysis were entered into multivariable logistic regression analysis. The strength association between risk factors and poor KAP were presented by OR and CI 95%, p < 0.05 was considered statistically significant.
Ethics statement
This study was approved by the Ethical Committee of Hanoi Medical University and was permitted by the Deputy of Nghe An Endocrinology Hospital; it was registered under the codes 866/QD-DHYHN. Additionally, informed consent was obtained from every participant before enrolling. The participants responded to the questionnaire anonymously.
Results
The characteristics of study subjects
A total of 335 participants, 79 male (23.6%), and 256 female (76.4%), age range from 18 to 85 with a mean age of 49.1 ± 14.3. Participants ≥60 years old accounted for 25.4% of the participants, 79.1% of participants were from rural areas, 91% were Kinh ethnic, 9% were not Kinh ethnic (ethnic minority group), 37.3% were junior high school degree, 14.3% were university and postgraduate degrees, 38.5% were housewife, 30% were business, 93.1% were married (Table 1).
Sociodemographic characteristics of study subjects (n = 335).

Sources of information about COVID-19 for the participants
The most common sources of information were TV/radio 95.8% and loudspeaker 82.7%. Social media as a source of information, as well as mobile, health professionals, and friends were 64.5%, 64.5%, 62.1%, and 60.6%, respectively (Figure 1).
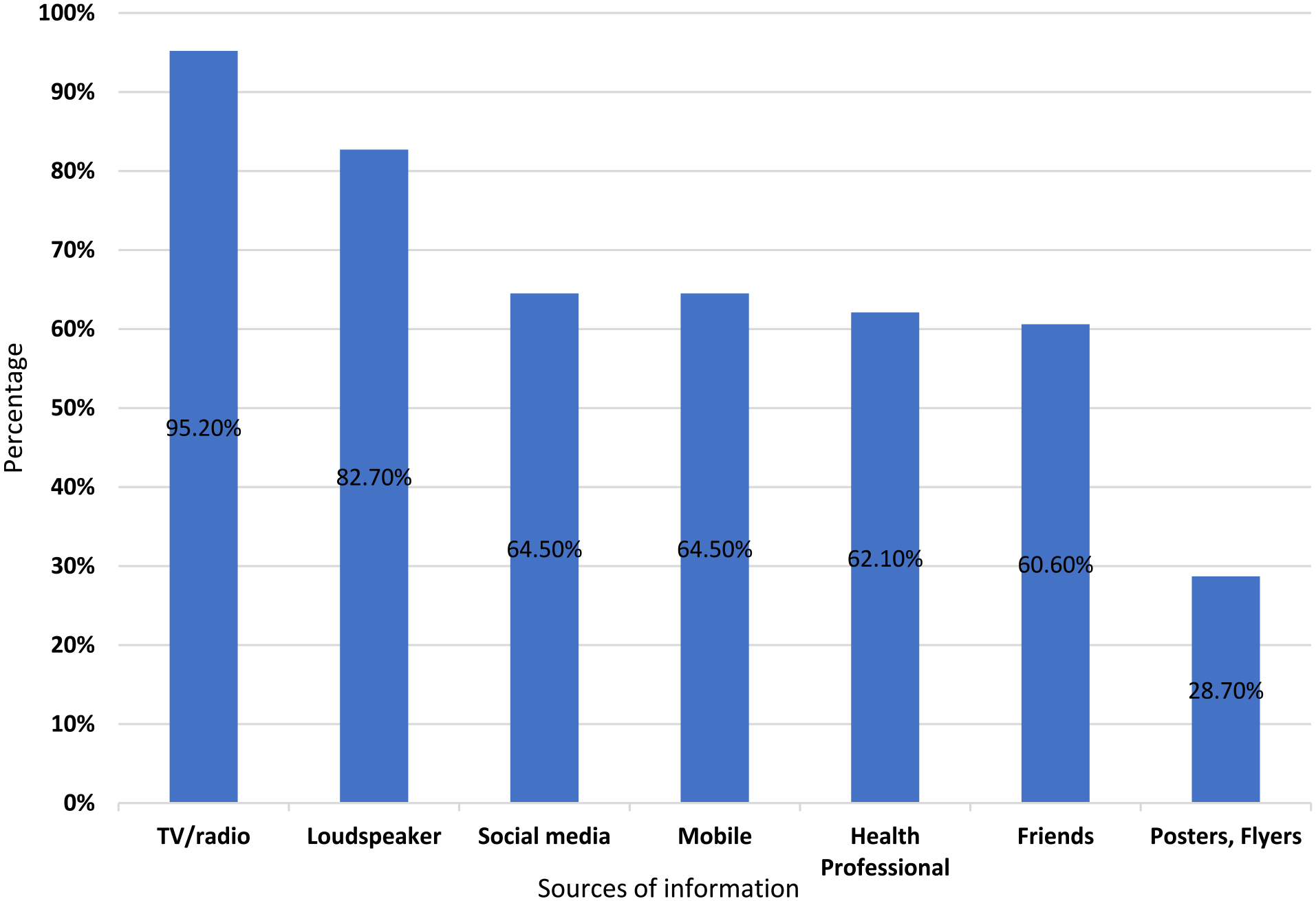
Sources of information about COVID-19.
