
Abstract
Background:
Hay fever cases, driven by factors such as global warming, are increasing globally, with Japanese cedar (JC) pollen being the primary allergen in Japan. While pharmacological therapies are available, their success heavily depends on patients’ preventive behaviors, which remain poorly documented. This study examines the relationship between symptom severity and preventive behaviors during the JC pollen season.
Design and methods:
This single-center, observational study included 161 new patients diagnosed with JC pollen allergy from January to March 2017. Patient data were collected through interviews and analyzed for severity using a five-point symptom scale and total Nasal Symptom Scores. Preventive behaviors, including preemptive antihistamine use, allergen immunotherapy, and pre-season consultations, were evaluated. Time-series analysis assessed trends in severe cases over the pollen season.
Results:
Patients who sought pre-season consultations were predominantly male (p = 0.006) and more likely to use preemptive antihistamines (p < 0.001) or allergen immunotherapy (p = 0.006). Severe symptoms were recorded in 38 patients, none of whom engaged in preventive behaviors, and only 10.5% sought pre-season consultations. Time-series analysis showed a daily increase of 6% severe cases after pollen season onset (p = 0.0064). Early preventive behaviors, such as preemptive antihistamine use (p = 0.007) and pre-season consultations (p < 0.001), significantly reduced severe cases.
Conclusions:
The study highlights the importance of early preventive measures to reduce symptom severity and improve patient outcomes. Promoting preventive behaviors could alleviate the growing economic burden of hay fever and enhance public health strategies globally.
Keywords
Significance for public health
Hay fever (seasonal allergic rhinitis) presents a significant public health challenge, as it not only reduces patients’ quality of life but also imposes considerable economic burdens. Globally, the prevalence of hay fever is increasing, driven by factors such as climate change. In Japan, universal health coverage facilitates low-cost access to seasonal allergy care, a system not commonly available in many countries. This study may offer important public health insights with potential applications in other healthcare systems. In Japan, rising healthcare costs associated with hay fever have become a critical social issue. The primary cause, Japanese cedar pollen, has prompted the development of effective, guideline-recommended preventive therapies. However, the successful implementation of these therapies relies heavily on patients’ proactive engagement and preventive awareness.
This study examines the relationship between symptom severity and preventive behaviors in hay fever patients, emphasizing the importance of such actions in preventing symptom exacerbation and lowering healthcare costs. These findings have substantial public health implications, addressing health disparities and contributing to the reduction of societal costs associated with hay fever.
Introduction
Hay fever (seasonal allergic rhinitis) is classified as a type I allergy and negatively affects patients’ quality of life, leading to economic losses due to decreased productivity. 1 Globally, the number of patients with hay fever is increasing annually because of factors such as global warming. 2 In Japan, the rising healthcare costs associated with hay fever have become a significant social issue, estimated at $2.3 billion in 2019.3,4
The primary cause of hay fever in Japan is Japanese cedar (JC) pollen. 3 Effective preventive therapies against JC pollen, recommended by guidelines, include allergen immunotherapy before the pollen season 5 and the preemptive use of antihistamines from the onset of initial symptoms.6,7
Preventing the exacerbation of hay fever symptoms is crucial for improving patients’ quality of life and reducing healthcare costs. 8 Although pharmacological therapies have been extensively researched,5,6,9 the success of these interventions relies heavily on patients’ proactive behaviors and preventive awareness. 10 However, comparative studies of preventive behaviors are lacking. In this study, preventive behaviors were operationally defined as a history of pre-season physician consultations, use of antihistamines before symptom onset, and receipt of allergen immunotherapy. In addition, because Japan provides relatively easy access to insured medical care compared to many other countries, understanding how these behaviors impact disease severity in such a context offers important lessons for other healthcare systems with higher treatment barriers.
This study aimed to investigate the relationship between symptom severity in new patients during the JC pollen season and their preventive behaviors.
