
Abstract
Introduction:
Non-communicable diseases (NCDs) cause 71% of global deaths, with many risk factors originating in childhood. Understanding adolescent health knowledge and behaviors across countries is essential for targeted public health interventions. This study compares health literacy, dietary habits, physical activity, mental health awareness, sexual health education, and substance use awareness between adolescents in India and the United States (US).
Design and methods:
A cross-sectional survey was conducted among 200 adolescents (100 per country) recruited through educational institutions and online platforms. Stratified sampling ensured representation across age (13–18 years), gender, and geographic location (urban vs rural). A structured questionnaire, adapted from validated instruments, assessed health-related behaviors and knowledge. Descriptive statistics and chi-square tests compared responses, and logistic regression adjusted for confounders.
Results:
Significant differences emerged between Indian and US adolescents. Indian respondents had lower mental health awareness (46% vs 88%, p = 0.0004) and Sexually Transmitted Infection (STI) prevention knowledge (58% vs 77%, p < 0.0001). Regular physical activity was higher in the US (50% vs 20%, p < 0.0001), as was nutrition awareness (83% vs 69%, p = 0.0152). Indian adolescents more often relied on school-based health education (29% vs 21%) and social media (30% vs 29%) for information.
Conclusion:
Findings highlight disparities in adolescent health literacy and behaviors across India and the US. Public health efforts should prioritize mental health literacy, nutrition education, and physical activity, especially in India. Digital platforms and school-based initiatives can help bridge knowledge gaps and promote healthier adolescent behaviors globally.
Keywords
Introduction
Non-communicable diseases (NCDs) have become a pressing global health concern, affecting over 2.1 billion children worldwide. 1 The World Health Organization (WHO) reports that NCDs account for nearly 41 million deaths annually, representing 71% of global mortality.2,3 These diseases, including cardiovascular conditions, diabetes, cancer, and respiratory disorders, often originate in childhood due to modifiable risk factors such as poor diet, physical inactivity, and substance use.4,5
A growing body of literature underscores the importance of early intervention in reducing the long-term burden of NCDs. 6 Studies have shown that over two-thirds of NCD antecedents begin in childhood, making adolescence a critical period for preventive measures. However, despite this urgency, children and adolescents are frequently underrepresented in global health policies. Surveillance efforts often exclude younger populations, leading to missed opportunities for intervention and policy development. 7
Research highlights significant differences in health behaviors, knowledge, and awareness across countries. 7 For instance, a study comparing youth health behaviors in high-income and low- to middle-income countries found that lifestyle patterns and access to healthcare resources vary widely, impacting overall health outcomes. 8 In the US, extensive public health campaigns and school-based interventions have improved awareness of nutrition, physical activity, and mental health. 9 In contrast, developing nations such as India continue to face challenges in implementing large-scale health education programs due to socio-economic disparities. 10
Understanding cross-national differences in adolescent health literacy is crucial for designing effective, context-specific interventions. 11 This study aims to compare health knowledge, dietary habits, physical activity, mental health awareness, sexual health education, and substance use awareness among adolescents in India and the United States. By identifying key areas of divergence, the findings will inform targeted public health strategies to address disparities and promote healthier behaviors.
Materials and methods
Study design and participant selection
This study employed a cross-sectional survey design to assess differences in adolescent health knowledge, dietary habits, physical activity, mental health awareness, and substance use education in India and the United States. A total of 200 adolescents (100 from each country) were recruited through educational institutions and online platforms. Although the sample size (100 participants per country) is relatively small compared to national adolescent populations, participants were selected using a stratified sampling approach to ensure representation across demographic groups, including variations in age (13–18 years), gender, and geographic location (urban vs rural). The study protocol was reviewed and approved by the Institutional Ethics Committee of Care International School, Tiruchirappalli, India (Approval Number: CIS/IEC/2024/014) and the Research Oversight Committee of The Village School, Houston, United States (Approval Number: TVS/ROC/2024/078). Participation was entirely voluntary. Written informed consent was obtained from all participants and, where applicable, from their legally authorized guardians prior to study initiation, in accordance with ethical guidelines for research involving minors. In addition, verbal assent was obtained from all adolescent participants before survey completion. Data were collected anonymously, and confidentiality was maintained throughout. The study was conducted in accordance with the principles of the Declaration of Helsinki.
