
Abstract
Background:
Although previous studies have identified worry about COVID-19 as an important determinant of COVID-19 vaccine-related intentions and behaviors, the exact mechanism by which worry influences these intentions and behaviors is still being investigated.
Design and method:
An online survey was conducted among 310 U.S. university students from mid-June to mid-July 2021, measuring worry about COVID-19, COVID-19 risk perception (perceived probability and perceived severity), vaccine perception (perceived vaccine safety and perceived vaccine effectiveness), and vaccine acceptance, along with demographics. Three models were tested using structural equation modeling (SEM): (1) worry, risk-perception, and vaccine-perception variables influence vaccine acceptance simultaneously; (2) worry partially mediates the relationships between risk/vaccine-perception variables and vaccine acceptance; (3) risk- and vaccine-perception variables partially mediate the relationship between worry and vaccine acceptance. All models are the originally specified models.
Results:
Results of SEM analyses suggest that Model (3) fit the data best (CFI = 1.000, TLI = 1.000, and RMSEA = 0.000). SEM analysis for Model (3) found that perceived probability of contracting COVID-19 is negatively, worry about COVID-19 is positively, and perceived vaccine safety (the strongest predictor) is positively associated with vaccine acceptance. Perceived severity of contracting COVID-19 and perceived vaccine effectiveness are non-significant predictors. Worry indirectly affects vaccine acceptance through perceived probability (negative) and perceived vaccine safety (positive).
Conclusions:
COVID-19 vaccine campaigns targeting college students should emphasize vaccine safety, use reasonable worry as an emotional cue, and avoid overemphasizing the likelihood of contracting COVID-19.
Significance for public health
First, addressing concerns about vaccine safety is crucial. Clear and transparent campaigns about vaccine safety can significantly motivate college students to accept COVID-19 vaccines. This aligns with Scott et al.’s (2021) review, which emphasized addressing vaccine mistrust to foster acceptance. 1 Second, highlighting the severity of COVID-19 or the effectiveness of the vaccine may not significantly influence vaccine acceptance among college students. Third, the counterintuitive finding that a higher perceived probability of contracting COVID-19 is associated with lower vaccine acceptance cautions against overemphasizing infection likelihood. Specifically, placing excessive focus on the probability of infection may unintentionally lead to a reduction in college students’ desire to get vaccinated. Finally, instilling a reasonable level of worry about COVID-19 is beneficial. When maintained at a reasonable level, worry about COVID-19 not only directly motivates college students to embrace vaccination, but also positively shapes their perceptions of vaccine safety, ultimately leading to increased vaccine acceptance.
Introduction
The COVID-19 pandemic was declared a national emergency in the U.S. on March 13, 20202; by May of 2022, the U.S. death toll had surpassed 1 million. 3 Although COVID-19 vaccines have been available since the summer of 2021, and they are the best defense against COVID-19 according to several health organizations, 4 their widespread acceptance remains a critical concern. As of the final CDC update on May 11, 2023, 81.4% of the U.S. population has received at least one dose of the COVID-19 vaccine. 5 However, this means that roughly 20% of the population had yet to receive even a single shot. Identifying factors that influence Americans in accepting or declining COVID-19 vaccines is essential for preparing against future outbreaks of similar pandemics.
Worry about COVID-19 has been identified as an important determinant of COVID-19 vaccine-related intentions and behaviors. Studies conducted in the U.S. have found that lower levels of worry about becoming infected with COVID-19 predict vaccine delay, 6 while higher levels of worry are associated with full vaccination status. 7 Among the American Indian/Alaska Native/Native American populations, worry about getting COVID-19 has also been identified as a significant predictor of willingness to receive a COVID-19 vaccine. 8 Similar findings have also been reported in non-U.S. samples, such as in the Netherlands, 9 Italy, 10 and Canada,11,12 where worry about COVID-19 has been positively associated with vaccination intention or uptake, and lower levels of worry have predicted vaccine hesitancy.
