
Abstract
Objective:
Breast self-examination (BSE) enhances self-awareness and may lead to earlier detection and treatment by increasing familiarity with one’s breasts. BSE may facilitate the earlier detection of abnormalities and prompt medical consultation. Educational interventions are significant in promoting BSE practices, strengthening knowledge, and modifying beliefs among women.
Methods:
This systematic review critically examines the current body of literature to thoroughly analyze the impact of educational interventions on BSE knowledge, beliefs, and practices in women. Studies based on experimental/interventional design, conducted globally on BSE practice, knowledge, and beliefs among women aged above 18 years, were included in this review.
Results:
A total of 24 studies with 5095 participants were included. The interventions consistently improved women’s knowledge, beliefs, and BSE-related outcomes. Meta-analysis of 10 experimental studies (n = 2424) showed a significant increase in BSE practice likelihood among intervention participants (OR = 8.30, 95% CI: 4.42–15.57; I2 = 88%).
Conclusion:
In conclusion the current systematic literature review demonstrates the efficacy of interventions in enhancing understanding of BSE and promoting practices among women.
Keywords
Introduction
Breast cancer (BC) remains the most diagnosed cancer and the leading cause of cancer-related mortality among women worldwide. According to GLOBOCAN 2020, an estimated 2.3 million women were newly diagnosed with BC, and approximately 685,000 deaths occurred globally in that year alone. 1 It accounts for one in every four cancer cases and one in six cancer deaths among women. The burden is especially pronounced in low- and middle-income countries (LMICs), where nearly 70% of BC-related deaths occur, often due to delayed diagnosis, inadequate screening programs, and limited access to timely treatment. 2 In South Asia, for example, BC incidence is steadily rising, with Pakistan exhibiting one of the highest age-standardized incidence rates in Asia, reporting about 50–55 cases per 100,000 women annually. 3 These trends highlight the urgent need for effective, scalable, and low-cost early detection strategies, particularly in settings with limited healthcare infrastructure.
Breast self-examination (BSE) is linked to self-awareness and supports BC detection. 4 This simple, convenient, and cost-effective technique allows women to practice at home. Regular BSE may enhance a woman’s awareness of breast changes, potentially prompting earlier clinical consultation and diagnosis of benign or malignant conditions. 5 While evidence on its impact on long-term outcomes remains limited, BSE may support earlier presentation and diagnosis by encouraging women to promptly seek medical attention upon noticing unusual changes. 6
To promote self-awareness and risk management in developing countries with limited resources, where mammography and other clinical screening methods are considered costly and not easily accessible for females, BSE is highly recommended for raising awareness 7 Younger women are advised to start practicing BSE in their 20s. 8 The advised time to perform BSE is monthly, when the menstrual cycle ends, because breasts are less likely to be tender and swollen. 9
Breast self-examination (BSE) practices vary among females in different regions, yet many low- and middle-income countries (LMICs) lack or have limited awareness campaigns on screening for BC and additional preventive measures, which results in insufficient awareness or compliance with. 10 BSE It is hypothesized that the low prevalence of BSE in LMICs is due to a lack of understanding of the procedure. 11 One study reported that in the U.S., approximately 75% of women perform BSE regularly; however, in Saudi Arabia, barely 30.3% of females are informed about BSE. Therefore, BSE should be promoted as a self-awareness strategy, particularly in low-resource settings, and educational initiatives should aim to increase knowledge and foster positive attitudes, 12 thereby encouraging timely health-seeking behavior when changes are detected. 13 However, it is difficult to create effective health education programs that target individual traits, which can then forecast the use of preventive services and health behavior. As beliefs affect behavior and may be adjustable, they may be excellent targets because they are influenced by individual traits. Beliefs distinguish people who share the same background. 14
Health behavior theories have proven effective in forecasting people’s engagement in programs to promote their health, and by using these ideas, significant advancements have been made in understanding the factors that influence people’s health. 15 A few health theories are used to modify the beliefs and attitudes of females toward BSE. Considerably, the commonly utilized theories in this aspect are the theory of planned behavior (TPB), the transtheoretical model (TTM), the social cognitive theory (SCT), 16 and the health belief model (HBM).17,18The target audience, the cultural context, the quality of the intervention, and the availability of resources and support are just a few examples of the variables that impact the effectiveness of these theories in altering behavior. 15
The current review addresses a considerable gap in the prevailing literature by targeting the effects of educational interventions on BSE practices, knowledge, and beliefs among women. Even though earlier reviews conducted in a similar area are useful, their generalizability has been limited since they frequently concentrated on certain groups. 19 Research evaluating its suitability for use across a variety of age groups is lacking. 20 By offering a thorough and inclusive examination across a range of ethnicities and age groups, this review and meta-analysis seek to close this gap. The meta-analysis conducted provides a nuanced understanding of the impact of interventions on BSE across diverse cultural backgrounds by synthesizing findings from the most recent and relevant studies. By incorporating the latest research. Furthermore, by identifying gaps in the literature, this review highlights areas for more advanced research and helps in designing more effective interventions with effective behavioral models that specifically promote BSE in low-resource settings, which ultimately improve breast cancer outcomes.