Survey instrument and validation
Source instruments
The structured questionnaire was adapted from previously validated tools assessing adolescent health literacy and health-related behaviors, specifically the World Health Organization’s Global School-Based Student Health Survey (GSHS) and the Health Literacy Questionnaire (HLQ). These instruments were selected for their robust psychometric properties and prior use among adolescent populations in diverse settings.
Language and translation considerations
As the survey was administered in English and all participants were fluent, linguistic translation was not necessary. However, we implemented a rigorous cultural and contextual adaptation process to ensure that questions were understandable, culturally appropriate, and relevant in both India and the United States.
Expert panel review
A multidisciplinary expert panel comprising five professionals in public health, adolescent psychology, education, and behavioral science from both countries independently reviewed each item for cultural and linguistic suitability. Their review focused on identifying items that required contextual refinement, including health-related terminology, schooling structures, and culturally variable behaviors (e.g. references to school-based health classes or typical dietary patterns).
Cognitive interviews
Following initial review, cognitive interviews were conducted with 10 adolescents from each country (n = 20 total) using think-aloud and verbal probing techniques. These interviews helped identify areas of confusion, misinterpretation, or contextual disconnect. Based on their feedback, several items were reworded to improve clarity, precision, and cultural resonance. For example, “junk food” was replaced with “foods high in sugar or fat,” and “seeing a counselor” was clarified as “talking to a trusted adult or mental health professional.”
Pilot testing and refinement
A pilot test of the revised instrument was conducted with 20 adolescents in each country (n = 40). This phase assessed item flow, readability, participant burden, and feasibility. The pilot also allowed us to evaluate missing responses and clarify any remaining ambiguities. The pilot confirmed that the adapted tool was acceptable in length and language for the target age group (13–18 years), and no major revisions were required post-pilot.
Psychometric properties
The finalized questionnaire demonstrated strong psychometric reliability across key domains including mental health, nutrition, physical activity, and sexual health. Internal consistency was high, with Cronbach’s alpha coefficients ranging from 0.75 to 0.82 across domains. To assess stability over time, test–retest reliability was evaluated in a subset of 20 participants across both countries after a 2-week interval. The resulting intraclass correlation coefficients (ICC) ranged from 0.72 to 0.80, indicating good reliability and measurement stability.
Data collection and bias mitigation
Participants completed an online survey, which included sections on health knowledge, sources of health information, dietary awareness, physical activity, mental health perceptions, sexual health education, and substance use awareness. To reduce self-reporting bias, responses were collected anonymously, and neutral language was used to frame sensitive questions. Socioeconomic status (SES) was assessed using a composite index comprising three indicators: parental education level (highest attained by either parent), self-reported household income category, and household asset ownership (e.g. refrigerator, two-wheeler, internet access). These components were standardized and aggregated into a cumulative SES score, which was then classified into tertiles—low, middle, and high—for adjusted comparative analyses.
Statistical analysis
Descriptive statistics were used to compare survey responses between India and the United States. The Chi-square test for independence was applied to determine whether there were statistically significant differences in responses between the two countries. A p-value less than 0.05 indicated statistical significance, suggesting that the observed differences were unlikely to have occurred by chance. Logistic regression models were employed to adjust for potential confounders, including gender, socioeconomic status, and geographic location (urban vs rural). Missing data were addressed using multiple imputation techniques to maintain dataset integrity.
Results
Baseline characteristics of study participants
A total of 200 adolescents (100 from each country) participated in the study, with recruitment through educational institutions and online platforms. Participants were selected using a stratified sampling approach to ensure representation across demographic groups, including variations in age (13–18 years), gender, and geographic location (urban vs rural). The distribution of participants by grade level was identical in both countries: 35% were in 9th grade, 21% in 10th grade, 27% in 11th grade, and 17% in 12th grade.