Although the above studies have consistently revealed an association between worry about COVID-19 and vaccination intentions or behaviors, most have not examined the potential theoretical mechanisms underlying this relationship. Among the above studies, it appears that only Hilverda and Vollmann (2021) have explored such a mechanism, suggesting that worry about COVID-19 mediates the relationship between perceived severity of the disease (a component of cognitive risk perception) and vaccination intention. 9 However, they did not examine whether cognitive risk perception may instead mediate the relationship between worry and vaccination intention. Thus, the present study seeks to address this gap by exploring several theoretical mechanisms through which worry about COVID-19 may influence COVID-19 vaccination intentions.
Theoretical frameworks
Individuals’ decisions to accept the COVID-19 vaccine are likely to be influenced not only by cognitive evaluations, such as perceived susceptibility and severity, but also by affective responses (i.e. feelings). 13 Accordingly, theoretical models that incorporate both cognitive and affective mechanisms provide a more comprehensive framework for understanding vaccination behavior.
The Health Belief Model (HBM) proposes that health behaviors are influenced by perceived susceptibility, perceived severity, perceived benefits and barriers, and self-efficacy (Rosenstock et al., 1988). 14 While affective components such as fear or worry are not formally defined as constructs in HBM, they are considered to function as “cues to action”—external or internal stimuli that may trigger health-related behavior. 15 HBM does not assume a direct or central role for feelings in behavior prediction; instead, emotional responses are thought to exert their influence indirectly, through cognitive appraisals.
Protection Motivation Theory (PMT) and the Extended Parallel Process Model (EPPM) explicitly incorporate affective responses—specifically fear—as an important construct within their models.16,17 These models propose that fear is elicited by fear appeals and influences behavior through cognitive pathways. In both models, cognitive appraisals (e.g. perceived probability, perceived severity) mediate the effects of fear on protective motivations/intentions/behaviors.16,17 Thus, while fear is recognized as an important construct in PMT and EPPM, its role remains subordinate to cognitive evaluation.
An important distinction between PMT/EPPM and HBM is that the former explicitly model fear as an emotional construct, while HBM treats feelings more implicitly. Moreover, PMT/ EPPM are narrowly focused on fear, whereas HBM allows for the consideration of a broader range of emotional cues, though not formally defined within the model.
The Risk-as-Feelings hypothesis differs fundamentally from the above theories by proposing that (1) feelings have a direct effect on judgments and decisions which “need not be cognitively mediated,” (as opposed to the above theories, which all assume that feelings are mediated by cognitions); (2) feelings mediate, at least partially, the relationship between cognitive evaluations of risk and behavioral decisions/behaviors (again, the opposite relationship posited by the above theories; p. 272). 13
Taken together, these distinctions raise important questions: In the context of COVID-19 vaccination, do feelings and cognitive beliefs each have a direct influence on behavior/intention? Is behavior/intention primarily driven by cognitive beliefs that mediate emotional responses, or by emotional responses that mediate cognitive beliefs? The current study seeks to empirically test these competing assumptions.
Worry about COVID-19
The present study focuses on worry, rather than other emotional responses, for several reasons. First, empirical evidence indicates that worry was one of the most prevalent emotional responses during the COVID-19 pandemic, surpassing other negative emotions including sadness, anger, and depression. 18 This suggests that worry may well reflect the public’s dominant affective experience during prolonged health crises like COVID-19.
Second, while fear is a central construct in both Protection Motivation Theory (PMT) and the Extended Parallel Process Model (EPPM), it is “a present-oriented and short-lived response to an identifiable and specific threat” (p. 190). 19 In contrast, worry is future-oriented and tends to persist over time.20,21 It typically arises in response to uncertain and potentially threatening outcomes that may or may not occur, making it particularly relevant during the COVID-19 pandemic—a prolonged and evolving crisis marked by ambiguity and unpredictability. 22 Given these characteristics of the pandemic, worry—rather than fear—was more likely to emerge as the dominant and enduring emotional response.
Third, worry has consistently been identified as a key emotional factor predicting preventive health behaviors, including vaccination.23,24 In the context of COVID-19, many studies have found that worry about COVID-19 is positively associated with vaccine intentions and uptake.6,7 These findings highlight worry as a robust predictor across different health contexts, making it a theoretically and practically relevant emotional response to examine for vaccination.
