
Abstract
Background:
Many Black Africans live in the UK. More than 850,000 people live with dementia in the UK, and more than 25,000 people with dementia are from Black and minority ethnic groups. The study explores themes of lay knowledge and beliefs about dementia.
Design and Methods:
This study employs a qualitative research design and methods to explore lay knowledge and beliefs about dementia amongst Black African populations living in London. The research is philosophically underpinned by social constructionism and sociological and anthropological lay concepts of health and illness. The researcher interviewed 31 adult respondents, male and female, from the Black African community in London to generate rich data. Participants were first-generation immigrants from West Africa living in London and were mainly carers. Thematic data analysis informed by a grounded theory approach was used to analyse the data.
Results:
The findings show that dementia is a complex biopsychosocial phenomenon. Four key themes with subthemes emerged and were developed: (i) Traditional views, (ii) Disease and illness, (iii) Help-seeking, and (iv) Caregiving and treatment. The group’s understanding of dementia evolved from traditional views to a more medical perspective. This study added witchcraft to the dementia literature on BAME in the UK.
Conclusions:
The study concluded that the group does not lack knowledge of dementia. Their understanding and beliefs about dementia are evolving, and further efforts are needed to enhance awareness through education, training, and outreach to support individuals with dementia and their families within the Black African community.
Keywords
Introduction
Equal opportunity to access dementia services is a priority and essential for a racially and ethnically diverse population in the UK, including those conducting dementia research. 1 Literature on Black and minority ethnic groups (BAME) in the UK suggests that Black Africans lack knowledge of dementia and rely on the community for advice and dementia care. 2 Black African populations in the UK are underrepresented in dementia specialist services, 3 delayed in using dementia specialist services, and often at higher risk of not being diagnosed and prescribed the appropriate care and medication for dementia. 4 Black Africans would instead use churches for dementia support. 3
Previous authors concluded that Black Africans, like other minority ethnic communities in the UK, lack knowledge of dementia without an in-depth exploration of the Black Africans’ own dementia ideas, meanings, experiences, and feelings about dementia.2,3 The data was limited in culture and often did not separate the findings of Black Africans from Caribbean people. Little do we know about dementia from the cultural perspectives of Black African populations in the UK. Evidence synthesis suggests more research is needed on Black African populations in the UK. 5
In the UK, about 25,000 BAME people are living with dementia, and this number is projected to increase sevenfold by 2051.6,7 The African population constitutes a significant demographic in the UK, with approximately a million Black people residing in London, and half of the Black population comprises Black Africans, 8 this can lead to increased dementia prevalence amongst the BAME in the UK.9,10 According to the 2021 Census, approximately 2.4 million Black individuals reside in the UK, accounting for 4.2% of the population. Africans comprise more than half of this demographic, with 1.5 million people representing 2.5%, an increase from 1.8% in 2011. Black African people are the largest ethnic group within this population, predominantly consisting of Nigerians (0.5%), Somalis (0.3%), and Ghanaians. (0.2%). 8
The average life expectancy has improved globally. 11 It has increased in Black African populations and is expected to rise above the average of 65 years in the UK due to better quality of life and access to essential health services. 12 Therefore, we anticipate the dementia rate to rise amongst Black African populations in the UK. More importantly, many Black African immigrants reside in London, 8 and migration impacts practice and knowledge about dementia. 13
In addition, approximately 850,000 people are living with dementia in the UK, and 1 in 14 people over 65 has dementia, affecting 1 in 6 people over 80, primarily impacting women. 7 Dementia can be considered one of the leading causes of death amongst women aged 60 and above. 14 The cost of dementia to the UK government exceeds £26 billion per annum, 14 whilst Black African communities in the UK present with a greater risk of dementia.2,4 Current research is needed in the population group, including a deeper understanding of the Black African populations’ lay knowledge and beliefs about dementia to inform practice and policy. 5 Lay concepts of dementia amongst Black Africans, like in any other culture, are sociocultural constructs that can intersect with biomedical constructions.15–17
Dementia is a complex biopsychosocial phenomenon. This research focuses on methodological adaptations 18 to continually ensure that the study is culturally sensitive and valid for Black African populations. 19 Incorporating the views, experiences, perspectives, and practices of Black African populations into the research process was essential and informed by the grounded theory (CGT) approach.20,21 The research adopts a pragmatist, relativist and constructivist methodological approach, which aligns with the constructivist grounded theory.22,23 It emphasises co-construction and relationality.24,25
Design and methods
Research aim
The study aims to utilise a qualitative research design and methods to explore themes of lay knowledge and beliefs about dementia amongst first-generation Black African immigrants from West Africa living in London, employing a grounded theory approach.