Health knowledge and information-seeking behavior
Health knowledge levels varied between India and the United States. In India, 24% of respondents rated their health knowledge as “excellent,” compared to 20% in the US. Conversely, 7% of Indian respondents rated their knowledge as “poor” or “very poor,” higher than the 6% in the US (p = 0.0023). In terms of health information-seeking behavior, 30% of Indian respondents frequently searched for health-related information, compared to 23% in the US. However, 21% of Indian respondents never sought health information, significantly higher than the 7% in the US (p = 0.0008). Table 1 presents a comparative analysis of adolescent health knowledge, habits, and awareness between India and the United States. The data highlight significant differences in health literacy, dietary habits, physical activity, mental health awareness, sexual health education, and substance use knowledge, reflecting variations in public health policies and socio-cultural influences.
Health knowledge, habits, and awareness: India versus United States.

This table presents a comparative analysis of adolescent health knowledge, habits, and awareness between India and the United States, with n = 100 respondents from each country. The survey responses highlight differences in various health-related aspects, including self-reported health knowledge, information-seeking behavior, dietary habits, physical activity levels, mental health awareness, sexual health comfort, and substance use knowledge. The percentage values represent the proportion of respondents from each country selecting a given response. Statistically significant differences (p-values provided in Table 2) indicate notable disparities in health literacy, access to health resources, and public health education between the two populations.
Nutrition and diet awareness
Awareness of balanced nutrition was higher in the US (83%) than in India (69%; p = 0.0152). In the US, 61% of respondents consumed 2–3 servings of fruits and vegetables daily, compared to 44% in India. Additionally, 34% of Indian respondents consumed only 0–1 servings per day, compared to 17% in the US (p = 0.0039). Knowledge of the difference between saturated and unsaturated fats was comparable between both countries, with 59% of Indian respondents and 43% of US respondents answering correctly (p = 0.0415).
Physical activity and exercise patterns
Regular physical activity was significantly higher in the US, where 50% of respondents engaged in at least 30 min of exercise five or more times per week, compared to 20% in India (Figure 1). Meanwhile, 10% of Indian respondents reported no physical activity, compared to only 1% in the US (p < 0.0001).

Physical activity frequency by country. This bar chart visually compares the percentage of adolescents in India and the U.S. by number of days per week they engage in ≥30 min of physical activity. Indian adolescents reported lower levels of physical activity, with only 20% exercising five or more days per week compared to 50% in the U.S. Conversely, 46% of Indian adolescents exercised only 1–2 days per week, significantly higher than the 10% in the U.S.
Mental health awareness and accessibility
Mental health awareness was considerably higher in the US, where 88% of respondents recognized symptoms of stress and anxiety, compared to 46% in India (p = 0.0004; Figure 2). Furthermore, 92% of US respondents knew where to seek help for mental health issues, whereas 48% of Indian respondents did not (p < 0.0001; Figure 3). Table 2 provides the statistical significance (p-values) of the observed differences in health knowledge, habits, and awareness between Indian and US adolescents. The results indicate that disparities in mental health awareness, physical activity, dietary habits, and sexual health education are statistically significant, underscoring the need for targeted interventions in both countries.