By focusing on worry, the present study aims to capture an emotional construct that was not only prevalent and enduring during the COVID-19 pandemic, but also theoretically appropriate for explaining protective behaviors (e.g. vaccination) that emerge in response to long-term uncertain health threats.
COVID-19 risk perception and vaccine perception
In efforts to predict COVID-19 vaccination intentions and behaviors, a substantial body of research has focused on cognitive factors such as risk perception—defined as individuals’ beliefs about the probability and severity of contracting COVID-199,25—and vaccine perception, which includes beliefs about vaccine safety and effectiveness. 11 These cognitive factors are often examined alongside emotional responses, such as worry about COVID-19.
Risk Perception of COVID-19
Several studies have examined how individuals’ COVID-19 risk perception influences their willingness or intention to receive a vaccine. Chen et al. (2023) found that perceived severity of COVID-19 was a significant predictor of vaccination willingness, whereas perceived susceptibility (i.e. the perceived likelihood/probability of getting infected by COVID-19) was not. 8 Similarly, Russo et al. (2023) reported that perceived severity of COVID-19, but not perceived susceptibility, predicted COVID-19 vaccine intentions. 10 These findings suggest that individuals may be more motivated to vaccinate when they believe the consequences of infection are serious, regardless of how likely they feel they are to contract the virus. In contrast, Hilverda and Vollmann (2021) found no significant direct effect of either perceived susceptibility or perceived severity of COVID-19 on vaccination intentions. 9 These findings highlight inconsistencies in the literature and suggest that additional research needs to be conducted.
Vaccine perception: Safety and effectiveness
A second major focus in the literature has been individuals’ beliefs about the safety and effectiveness of COVID-19 vaccines. Coleman et al. (2024) observed that concerns about both safety and effectiveness were associated with increased vaccine hesitancy. 11 Latkin et al. (2021) similarly found that concerns about vaccine side effects, coupled with low confidence in the vaccine’s efficacy, significantly predicted delays in receiving COVID-19 vaccines. 6 Karlsson et al. (2021) further demonstrated that perceived vaccine safety was the strongest predictor of COVID-19 vaccination intentions, with COVID-19 risk perception playing a minor role. 26 Notably, they also found that worry about falling ill with COVID-19 did not significantly predict vaccination intentions, highlighting the primacy of vaccine-specific beliefs over negative emotional responses in shaping those intentions.
Although findings vary across studies, a consistent pattern emerges: cognitive beliefs—including perceived susceptibility to COVID-19, perceived severity of COVID-19, and perceived vaccine safety and effectiveness—as well as COVID-19-related worry, appear to play important roles in shaping COVID-19 vaccination intentions and behaviors. However, these predictors have often been studied in isolation or in limited combinations, without an integrated framework that jointly examines their influence.
The present study seeks to address this gap by simultaneously examining multiple cognitive and affective predictors of COVID-19 vaccination acceptance—namely, perceived probability, perceived severity, vaccine safety and effectiveness perceptions, and worry about COVID-19. In doing so, it aims to provide a more comprehensive understanding of how these factors collectively shape vaccine decision-making.
College students
The present study focused on the college student population for three reasons. First, college students are considered at higher risk for COVID-19 transmission due to their frequent social interactions in shared living spaces, classrooms, and campus events, which facilitate the spread of the virus.27,28 Second, although college students are generally younger and, therefore, more likely to experience mild symptoms or even remain asymptomatic after infection, they can unknowingly transmit the virus to others, including individuals at greater risk for serious illness or death—such as older adults or those with underlying health conditions. 29 Third, research has indicated relatively high levels of vaccine hesitancy30,31 and low motivation to get vaccinated among college students. 32 For instance, in a study conducted at a Midwestern university in November 2021, Wotring et al. (2022) found that 50% of student participants were unvaccinated; among them, 49% reported no intention to get vaccinated, and 22% were undecided. 31
Given the role of the college student population in transmission dynamics and the evidence of their vaccine hesitancy, it is important to understand and address college students’ intentions or acceptance toward COVID-19 vaccination. Promoting vaccine uptake across all population sectors—including college students—is essential for preventing future pandemics. Therefore, the present study specifically examines the college student population.