Objective
To assess and review the evidence on the effect of educational interventions on breast self-examination (BSE) practices, knowledge, and beliefs among women globally.
Research question
What is the impact of educational interventions on the knowledge, beliefs, and practice of breast self-examination among females across diverse backgrounds and geographic regions?
Methodology
The Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) guidelines (PRISMA-P) 2020 were followed in the reporting of this systematic review. The current review was carried out by a predetermined protocol registered on the International Prospective Register of Systematic Reviews (PROSPERO) with registration number CRD42023468462.
Eligibility criteria
Inclusion criteria
Articles reporting the consequences of interventions on awareness, beliefs, and performance of BSE were considered eligible.
Study area. Carried out globally.
Study design. Interventional/experimental studies, whether theory-based or not, were included.
Language. English.
Publication duration: articles published from January 2015 to June 2023. (The time frame is applied to narrow down the pool of studies to manage and focus on recent studies.)
Population: Experimental studies involving females aged 18 years or older with no previous history of BC. Importantly, the research population purposefully omitted BC survivors and diagnosed patients to reduce the possibility of bias in the results.
Exclusion criteria
Qualitative studies, studies that did not report the outcome of interest and studied population, research articles that were not accessible through databases, or full text was not retrieved, were excluded
Outcome of interest
Initial search approach
Several fulsome strategies were employed, such as manual journal searches, forward and backwards reference harvesting, and formal and informal literature searches. Three electronic databases, Science Direct, PubMed, and Scopus, were used in a methodical search in addition to these other databases, and a manual search was also performed on Google Scholar. The reference lists of the included studies and the websites of pertinent organizations, including the World Health Organization, were searched for other potential articles. The primary search terms utilized in each electronic search are provided (Supplemental file S1).
Study selection and screening
Studies were selected according to the PICOS framework (population, intervention, comparator, outcome, and study type) provided (Supplemental file S4).
Full PDF retrieval of studies
The full texts of the selected abstracts were retrieved, and the reviewers carefully examined the complete texts of the articles to determine their suitability. The reviewers thoroughly evaluated each article’s content to determine whether it satisfied the predetermined selection standard.
Data extraction
The two reviewers independently extracted the data from the articles by utilizing a standardized data extraction format. Disagreements were discussed and reconciled by the third author. The extracted data included details on the study’s first author, location, year of publication, study objective, population, sample size, study setting, intervention components, theoretical framework (if utilized), study outcome, follow-up time points, questionnaire administration method, and type of tool used, and psychometric properties of the questionnaire.
Quality assessment
The quality of these research articles was assessed using the Effective Public Health Practice Project (EPHPP) tool for intervention design studies. The following six domains were assessed: selection bias, research design, confounders, blinding, data collection technique, dropout and withdrawal, and overall rating called the Global rating. Each category was given a score between 1 (strong), 2 (moderate), and 3 (weak). By summing the scores for each of the six categories, a global rating of low, moderate, or high was provided. In the end, their global ranking assigned a high-quality rating to studies that received strong ratings in every category. Research with a moderate quality rating has one weak category, whereas studies with a low-quality grade have weak ratings in minimum two or more categories.
Metanalysis
A meta-analysis for BSE practice was conducted using a random-effects model to synthesize post-intervention outcomes from studies with a two-group experimental design. The primary effect measure was the odds ratio (OR) for BSE practice, with 95% confidence intervals. Heterogeneity across studies was assessed using Tau2, Chi2, and I2 statistics. All analyses were performed using RevMan software.
Results
Search outcomes
A literature search of three online databases and Google Scholar resulted in a total of 865 articles. After removing duplicates, 512 studies remained. Among them, 492 were screened for the software, and 20 articles were screened manually. After reviewing the titles and abstracts, 450 articles were excluded, resulting in a total of 62 full-text studies for complete review. Next, the studies were rigorously screened. Among them, 8 studies were removed because they were in the adolescent age group, and 30 studies were excluded due to irrelevant outcomes and study designs. After the inclusion criteria were met, 24 articles were retained. (Figure 1).

PRISMA flow diagram of the study.
Characteristics of the studies
Study designs
Among them were two RCTs; one was a CRCT trial; nine were quasi-experiments with 2 groups; and 12 had a pre/post design, as shown in Table 1. The study locations are as follows: one from Sri Lanka, three from Egypt, one from Saudi Arabia, one from Yemen, six from Iran, one from Korea, one from Malaysia, two from Türkiye, one from Nigeria, one from Thailand, one from China, two from India, one from Pakistan, one from Ethiopia, and one from Bangladesh.
Characteristics of the studies.
