
Abstract
Background:
Central obesity, characterized by excess fat as measured by waist circumference, is a significant public health concern that impacts health outcomes in both developed and developing countries, including Ethiopia. This study aimed to assess the prevalence of central obesity and its associated factors among adult public sector workers in Jigjiga town, Somali Region, Eastern Ethiopia.
Design and methods:
An institutional cross-sectional study was conducted from April 15–30, 2024, among 628 public sector workers selected by a multistage sampling method in Jigjiga town, Somali region, Eastern Ethiopia. Data was collected using a pretested structured questionnaire. Descriptive analysis was done. Bivariable and multivariable logistic regression analyses were performed to assess associations. The strength of associations between central obesity and independent variables was determined by adjusted odds ratios (AORs) with 95% confidence intervals.
Results:
Of the 628 public sector workers included in April 2024, the prevalence of central obesity was 48.6% (95% CI: 44.7%–52.6%), with 46.7% in males and 53.4% in females. Being female (AOR = 1.52, 95% CI = 1.04–2.21), physical inactivity (AOR = 2.02, 95% CI = 1.14–3.58), eating red meat 1–2 times per week (AOR = 1.55, 95% CI = 1.02–2.34), being non-diabetic patients (AOR = 0.35, 95% CI = 0.12–0.97), and non-stressful work (AOR = 0.38, 95% CI = 0.17–0.85) were significantly associated with central obesity.
Conclusion:
The prevalence of central obesity among public sector workers in this study was high. As a result, interventions should focus on promoting physical activity through workplace wellness programs, encouraging healthier dietary choices, providing resources for stress management, and monitoring health and work environments, along with behavioral change interventions, which would be crucial in reducing central obesity among public sector workers.
Introduction
Obesity is a significant public health issue, characterized by excess fat accumulation in the central body, which has serious health consequences. It is considered when the body mass index (BMI) of individuals is 30 or higher, which is the usual benchmark, or when the waist circumference (WC) is greater than 94 cm and 80 cm for males and females, respectively. 1
The most common type of obesity is central obesity, also known as abdominal obesity or truncal obesity, which is a medical condition characterized by an excessive accumulation of visceral fat around the stomach and abdomen.2,3 Globally, around 1.9 billion adults were overweight, and of these, obesity accounted for over 650 million in 2016. 4 The overweight population was increased by over 2.6 billion in 2020, suggesting that over 4 billion people may be affected by 2035, which reflects an increase from 38% of the world’s population to over 50% in these 15 years. 5 Adult obesity prevalence in the 10 high-burden countries in Africa, including Ethiopia, ranged from 13.6% to 31% in 2022, according to a WHO study. 6 By December 2023, it was predicted that one in five people would be obese if strong action is not taken to buck the trend.6,7 Specifically, the global prevalence of central obesity was 41.5%. 8 In Ethiopia, a systematic review and meta-analysis revealed that the magnitude of central obesity was estimated to be 37.31%, 9 and in Dire Dawa Administrative City, Eastern Ethiopia, it accounted for 76.1%. 10
Obesity is one of the leading risk factors for premature death, and 8% of global deaths were ascribed to obesity.11,12 Furthermore, central obesity is linked to increased disease-specific morbidity, 4.0 million deaths worldwide, roughly 36.3 million YLLs, and costs $4.32 trillion worldwide, $3.8 billion in Saudi Arabian health spending, and $552.31 million in Ethiopia.13–18 It’s a major risk factor for several health issues, such as cardiovascular disease, which can lead to heart attacks, strokes, and other serious health problems; type 2 diabetes, cancer, and Alzheimer’s disease.19–21 WHO acknowledges that obesity-related non-communicable diseases (NCDs) pose a significant threat to the 2030 Agenda for Sustainable Development. 22
Factors associated with central obesity included female sex, higher age groups, occupational status, such as housewives, self-employed workers, and government/private/non-public sector workers. 9 Skipping breakfast, genetics, physical inactivity, poor diet, stress, and lack of sleep were significantly associated with central obesity. 23 The most common risk factors that lead to the accumulation of visceral fat are a sedentary lifestyle, overeating, Cushing’s syndrome, alcoholism, and polycystic ovarian syndrome (PCOS).10,24,25
Several strategies are drafted to reduce the severity and burden of central obesity; engaging in regular physical activity, consuming a healthy diet that is low in saturated and trans fats, added sugars, and refined carbohydrates, managing stress, and getting enough sleep can help regulate hormones that control appetite and metabolism. Additionally, behavioral weight management interventions, such as those delivered in primary care settings, are effective for reducing central obesity.26,27
Central obesity is common among public sector workers because they sit for more than 5 hours at work, are physically inactive, and consume unhealthy diets and alcohol.28,29 Indeed, different strategies have been recommended; several findings are still showing the incremental trends of obesity, including central obesity, which were observed from global to local, specifically among public sector workers.1,8,23 Even though many efforts were made to reduce the magnitude and morbidity of obesity, central obesity is still increasing in developed and developing countries, including Ethiopia.30,31
The Ethiopian government has worked on the prevention and control of adult obesity by encouraging physical activity, promoting fruit and whole grain intake, educating on reducing processed meat intake, implementing prevention, and placing emphasis on mental health. 17 Even though different studies have reported the importance of workplace obesity intervention, no single study has been done on central obesity among public sector workers, particularly in our study area, since the focus of the Somali region is on undernutrition rather than obesity. Therefore, this study aims to assess the prevalence of central obesity and associated factors among adult public sector workers in regional bureaus in the Somali region of Ethiopia.
