
Abstract
Background:
During the COVID-19 pandemic in Peru, primary health care services redistributed personnel to hospitals. In this context, Antenatal care (ANC) could have been limited in the general population, especially among indigenous communities.
Objective:
To determine differences in compliance with adequate ANC based on ethnic groups in Peru prior to and throughout the COVID-19 pandemic.
Methods:
Observational, retrospective study, secondary analysis of the Demographic and Family Health Survey conducted in the course the period 2017–2022. The sample consisted of women of childbearing age from 15 to 49 years and considered the variables of ethnicity, ANC, and sociodemographic factors. For statistical analysis, generalized linear models from the Poisson family utilizing a logarithmic link function were used. Crude and adjusted Prevalence Ratios were calculated along with their 95% confidence intervals.
Results:
A total of 20,165 records were reviewed. Before the pandemic, the frequency of inadequate ANC was 57.91%, and during the pandemic, it increased to 64.91%. Compared to mestizos, belonging to the Quechua ethnic group (PR: 1.08; 95% CI: 1.04–1.13), Aymara (PR: 1.21; 95% CI: 1.12–1.30), natives of the Amazon (PR: 1.15; 95% CI: 1.04–1.27), and those belonging to other races (PR: 1.15; 95% CI: 1.02–1.29) had a higher prevalence of inadequate ANC. During the pandemic, only Aymara women maintained a higher prevalence of inadequate ANC (PR: 1.18; 95% CI: 1.06–1.31).
Conclusions:
Before the pandemic, there were ethnic differences in the prevalence of inadequate ANC, and during the pandemic, only Aymara pregnant women maintained a higher prevalence of inadequate ANC.
Introduction
Antenatal care (ANC) is characterized as a series of scheduled appointments or visits to a healthcare center where a healthcare team monitors the progress of gestation to ensure optimal health conditions for both the mother and the child, aiming to reduce maternal and perinatal morbidity and mortality.1–3 The recommended number of ANC visits varies among countries, with Peru advocating for a minimum of six visits, ideally initiated before the 14th week of gestation. 4
In 2020, although 88.4% of Peruvian pregnant women received at least six ANC, there are still disparities in compliance. 5 A study using a nationally representative questionnaire found that only 35% of pregnant Peruvian women were adequately adhering to ANC, with the lowest compliance observed in the content of care that included all essential services recommended by the WHO, 6 such as clinical assessments, laboratory tests, supplementation, and counseling. 7 This study revealed that, compared to pregnant women residing on the coast, those living in the Andes exhibited inadequate adherence to ANC. Similarly, inadequate compliance was identified among pregnant women belonging to a native ethnic group compared to non-native counterparts. This is significant as it highlights another aspect of disparities in care and certain health indicators within a vulnerable population, such as indigenous communities.8–10
Peru, a multiracial and multiethnic country, comprises 55 indigenous persons and 48 indigenous languages, with 25.8% of the population self-identifying as part of an indigenous community.11,12 Nevertheless, despite coexisting with socio-economic disadvantages, not all indigenous communities share identical characteristic. Previous research has demonstrated ethnic differences in various health conditions.12,13 For instance, research has shown that being a Quechua-speaking or native language-speaking individual doubled the likelihood of not seeking health services due to mistreatment, and being of Aymara ethnicity tripled this probability. Similarly, during the pandemic, compared to indigenous peoples from the jungle, patients from Andean indigenous communities faced almost eight times the risk of dying from COVID-19. 13
For perinatal care-related outcomes, several studies have highlighted the impact of pandemic-related challenges on achieving adequate ANC.14,15 Similarly, various studies in other countries have shown ethnic differences, including variations in compliance with ANC.16–19 However, because the impact of social determinants of health varies among countries, these results may not be applicable to our country. On the other hand, the burden of these social determinants also varied during the pandemic, possibly explaining differences in mortality among Peruvian ethnic minorities during the pandemic, 13 or compliance with ANC in other countries. 20 In this regard, understanding these differences will allow quantifying a problem and proposing improvement strategies, taking into account an intercultural approach in public health policies. Consequently, the objective of this study was to determine the differences in compliance with ANC based on the ethnic group in Peru prior to and during the COVID-19 pandemic.