Research questions
To explain the relationships among worry about COVID-19, COVID-19 risk perceptions (including perceived probability and perceived severity), vaccine perceptions (including perceived safety and perceived effectiveness), and vaccine acceptance among college students, the present study proposes three competing path models, drawing upon the theoretical frameworks reviewed above: (1) worry, the two risk-perception variables, and the two vaccine-perception variables influence vaccine acceptance simultaneously (see Figure 1); (2) worry partially mediates the relationships between the risk-perception variables/vaccine-perception variables and vaccine acceptance (see Figure 2); (3) the risk-perception and vaccine-perception variables partially mediate the relationship between worry and vaccine acceptance (see Figure 3). After the best-fitting model is identified, the current study also aims to investigate the direct or indirect effects of worry, COVID-19 risk perception, and vaccine perceptions on COVID-19 vaccine acceptance.

Hypothesized model (1).

Hypothesized model (2).

Hypothesized model (3).
The following research questions are posed:
RQ1: Which of the three proposed models best fit the data?
RQ2: Based on the best-fitting model, what are the direct and indirect effects of worry about COVID-19, risk perception of COVID-19, and vaccine perception on vaccine acceptance?
Figures 1–3 show the proposed models predicting vaccine acceptance.
Method
COVID-19 situation and policies during data collection
After the study was approved by the Institutional Review Board (IRB), the lead author conducted an online survey from mid-June to mid-July 2021 at a public university in the state of Texas, U.S. As of mid-July 2021, Texas’ positivity rate was over 10%, indicating there was high transmission of the virus in the area. 33 At that time, approximately 41.5% of Texas residents were fully vaccinated, which was below the national full vaccination rate of 47%. 34 Regarding COVID-19 restrictions, the statewide mask mandate in Texas had been lifted and all businesses were permitted to operate at full capacity as of March 10, 2021. 35 Furthermore, as of May 21, 2021, government entities in Texas were prohibited from imposing mask mandates. 35 Thus, during the data collection period, Texas had no enforceable statewide mask or vaccination requirements.
Participant recruitment
The lead author contacted instructors at that university who were teaching summer classes, requesting their help with gathering data. A number of these instructors consented to share the survey link with their students and gave extra credit to students who participated in the survey. The survey included measures for all variables in the proposed models, as well as demographic variables. Participants were instructed to review an online consent form and confirm their willingness to participate by selecting “I consent to participate” before starting the survey. Each participant earned extra credit based on their instructor’s criteria.
Two screening questions unrelated to the study were embedded in the survey to assess response validity: (1) “Where is the capital of the USA located today?” and (2) “What language is mostly spoken in Mexico?” Each question included multiple-choice answers, with one clearly correct option. Participants who answered either question incorrectly were excluded from the analysis. In total, 12 participants were excluded based on these criteria. In total, 310 students provided valid responses, and they constituted the final sample used in the analyses.
Power analysis
A power analysis was conducted using the semPower package in R, which supports power analysis for structural equation models. 36 Following recommendations outlined by Regorz (2024), 37 including specifying α = 0.05 and power = 0.80, the analysis returned a required sample size of 206 participants. As the actual sample size in the present study was 310, the study has sufficient power to detect model effects.
Measures
The survey assessed worry about COVID-19, COVID-19 risk perception (perceived probability of contracting COVID-19 and perceived severity of contracting COVID-19), vaccine perception (perceived vaccine safety & perceived vaccine effectiveness), and COVID-19 vaccine acceptance, along with demographic variables. The present study used a measure of “intention to get vaccinated against COVID-19” as a proxy for measuring COVID-19 vaccine acceptance. The assessment items for all key variables were derived from peer-reviewed literature and subsequently adjusted to align with the context of COVID-19.26,38–40 Table 1 displays measurement items, ranges, means, standard deviations (SDs) and, where applicable, reliabilities of the key variables.
Measuring items, ranges, means, standard deviations (SDs), and reliabilities (when applicable) of key variables.