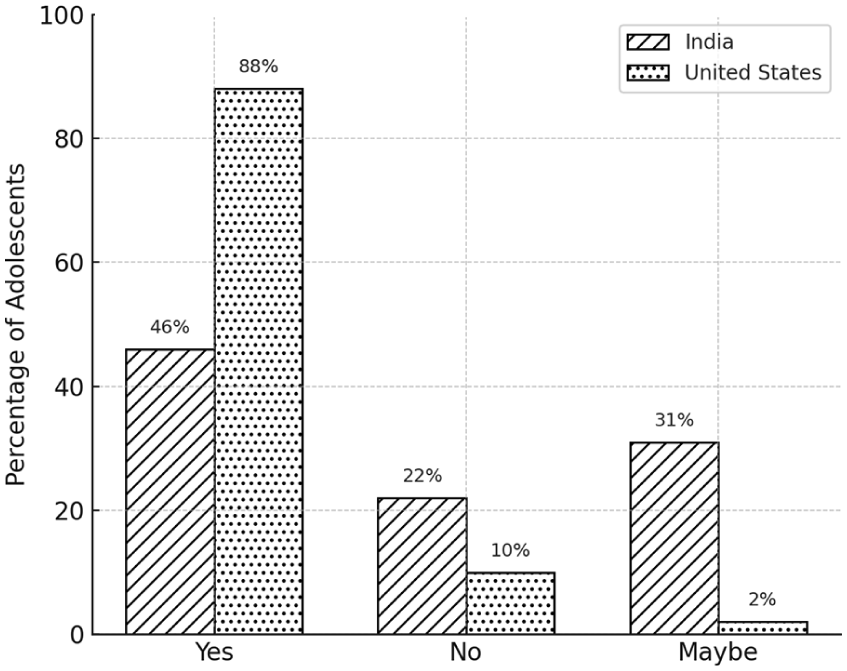
Awareness of signs of stress and anxiety. This bar chart compares the awareness of signs of stress and anxiety among adolescents in India and the US. It shows that only 46% of Indian adolescents recognized stress and anxiety signs, compared to 88% in the US.
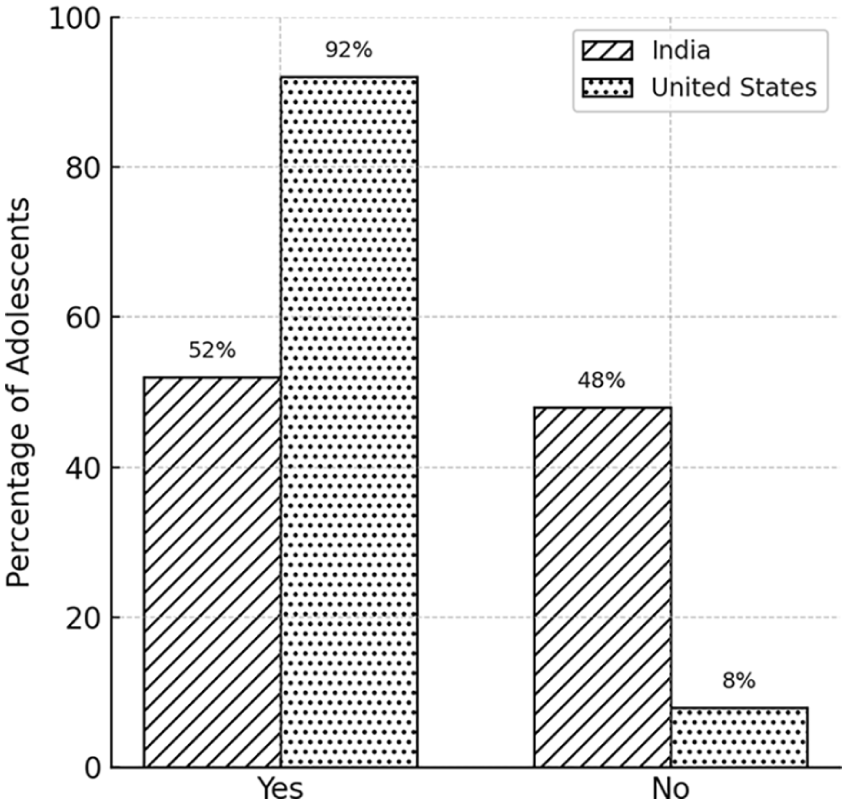
Knowledge of where to seek help where to seek help for mental health issues. This bar chart illustrates cross-national differences in knowledge of where to seek help for mental health issues. It shows that 52% of Indian adolescents knew where to seek help, whereas 92% of U.S. adolescents did.
p-Values for health knowledge, habits, and awareness questions (India vs United States).

Figures in bold are significant with p-value <0.05.
The Chi-square test for independence was applied to analyze whether there is a statistically significant difference in survey responses between India and the United States. The p-value measures the probability that the observed differences occurred by random chance. A p-value less than 0.05 indicates a statistically significant difference between the two countries. All questions in this analysis have significant p-values, meaning we reject the null hypothesis in each case. This suggests that responses on health-related knowledge and behaviors differ significantly between India and the United States.