Methods
Study design
Secondary analysis of the Demographic and Family Health Survey (ENDES, acronym in Spanish) during the period 2017–2022. ENDES is a cluster-stratified, nationally representative sample survey conducted yearly by the National Institute of Statistics and Informatics (INEI in Spanish). The survey includes three questionnaires (household, individual, and health) and is conducted with the aim of updating knowledge on health indicators for the Peruvian population. 21
Population, sample, and sampling
The study population included women of reproductive age (WRA), ranging from 15 to 49 years old. The sampling method used in ENDES is a balanced, two-phase, stratified, and independent probabilistic sampling at the departmental level, distinguishing between urban and rural regions. ENDES estimates are annually representative at the national level, urban/rural breakdown, by geographical domain (Lima Metropolitan Area, Coast, Highlands, and Jungle), and for all 24 regions of Peru and the constitutional province of Callao. 21
Peru is an Andean–Amazonian country with pronounced geographic and cultural diversity. Most referral obstetric hospitals are clustered in coastal cities, whereas the highlands and jungle regions depend on lower-level facilities that offer basic prenatal care and refer high-risk pregnancies to higher-tier centers. 22 Household incomes follow a similar gradient, being highest in urban coastal areas and lowest in rural Andean and Amazonian communities, which further widens disparities in access to and quality of maternal care nationwide.23,24
Eligibility criteria
Women of childbearing age (15–49 years) who had given birth within the last year prior to the survey application were included. Pregnant women and those with incomplete information in our variables of interest were excluded.
Variables
The dependent variable was inadequate ANC. This variable was constructed based on non-compliance with any of the recommendations from the World Health Organization (WHO). 6 Additionally, the methodology used in earlier studies was taken into account for its construction.7,25 The construction of the variable involved the assessment of four aspects: (i) First ANC visit during the first trimester; (ii) Number of ANC visits during pregnancy; (iii) Adherence to the programs featured in each ANC visit, and (iv) ANC provided by trained personnel. Non-compliance with any of these four aspects was considered inadequate ANC. ENDES does not include medical-record abstraction; therefore, compliance is based on self-report.
Regarding the first ANC visit in the first trimester, it was assessed with the question: “How many months pregnant were you when you had your first antenatal care visit?” an ANC visit during the first trimester was considered appropriate.
The number of ANC care visits was assessed with the question: “How many ANC visits did you attend during your pregnancy with (child’s name)?” A number of visits six times or more was considered adequate according to the guidelines of the Technical Standard of the Ministry of Health (MINSA) of Peru. 4
To comply with the programs featured in each antenatal visit, the guidelines provided by the World Health Organization (WHO) for the care of expectant mothers during each antenatal visit 6 and previous studies 26 were considered. These programs included: HIV/AIDS analysis, syphilis screening, blood and urine analysis to clarify issues that arise during pregnancy, guidance on where to seek help in the event of complications, blood pressure measurement, taking iron supplements as advised by healthcare professionals, and tetanus vaccination.
ANC provided by trained personnel was assessed with the question: “Who attended to you during the delivery of (child’s name)?,” with possible responses working as a doctor, nurse, obstetrician, nursing technician, or midwife. Trained personnel were considered to be doctors, nurses, obstetricians, and nursing technicians.
The main independent variable was the ethnicity of the mother (mestizo, Quechua, Amazon native, member of another indigenous group, or black, white, and other races). This variable was constructed based on the respondent’s answers to the question: “According to your ancestors and according to your customs, do you feel or consider yourself to be:.” Potential responses were Quechua, Aymara, indigenous people of the Amazon, associated with or part of another native group, Black/moreno/zambo/mulato/Afro-Peruvian or Afro-descendant, white, mestizo, other races. Responses of “Don’t know/No response” were excluded.