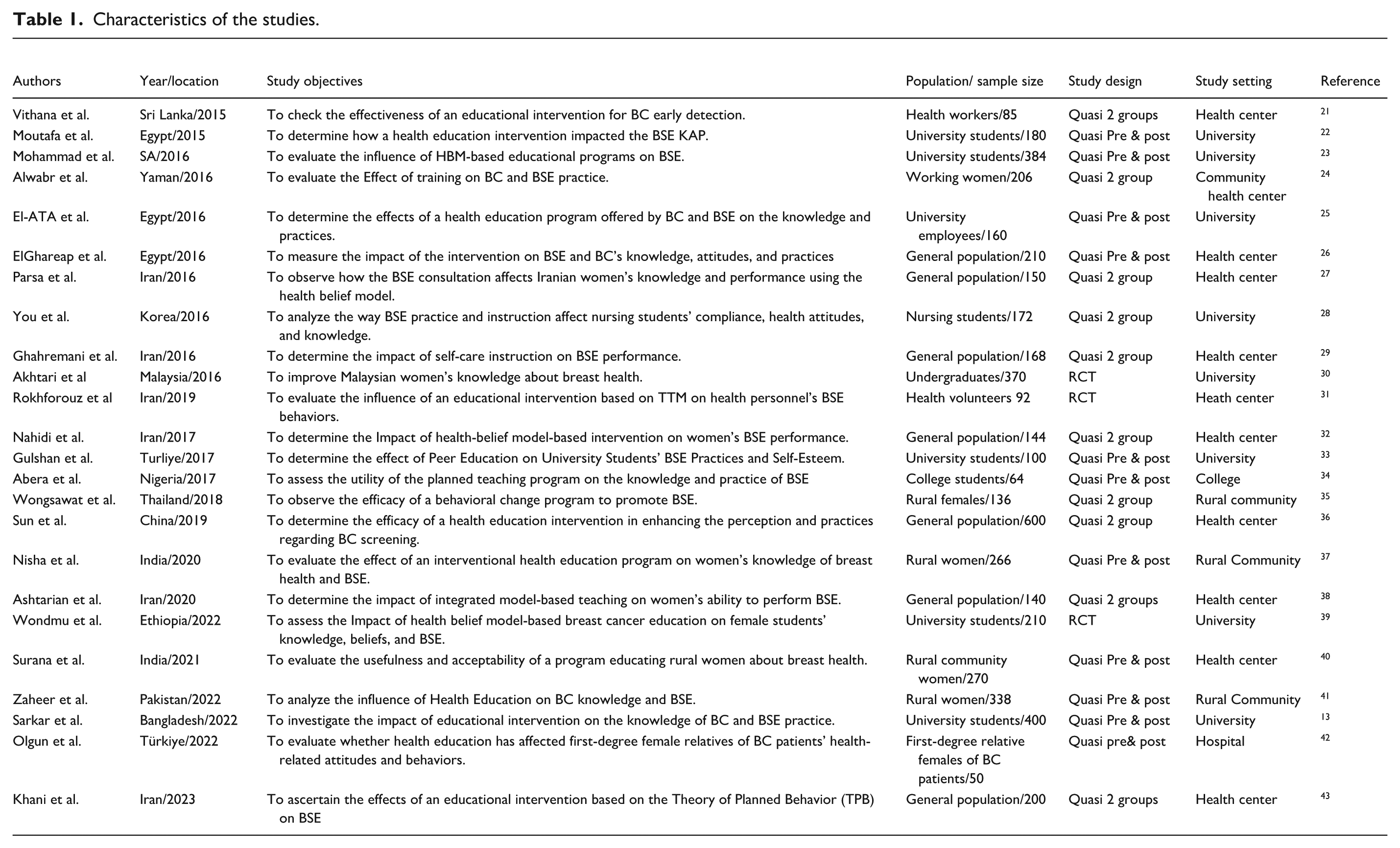
Study participants
The participants in this study were females aged 18 years and older. The current study had a sample size of 5095, and the sample sizes of the included studies ranged from 50 to 600. There are nine studies conducted among female college/university students; however, many studies were conducted in health care centers, 12 and three studies were conducted among rural communities.
Quality assessment
The EPHPP Quality Assessment Tool was used to rate the studies (Figure 2). Among all included studies, seven (n = 7) were well designed and ranked high quality; Ten (n = 10) were classified as moderate, and seven (n = 7) were classified as low. Most of the studies have been rated as weak in the “confounder control” domain. However, for the current study under the “blinding” subcategory, all studies were ranked with moderate risk because study participants knew they would be assigned to delivery schemes. Further details are provided in Supplemental file S2.

Overall summary of EPHPP risk of bias scores.
Intervention components and mode of delivery
All the interventional modules were characterized by theory- and language-based methods. The educational module content mostly addressed breast cancer and general knowledge associated with it. Awareness and knowledge of BSE, health beliefs associated with BSE, and methods of conducting BSE, as well as the importance and utility of BSE, Table 2.
Intervention components and study outcomes.