Knowledge status
The overall knowledge of the participants about COVID-19 it was observed that 97 (28.9%) had poor knowledge, while 170 (50.7%) had good knowledge (Figure 2). A high ratio of correct knowledge was observed in aspects such as the transmission of COVID-19 through close contact (92.5%) and respiratory droplets (91.3%), and the ability of the virus to cause death (95.8%). Also, the need to wear a mask when going out was known by 96.4% of the participants. However, some misconceptions or areas of lesser knowledge were also noted. Only 48.1% of participants were aware that contacting a contaminated surface, then contacting one’s lips, nose, or eyes, could spread the disease. Understanding the full range of COVID-19 symptoms also varied, with high awareness of fever (85.1%) and cough (84.5%) but reduced recognition of loss of taste and smell (23.6%) and headache (22.7%) as possible symptoms. Knowledge related to the “5K message,” a public health campaign related to COVID-19, was variable. While 77% of participants were aware that it included mask-wearing, only 60.6% knew it involved health declarations. Furthermore, participants showed a substantial understanding of the importance of personal sanitation practices like hand washing with soap or sanitizer for at least 20 s (90.1%) and frequent hand washing (88.1%). Yet, only 61.5% recognized the importance of properly disposing of used masks into a lidded wastebasket and subsequent hand sanitization (Table 2).

Level of patient’s overall knowledge about Covid-19.
Patient’s knowledge toward COVID-19 prevention.

In this study, factors were associated with independently increased risks with poor knowledge about COVID-19 include age ≥60 (OR = 2.23; CI: 1.11–4.48; p = 0.024), those who were not of Kinh ethnicity (OR = 3.05; CI: 1.11–8.41; p = 0.03), and those who had limited access to social media (OR = 2.86; 95% CI: 1.47–5.56; p = 0.002) or to mobile phones (OR = 3.08; CI: 1.59–5.96; p = 0.001). The most prominent risk factor is an education level below high school (OR = 8.80; CI: 4.16–18.64; p < 0.001) (Table 3).
Factors associated with patient’s poor knowledge about Covid-19 in univariable and multivariable analysis.