Additionally, we included covariates such as age (15–25, 26–35, and 36–49 years), education level (primary or lower, secondary, non-university higher education, university), marital status (single, married, cohabiting, widowed, divorced/separated), number of children (one child, two children, three children, four children or more), health insurance coverage (no, yes), wealth index (very poor, poor, middle, rich, very rich), area of residence (urban, rural), and geographic region of residence (Lima Metropolitan Area, remaining areas of the coast, highlands, and jungle).
Statistical analysis
The databases of the ENDES for the period 2017–2022 were downloaded in SAV format, subsequently exported and analyzed using STATA v16.0 (TX, StataCorp LP). All sampling patterns were evaluated based on stratum and weighting factor., considering the intricate sampling design of the ENDES, using the svy command.
In the descriptive analysis, categorical variables were presented as frequencies and percentages along with their 95% confidence intervals (CI). Numeric variables were presented as means with their respective 95% CIs. To determine if there were significant differences between categorical variables according to the proposed outcomes, the Chi-square test with Rao Scott correction for complex sampling was used. Wald test was employed to assess differences between numeric variables.
To evaluate the association between ethnicity and inadequate ANC, generalized linear models from the Poisson family with a logarithmic link function were constructed. Crude Prevalence Ratios (PRc) and adjusted Prevalence Ratios (PRa) were calculated with their respective 95% CIs. The crude model was a bivariate regression, whereas the adjusted model included variables that reported a p-value < 0.20 according to a backward selection model. Multicollinearity was assessed using variance inflation factors, considering a cutoff point greater than 5. A p-value less than 0.05 was established as statistically significant for all analyses.
Ethical considerations
We analyzed secondary data from the ENDES, which is freely available on the INEI website (http://iinei.inei.gob.pe/microdatos/). The databases can be downloaded without including identifiers, thereby ensuring the confidentiality of the respondents’ information. It is important to highlight that all participants provided informed consent to be surveyed.
Results
We identified a total of 125,452 reproductive events (WRA) during the period 2017–2022. About 93,188 participants were excluded for not having had any children in the last year, and 116 participants were excluded due to pregnancy. Subsequently, 11,982 participants were excluded due to incomplete or inconsistent information in the variables of interest. Finally, 20,165 (WRA) records were analyzed, representing a population of 1,560,371 individuals (Figure 1).

Participant selection flowchart included in the analysis, ENDES 2017–2022.
The mean age was 28.7 (28.6–28.8) years, with 47.36% having secondary education, and 64.14% being in a cohabiting relationship. The average number of children was 2.19 (2.17–2.22) children. About 24.22% were classified as very poor, 74.43% lived in urban areas, and 29.43% resided in Lima Metropolitan Area. Concerning ethnicity, 48.77% identified as mestizo, followed by Quechua at 25.52%, and Aymara at 1.69%. The frequency of inadequate ANC in the last pregnancy was 61.17%. Regarding ANC, 77.17% had their first check-up during the first trimester, 85.05% had six or more check-ups, only 0.01% were not attended by trained personnel, and 51.41% reported adequate compliance with ANC components (Table 1).
General characteristics of sample included in the analysis, ENDES 2017–2022 (n = 20,165; N = 1,560,371).