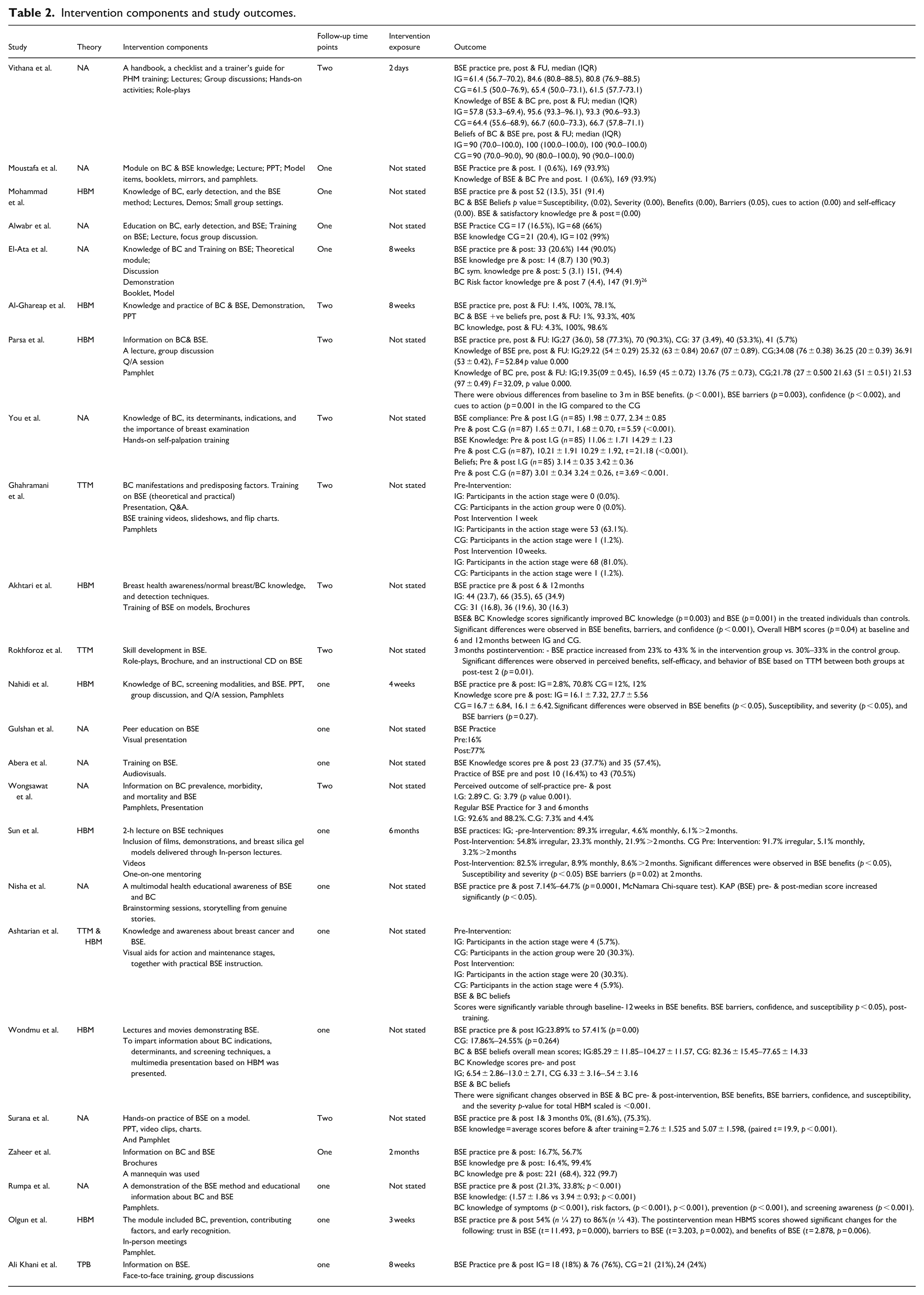
Theoretical framework
Three well-known theoretical frameworks were used as the foundation for the treatments in the included studies: HBM, TTM, and TPB, which were used to guide the methods used to design and evaluate the interventions. Twelve studies used these models; among them, eight studies used the HBM, one used the TBP, one utilized the TTM, and one used a mixed model approach by utilizing the HBM and TTM together. Out of 12 studies, 10 studies designed their intervention modules extensively according to health behavior theories.
Follow-up time points
Among 24 studies, the majority (15 out of 24) utilized one follow-up time point to evaluate the impact of interventions. Nine studies collected postintervention feedback at two different follow-up time points.
Study outcomes
BSE practice
In the current review, studies were selectively included based on the primary outcome measure of BSE practice percentage or score. The findings from research studies that examined women’s BSE practices were consistent. Experimental studies showed that after the intervention, individuals in the intervention group performed BSE more frequently (p < 0.05) than did those in the control group. Similarly, nine pre-postintervention investigations revealed that following the intervention, participants’ BSE performance significantly improved (Table 2).
BSE & BC beliefs
Among the 24 studies, 9 used the HBM standardized questionnaire to determine beliefs associated with BC and BSE. Almost all the studies showed consistent results and reported modified beliefs toward BC and BSE postintervention compared to those of the control groups. Experimental studies reported significant differences in the belief scores of the treatment group (Table 2).
Knowledge of BSE and BC
Changes in BC & BSE knowledge scores have been reported to be consistent. Studies with two groups reported increased knowledge in the treated group, and research studies with pre/post designs reported significant differences in knowledge scores at post-analysis.