Materials and methods
Study period and patients
This study included all patients who visited the Pharmacy for the first time during the JC pollen season, from January 13 to March 15, 2017, to obtain medication after being diagnosed with JC pollen allergy at a clinic. No exclusion criteria were applied; all patients interviewed by pharmacists for operational improvement were included and analyzed without exception.
Evaluation and comparison of patient severity
The severity of JC pollen allergy was assessed according to the Japanese guidelines for allergic rhinitis. 7 Pharmacists evaluated the severity based on symptoms such as the frequency of sneezing, nasal discharge, nasal congestion, and impact on daily life using a five-point scale (0 = no symptoms, 1 = mild, 2 = moderate, 3 = severe, and 4 = very severe). Patients were classified as having severe symptoms if their scores fell within the severe-to-very severe range. Additionally, the total Nasal Symptom Score (NSS), ranging from 0 to 12, was calculated and analyzed. 6
Measurement of JC Pollen Dispersal
From January 1, 2017, daily measurements of JC pollen were conducted using a Durham sampler installed on the rooftop of the Apotex Corporation, Apco Higashi-Onomichi Pharmacy. The first 2 consecutive days with more than 1 grain/cm² were defined as the start of the pollen dispersal period. 6 The pollen season was defind in accordance with Galán et al.′s recommendation that the season begins when the cumulative pollen count exceeds a defined threshold over several consecutive days. 11 Pollen counts were measured using a Durham sampler, which, while widely used in Japan, differs from the Hirst-type volumetric spore trap recommended in international standards such as the CEN 16869:2019. 11 Data recovery using Hirst-type traps was not possible in this retrospective setting.
Evaluation items for patients
Patient backgrounds and JC pollen prevention behaviors were collected through interviews conducted by pharmacists. The interview details are shown in Supplemental Figure S1. Patient characteristics included age and sex. JC pollen prevention behaviors included the preemptive use of antihistamines before the first visit, allergen immunotherapy (Supplemental Figure S2), and medical visits before pollen dispersal. To investigate the relationship between initial visit severity and preventive behaviors before and after pollen dispersal, patients were divided into pre- and post-dispersal visit groups for comparison (Supplemental Figure S3). Additionally, the temporal relationship between the number of patients with severe hay fever and the start of the JC pollen season was analyzed. Furthermore, patients were categorized into mild (no symptoms to moderate) and severe (severe to very severe) groups to compare the proportion of patients with severe JC pollen allergy in relation to prevention behaviors (Supplemental Figure S4). 12
Statistical analyses
Categorical data were analyzed using Fisher’s exact test for binary variables and the Mann–Whitney U-test for continuous variables. Pairwise comparisons among groups (no preventive behaviors, preemptive use of antihistamines, allergen immunotherapy, and pre-dispersal visits) were performed using Fisher’s exact test, with p-values adjusted using Holm’s method. Interrupted time-series analysis (ITSA) with generalized linear regression was conducted over two periods (pre-dispersal: January 13, 2017, to February 16, 2017; post dispersal: February 17, 2017, to March 17, 2017). The model included intercept (β0), baseline trend (β1), level change post-dispersal (β2), and trend change post-dispersal (β3). 13 The dependent variable was the number of severe JC pollen patients at their initial visit during the JC pollen season, with post-dispersal time as the independent variable, evaluating changes in trends. Statistical significance was set at p < 0.05. Analyses were performed using EZR version 1.32. 14
Ethics statement
This study involved the secondary use of interview data originally collected by community pharmacists for internal quality improvement purposes. For this secondary use of data, the need for written informed consent was waived in accordance with the Ethical Guidelines for Medical and Health Research Involving Human Subjects in Japan. Instead, participants were notified about the study and given the opportunity to opt out, ensuring their right to refuse participation.