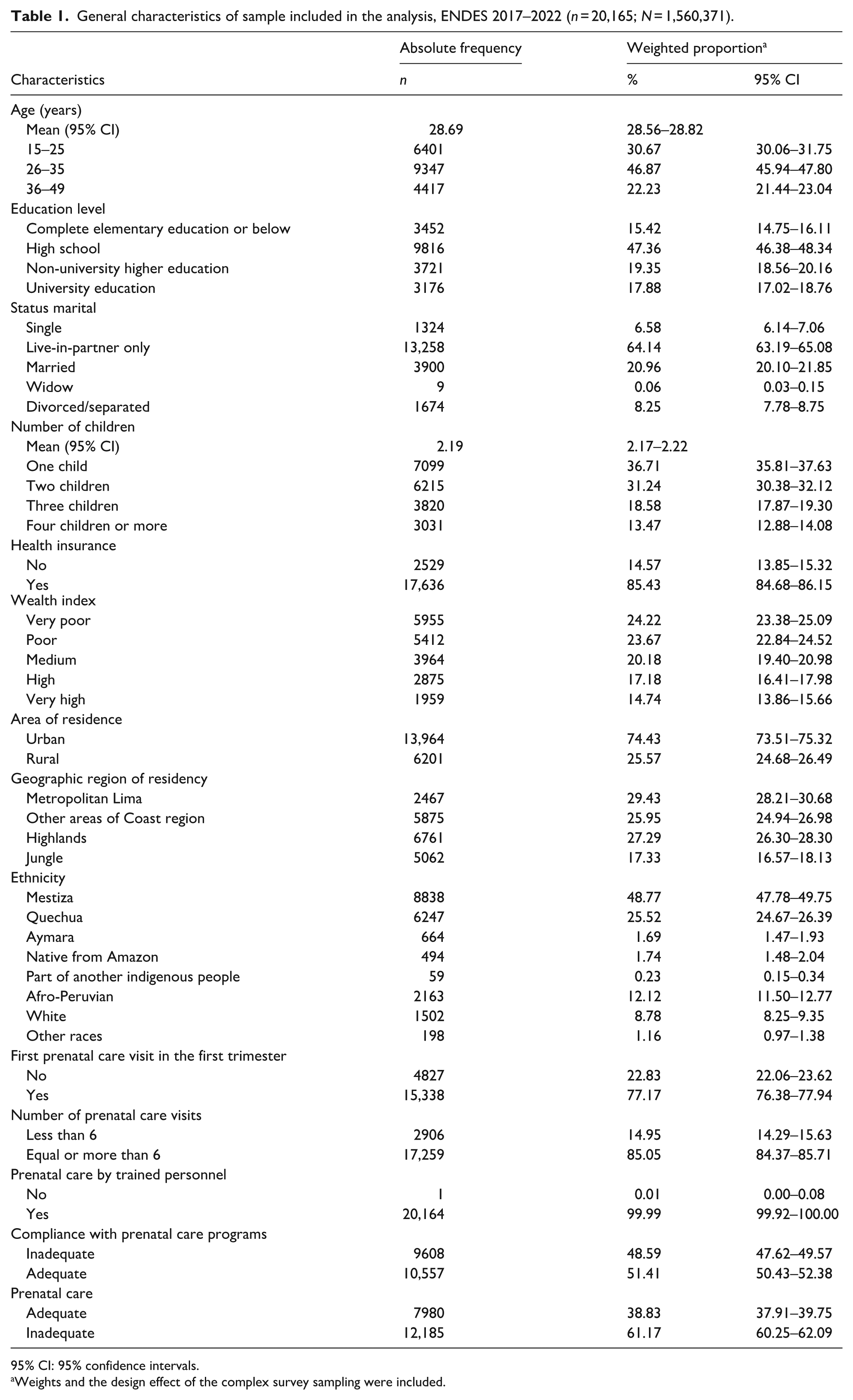
95% CI: 95% confidence intervals.
Weights and the design effect of the complex survey sampling were included.
In the bivariate analysis of general characteristics according to ethnicity, statistically significant differences were found for all variables (Table 2).
General characteristics of the sample included in the study according to ethnicity.

Weights and the design effect of the complex survey sampling were included.
The bold font in Table 2 indicates values where the p-value is statistically significant.
Refers to the statistical significance obtained from the comparison of the proportions between the categories of the variables considering the complex sampling of the survey.
The frequency of inadequate ANC during the COVID-19 pandemic saw a notable increase compared to the period before it (64.95% vs 57.91%; p < 0.001). These differences were observed among mestizo women (62.86% vs 52.68%; p < 0.001), Quechua women (69.02% vs 65.50%; p = 0.025), and white women (64.96% vs 58.64%; p = 0.045; Table 3).