Methods and materials
Study design and setting
An institutional-based cross-sectional study was conducted from April 15–30, 2024, in Jigjiga town, Somalia’s regional state, Eastern Ethiopia. Jigjiga town is situated at a distance of 621 km from Addis Ababa. The total population of the town was 197,966, consisting of 102,529 men and 95,437 women. A total of 43 organizations (29 governmental, 6 private, and 10 NGOs) are found in the town. In Jigjiga town, there are around 7158 public sector workers. The city has one general hospital, one referral hospital, one primary hospital, three health centers, and 27 health posts.
Population and sampling
All adult public sector workers who were working in the Jigjiga town were the source population, whereas all adult public sector workers in the selected offices of the Jigjiga town during the study period were the study population. Adult public sector workers who worked for at least 6 months at the time of data collection were selected randomly and included in the study, whereas pregnant mothers and adult workers who were absent or on leave during data collection were excluded from the study. The sample size was determined using both a single and a double population proportion formula. The maximum sample size was achieved by using a single proportion formula

By considering a confidence level of 95%, a marginal error of 5%, 32 and the population proportion of 54.7% from the study conducted in Bedele town, Southwest Ethiopia. 28 After applying a design effect of 1.5 33 and a 10% non-response rate, the final sample size was determined to be 628.
In this study, a multistage sampling method was used. From all 28 public sectors in Jigjiga town, considering representation, the nine offices were randomly selected by lottery method. For selecting study participants (public sector workers) in the selected offices, proportional allocation, based on the number of Government employees in each Government sector, was used. Finally, sample sizes for each public sector were calculated based on the total number of public sector workers in each office, and then selected using simple random sampling by lottery method.
Data collection and quality control
The data were collected using standardized tools that were adapted from the WHO-Stepwise for non-communicable disease surveillance, the Ethiopian Demographic Health Survey, the WHO Global Physical Activity Questionnaires (GPAQs), and the Food and Agriculture Organization (FAO).34–36 The questionnaires consisted of socioeconomic, behavioral, diet-related, and physical activity questions, as well as anthropometric measurements of WC and HC.
Dietary pattern was evaluated using food frequency questionnaires (FFQs), which were adapted from the WHO stepwise and are used to measure the frequency of consumption of various food groups. Participants were asked to report how many times they consumed each week over the previous 3 months. 36 Waist circumference (WC) was measured using non-stretchable fixed tension tape, which was wrapped around the body at this point, parallel to the floor. Care was taken to adjust the tape without compressing the skin. The measurement was taken at the midpoint between the top of the anterior superior iliac crest and the lower margin of the least palpable rib along the mid-axillary line. The participant had to stand comfortably with their feet close together, their arms at their sides, and their body weight equally distributed while collecting the measurement. They were also required to wear light clothing. After a typical expiration, the measurement was made. Every measurement was made twice, and the average was determined when the measurements were within 1 cm of each other. The two measurements were taken again when there was a discrepancy of more than 1 cm. 37
Data was collected by four trained nursing professionals. Data collectors and supervisors received 2 days of training on the purpose and procedure of data collection related to this research by the principal investigator. They were assigned to each selected bureau and supervised by the principal investigator. Data was collected through a face-to-face interview of the participants using structured and interviewer-administered questionnaires. English version questionnaires were translated into the Somali language and back-translated to English to check for any ambiguity in language translation. A pretest was conducted on 5% of the sample size outside the study area before actual data collection, and a necessary modification was made to the instrument. Rechecking was made each day to confirm the reliability of the collected data. Data from each respondent was checked for completeness, clarity, consistency, and accuracy by the supervisor.