Sexual Health and STI awareness
Comfort in discussing sexual health varied between the two countries. In India, 38% of respondents were “somewhat comfortable,” 38% were “very comfortable,” and 24% were “not comfortable.” In contrast, 52% of US respondents were “somewhat comfortable,” 36% were “very comfortable,” and 12% were “not comfortable” (p = 0.0187). Awareness of STI prevention was higher in the US (77%) compared to India (58%) (p < 0.0001).
Substance use awareness and exposure
Knowledge of smoking and vaping effects was more widespread in the US, where 70% of respondents reported being “very knowledgeable,” compared to 38% in India (p < 0.0001). Additionally, 38% of Indian respondents never encountered information on alcohol and drug use, significantly higher than the 4% in the US (p = 0.0006).
Health information preferences
In both countries, respondents relied on different sources for health information. In India, social media (30%) and school programs (29%) were the most common sources, whereas in the US, online resources (32%) and social media (29%) were predominant (p = 0.0271). Workshops were the least preferred source in both countries.
Health topics of interest
Interest in nutrition and physical fitness was strong in both countries. In India, 39% of respondents wanted to learn more about physical fitness, followed by 37% for nutrition. Similarly, in the US, nutrition (33%) and physical fitness (26%) were the top areas of interest (p = 0.0345). Mental health interest was greater in the US (19%) than in India (24%).
Physical activity participation
Preferences for physical activities differed between the two countries. Team sports were more popular in India (43%) than in the US (36%), while gym workouts were slightly more common in the US (27%) than in India (21%). Walking and running were equally popular, with 31% of Indian respondents and 33% of US respondents participating. Individual sports participation was higher in the US (21%) than in India (13%; p = 0.0196).
Discussion
This study highlights key differences in health knowledge, behaviors, and awareness among adolescents in India and the United States. These differences reflect broader disparities in education, healthcare access, and public health policies, emphasizing the need for tailored interventions.1–5
Indian adolescents were more likely to seek health information frequently (30% vs 23% in the US). However, a notable proportion (21%) never sought health information, compared to only 7% in the US. This pattern suggests that while some Indian adolescents are proactive, barriers such as limited digital access, lower health literacy, and gaps in school-based health education may prevent others from seeking information.8–11 In contrast, US respondents showed higher confidence in their health knowledge, likely due to stronger school-based health programs and greater exposure to public health campaigns.
Nutritional awareness was higher among US adolescents, with 83% understanding what constitutes a balanced diet, compared to 69% in India. Additionally, 61% of US respondents consumed 2–3 servings of fruits and vegetables daily, compared to 44% in India. Alarmingly, 34% of Indian respondents consumed only 0–1 servings per day, nearly double the 17% in the US. These findings are consistent with global nutrition studies that report lower dietary diversity among adolescents in South Asia, often influenced by economic factors, food availability, and cultural dietary practices. 12
Regular exercise was more common among US adolescents, with 50% engaging in at least 30 min of activity five or more times per week, compared to 20% in India. Additionally, 10% of Indian adolescents reported no physical activity, compared to just 1% in the US. These findings reflect broader global trends, as reports suggest that adolescents in high-income countries benefit from greater access to recreational facilities, organized sports, and structured school-based physical activity programs.10,11 A 2022 WHO report found that 80% of adolescents worldwide fail to meet recommended physical activity guidelines, particularly low engagement in South Asia due to infrastructural and cultural limitations. 13
The most significant disparity emerged in mental health awareness. In the US, 88% of respondents recognized symptoms of stress and anxiety, compared to only 46% in India. Furthermore, 92% of US participants knew where to seek help for mental health concerns, while 48% of Indian adolescents did not. These results align with prior studies highlighting the limited availability of mental health resources in India, where the mental health workforce is critically inadequate, with only 0.3 psychiatrists per 100,000 people—far below the 16 per 100,000 available in the US. 14 Additionally, cultural stigma surrounding mental health in India may contribute to lower levels of awareness and help-seeking behaviors. 14