Frequencies of prenatal care in the pre-pandemic period and during the COVID-19 pandemic by ethnic group.

95% CI: 95% confidence intervals.
Weights and the design effect of the complex survey sampling were included.
The bold font in Table 3 indicates values where the p-value is statistically significant.
p-Values from survey-adjusted Rao–Scott χ² tests comparing the distribution of adequate versus inadequate care between the pre-pandemic and pandemic periods within each ethnic group (and for the entire sample).
In the bivariate analysis of general characteristics concerning ANC, all variables were significant except for health insurance (Table 4).
General characteristics of the sample included in the study according to prenatal care.
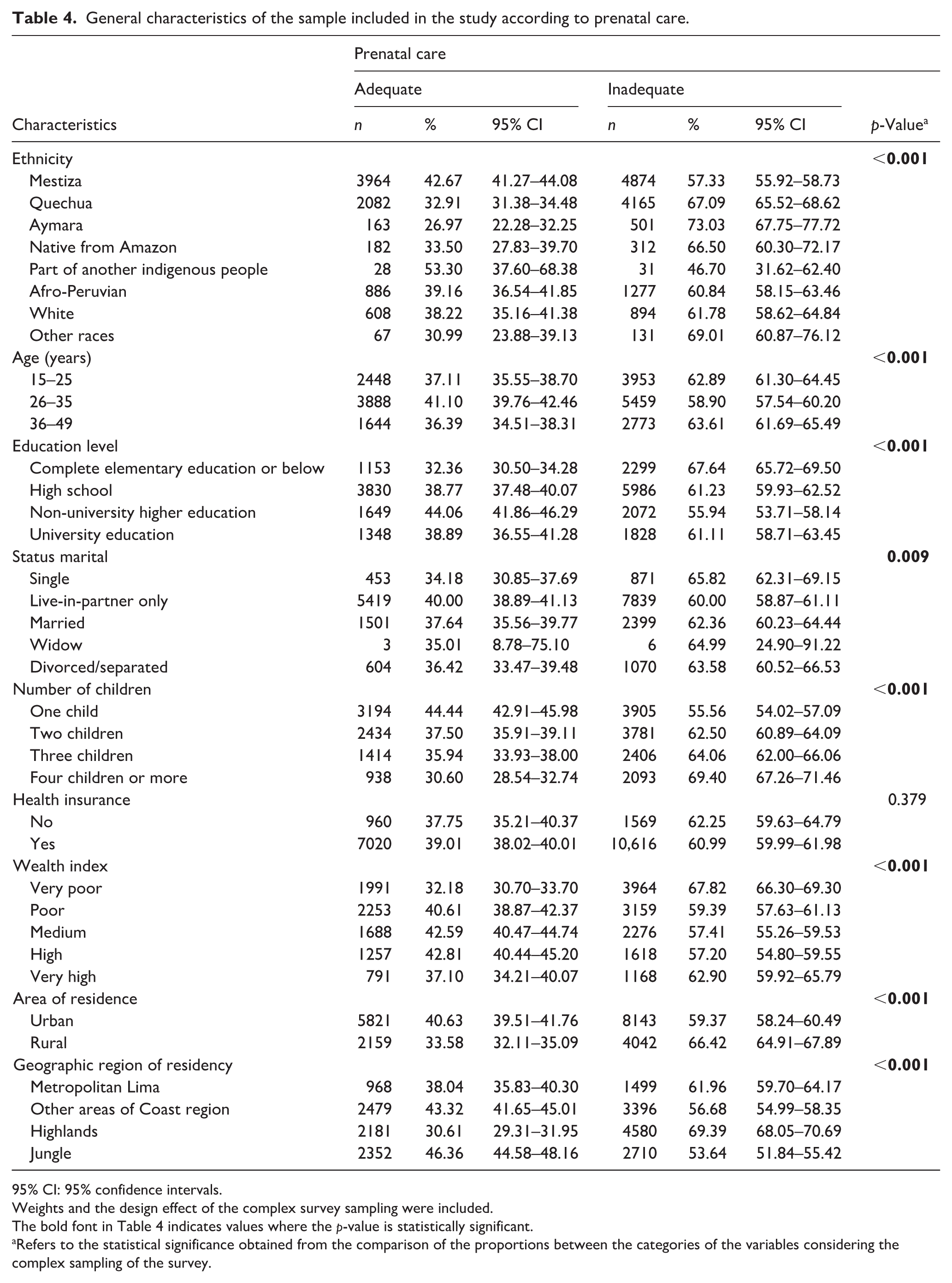
95% CI: 95% confidence intervals.