Data processing and analysis
All collected data were checked for completeness and internal consistency, and the data were coded and entered in the Epi Data 3.1 computer software package. After cleaning, the data were exported to SPSS version 26 for analysis. Descriptive statistical measures like mean and standard deviation were done, and the data were presented using frequency tables, figures, and graphs. Binary logistic regression was carried out to identify factors associated with central obesity. Accordingly, variables that fulfilled a p-value less than 0.25 in the bivariable binary logistic regression were considered for further multivariable logistic regression to control for possible confounding factors. In the multivariable binary logistic regression, the odds ratio along with a 95% confidence interval was used to present the association of the dependent and independent variables, and variables with a p-value of less than 0.05 were declared as statistically significant. The goodness of model fitness was assessed using the Hosmer-Lemeshow statistic (p = 0.7652). Multicollinearity tests were carried out to see the correlation between independent variables and checked by using the standard error and collinearity statistics (variance inflation factors >10 and standard error >2 was considered suggestive of the existence of multicollinearity. Missing data were minimal and handled using the Listwise deletion method.
Results
Socio-demographic characteristics of the respondents
A total of 623 public sector workers were enrolled in the current study, with a response rate of 99.2%. The age of the respondents ranged from 20 to 60 years, with a mean (+SD) of 34.8 (+7.2) years. The majority, 440 (70.6%) of respondents, were male. Nearly half, 43.0% of respondents, were married. Regarding educational level, the majority, 500 (80.3%), of respondents were degree holders, and about three-fourths (70.3%) of the study participants’ family size was <5. The majority, 576 (92.5%), of the respondents had a monthly income of between 3934 and 9055 Ethiopian Birr with a 20% tax rate (4001–7000) and 25% (7001–10,000) (Table 1).