Instruments/questionnaires used in studies
The main method for instrument administration used across most studies was a self-administered questionnaire (SAQ); however, two studies employed an interview method, as shown in Table 3. HBM-based studies utilized the Champion’s Health Belief Model Constructs Scale (CHBMS) to measure the health beliefs of participants toward BSE and BC. In addition to SAQs, BSE observation checklists with different numbers of items were administered pre- and post-BSE training in some studies. Overall, the studies utilized a combination of self-developed, adapted, and standardized tools to comprehensively evaluate knowledge, perceptions, and practices related to BC and BSE. Several studies have incorporated additional scales and models, such as the TPB and TTM, to extend their assessments.
Characteristics of the questionnaires.
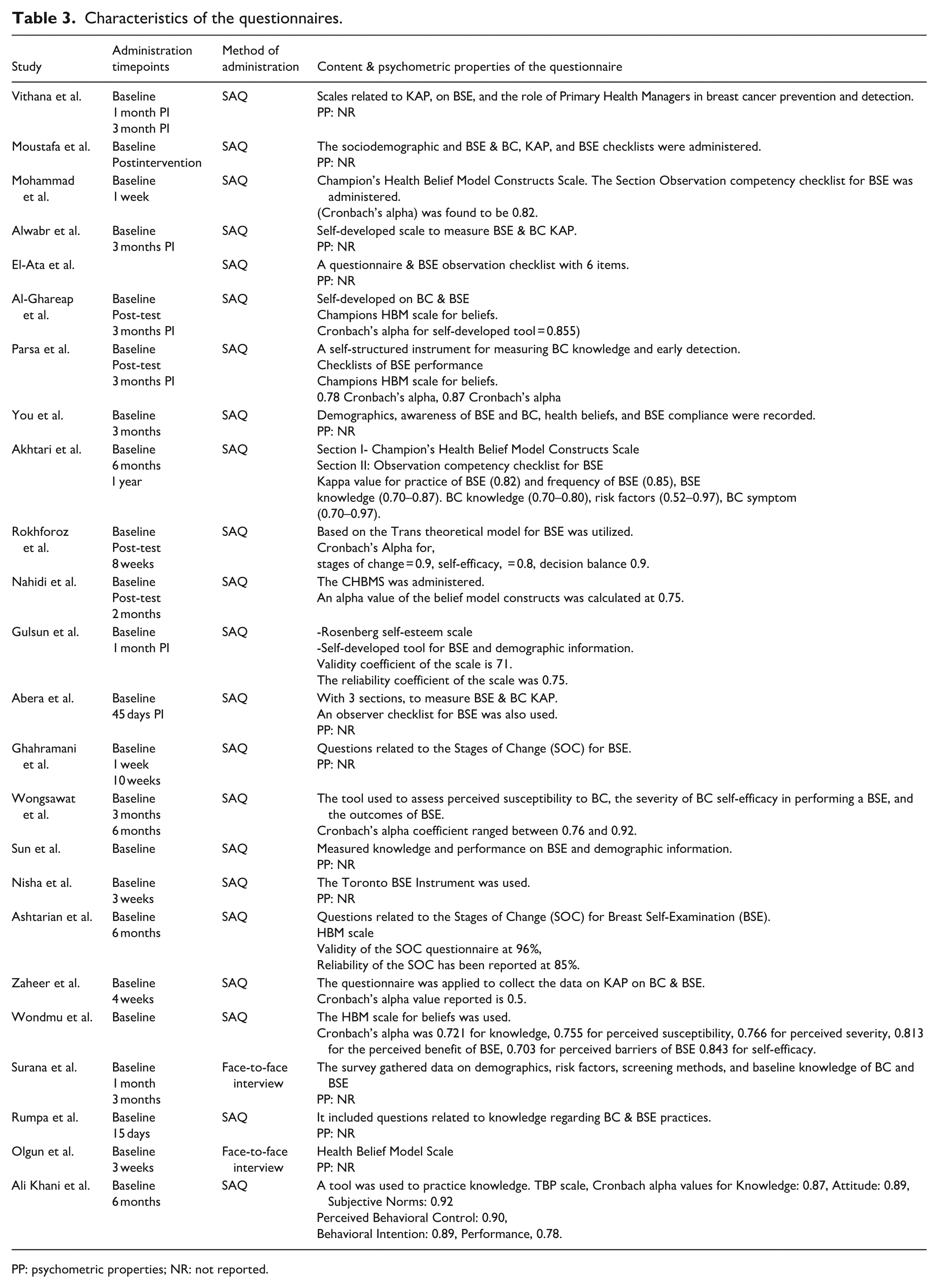
PP: psychometric properties; NR: not reported.
Meta analysis
A meta-analysis was conducted between the participants (intervention n = 1213, control n = 1211) of studies that used a two-group experimental design (Figure 3). The Primary outcome, Likelihood of BSE practice, was compared between the intervention and control groups, post-intervention. Remarkably high heterogeneity was observed between the studies, Tau2 = 0.93, X2 80.52, df = 10, (p < 0.00001), and I2 is 88%. The reported odds ratio of 8.30 (4.42–15.57) in our results suggests a substantial association or effect between the intervention and the likelihood of practicing BSE in the treated group.