Weights and the design effect of the complex survey sampling were included.
The bold font in Table 4 indicates values where the p-value is statistically significant.
Refers to the statistical significance obtained from the comparison of the proportions between the categories of the variables considering the complex sampling of the survey.
In the multivariate analysis adjusted to assess the association between ethnicity and ANC in the last pregnancy, it was found that, compared to mestizo women, belonging to the Quechua ethnicity (PR: 1.08; 95% CI: 1.04–1.13; p < 0.001), Aymara ethnicity (PR: 1.21; 95% CI: 1.12–1.30; p < 0.001), Amazonian natives (PR: 1.15; 95% CI: 1.04–1.27; p < 0.001), and those belonging to other races (PR: 1.15; 95% CI: 1.02–1.29; p = 0.021) had a higher prevalence of inadequate ANC (Table 5).
Crude and adjusted models to evaluate the association between the ethnicity and the inadequate prenatal care in the sample included in the analysis.

PR: prevalence ratio; 95% CI: 95% confidence intervals.
The bold font in Table 5 indicates values where the p-value is statistically significant.
A generalized linear model of the Poisson family with a log link was made considering the effect of the design and the weights of the complex sampling of the survey.
Adjusted for age, number of children, health insurance, wealth index, area of residence, geographic region of residence.
In the adjusted analysis to assess the prevalence of inadequate ANC before and during the pandemic, it was found that, before the pandemic, compared to mestizo women, belonging to the Quechua ethnicity (PR: 1.11; 95% CI: 1.05–1.18; p < 0.001), Aymara ethnicity (PR: 1.23; 95% CI: 1.10–1.36; p < 0.001), Amazonian natives (PR: 1.21; 95% CI: 1.05–1.38; p = 0.008), and those belonging to other races (PR: 1.21; 95% CI: 1.04–1.40; p = 0.014) had a higher prevalence of inadequate ANC. On the other hand, during the pandemic, only Aymara women (PR: 1.18; 95% CI: 1.06–1.31; p = 0.002) had a higher prevalence of inadequate ANC (Table 5).
Discussion
Our main results show that 6 out of 10 pregnant women had inadequate ANC, and, compared to mestizo pregnant women, those of Quechua, Aymara, Amazonian native, and other ethnicities had a higher prevalence of inadequate ANC. Likewise, during the pandemic, only Aymara pregnant women had a higher prevalence of inadequate ANC.