Analyses
The current study utilized AMOS 21.0 to perform structural equation modeling (SEM) analyses to test the three hypothesized models. After identifying the best-fitting model, bootstrapping procedures (2,000 resamples) were conducted to test the significance of each mediating path. Bias-corrected 95% confidence intervals were computed for each mediating path, and conclusions regarding statistical significance were drawn based on these intervals.
Multiple fit indices were utilized to assess how well the proposed models matched the data. In structural equation models with either continuous or categorical outcomes, a CFI or TLI score above 0.90 reflects a good alignment between the model and the data. 41 An RMSEA value below 0.05 indicates an excellent model fit, whereas values ranging from 0.05 to 0.08 suggest an acceptable level of fit. 41
The chi-square (χ²) statistic was also applied to compare models, as it remains the best test available for identifying issues within a model.42,43 A statistically-significant χ² value indicates that the model’s fitting function could not identify parameter estimates that adequately represent the data. 43 When the p-value of the model’s χ² test is below 0.05, it implies that the model deviates from the observed data. 44 Therefore, such a model is unlikely to be the best-fitting model.
Results
Sample characteristics
Table 2 presents sample characteristics (age, gender, and ethnicity).
Sample characteristics.

Model Testing
Three competing models were tested by SEM: (1) worry, the two risk-perception variables, and the two vaccine-perception variables influence vaccine acceptance simultaneously; (2) worry partially mediates the relationships between the risk-perception variables/vaccine-perception variables and vaccine acceptance; (3) the risk perception and vaccine perception variables partially mediate the relationship between worry and vaccine acceptance.
SEM analyses were conducted using maximum likelihood (ML) estimation. The AMOS output indicates that, for each variable in the hypothesized model, the absolute skewness values are less than 2 and the absolute kurtosis values are less than 7. According to Hair Jr. et al. (2010), 45 data are considered to exhibit univariate normality when skewness is between −2 and +2, and kurtosis is between −7 and +7. Therefore, the univariate normality assumption for all variables is satisfied. Results indicated that all analyzed models were identified. The reporting of this study conforms to the APA JARS-Quant guidelines for Structural Equation Modeling (Table 7). 46 (see Supplemental File 1).
SEM analysis for Model (1) revealed a significant chi-square value: χ2/df = 27.11/6 = 4.52, p < 0.001. The fit indices were: CFI = 0.979, TLI = 0.947, and RMSEA = 0.107. These findings suggest that Model (1) did not fit the data well.
SEM analysis for Model (2) also revealed a significant chi-square value: χ2/df = 10.29/4 = 2.57, p = 0.036. The fit indices were: CFI = 0.994, TLI = 0.976, and RMSEA = 0.071. These findings suggest that Model (2) did not fit the data well either.
SEM analysis for Model (3) revealed a non-significant chi-square value: χ2/df = 1.70/4 = 0.425, p = 0.791. The fit indices were: CFI = 1.000, TLI = 1.000, and RMSEA = 0.000. These findings suggest that Model (3) fit the data exceptionally well. Table 3 presents the Chi-square values and fit indices of the three SEM models.
Chi-square values and fit indices of the three SEM models.