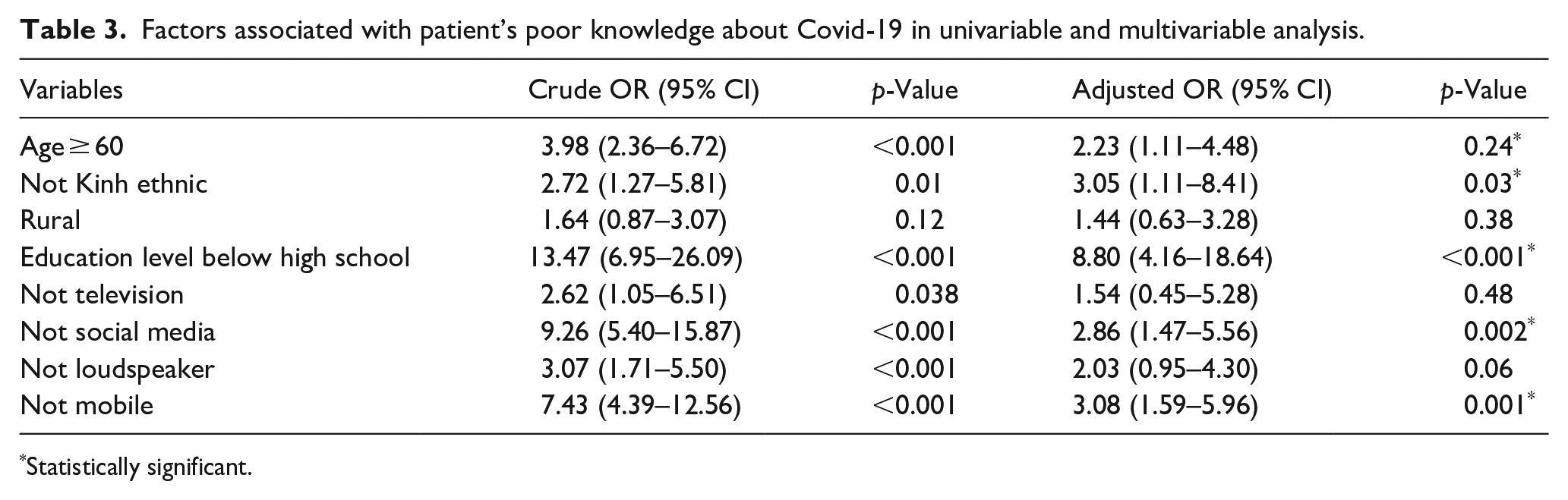
Statistically significant.
Attitude status
The participants’ general attitude toward COVID-19 revealed 52 (15.5%) were poor attitude, and 268 (80%) were good attitude (Figure 3). Overwhelmingly, participants agreed on the severity of COVID-19(92.2%). The majority of those interviewed also endorsed the effectiveness of the Ministry of Health’s preventive measures (90.7%). When it came to specific preventive measures, participants showed a strong understanding and agreement. Most notably, 91% agreed on the necessity of wearing a mask when going out, and 89.5% agreed on the importance of hand hygiene, specifically washing hands with soap or sanitizer. Furthermore, 84.8% agreed on the importance of limiting visits to crowded places or areas with high infection rates. Regarding behaviors at healthcare facilities, 82.7% of participants agreed that providing complete and accurate medical declarations was essential for COVID-19 prevention. Additionally, 85.4% of the participants recognized the need to maintain distancing while waiting for medical examinations. Lastly, in terms of vaccination, 78.8% of the participants were of agreement that getting the COVID-19 vaccine was essential (Table 4).

Level of patient’s overall attitude about Covid-19.
Patient’s attitude toward COVID-19 prevention.

When multivariable analysis revealed factors associated with increased risks of poor attitudes toward COVID-19 such as those were not of the Kinh ethnicity (OR = 5.00; CI: 1.62–15.39; p = 0.005), individuals with an education level below high school (OR = 14.79; CI: 3.25–67.15; p < 0.001) and poor knowledge about COVID-19 (OR = 8.16; CI: 3.48–19.08; p < 0.001). Age ≥ 65, on the other hand, did not significantly influence the attitude (OR = 1.35; CI: 0.61–2.98; p = 0.45) (Table 5).
Factors associated with patient’s poor attitude about Covid-19 in univariable and multivariable analysis.

Statistically significant.