Results
Characteristics of JC pollen patients
Among the 161 patients included in the analysis, the initial severity distribution was as follows: asymptomatic, 25% (n = 40), mild 35% (56), moderate 17% (27), severe 17% (27); and very severe 7% (11). The NSS and degree of interference with daily life were significantly lower in the mild group (1.0 vs 7.0, p < 0.001 and 0.0 vs 1.5, p < 0.001, respectively; Table 1).
Patient demographics and symptom severity of JC pollen allergies.
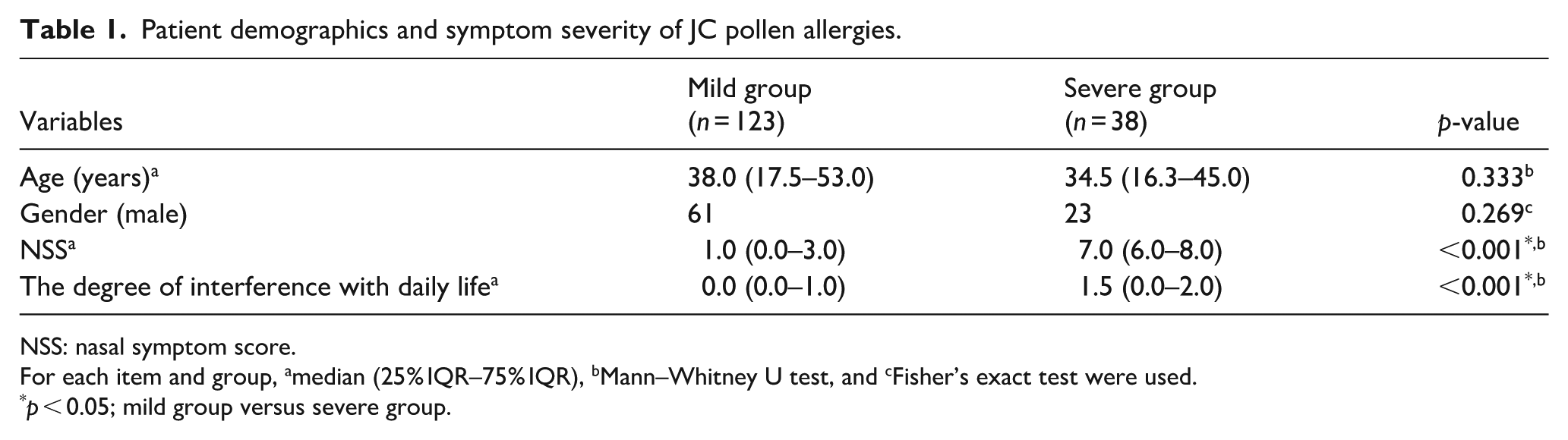
NSS: nasal symptom score.
For each item and group, amedian (25% IQR–75% IQR), bMann–Whitney U test, and cFisher’s exact test were used.
p < 0.05; mild group versus severe group.
JC pollen dispersal
In 2017, the total JC pollen count was 2194 grains/cm². The JC pollen dispersal period lasted 64 days, from February 17 to April 21, with a pollen count consistent with the national average (Supplemental Figure S5).
Evaluation of initial severity and preventive behavior in JC pollen patients before and after pollen dispersal
Among the 161 initial patients during the JC pollen season, those who visited before dispersal were more likely to be male and preemptively use antihistamine prophylaxis and allergen immunotherapy (48.8% vs 51.2%, p = 0.006; 83.3% vs 16.7%, p < 0.001; 87.5% vs 12.5%, p = 0.006; Table 2). The NSS and interference with daily life were higher in the pre-dispersal visit group (1.0 vs 3.0, p < 0.001; 0.0 vs 0.0, p < 0.001). The severe group had a higher proportion of post dispersal visits (10.5% vs 89.5%, p < 0.001; Table 2).
Relationship between initial severity and prevention behavior in patients with JC pollen before and after pollen dispersal.

NSS: nasal symptom score.
For each item and group, amedian (25% IQR–75% IQR), bMann–Whitney U test, and cFisher’s exact test were used.
p < 0.05; pre-dispersal visit group versus post-dispersal group.