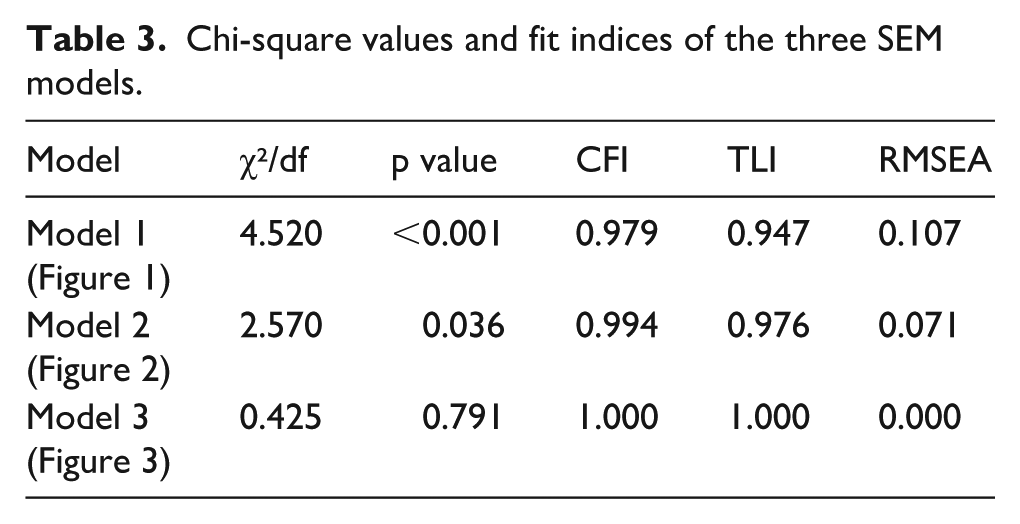
Based on the chi-square values and fit indices of the three models, Model (3) is the one that best fits the data, thus RQ1 was answered. Model (3) accounted for 50.3% of the variance in vaccine acceptance (R 2 = 0.503). The following sections present direct and indirect effects of all predictors on vaccine acceptance based on Model (3).
Regarding the direct effects of all predictors on vaccine acceptance, SEM analysis for Model (3) found that perceived probability of contracting COVID-19 (B = = −0.212, SE = 0.076, β = −0.126, p = 0.006), worry about COVID-19 (B = 0.222, SE = 0.090, β = 0.128, p = 0.014), and perceived vaccine safety (B = 0.947, SE = 0.147, β = 0.642, p < 0.001) are significant and direct predictors of vaccine acceptance. Perceived severity of contracting COVID-19 (B = 0.110, SE = = 0.084, β = 0.068, p = 0.192) and perceived vaccine effectiveness (B = 0.026, SE = 0.153, β = 0.017, p = 0.867) are non-significant predictors of vaccine acceptance.
As to the indirect effects of worry on vaccine acceptance, bootstrap mediation analyses for Model (3) found that the mediating paths from worry about COVID-19 to vaccine acceptance through perceived probability of contracting COVID-19 (B = −0.085, 95% CI = [−0.167, −0.024], p = 0.008) and through perceived vaccine safety (B = 0.310, 95% CI = [0.163, 0.520], p = 0.001) are significant; the mediating paths from worry about COVID-19 to vaccine acceptance through perceived severity of contracting COVID-19 (B = 0.069, 95% CI = [ −0.044, 0.174], p = 0.230) and through perceived vaccine effectiveness (B = 0.008, 95% CI = [−0.119, 0.125], p = 0.908) are non-significant. Thus, the direct and indirect effects of all predictors on vaccine acceptance for Model (3) were revealed, answering RQ2. Worry about COVID-19 has an indirect effect on vaccine acceptance through perceived probability (negative) and through perceived vaccine safety (positive). Figure 4 displays the path coefficients of the best-fitting model (Figure 3).

Standardized path coefficients of Model (3), the best fitting model.
Discussion
This study examines effects of COVID-19 risk perception (including perceived probability and perceived severity), vaccine perception (including perceived vaccine safety & perceived vaccine effectiveness), and worry about COVID-19 on vaccine acceptance, testing three competing models: (1) all predictors influence vaccine acceptance simultaneously; (2) worry serves as the mediator between the two risk-perception variables and vaccine acceptance, as well as between the two vaccine-perception variables and vaccine acceptance; (3) the risk-perception and vaccine-perception variables serve as mediators between worry and vaccine acceptance. SEM analyses found that only Model (3) shows an excellent fit to the data. Results of Model (3) analyses found that perceived probability of contracting COVID-19 has a direct and negative, and perceived vaccine safety (the strongest predictor) has a direct and positive influence on vaccine acceptance. The impacts of perceived severity of contracting COVID-19 and perceived vaccine effectiveness on vaccine acceptance are non-significant. Worry about COVID-19 has a direct and indirect influence on vaccine acceptance; the indirect influence is mediated by perceived probability of contracting COVID-19 and perceived vaccine safety. Implications of the present study are discussed below.