Socio-demographic characteristics of public sector workers in Jigjiga town, Somali region, Eastern Ethiopia, 2024 (n = 623).

Behavior-related factors of respondents
Of the total participants, about three-fourths of 495 (79.4%) were nonsmokers, 597 (95.8%) of participants were non-alcohol consumers, and more than half, 384 (61.6%), of them were non-chewers. The majority of 553 (88.8%) respondents were physically inactive. More than half of the 429 (68.9%) respondents used public transportation while going to their workplace. More than half, 392 (62.9%) of respondents slept 7–8 h per day (Table 2).
Behavioral related factors of public sector workers in Jigjiga town, Somali region, Eastern Ethiopia, 2024 (n = 623).

Diet-related conditions of public sector workers
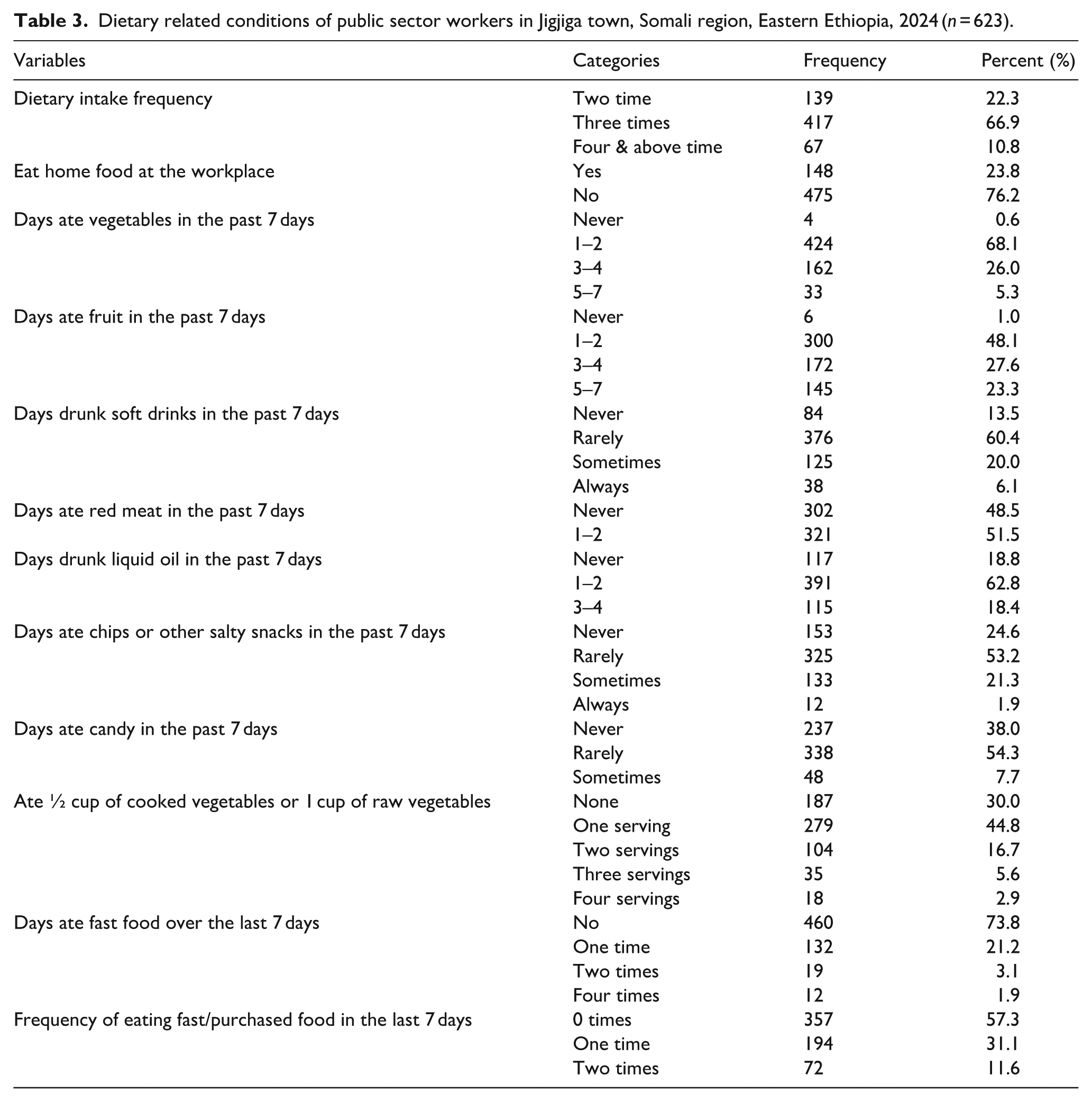
Of the total study participants, more than half, 417 (66.9%), reported that their dietary intake frequency per day was three times, and about three-fourths, 475 (76.2%), of them didn’t eat homemade food at the workplace. When assessing vegetable intake over the past week, approximately two-thirds, 424 (68.1%) of the participants consumed vegetables 1-2 times. Fruit consumption was also low, with 48.1% eating fruit 1–2 times. Regarding soft drink consumption, 60.4% reported drinking them rarely, while 13.5% never consumed soft drinks. Red meat was consumed by 51.5% of participants 1–2 times a week, while 48.5% reported never eating it. Additionally, 62.8% consumed liquid oil 1–2 times, and 53.2% rarely ate chips or salty snacks. Most participants (73.8%) did not eat fast food in the past week, with 57.3% reporting no purchase of fast food (Table 3).
Dietary related conditions of public sector workers in Jigjiga town, Somali region, Eastern Ethiopia, 2024 (n = 623).
Health conditions and work environment-related factors
Of the total respondents, about 59 (9.5%) reported they had hypertension, 35 (5.6%) of their work was stressful, 23 (3.7%) of them had DM, and 22 (3.5%) of the respondents reported that they had stress confirmed by a health professional (Figure 1).