Sexual health awareness was higher among US respondents (77%) compared to Indian respondents (58%). Prior studies indicate that comprehensive sex education is more prevalent in high-income countries, while discussions on sexual health in India may be constrained by sociocultural barriers and inconsistent school-based curricula. 15
Substance use awareness showed a similar trend, with 70% of US respondents reporting high knowledge of smoking and vaping risks, compared to 38% in India. Prior studies have linked this disparity to stricter tobacco control measures, widespread anti-smoking campaigns, and higher exposure to preventive education in US schools. In contrast, a lack of stringent tobacco regulations in many parts of India, coupled with the social acceptability of certain tobacco products like smokeless tobacco, may contribute to lower awareness and higher adolescent tobacco use. 16
Health information sources varied between countries. Indian adolescents relied more on school programs (29%) and social media (30%), while US respondents preferred online resources (32%) and social media (29%). These findings align with studies on digital health literacy, which suggest that adolescents in developing countries increasingly use social media as a primary source of health information, despite concerns about misinformation and reliability.17,18
Exercise preferences also varied. Team sports were more popular in India (43%) than in the US (36%), whereas US adolescents showed a greater preference for gym workouts (27% vs 21% in India). Walking and running were common in both countries (31% in India, 33% in the US). These results suggest that public health initiatives should be tailored to local preferences, emphasizing community-based and school-supported physical activity programs.19,20
Multiple factors, including cultural norms, healthcare access, and public health policies shape health knowledge and behaviors. The observed differences between Indian and US adolescents reflect broader structural disparities in education, healthcare availability, and social attitudes toward health. For example, limited mental health awareness in India may be linked to cultural stigma and a lack of mental health services in schools, whereas structured mental health programs and awareness campaigns are more prevalent in the United States. Similarly, nutrition awareness and physical activity engagement differences may be influenced by economic factors, urban planning, and parental health education. To address these disparities, targeted interventions are necessary. Given the significant gap in mental health awareness and accessibility in India, campaigns and school-based interventions should be prioritized.14,21 Public health initiatives must also improve nutrition education by increasing awareness of balanced diets and healthy eating habits. 22 Policies promoting physical activity through improved sports facilities and awareness programs can encourage active lifestyles. 23 Additionally, incorporating comprehensive sexual health curricula in schools can help bridge knowledge gaps. 15 Finally, digital platforms should be leveraged to disseminate reliable health information, especially in India. 24
Based on the study findings, several actionable public health policy recommendations emerge. First, the implementation of mandatory mental health literacy programs in Indian secondary schools is strongly recommended. These programs should be embedded in the national curriculum and focus on stress recognition, emotional regulation, stigma reduction, and providing clear pathways for seeking professional help. Existing frameworks—such as the WHO’s Mental Health Gap Action Programme (mhGAP) and UNICEF’s Life Skills Education initiative—can serve as culturally adaptable and scalable models for implementation. In parallel, school personnel—including teachers and counselors—should be trained to recognize early signs of psychological distress and to activate appropriate referral pathways to mental health services. Additionally, collaborations among schools, ministries of health and education, and adolescent mental health organizations will be essential to ensure sustainability and scale. Finally, digital platforms and social media can be leveraged to complement school-based initiatives, enhance adolescent engagement, and increase access to accurate and age-appropriate health information.
Strengths and limitations
This study has several strengths. First, it provides a comparative perspective on adolescent health behaviors between India and the United States, offering insights into country-specific gaps. Second, the study highlights multiple aspects of health, including nutrition, mental health, physical activity, and sexual health, contributing to a holistic understanding of adolescent well-being. Third, the findings can inform targeted public health strategies to address the specific needs of adolescents in both countries.