Temporal relationship between JC pollen dispersal and severe patients
ITSA results showed an increase of 6% severe cases per daily after JC pollen dispersal began (95% CI: 1.02–1.11; p = 0.0064). However, no immediate change was observed, with an initial severe case count change of 3.15 (95% CI: 0.5–36.13; p = 0.2747; Figure 1).

Trends in severe hay fever patients at their initial visit during the Japanese cedar pollen season in 2017.
Severity evaluation of JC pollen allergy as per dispersal season
Among the 161 initial patients diagnosed with allergy during the JC pollen season, 38 were classified as severe (including very severe) with no use of antihistamine prophylaxis or allergen immunotherapy. Four of the 38 patients (10.5%) visited before the JC pollen dispersal. All 18 patients who received oral antihistamines also received olopatadine hydrochloride treatment. Compared to those without preventive behaviors, those on preemptive use of antihistamines had a lower proportion of severe cases (p = 0.006593). Similarly, those who visited before the JC pollen dispersal had a lower proportion of severe cases (p < 0.001; Table 3).
Relationship between preventive behaviors and symptom severity in patients with Japanese Cedar (JC) pollen allergies.

For each item and group, apairwise comparisons were performed using Fisher’s exact test, with p-values adjusted using Holm’s method. Some of the patients have implemented multiple preventive measures.
1p = 0.006593, *2p = 0.00005459.
Discussion
This study revealed the novel finding that male patients and those engaging in preventive behaviors were more likely to visit before JC pollen dispersal. The association between preventive actions and reduced severity in patients with pollen allergies is consistent with previous research. 7 In addition, the number of severe cases increased over time after the dispersal of the JC pollen. Seasonal preventive actions, such as taking antihistamines before the first visit and consulting a doctor before the JC pollen season, are more effective than continuous measures for preventing severe symptoms.
Interestingly, our study identified a higher rate of predispersal visits among male participants within our sample. This finding contrasts with general reports suggesting higher health consciousness among females. 15 However, this trend may reflect specific characteristics of our study population or regional cultural factors. Further research is necessary to confirm this trend and investigate underlying causes. Additionally, the study found that patients using preventive antihistamines and allergen immunotherapy had higher rates of pre-dispersal visits, indicating strong preventive awareness. Previous reports have shown that engaging in multiple health behaviors leads to better health outcomes, which likely contributes to these findings. 16
Previous reports have suggested that the incidence of allergic rhinitis increases with increasing antigen levels. 7 In this study, the number of severe pollinosis cases increased over time after JC pollen dispersal. None of the 38 severe cases used preventive antihistamines or immunotherapy, which potentially affected the time-series changes. Four patients (10%) had severe disease despite visiting the hospital before dispersal, likely because of discrepancies between the fixed observation site and their residences. 17 Early preventive behaviors are therefore recommended. Future studies could explore the role of pharmacists and weather forecasters in effectively disseminating dispersal information to promote early prevention.
This study did not find that allergen immunotherapy statistically reduced hay fever severity compared to no prophylaxis, possibly because of the small sample size. The effects of immunotherapy last 2 years after 3 years of treatment, 17 but only 1 year if the treatment lasts 2 years. 18 Adherence of at least 70% was required. 19 Continuation for at least 3 years is necessary, making this method more difficult to adhere to compared to other preventive methods.
From a public health and international perspective, the universal healthcare system in Japan lowers barriers to clinic access, facilitating early consultation and intervention. In contrast, the more limited insurance coverage in many other countries may restrict access to care, highlighting global health disparities. Cost-effective early interventions may reduce long-term medical costs and productivity losses. 8 A prior Japanese Cabinet Office report estimated the economic burden of hay fever, including direct medical costs and indirect productivity losses, at $2.3 billion annually, 4 Early preventive care may help to reduce these costs.