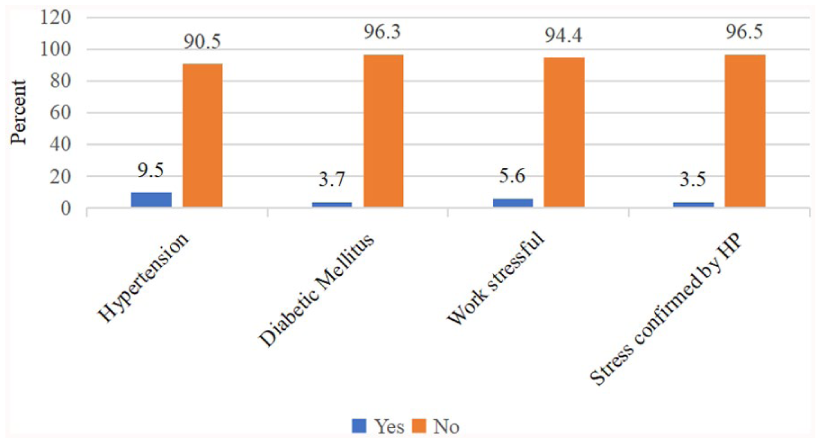
Health condition and work environment-related factors of public sector workers in Jigjiga town, Somalia region, Eastern Ethiopia, 2024.
The prevalence of central obesity among public sector workers
The current study revealed that the overall prevalence of central obesity was 266 (42.7%) with a 95% CI of 38.9%–46.6%, and central obesity was 39.1% and 51.4% among males and females, respectively (Figure 2).

The magnitude of central obesity among public sector workers in Jigjiga town, Somalia region, Eastern Ethiopia, 2024.
Factors associated with central obesity among public sector workers
In the bivariable analysis, variables such as sex, age categories, marital status, chat chewing, physical activities, mode of transportation, dietary frequency, frequency of drinking soda (soft drink), frequency of eating red meat, fasting frequency, having diabetes mellitus, and having stressful work were significantly associated with central obesity at a p-value < 0.25 (to include potentially important variables) and were candidates for multivariable binary logistic regression analysis.
However, in the final model of the multivariable binary logistic regression analysis, sex, physical activities, frequency of eating red meat, diabetes mellitus, and stressful work were found to be significantly associated with central obesity at a p-value < 0.05 among public sector workers in the study. Accordingly, the study revealed that public sector workers who are female were 1.78 times more likely to have central obesity compared to those who are male (AOR = 1.78, 95% CI = 1.22–2.59). Similarly, public sector workers who didn’t do physical activities were 1.84 times more likely to have central obesity than those who did physical activities (AOR = 1.84, 95% CI = 1.02–3.30). In addition, public sector workers who ate red meat 1–2 times per week were 1.57 times more likely to have central obesity compared to those who never ate red meat per week (AOR = 1.55, 95% CI = 1.03–2.37). Likewise, public sector workers who had no diabetes mellitus were 72% less likely to have central obesity than those who had diabetes mellitus (AOR = 0.28, 95% CI = 0.10–0.79). In addition, public sector workers whose work had no stress were 56% less likely to have central obesity than those whose work was stressful (AOR = 0.44, 95% CI = 0.20–0.96; Table 4).
Bi-variable and multivariable logistic regression analysis of factors associated with Central Obesity among public sector workers in Jigjiga town, Somali region, Ethiopia 2024 (n = 623).
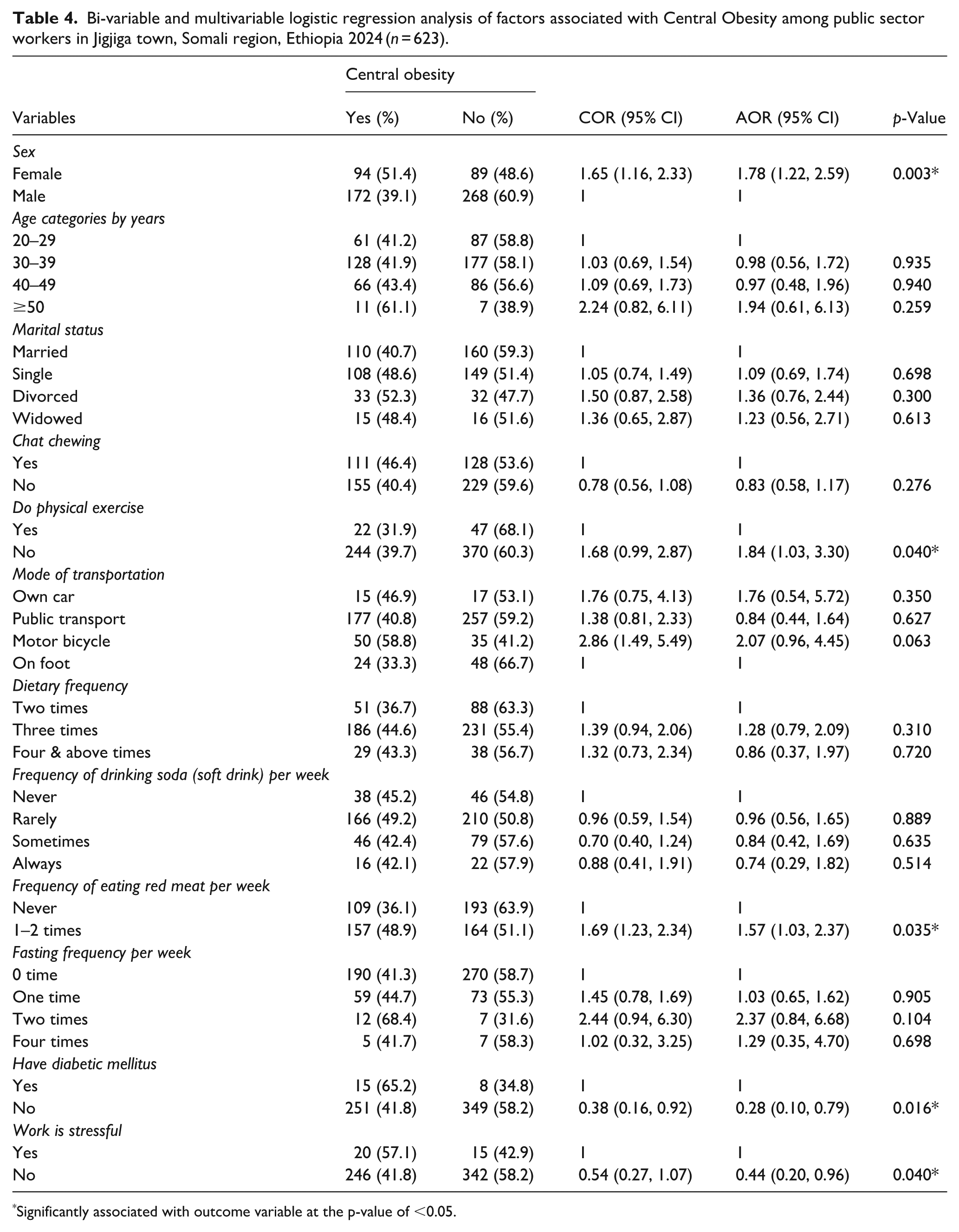
Significantly associated with outcome variable at the p-value of <0.05.
Discussion
The findings of this study showed that the prevalence of central obesity among public sector workers in the study area was 42.7% (95% CI: 38.9%–46.6%). This result was lower than the study conducted in Bedele town, which showed that central obesity among government workers was 54.7%. 28 Conversely, our study was higher than a study conducted in Adama, 24.2%, 38 and a study conducted in Addis Ababa, 29.5%. 39 This difference may be explained by a study conducted in Bedele, which used a cut point for WC lower than this study, which was not based on WHO cut points. However, for the higher magnitude, the difference may be due to environmental and lifestyle differences. Indeed, in Jigjiga, the availability of processed food at home was also significantly associated with processed food consumption, and so processed foods are a factor in central obesity. 40