Overall, national ANC coverage improved. A study found that the number of ANC visits increased from 77.22% to 87.52% from 2009 to 2019. 27 During the same period, the relative difference between women in rural and urban areas shrank from 15% to 3%, while the percentage of pregnant women lacking access to quality visits dropped from 45.16% to 29.35%. 27 Regarding access to quality check-ups, absolute inequality by wealth quintile also nearly halved, from 55.96% to 25.95%. 27 Despite these improvements, barriers persist that hinder compliance with visits or the quality of ANC. Using the 2017 ENDES data, another study demonstrated that receiving more ANC increased the likelihood of receiving quality ANC. 26 Furthermore, it was found that being a pregnant woman from the highlands, living in a rural area, and belonging to a native ethnicity were associated with a lower likelihood of receiving quality ANC. 26 Having secondary and higher education, being in the wealth quintile 2–5, belonging to the rest of the Coastal and Jungle regions, having health insurance affiliation, and receiving ANC in the first trimester were associated with a higher likelihood of receiving quality ANC. 26 Subsequently, a study utilizing the 2019 ENDES data revealed that being in the age groups of 20–34 and 35–49, with secondary or higher education, being in a wealth quintile above the poorest, coming from the Amazon region, not identifying as indigenous, experiencing a second or third pregnancy, along with having a planned pregnancy, raised the likelihood of achieving adequate compliance with ANC. 7
These results demonstrate that, in addition to certain obstetric conditions, sociodemographic aspects influence the proper fulfillment of ANC, including ethnic origin and other characteristics common among indigenous peoples that predefine them as vulnerable populations. In this regard, originating from rural areas, being from the highlands or the Amazon, and the condition of poverty found in these studies are common characteristics among pregnant women from indigenous communities and could explain our results.7,26
Indeed, a nationwide survey in 2015 aimed at illustrating ethnic dynamics in our country showed that individuals who self-identified as mestizo reported living in urban areas to a greater extent than those who identified as indigenous (57.1% vs 56.2%). 28 Similarly, Andean households were 80% more likely, and Amazonian households were 170% more likely to live in poverty compared to “white-mestizo” households. 28 Descriptive variables regarding labor market characteristics indicated that education allows for achieving better goals and living conditions. Again, the Amazonians, Quechuas, and Aymaras showed lower levels of education attainment, with fewer chances of accessing the labor market In the case of the Aymaras and Quechuas, especially those in the remote areas of the country, distance from productive niches and lack of infrastructure make it challenging to attain higher educational levels compared to mestizos or whites, diminishing opportunities to access the productive job market. 28
Much like in the case of ANC, these characteristics potentially explain the poorer health indicators in these populations,29,30 alongside factors hindering access to health services. These factors include linguistic barriers, distance to health centers, lack of transportation, discrimination, and mistreatment in healthcare establishments in Peru.12,31 Similar to our country, other studies have also suggested that ethnic minorities or indigenous peoples face disadvantages in terms of social determinants of health, making them susceptible to less antenatal attention or overall obstetric care. This warrants the design of specific strategies considering their unique characteristics.16–19,32 During the pandemic, these social determinants worsened for ethnic minorities, 33 which, in the case of Peru, led to variations in mortality among indigenous peoples 13 and potentially could have also affected ANC compliance.
In the United States, a study found that, during the pandemic, while most racial and ethnic groups in Medicaid expansion states experienced a decrease in inadequate ANC, the odds of lacking ANC increased for some ethnicities. 20 Specifically, they increased by 15% for non-Hispanic whites, 9% for non-Hispanic Blacks, 33% for Native American Alaskan Natives, 25% for Asians/Pacific Islanders, and 13% for Hispanics in states without Medicaid expansion. 20 Peru was one of the countries most affected during the pandemic due to various factors, including structural issues in its healthcare system. 34 The pandemic led to an overload of hospital systems focused on caring for COVID-19-infected patients, sidelining aspects such as ANC because pregnant women faced difficulties accessing health services. 35 These conditions likely explain the 7% decrease in adequate ANC during the pandemic nationwide. However, the use of teleconsultations and mobile devices represented an alternative to improve care for pregnant women during this period.36,37 Although their coverage by ethnicity or geographical region was not studied in our country, their variations could possibly also influence the variation in inadequate ANC in our country.
The Aymara people are one of the largest indigenous groups in Peru, and according to the national census of 2017, 548,311 individuals self-identified as Aymara, primarily residing in six provinces in Puno and some rural districts in Moquegua and Tacna. 38 Puno, a mountainous region, experienced a rise in the number of pregnant women receiving six ANC visits before the pandemic. 28 Although not one of the regions in Peru with the highest number of COVID-19 deaths, 39 Puno is among the less privileged regions in the country. While our study does not aim to describe why, during the pandemic, only Aymara pregnant women persisted with a higher prevalence of inadequate ANC, these explanations may lie in the limitations of the healthcare system in this region. For example, during the first wave, the first level of care was non-operational, leading to the entire demand for care of infected patients being shifted to the second level of care. 40 In this sense, pregnant women may not have had a place to undergo ANC. However, despite evidence of teleconsultation implementation for ANC, 41 there is no data on its effectiveness, and there is no evidence of cultural adaptations of teleconsultation to the customs and practices of the Aymara nation that may limit its implementation.