Pooled odds ratios for the effectiveness of educational interventions on BSE practice.
Discussion
Early detection and prevention are critical for improving BC outcomes; therefore, health researchers have recognized the need for educational interventions to address this challenge by helping females become knowledgeable about BC and screening modalities. 44 The current study was planned to evaluate the efficiency of educational module-based interventions in improving breast self-awareness. In general, these studies have focused primarily on BSE knowledge and practices, and few have targeted participants’ beliefs about BSE and BC and overall general knowledge about breast cancer. However, during this systematic review, a noteworthy trend was observed in the available literature. Research on knowledge, attitudes, and practices (KAPs) related to BSE is lacking in high-income countries. For early detection, these regions often prioritize mammography and other screening programs, although poor countries have a greater frequency of BSE-focused studies. This discrepancy underscores the need to promote BSE as a self-awareness strategy for earlier detection in resource-constrained countries, where formal screening tools like mammography may not be accessible.
The primary outcome measured in the current review was breast self-examination. It is evident from the included studies that educational intervention plays a crucial role in encouraging females to practice BSE regularly. All reviewed studies reported great changes in BSE practices postintervention, and previous studies revealed similar findings. 45 This highlights the effectiveness of interventions in promoting BSE as a self-care practice. However, the criteria for evaluating “effectiveness” were not standardized across studies. Studies employed varied outcome measures such as frequency of BSE practice and improvement in technique, Improvement in knowledge and beliefs score in contrast to preintervention scores.
The studies included in this review highlighted the consistent improvement in knowledge scores associated with BC and BSE. These results demonstrate the efficacy of interventions in enhancing women’s understanding of these areas and in filling the knowledge gap. Our findings are in line with the findings of the current body of systematic review conducted by Bane Hashimi 20 and Sarah. 19
The studies included in this review paper reported varied time points, which helps to assess the long-term impacts of interventions. Most studies 15 collected data at a single time point postintervention; however, nine studies reported two follow-up data points to evaluate the effectiveness of interventions over both the short and long term. This approach offers a more thorough understanding of the long-term effects of educational interventions on BSE knowledge, practice, and beliefs; however, it is worth noting that the timing of follow-ups had an impact on the observed effectiveness of interventions. Studies with shorter follow-up periods (e.g. 1 month) often reported immediate but potentially transient improvements, while longer follow-ups (e.g. 6 months) provided insights into sustained behavioral changes. Future research should identify optimal follow-up intervals to ensure both short-term and long-term effectiveness are adequately captured.
Additionally, the meta-analysis results also showed that educational interventions significantly increased the likelihood of BSE, with an odds ratio of 8.30. Despite high heterogeneity (I2 = 88%), the strong and consistent effect across studies highlights the effectiveness of such programs in promoting BSE behavior. These findings reinforce the value of structured health education in improving preventive breast health practices.
The current review also delves into the modifications in beliefs related to BSE and BC following interventions. The HBM serves as a principal theoretical framework applied by 9 of the 12 studies. The HBM component’s perceived susceptibility, seriousness, benefits, barriers, and cues to action were used to reshape the beliefs of females through interventions. The findings from the reviewed articles showed notable improvements in beliefs related to BSE barriers, benefits, motivation, and confidence in treated groups in contrast to their counterparts, which is also consistent with the findings of previous research. 46 This finding implies that educational programs influence behavior in addition to positively altering women’s perceptions of the advantages and significance of BSE. This modification in belief is important, as it can motivate females to understand the importance of BSE more seriously. 47
The current study revealed three health behavior models used to enhance BSE practices: the TBP, a value expectancy health model. According to this theory, people will alter their behavior if they believe that personal gains from the result will exceed any costs associated with engaging in the action. 48 It is focused on decision-making and cognitive processes; it believes that perceptions are paramount and can be modified by health-promotion activities, and provides modifiable factors that may be addressed through education. 49 Additionally, it acknowledges the importance of environmental conditions, although its fruitful utilization in promoting health behaviors. 50 Among the reviewed studies, TBP is utilized by one study in BSE promotion. Its limited use may be certain underlying factors, as it does not address emotional and psychological variables, including fear, anxiety, and worries about breast cancer, that are linked to BC screening. 48
The health belief model is a model based on perceived fear and threat; this is the first model that incorporates the perceived threat construct in public health research. 51 It explains the fear process as a value-expectancy combination of two motivating factors: the perceived threat of the fear appeal and the expected benefit of a protective health behavior. 48 Fear, a powerful emotional and cognitive response, can be utilized to promote healthy behavior. It has been demonstrated that instilling fear in messages can alter either maladaptive or adaptive behaviors by heightening the perceived threat of a health condition or disease. The HBM suggests that an individual’s perception of taking preventative action depends greatly on how seriously and how susceptible they view a health issue to be a threat. 52
The trans-theoretical model, or the stages of change model, is neither a perceived fear or threat model nor a value-expectancy paradigm. Rather, it is a health behavior model that emphasizes the phases people go through when they decide to modify their behavior, particularly behaviors linked to their health. 48 TTM does not expressly focus on values or fear as the main motivating elements; rather, it is predicated on the notion that behavior modification is a process that includes numerous phases.