Pilot study
Before the main study, a preliminary pilot study recruited three participants (n = 3) to test the research procedures, including the vignette and the semi-structured interview guide, to identify what was effective and what was not. The researcher reflected on the process and adapted the vignette based on the literature. 26 The vignette and interview guide were validated 27 by pilot testing during the research process, through expert reviews with peers, academic supervisors and participant feedback (see Figure 1). The researcher developed the interview guide using a framework 28 that involves:
Identifying the prerequisites for using semi-structured interviews
Retrieving and using previous knowledge
Formulating the preliminary semi-structured interview guide
Pilot testing of the guide
Presenting the semi-structured interview guide

Thematic data analysis informed by a grounded theory approach.
Quality indicators
Trustworthiness discourse was used to evaluate the quality of this study. It offered sufficient flexibility to accommodate the diverse approaches and multiple interpretive best practice methods for achieving the study’s quality, rigour, and trustworthiness within the qualitative paradigm,29–32 drawing on key concepts: Credibility, Transferability, Dependability, Confirmability, and Authenticity.
The following questions illuminate authenticity:
Do the findings have a transformative potential in dementia practice in the UK?
Is there a community consensus amongst the Black African population and health practitioners that the findings are ‘useful and have meaning for action and further steps’ that could be applied in dementia services in the UK. 32
Member checking 33 was used to verify the apparent authenticity, ensuring that members reviewed the transcripts for accuracy and that the data accurately represented them. The researcher shared the findings with health practitioners in the UK who served as ‘the end-user’ in the community and can apply the findings in dementia practice, 32 enhancing the study’s external validity. 27
Research refining process
The research questions, interview guide, and vignette were continually refined in the research process. Examples of protocol questions include: What do you know about dementia? What are your beliefs towards dementia? Prompt: Tell me a bit more.
The vignette favoured a gradual entry that allowed the respondent’s feeling of intrusion to be managed socioculturally,
34
generating a rapport and relationship of trust between the researcher and participants. The researcher kept field notes, observations and memos, which enriched the inquiry. For example: Inquiry: What are your thoughts about the vignette [the short scene] I just read to you?
A summary of an adapted scene, the vignette. 26
Bola is a Nigerian woman living in Woolwich with her son and daughter-in-law, who identify as Black Africans despite being of British nationality. She is in reasonably good physical health. Over the past 3 to 4 years, her family has noticed her becoming increasingly withdrawn, inactive, and sometimes careless about her appearance. She has also become very forgetful, often not recognising close family members. . .
The study further employed constant comparative analysis and reflexivity in refining and tweaking subsequent interviews for theoretical saturation.23,35 For example:
Tweaking: tell me more about forgetfulness
This study was conducted in London and primarily utilised online platforms due to the increased spread of coronavirus in England. The researcher avoided face-to-face contact with participants to ensure a secure COVID-19 environment and selected participants from two Pentecostal church sites within the Black African communities in the London borough. Most Pentecostal churches believe in ‘spirit possession’.36,37
Inclusion criteria
For pragmatic reasons, the researcher included:
Black Africans
Churchgoers
Aged 20–85 years old
Male and female
Able to speak English
Capacity to make a valid decision
Compliance with online ‘terms of use’
Exclusion criteria
For pragmatic reasons, the researcher excluded:
Non-Black Africans
Non-Churchgoers
Aged less than 20 and above 85 years
Limited capacity with English
Lack of capacity to make a valid decision
Registered health professionals
Non-compliance with online ‘terms of use’.
Sampling and interviews
The study adopted convenience sampling methods.38–41 Enrolled participants provided verbal consent to participate, and each signed an informed consent form during the interviews. Thirty-one respondents (n = 31), comprising 14 women and 17 men, aged 20–85, participated in the study. The respondents were first-generation Black African migrants from West Africa, mainly carers. Each online interview lasted approximately 35–60 min. The interviews were recorded and transcribed verbatim by the researcher. The researcher excluded individuals over 85 years old from the study due to the sensitive nature of the research topic and the practical challenges of potentially exposing older participants to associated risks primarily related to increased frailty. He offered each participant a £10 voucher to reimburse their time. The motivation was reasonable, not coercive, and did not undermine respondents’ voluntary consent. The participants’ names are anonymised (pseudonyms were used), as shown in the table (see Table 1).
Details of interview participants (the sample).

Topic sensitivity
The dementia study was a sensitive topic, and the researcher carefully considered the risks, factoring in a few additional elements into the research protocol to ensure participants could access help if needed. Psychological emotions and online abuse were identified as risks and measured as medium risk. The researcher engaged in the detailed steps as a measure of managing the identified risks:
The participants were informed of the sensitivity of the research topic, and all respondents were required to give informed consent. A contingency plan was in place to halt any interviews and direct respondents to help should they need it.
The researcher was self-conscious about the power imbalance between him and the respondents. 42 He mitigated the power differences in the research using the vignette, encouraging disclosure and authenticity between him and the participants. 43
The study established clear online safety boundaries and essential principles to reduce risks. It also used an ethical checklist 44 that emphasises trust, honesty, and cultural sensitivity, ensuring that online communication is neither offensive nor abusive. Anonymity and confidentiality were priorities when managing participants’ information and online conversations.