Despite these strengths, there are limitations. The relatively small sample size (100 respondents per country) limits the generalizability of findings. While this sample provides valuable cross-national insight, it may not fully capture the variability of adolescent health behaviors across diverse socio-cultural settings. Future studies should aim for larger and more demographically varied cohorts to improve representativeness and external validity. As with all self-reported survey studies, there is an inherent risk of measurement bias—particularly recall bias and social desirability bias. Recall bias may arise when participants struggle to accurately recall past behaviors or experiences. Social desirability bias may lead respondents to overstate behaviors they perceive as socially approved or underreport those considered stigmatized. To reduce these risks, several precautions were implemented. Surveys were administered anonymously to minimize social pressure and promote honest disclosure. All items were carefully phrased using neutral, non-judgmental language, and trained enumerators provided standardized instructions without offering cues that could bias responses. Participants were also reminded that there were no right or wrong answers and were encouraged to answer truthfully. While these strategies helped reduce bias, some degree of response distortion may remain. Moreover, while age, gender, socioeconomic status, and geographic location were accounted for, other contextual factors such as parental education, school-level interventions, or media exposure were not captured. Future research should use larger and more diverse samples, incorporate longitudinal or mixed-method approaches, and explore the use of objective measures—such as wearable devices or standardized screening tools—to improve validity and enrich understanding of adolescent health behaviors across cultural contexts.
Based on the gaps identified in this study, we propose the concept of a mobile application, tentatively named FitFuture, designed to integrate mental health support, nutrition education, and physical activity guidance into a single, adolescent-friendly platform. While the app is not currently under development, the concept reflects a future direction for addressing the multidimensional health needs of adolescents. By leveraging digital tools, this initiative aims to improve health literacy and engagement among young individuals in both India and the US. Until such a platform is developed, several existing evidence-based digital tools such as MindDoc 25 and Health4Life App 26 can be adapted to support adolescent well-being. Facilitating access to such platforms through schools, community outreach, or digital literacy initiatives may help bridge current gaps in adolescent health education and support.
Conclusion
This study reveals significant cross-national differences in adolescent health knowledge, behaviors, and awareness. US adolescents demonstrate higher awareness in mental health, STI prevention, and substance use, while Indian adolescents rely more on school-based health education and social media for information. These findings highlight the need for targeted public health initiatives, particularly in India, to improve mental health literacy, nutrition education, access to healthcare resources, promote positive behaviors, and reduce future non-communicable disease risk. Future interventions should leverage digital platforms, enhance school curricula, and address socio-economic barriers to ensure equitable health education for adolescents worldwide. We further recommend the development of culturally tailored, comprehensive health education programs that integrate into national curricula and utilize technology to improve reach and engagement. Future research should evaluate the effectiveness of such interventions across diverse socioeconomic settings, using longitudinal designs to assess sustained improvements in adolescent health knowledge, behavior, and outcomes. To support these efforts, researchers should focus on developing culturally relevant digital health education tools that align with adolescents’ media habits and learning preferences. Longitudinal studies are also needed to evaluate the sustained impact of such interventions on health knowledge, behavior, and long-term outcomes.
Significance for public health
This study provides critical insights into the disparities in health knowledge, behaviors, and awareness among adolescents in India and the United States—two countries with contrasting public health infrastructures and socio-cultural contexts. By identifying gaps in mental health literacy, dietary habits, physical activity, and substance use awareness, especially among Indian adolescents, the findings underscore the urgent need for context-specific health education initiatives. The results can inform targeted public health interventions that prioritize digital platforms and school-based programs to improve adolescent health literacy, reduce preventable non-communicable disease risks, and foster healthier lifelong behaviors. Strengthening adolescent health education not only enhances individual well-being but also contributes to broader public health goals by reducing future healthcare burdens and promoting equity in global health outcomes.
Footnotes
Consent to participate
Written informed consent was obtained from all participants and, where applicable, from their legally authorized guardians prior to study initiation, in accordance with ethical guidelines for research involving minors. In addition, verbal assent was obtained from all adolescent participants before survey completion.
Author contributions
Ahsan Kaja Abdul Majeed and Jay Raj conceived the study, designed the survey instrument, and were involved in data collection, data analysis, and interpretation of findings. Both authors contributed to drafting the manuscript and made critical revisions for intellectual content. Ahsan Kaja Abdul Majeed takes full responsibility for the overall content of this work, had full access to all the data, and affirms the integrity and accuracy of the data analysis.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflict interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.