The TTM was applied in previous research to group people into precontemplation, contemplation, preparation, action, and maintenance stages of transformation. 53 By using a staged strategy, researchers were able to customize their interventions to each participant’s unique needs and level of preparation, ensuring that the interventions were appropriate for their present stage of transformation. However, less TTM was used for BSE adoption, possibly because the implementation of TTM interventions is time-consuming, often involves multistage interventions, and requires more resources to implement. Another limitation of TTM is that the stages are not clear according to the BSE perspective. BSE is more of a standard procedure that does not precisely fit into these phases. Since people are encouraged to self-examine frequently, it is difficult to categorize individuals into certain TTM stages. BSE is not a behavior that can be categorized into specific stages because it is a continuous, ongoing practice.
Although it is important to note that the application of these models varied among the included studies. While some studies assessed all components of the HBM, others focused on specific constructs, such as barriers and benefits. Despite this variability, the basic principles of these models consistently demonstrated their relevance in promoting BSE. These observations highlight the adaptability of the models to different study contexts while suggesting opportunities for future studies to explore standardized applications for enhanced comparability.
The fear and perceived threat models (HBMs) are probably more successful at encouraging BSE because they can effectively communicate the magnitude of the health concern (BC) and motivate women to conduct routine self-examinations to identify potential issues early. 48 These models can assist in addressing the perceived risk and emotional components, which are important factors in driving BSE behaviors. 53 However, before implementing fear and threat models, it is crucial to create a balance between empowerment and fear, ensuring that messages also offer appropriate remedies and boost self-efficacy for carrying out BSE successfully and without excessive worry.
Selecting the appropriate measuring tool is essential for obtaining high-quality study results. While differences in tools make cross-study comparisons more difficult, consistency across studies improves comparability. The reviewed studies utilized diverse tools and scales with extended focuses and designs, including Likert scales and structured tools. Tools such as the Breast Cancer Knowledge Test (BCKT) and Champion’s Health Belief Model Scale (CHBMS) were observed as the most commonly utilized tools in the included studies. Most of the studies utilized self-administered questionnaires, with only two utilizing in-person interviews,40,42 despite the potential for bias in both techniques. Study goals and participant comprehension influence instrument selection. Additionally, some studies failed to provide details on the reliability and validity of their instruments, raising concerns about the quality of the data. Therefore, it is essential to interpret the study findings carefully. The absence of reliability and validity details could introduce biases, including measurement error and misclassification, thereby potentially underestimating or overestimating the true effect of interventions. Addressing this gap by using validated tools would mitigate such risks and enhance the robustness of the findings. Future studies should adopt validated instruments, such as the BSE Knowledge Scale (BSEKS), Breast Cancer Awareness Measure B-CAM and Champion’s Health Belief Model Scale (CHBMS), to ensure consistency and methodological rigor
The synthesis of findings from this review reveals a consistently favorable influence of educational interventions on women’s comprehension of breast cancer (BC), cognitive perceptions, and engagement in BSE behaviors. Across heterogeneous populations representing diverse cultural and socioeconomic strata, these interventions were associated with marked enhancements in knowledge acquisition, diminished perceived barriers, strengthened self-efficacy, and increased adherence to recommended BSE practices. The consistency of these outcomes underscores the efficacy of structured, theory-driven educational frameworks in fostering proactive breast health behavior globally.
The findings underscore the effectiveness of educational interventions in enhancing BC knowledge, beliefs, and BSE practices among women. These results hold significant public health implications, particularly for low-resource settings where formal screening programs are limited. By integrating theory-driven educational strategies into existing community health frameworks, policymakers can design culturally appropriate, scalable, and cost-effective programs to promote early detection behaviors. Such interventions can be incorporated into national cancer control plans, school health curricula, or workplace wellness initiatives to foster sustained behavioral change and reduce the burden of late-stage BC diagnoses.
Additionally, this review highlights a critical gap in previous literature, where many studies focused on narrowly defined populations without addressing the cultural and contextual factors influencing BSE practices. By synthesizing evidence from diverse geographic, cultural, and socioeconomic settings, this review emphasizes the importance of culturally sensitive interventions tailored to local beliefs and health systems. Furthermore, it advocates for the use of standardized yet adaptable protocols that can be scaled globally, ensuring relevance and effectiveness across varied public health contexts.
Conclusion
Educational interventions effectively improve women’s knowledge, beliefs, and breast self-examination (BSE) practices, especially in settings where formal screening services are limited. Despite methodological variation across studies, the evidence supports integrating structured, theory-based education into community and public health programs. Standardized tools and longer follow-up periods are needed to strengthen future research and ensure sustained behavioral change.
Strength
One of the significant strengths of the current review is its global representation of diverse backgrounds. The use of experimental investigations is another crucial component of this review. Because they allow the manipulation of variables, experimental investigations come up with a more profound interpretation of causation and dynamics at work in study.