A counterintuitive finding of this study is that perceived probability of contracting COVID-19 has a negative influence on vaccine acceptance. In other words, college students who have higher perceived probability of contracting COVID-19 have lower vaccine acceptance. One possible reason for this finding is fatalistic beliefs. 47 This is often seen in the context of cancer, where individuals can exhibit “deterministic thoughts about the external causes of the disease, the inability to prevent it, and the inevitability of death at diagnosis” (p. 461), 48 and thus are less likely to take various preventive actions, according to Niederdeppe and Levy’s (2007) 47 study on a large national sample of U.S. adults. Similarly, if college students are convinced that they are going to contract COVID-19 anyway (a fatalistic belief), they are less likely to accept vaccines (a protective action against COVID-19).
Perceived severity of contracting COVID-19 was not significantly associated with vaccine acceptance in the present sample. One plausible explanation is the age composition of our participants, who were primarily young adults (mean age = 24.09). Research suggests that younger individuals often perceive themselves as less vulnerable and tend to underestimate the consequences of health-related threats, due to a sense of invincibility or optimism bias. 49 Consequently, they may not view COVID-19 as a serious personal threat, which could lead to rejection of vaccines. Additionally, reports on COVID-19 morbidity and mortality show that younger adults are significantly less likely to experience severe outcomes from COVID-19 compared to older age groups. 29 This actual low severity may reinforce the perception that vaccination is less necessary, thereby weakening the association between perceived severity and vaccine acceptance in this demographic.
The finding that perceived vaccine safety has a direct and positive influence on vaccine acceptance, while perceived vaccine effectiveness had no significant impact, suggests that whether vaccines are safe is much more important than whether they are effective when college students weigh their decisions to accept vaccines or not. One possible explanation is that getting vaccinated is not like taking oral medications, an activity which only involves drinking/eating, which people are used to doing in their daily life; the fact that it requires an injection might make it feel more intrusive, 50 thus triggering greater concerns about its safety. Another potential explanation is that the participants were American college students, as prior research indicates that individuals from developed countries tend to have greater doubts regarding the safety of vaccines. 51
Another interesting finding is that effects of worry on vaccine acceptance are partially mediated by perceived probability of contracting COVID-19 and perceived vaccine safety. Although this finding is inconsistent with the risk-as-feelings hypothesis, which suggests that feelings mediate cognition, it is in line with Chen and Liu’s (2023) 52 study, which reported that cognition mediates the effects of feelings on intentions to wear a mask or use an air-purifier in the context of air pollution; it is also consistent with Chen and Yang’s (2017) 53 study, which found that cognition mediates the effects of feelings on intention to quit smoking. Perhaps what they have in common is that these are all deliberate behaviors, rather than spontaneous ones: they require advance planning, scheduling, etc. Thus cognitions, rather than feelings, become the main determinants in vaccine acceptance.
Theoretical implications
Our findings carry important theoretical implications. First, the result that worry about COVID-19 is a significant and direct predictor of vaccine acceptance underscores the role of feelings in health-related decision making. This aligns with the risk-as-feelings hypothesis, which posits that emotional reactions can directly influence behavior, particularly in contexts involving uncertainty or risk. 13
Second, the finding that worry indirectly affects vaccine acceptance through perceived probability and perceived vaccine safety suggests that, in the context of deliberate health decisions such as vaccine uptake, it’s more likely that feelings influence decision making through cognitive pathways, rather than that cognition influences decision making through feelings. This supports the central tenets of both the Health Belief Model (HBM) 15 and Protection Motivation Theory (PMT), 16 which propose that cognitive factors—such as perceived susceptibility and severity—are the primary, proximal determinants of health behaviors and intentions, and that feelings like worry function as distal factors, shaping behavior indirectly by influencing cognitive appraisals.
Finally, these findings suggest that HBM and PMT offer more appropriate theoretical frameworks for understanding deliberate health behaviors than the risk-as-feelings hypothesis. In other words, while feelings do play a role, cognition appears to be the main driver of deliberate health-related decisions.
Limitations
This study has some limitations. First, all measures relied on self-reports, therefore, there is a possibility that social desirability may have biased the findings. Nevertheless, the survey questions in the current study were not intrusive, and “not applicable” options were included where appropriate, likely encouraging honest responses from most participants.