Practice
The participants’ general behavior toward COVID-19 revealed that 48 (14.3%) were poor attitude, and 216 (64.5%) were good attitude (Figure 4). All participants (100%) reported undergoing health declarations and temperature measurements before entering the hospital and wearing a mask every time when they went outside. The use of medical masks was reported with 71.6% proper use and the remaining 28.4% incorrect use. Similarly, 83% of the participants sat in the correct position during medical examinations, with 17% failing to adhere to this preventive measure. Frequent handwashing with soap or hand sanitizer was 75.5% of the respondents, while the remaining 24.5% did not consistently adhere to this hygiene practice. Similarly, 71.9% of respondents followed the practice of covering their nose and mouth when coughing or sniffling with their elbow or a towel, indicating adherence to respiratory hygiene. The practice of avoiding crowded places takes up a high proportion of the respondents with 93.1%. Finally, frequent cleaning of objects that are frequently touched was reported by 80.3% of respondents (Table 6).

Level of patient’s overall practice about Covid-19.
Patient’s practice toward COVID-19 prevention.

In this study, we found independent predictors of inadequate practices toward COVID-19 prevention including age ≥ 60 (OR = 2.26; CI: 1.06–4.85; p = 0.035), education level below high school OR = 5.74; CI: 1.83–17.99; p = 0.003), poor knowledge about COVID-19 (OR = 3.33; CI: 1.44–7.70; p = 0.005) and poor attitudes toward COVID-19 (OR = 2.42; CI: 1.06–5.50; p = 0.035). However, not being of Kinh ethnicity didn’t significantly affect poor practice (OR = 1.58; 95% CI: 0.53–4.65; p = 0.40) (Table 7).
Factors associated with patient’s poor practice about Covid-19 in univariable and multivariable analysis.

Statistically significant.
Discussion
The significance of conducting this study in a rural hospital in Vietnam cannot be overstated. Given the unique demographic(age 49.1 ± 14,3 with 25.4% age ≥ 60 years; 23.6% were male and 76.4% were) female), cultural, and socio-economic characteristics (37.3% were junior high school degree, 14.3% were university and postgraduate degrees, 38.5% were housewife, 30% were business, 93.1% were married) of rural communities.8,9,12 Rural communities in Vietnam are typically characterized by lower literacy levels and reduced access to reliable health information, which could potentially influence their knowledge about, attitudes toward, and practices in preventing COVID-19.11,12 Our study engaged multivariable analysis using adjusted odds ratios to eliminate potential confounding factors. This has allowed for a deeper examination of the disparities in understandings, beliefs, and habits toward COVID-19 prevention, to have public health interventions and effective strategies to increase knowledge and improve attitudes and practices, thereby contributing to the broader global efforts in controlling and managing the COVID-19 pandemic. The participant cohort of our study was varied, encompassing a range of ages (aged 18–90 years), educational backgrounds (the majority of participants answered that they junior high school or above), genders, and geographical locations (range urban to rural). This ensured a comprehensive evaluation of different population segments, consistent with other comparable studies.5,6,8,10,13 The limited access to media among this group could hinder their ability to gather information effectively, combined with reduced interaction with healthcare workers, this might result in their inadequate knowledge about COVID-19. 6 This aligns with earlier studies by Nguyen et al., a study on 2769 adult patients also showed that age ≥60 had poor understandings about COVID-19- with a lower score of 13.09 ± 1.55 than other age groups.6,14,15 In exploring the knowledge factor, we found an education level below high school to be an significant contributor to poor knowledge about COVID-19 with education level below high school has poor knowledge about COVID-19 with OR = 8.80 (95% CI: 4.16–18.64; p < 0.001) this aligns with Bazaid et al., researchers reported similar findings find individuals with lower educational attainment will rarely answer correctly related knowledge about COVID-19 (OR = 0.606, p = 0.001, underlining the connection understanding of the disease). 13 And similar to the Feleke et al. study that who have less educational status was people with less education have low knowledge (OR = 3,04, 95% CI: 1.43–6.46). 16
We found that the poor knowledge people had limited access to social media with OR = 2.86 (95% CI: 1.47–5.56, p = 0.002) or limited access to mobile phones OR = 3.08 (95% CI: 1.59–5.96, p = 0.001) this is also similar to the study of Nguyen et al. 6 and the study conducted by Van Nhu et al. 17
In our study, we found a significant difference in knowledge levels between Kinh people and individuals of other ethnicities. Those of minority non-Kinh ethnicities displayed poorer knowledge, with an odds ratio of 3.05 (95% CI: 1.11–8.41, p = 0.03). This aligns with Minh An et al. who reported similar findings that Kinh ethnicity (84.3%) had greater knowledge than minority non-Kinh groups (72.0%) However, these findings should be regarded with caution due to our limited sample size, particularly concerning the representation of the Kinh ethnic group. 18
Interestingly, most participants in our study correctly identified COVID-19 transmission methods and symptoms, indicating a higher awareness level compared to prior studies. This might reflect the efficacy of public health interventions in disseminating necessary information to the populace. The findings underscore the necessity for targeted interventions to improve COVID-19 knowledge among these vulnerable groups.