Limitations and future research directions
The current body of literature on educational interventions aimed at improving BSE practices and BC awareness demonstrates notable methodological diversity. Studies vary widely in terms of research design, participant demographics, intervention content, and measurement tools. This heterogeneity poses challenges for direct comparisons and limits the generalizability of findings. Additionally, many studies utilize short follow-up durations, which restrict the ability to assess the long-term impact and sustainability of behavioral change.
A further limitation is the use of diverse data-gathering instruments across populations, which may result in inconsistent data quality. The predominance of self-reported outcomes introduces the possibility of response bias, as participants may overstate or underreport their knowledge, beliefs, or BSE practices. A key limitation is that one-third of studies did not report intervention or follow-up duration, which limits our ability to distinguish short-term from long-term effects; therefore, conclusions about effect sustainability should be interpreted with caution. Moreover, insufficient control of potential confounding variables, such as age, education level, and socioeconomic status, may influence outcomes, especially in culturally and socioeconomically diverse populations. Additionally A meta-analysis for knowledge and belief outcomes could not be performed because the included studies used highly heterogeneous tools, scoring systems, and reporting formats, making statistical pooling inappropriate.
To enhance the quality and comparability of future research, there is a need for the use of standardized and validated tools, more robust study designs such as randomized controlled trials, and extended follow-up periods to evaluate the durability of intervention effects. Incorporating objective outcome measures, in addition to self-reported data, may improve data accuracy. Finally, future studies should emphasize the development and testing of culturally sensitive, adaptable interventions that can be implemented across diverse low-resource settings, thereby contributing to more equitable and effective breast cancer prevention strategies.
Supplemental Material
sj-docx-1-phj-10.1177_22799036261423725 – Supplemental material for The impact of educational interventions on breast self-examination practice, knowledge, and beliefs among women: A systematic review and meta-analysis
Supplemental material, sj-docx-1-phj-10.1177_22799036261423725 for The impact of educational interventions on breast self-examination practice, knowledge, and beliefs among women: A systematic review and meta-analysis by Benazir Mahar, Malina Binti Osman, Fatimah Ahmad Fauzi and Sani Aliyu in Journal of Public Health Research
Supplemental Material
sj-docx-2-phj-10.1177_22799036261423725 – Supplemental material for The impact of educational interventions on breast self-examination practice, knowledge, and beliefs among women: A systematic review and meta-analysis
Supplemental material, sj-docx-2-phj-10.1177_22799036261423725 for The impact of educational interventions on breast self-examination practice, knowledge, and beliefs among women: A systematic review and meta-analysis by Benazir Mahar, Malina Binti Osman, Fatimah Ahmad Fauzi and Sani Aliyu in Journal of Public Health Research
Supplemental Material
sj-docx-3-phj-10.1177_22799036261423725 – Supplemental material for The impact of educational interventions on breast self-examination practice, knowledge, and beliefs among women: A systematic review and meta-analysis
Supplemental material, sj-docx-3-phj-10.1177_22799036261423725 for The impact of educational interventions on breast self-examination practice, knowledge, and beliefs among women: A systematic review and meta-analysis by Benazir Mahar, Malina Binti Osman, Fatimah Ahmad Fauzi and Sani Aliyu in Journal of Public Health Research
Supplemental Material
sj-docx-4-phj-10.1177_22799036261423725 – Supplemental material for The impact of educational interventions on breast self-examination practice, knowledge, and beliefs among women: A systematic review and meta-analysis
Supplemental material, sj-docx-4-phj-10.1177_22799036261423725 for The impact of educational interventions on breast self-examination practice, knowledge, and beliefs among women: A systematic review and meta-analysis by Benazir Mahar, Malina Binti Osman, Fatimah Ahmad Fauzi and Sani Aliyu in Journal of Public Health Research
Supplemental Material
sj-docx-5-phj-10.1177_22799036261423725 – Supplemental material for The impact of educational interventions on breast self-examination practice, knowledge, and beliefs among women: A systematic review and meta-analysis
Supplemental material, sj-docx-5-phj-10.1177_22799036261423725 for The impact of educational interventions on breast self-examination practice, knowledge, and beliefs among women: A systematic review and meta-analysis by Benazir Mahar, Malina Binti Osman, Fatimah Ahmad Fauzi and Sani Aliyu in Journal of Public Health Research
Supplemental Material
sj-docx-6-phj-10.1177_22799036261423725 – Supplemental material for The impact of educational interventions on breast self-examination practice, knowledge, and beliefs among women: A systematic review and meta-analysis
Supplemental material, sj-docx-6-phj-10.1177_22799036261423725 for The impact of educational interventions on breast self-examination practice, knowledge, and beliefs among women: A systematic review and meta-analysis by Benazir Mahar, Malina Binti Osman, Fatimah Ahmad Fauzi and Sani Aliyu in Journal of Public Health Research
Footnotes
Ethical considerations
This study is a systematic literature review and did not involve direct human participants or animals. Therefore, ethical approval was not required. However, all sources were properly cited, and the review followed ethical research standards, including transparency in methodology and adherence to PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The article includes accessible analysis files and extended methodology files as Supplemental Material on the Sage Journals platform.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.