Second, this study treated perceived probability and perceived severity as distinct and independent predictors. This approach aligns with much of the existing literature on COVID-19 vaccination behavior and intentions.8–10 Moreover, one study found that the combined construct (i.e. the product of perceived probability and severity) was not a significant predictor of COVID-19 vaccination behavior. 25 However, some scholars have advocated for combining perceived probability and severity multiplicatively. 15 Future research may benefit from comparing models that treat perceived probability and severity independently with those that combine them multiplicatively, to determine which approach more effectively predicts health-related behaviors and intentions.
Third, it should be noted that the present sample reported relatively low levels of worry (M = 2.35 on a scale from 1 to 7). This may have influenced the strength or significance of associations between the mediators (i.e. perceived probability of contracting COVID-19, perceived severity of contracting COVID-19, perceived vaccine safety, and perceived vaccine effectiveness) and the outcome variable (i.e. vaccine acceptance) in our final model (see Figure 3). Future studies should consider recruiting larger and more diverse samples to allow for subgroup analyses based on worry levels, which would enable a more nuanced understanding of how worry may moderate these relationships.
Fourth, this study used a sample of college students, who are mostly younger adults. Compared to older adults or individuals with underlying health conditions, younger adults are less likely to experience severe symptoms—or may even remain asymptomatic—after contracting COVID-19. 29 This lower severity of COVID-19 in younger populations may influence their beliefs about the virus and reduce their motivation to get vaccinated, potentially limiting the generalizability of our findings to more vulnerable groups.
Fifth, the current sample consisted of a notably high proportion of female participants (69.4%), which surpasses the national average of 58% female undergraduate students in the United States in 2021. 54 This sample characteristic may limit the generalizability of the findings to the broader U.S. college student population. Finally, the cross-sectional nature of this study determines that the causal relations between predictors and the outcome variable should be interpreted with caution.
Conclusion
Despite the limitations mentioned above, the present study represents the first attempt to test three competing models involving cognitions, feelings, and vaccine acceptance in the COVID-19 context. Findings suggest that higher perceived probability of contracting COVID-19 and lower perceived vaccine safety are related to lower vaccine acceptance. Worry about COVID-19 directly and indirectly influences vaccine acceptance, with indirect influences partially mediated by perceived probability of contracting COVID-19 and perceived vaccine safety. Findings contribute to public health research by demonstrating that cognitions, instead of worry, are the main drivers of COVID-19 vaccine acceptance. Moreover, this study contributes to public health practice by recommending that vaccine campaigns targeting college students focus on vaccine safety, utilize reasonable worry as an emotional cue, and refrain from excessive emphasis on the likelihood of contracting COVID-19. Future research may want to test the three competing models in other health/risk behaviors, including deliberate behaviors and spontaneous ones.
Supplemental Material
sj-xlsx-1-phj-10.1177_22799036251374804 – Supplemental material for Worry, risk perception, vaccine perception, and vaccine acceptance: Testing three competing path models in the context of COVID-19
Supplemental material, sj-xlsx-1-phj-10.1177_22799036251374804 for Worry, risk perception, vaccine perception, and vaccine acceptance: Testing three competing path models in the context of COVID-19 by Yixin Chen in Journal of Public Health Research
Footnotes
Acknowledgements
I thank my colleagues at Sam Houston State University including Lisa Chaddick, Danhong Chen, Douglas Constance, Lisa Dahlgren, Desiree Hickman, Katharine Hubbard, Anya Hommadova Lu, Candy Lynch, Lauren L. McLean, Willis Oyugi, Christopher Patane, Jessica Scoggins, Caroline Waldbuesser, Xiaobo Wang, and Melinda R. Weathers for inviting their students to participate in the survey of this study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical considerations
This study was approved by the Sam Houston State University Institutional Review Board (PROTOCOL #: IRB-2021-197).
Consent to participate
Participants were instructed to review an online consent form and confirm their willingness to participate by selecting “I consent to participate” before starting the survey.
Data availability statement
The data is available upon request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.