Regarding attitude toward COVID-19, 64.4% (n = 216) of participants had good attitude, this result is lower than that in the study of Ho et al. (78.2%). 19 Besides, we discovered a considerable influence of ethnicity and education. Particularly, individuals from the ethnic group showed different beliefs toward COVID-19 prevention. In this study, not Kinh people had more negative sentiments toward COVID-19 prevention in comparison to other groups (AOR = 5.00; 95% CI: 1.62–15.39; p = 0.005). The reason for the differences may be attributed to the limited sample size and the non-representation of the ethnic majority in our study, which might limit the generalizability of the findings to this specific group. In addition, the high poverty rate lies among minority non-Kinh ethnicities in Vietnam, as they are isolated by society due to cultural and language barriers, limited access to social media, and COVID-19 prevention program. 20 Therefore, these factors may prevent ethnic minority patient groups from accessing the COVID-19 prevention and awareness program.
In this study, it was found that patients with an education level below high school (AOR = 14.79; 95% CI: 3.25–67.15; p < 0.001) exhibited a poorer attitude toward COVID-19 when compared to a study conducted by Nguyen et al. 6 in Ho Chi Minh City (AOR = 1.28; 95% CI: 1.01–1.63, p = 0.044). In this study, we discerned that the participants exhibited limited knowledge about COVID-19 (AOR = 8.16; 95% CI: 3.48–19.08; p < 0.001), which contributed to poor attitudes to the management of COVID-19. The results could be attributed to differences in our study, the patients’ limited access to sources of information about COVID-19, so participants were unable to update their knowledge effectively about coronavirus prevention methods. Besides, they may lack awareness of the importance of complying with the preventive measures and may inadequately perceive the severity of the pandemic. These findings highlight the impact of ethnic background, educational attainment, and disease knowledge on shaping attitudes toward COVID-19.
When examining practices, we found that a higher proportion of participants in our study 100% of participants regularly wore masks when going outdoors and 75.5% of participants washing hands frequently, quite similar to the findings by Van Nhu et al., 17 95.8% of participants wear a face mask often and keeping hands clean with 98.5%. In addition, this result nearby is to the study of Zhong et al. 21 This might suggest a successful emphasis on mask-wearing in our study location. Importantly, Vietnam has excelled in COVID-19 prevention communication, thereby contributing to raising awareness and promoting positive actions in wearing masks and implementing preventive measures to ensure the safety of the community and society responses during the COVID-19 pandemic. 22 Besides, we observed that participants with poor knowledge (AOR = 3.33; 95% CI: 1.44–7.70; p = 0.005) and poor attitude (AOR = 2.42; 95% CI: 1.06–5.50; p = 0.035) are associated with poor practice toward management COVID-19. In addition, our study corroborates the observations that lower educational levels and poor knowledge significantly contribute to poor preventive practices toward COVID-19 in multiple previous studies.17,23 In this regard, this can be explained that low educational levels and poor knowledge can make it difficult for people to access accurate information about COVID-19. There might be misunderstandings of the instructions and recommendations from health authorities as this information is often presented in complex language and scientific concepts.
Taken together, these results indicate that while some practices such as health declarations, mask-wearing, and avoidance of crowded places were well adhered to, other practices, such as correct mask use, hand hygiene, respiratory hygiene, and frequent object cleaning, were less consistently observed. These findings highlight areas where further education and enforcement of COVID-19 precautionary measures may be necessary. In addition, these findings also emphasize the influence of age, education, disease knowledge, and attitude on adherence to COVID-19 preventive measures.