Accordingly, our study also revealed that public sector workers who are female were more likely to have central obesity compared to those who are male. This finding is in line with similar studies conducted in Bedelle, southwest Ethiopia, 28 and a study done in Dire Dawa, eastern Ethiopia, 10 which showed that females are more exposed to central obesity than males. This is explicitly related to the fact that, due to biological differences, women by nature have a higher percentage of body fat compared to men, and hormonal changes that women experience throughout their lives can also significantly affect metabolism and fat distribution.41–43
The study also revealed that public sector workers who didn’t do physical activities were more likely to have central obesity than those who did physical activities. This finding is supported by similar studies that found that physical inactivity is a factor in central obesity among government workers.28,38,44 This is explicitly related to the fact that a lack of physical activity, caloric intake, and expenditure are not equal, which causes long-term adipose tissue accumulation, which is directly related to central obesity among individuals.43,45 Indeed, it is known that sedentary lifestyles, which are common among office workers, can contribute significantly to the accumulation of abdominal fat because prolonged periods of inactivity can lead to weight gain and fat accumulation, particularly around the abdomen. 46
In addition, this study showed that public sector workers who ate red meat 1–2 times per week were more likely to have central obesity compared to those who never ate red meat. This finding is supported by the study that revealed consuming red meat is associated with an increased risk of central obesity, which is the accumulation of fat around the abdomen.47–49 One possible explanation may be that red meat is often high in calories, and contains significant amounts of saturated fats, which are solid at room temperature; as a result, a high intake of saturated fats is linked to increased body fat and central obesity.50–52
Moreover, our study revealed that public sector workers who had no diabetes mellitus were less likely to have central obesity than those who had diabetes mellitus. This finding aligns with studies that have found diabetes mellitus to be a significant factor in weight gain, including central obesity, among individuals.38,53,54 This is related to the fact that in type 2 diabetes, the body becomes resistant to insulin, which is the hormone responsible for regulating blood sugar levels. To compensate, the pancreas produces more insulin. The effect of these high levels of insulin can promote fat storage, especially around the abdomen. 55 When blood sugar levels are high, the body may signal hunger more frequently, leading to increased food intake or appetite, and individuals may adopt diets that result in weight gain and the development of central obesity. Indeed, sometimes insulin therapy can lead to weight gain as the body starts to utilize sugar, fat, and protein more effectively, which directly causes central obesity among individuals. 56
Finally, the study revealed that public sector workers, whose work had no stress, were less likely to have central obesity than those whose work was stressful. This finding is in line with previous studies.57–59 This could be related to the fact that when individuals are under chronic stress, their bodies produce higher levels of the hormone cortisol; this can disrupt metabolism and contribute to weight gain. 60 Stress can also influence eating behaviors, often leading to the consumption of diets that are high in sugar and fat; this combination of physiological and behavioral responses to stress can significantly contribute to central obesity.61,62