Our results have implications for public health. Firstly, despite existing public initiatives that include interculturality, 12 our findings show that ethnic differences persist in the healthcare of pregnant women. Therefore, considering the consequences of inadequate ANC on perinatal morbidity and mortality in our country, 42 this should prompt the development of strategies that reinforce the intercultural competencies of healthcare professionals. Additionally, due to the challenges of access to healthcare services for individuals belonging to indigenous peoples,8,30,31 the reinforcement of telemedicine,36,37 should continue, taking into account the cultural relevance of care. In this regard, policies to promote better adherence to ANC, institutionalized childbirth, 43 vertical delivery, and other strategies, unfortunately, regressed during the pandemic.
Our research has some limitations. First, although our study is based on secondary data and thus subject to potential recall or social desirability bias, it is important to note that ENDES employs validated questionnaires developed by expert panels to ensure clarity and cultural appropriateness. Furthermore, data collection is carried out by trained health personnel using standardized protocols under strict supervision, which helps to minimize measurement errors and enhance the reliability of the self-reported information. Additionally, the survey applies a complex, probabilistic, and stratified sampling design, which ensures national and regional representativeness and reduces the likelihood of selection bias. Second, the definition of adequate ANC was based exclusively on the frequency and timing of antenatal visits, without incorporating aspects of quality of care such as the type of health professional providing the service, the availability of screening tests (double test, triple test, or Non-Invasive Prenatal Test (NIPT)), or the performance of morphologic ultrasound examinations. Third, the ENDES does not collect information on maternal clinical history or risk factors that could influence the number of ANC visits, such as maternal comorbidities (hypertension, diabetes), previous obstetric complications, nutritional status, or contextual barriers (socioeconomic, cultural, and geographic). Although we used multivariable regression models to control for potential confounders, residual confounding due to unmeasured variables cannot be ruled out. Addressing these aspects in future studies would provide a more comprehensive understanding of the determinants of ANC utilization. Fourth, it is not possible to establish cause-and-effect relationships; only associations can be determined.
It is also essential to deepen the understanding of how much of the inadequate antenatal care disproportionately affecting different ethnic groups actually translates into adverse outcomes during pregnancy and the neonatal period. The marked cultural, social, and geographic diversity of Peru suggests that this relationship is unlikely to be homogeneous, making it relevant to promote research that examines how ANC adequacy may mediate the link between ethnicity and maternal-perinatal outcomes, thereby providing more contextualized evidence to design culturally appropriate interventions.
Despite these limitations, the ENDES is a nationally and regionally representative survey with quality control processes and extensive use for studying health topics in the Peruvian population. Furthermore, it records data used to assess the adequate fulfillment of ANC based on WHO recommendations and is regulated by the Ministry of Health (MINSA).
Conclusion
In conclusion, there are ethnic differences in ANC compliance among Peruvian pregnant women, which persisted during the pandemic for some indigenous peoples. A continued intercultural approach in ANC and reinforcing cultural relevance in telemedicine is necessary to improve health system coverage.
Footnotes
Acknowledgements
Not applicable.
Author contributions
Agueda Muñoz-del-Carpio-Toia, Percy Herrera-Añazco, Jerry K. Benites-Meza, and Vicente A. Benites-Zapata: Conceptualization and study design, data acquisition, formal analysis and interpretation, drafting the original manuscript, and final approval of the version to be submitted.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by the project “Importancia de la vacunación y el autocuidado de la salud COVID-19” from the internal fund of the Vicerrectorado de Investigación of Universidad Católica de Santa María, Arequipa, Peru.