Our study’s results stress the importance of targeted interventions, especially for individuals with limited educational attainment or those who live in rural locations. Customized strategies could enhance their knowledge and facilitate more constructive attitudes and practices regarding COVID-19. This aligns with the study by Bukata et al. and another study conducted by Brankston et al. which highlights the significance of recognizing and addressing demographic disparities in COVID-19 responses.24,25
In the discussion of our findings, it’s worth emphasizing the conducting a multivariable logistic regression to identify the elements influencing the preventive measures against COVID-19. This statistical tool was particularly important as it allowed us to control for various confounding factors, thus ensuring a more accurate and reliable analysis of the relationship between the independent and dependent variables. 26
The multivariable analysis made it possible to simultaneously examine several characteristics such as age, gender, education level, area of residence, and source of COVID-19 information. The results highlighted that some factors had significant associations with preventive practices. For instance, older individuals and those with an education level below high school were more likely to engage in inadequate preventive measures. Furthermore, it was noted that poor knowledge about COVID-19 and negative attitudes toward the disease were associated with inadequate preventive behaviors.6,27,28
Such outcomes confirm previous studies such as those by Nguyen et al. 6 and another research conducted by Doan et al., 29 who found similar trends among Vietnamese populations. Our results also align with findings from Huynh et al.’s 5 research (2020) on outpatients at Second District Hospital, Ho Chi Minh City. However, reported different findings in a context among the Chinese-Canadian community in Canada, 30 underscoring the importance of cultural and regional variations in shaping attitudes and behaviors toward COVID-19.
The use of multivariable logistic regression in our study presents a comprehensive picture of the intricate interplay of ecological, socio-economic variables, knowledge, and attitudes in influencing COVID-19 preventive practices. This not only enhances our understanding of public responses to the pandemic but also allows us to propose more targeted and effective interventions. For example, strategies could focus on enhancing COVID-19-related awareness and attitudes across older individuals and those with lower educational levels.
Conclusion
In summary, our research enhances the existing knowledge of the pivotal aspects of COVID-19 prevention. It highlights the significant role of individual knowledge, attitudes, and practices in mitigating the spread of COVID-19. As the global community continues to grapple with the COVID-19 pandemic, studies like ours are critical in informing public health strategies and policies. Furthermore, the implications of this study extend beyond the immediate context of the COVID-19 pandemic. Indeed, the findings provide valuable insights for epidemiologists, researchers, health managers, and policymakers effectively strategize and respond to future pandemic-like events.
Study limitations
The research toolkit is designed based on existing questions, interviewing research subjects, and observing some contents in the patient’s practice. Therefore, the information obtained depends on the positive response and psychological influence during the interview attitude of the subjects. In addition, data collection is based on the interview form, the interviewing skill and the subjectivity of the investigator can be avoided. This can affect the accuracy of assessing the extent of the problem and lead to errors. The study was carried out by interviewing outpatients at a single site at Endocrinology Hospital of Nghe An Province and sampled by convenient sampling method, which could limit the generalizability of our findings due to potential selection bias. These considerations should be kept in mind when interpreting the study.
Supplemental Material
sj-docx-1-phj-10.1177_22799036241243269 – Supplemental material for Knowledge, attitude and preventive practice toward Covid-19 and associated factors among outpatients in a rural hospital in Vietnam
Supplemental material, sj-docx-1-phj-10.1177_22799036241243269 for Knowledge, attitude and preventive practice toward Covid-19 and associated factors among outpatients in a rural hospital in Vietnam by Vu Hai Ha, Nguyen Hoang Duc, Doan Thi Anh Van, Nguyen Viet Lac Thu, Nguyen Minh Son, Nguyen Thi Xuan Hien, Nguyen Huu Le, Duong Tien Hung, Nguyen Thi Bich Ngoc, Le Thanh Hung and Nguyen Tien Huy in Journal of Public Health Research
Footnotes
Acknowledgements
None
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.