Limitations of the study
This study is not without limitations. Anthropometric measurements are also prone to errors; however, this study was conducted with the highest precautions in training anthropometric data collection, equipment calibration, and standardization of procedure to minimize the possibility of errors. This study delimits the relevance of its results to public sector workers in eastern Ethiopia, which cannot be generalized to the general population of Ethiopia. Additionally, the study was interviewer-administered; there may be a risk of social desirability and recall bias.
Conclusion
The findings from this study indicated that nearly four out of ten public sector workers had central obesity. Factors such as sex, physical inactivity, eating red meat, diabetes mellitus, and stressful work were found to be significantly associated with central obesity. Therefore, follow-up on the health and work environment, as well as behavioral change interventions, would be important in reducing central obesity among public sector workers.
Supplemental Material
sj-docx-1-phj-10.1177_22799036251388562 – Supplemental material for Central obesity and its associated risk factors among public sector workers in Jigjiga Town, Somali Region, Ethiopia: A cross-sectional study
Supplemental material, sj-docx-1-phj-10.1177_22799036251388562 for Central obesity and its associated risk factors among public sector workers in Jigjiga Town, Somali Region, Ethiopia: A cross-sectional study by Bashir Abdi Hussein, Tara Wilfong, Alemayehu Tesfaye, Dawit Firdisa and Aboma Motuma in Journal of Public Health Research
Footnotes
Acknowledgements
We acknowledged Haramaya University Colleges of Health and Medical Sciences Institutional Health Research Ethical Review Committee for giving the ethical clearance. We would also like to thank the data collectors and supervisors for their commitment during data collection.
Acronyms
AOR: Adjusted Odds Ratio, BMI: Body Mass Index, CVD: Cardiovascular Diseases, DM: Diabetic Mellitus, DHS: Demographic Health Survey, EDHS: Ethiopian Demographic Health Survey, NCD: Non-Communicable Disease, WC: Waist Circumference, WHO: World Health Organization
Ethical considerations
Ethical clearance was obtained from the Institutional Health Research and Ethics Review Committee, reference number (IHRERC/087/2024) of Haramaya University, College of Health and Medical Science. A formal letter from Haramaya University, CHMS, was submitted to each selected bureau. Also, a support letter was obtained from the administrative heads of the bureau.
Consent to Participate
Informed, voluntary, written, and signed consent was obtained from study subjects. All study participants were informed about the purpose of the study and the benefits and risks of the study. The participant’s right to self-determination and autonomy was respected. To protect the confidentiality of the information, names and ID numbers were not recorded on the questionnaire.
Author contributions
BA, AM, and TW were involved in the conception and design, acquisition of data, or analysis and interpretation of data. DF contributed to data analysis, writing, and editing the document. AT gave valuable ideas for the manuscript and revised it critically for important intellectual content. Finally, all authors read and approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.