This study has several limitations. First, it was conducted at a single institution without a predetermined sample size. However, a post hoc power analysis (effect size w = 0.3, α = 0.05, power = 0.80, df = 3) indicated that 122 participants were required; this study included 161, satisfying this criterion. Second, pollen counts were measured using the Durham sampler, which is widely applied in Japan, but less sensitive than the internationally recommended Hirst-type volumetric sampler. This may have led to an underestimation of airborne pollen, which could have affected the classification of dispersal periods. Third, although the study compared different preventive behaviors, it did not explore which methods enhance preventive awareness and actions among patients with hay fever, highlighting the need for future research.
This study emphasizes the importance of early preventive behaviors before pollen dispersal to alleviate the symptoms of hay fever. In conclusion, seasonal preventive actions, such as pre-pollen consultation and antihistamine use, are more effective in preventing severe symptoms than continuous measures and may help reduce medical costs. After pollen dispersal, prompt use of preventive measures is crucial. Preventive actions, such as consulting a doctor before the JC pollen season or taking antihistamines before the first visit, are effective in preventing severe symptoms and may improve patients’ quality of life and reduce healthcare costs.
Conclusion
Early preventive actions, including pre-season consultations, antihistamines, and immunotherapy, were linked to milder cedar pollen allergy symptoms. Severe cases were observed only among those who did not engage in these behaviors. The time-series analysis indicated a narrow window for effective intervention after pollen dispersal begins.
Supplemental Material
sj-docx-1-phj-10.1177_22799036251380784 – Supplemental material for Comparative study on severity and preventive behaviors of Japanese cedar pollen allergy during pollen scattering season: Single-center analysis
Supplemental material, sj-docx-1-phj-10.1177_22799036251380784 for Comparative study on severity and preventive behaviors of Japanese cedar pollen allergy during pollen scattering season: Single-center analysis by Tatsuya Tai, Masahiro Watanabe, Sayaka Yamashita, Keiji Okada, Hiroyuki Namba, Takaaki Yamamoto, Kei Kawada, Takahiro Motoki, Hiroaki Tanaka and Shinji Kosaka in Journal of Public Health Research
Supplemental Material
sj-pptx-2-phj-10.1177_22799036251380784 – Supplemental material for Comparative study on severity and preventive behaviors of Japanese cedar pollen allergy during pollen scattering season: Single-center analysis
Supplemental material, sj-pptx-2-phj-10.1177_22799036251380784 for Comparative study on severity and preventive behaviors of Japanese cedar pollen allergy during pollen scattering season: Single-center analysis by Tatsuya Tai, Masahiro Watanabe, Sayaka Yamashita, Keiji Okada, Hiroyuki Namba, Takaaki Yamamoto, Kei Kawada, Takahiro Motoki, Hiroaki Tanaka and Shinji Kosaka in Journal of Public Health Research
Footnotes
Acknowledgements
The authors thank the staff of Apotex Corporation, Apco Higashi-Onomichi Pharmacy (Onomichi, Hiroshima, Japan) for their efforts in collecting patient information.
Ethical considerations
This study protocol, including this opt-out procedure, was approved by the Institutional Review Board of the Kagawa Prefecture Pharmacists Association (Approval No. 2024KAYAKUDAI6GOU).
Consent to participate
Informed consent was obtained through an opt-out method on the website in accordance with the ethical guidelines for medical and biological research involving human subjects in Japan.
Author contributions
All authors meet the ICMJE authorship criteria. Tatsuya Tai participated in the design of the study, collected the study data, and prepared the manuscript. Takaaki Yamamoto, Masahiro Watanabe and Kei Kawada participated in the study design and editing of the manuscript. Takahiro Motoki, Keiji Okada, Hiroyuki Nanba, Sayaka Yamashita, Hiroaki Tanaka, and Shinji Kosaka assisted in the preparation of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
Data are available upon request and subject to privacy, ethics, and other restrictions.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.