At the end of the interviews, the researcher asked each respondent how they felt about the interview. All gave a positive response.
The researcher monitored and ensured the well-being of the interviewees by conducting a follow-up telephone call. All participants reported positive emotions afterwards.
Ethical considerations
The research received ethical approval from the Research Ethics Committee of the College of Health, Medicine and Life Sciences at Brunel University London. Approval was granted to conduct the research from December 1, 2020, to September 1, 2022, under reference number 25440-MHR-Dec/2020-28887-2. Each community church provided written informed consent before the research ethics committee approved the study and prior to the enrolment of participants. All enrolled participants gave verbal consent and signed informed consent forms during their participation interviews. Ethical issues bridge the study’s philosophical and praxis aspects linked to the research’s ontological, epistemological, and functional imperatives, 45 and the study was governed by the foundational norms of research ethics: beneficence, respect for persons, and justice. 46
Data analysis
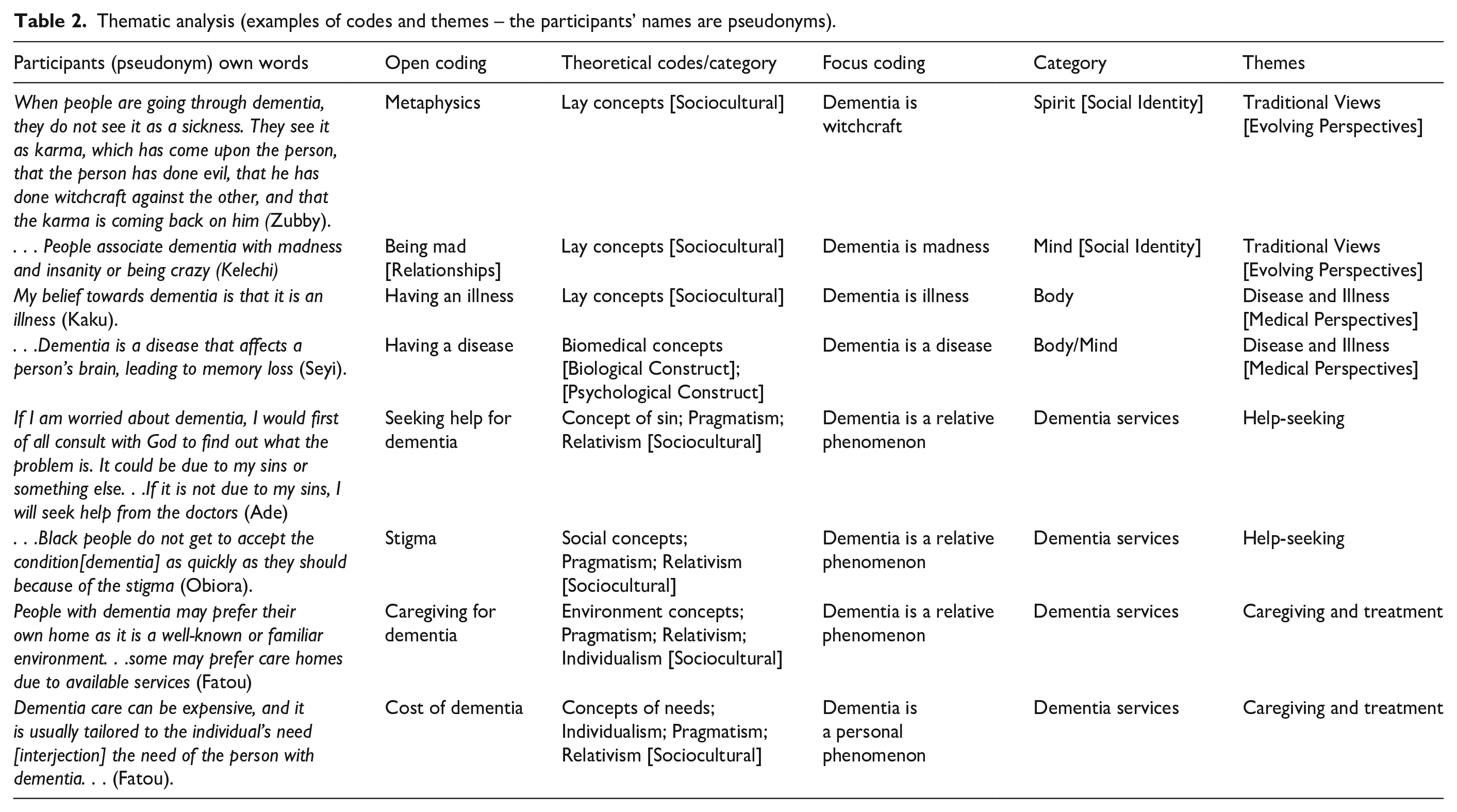
The doctoral researcher (RM) recruited, interviewed, and analysed data from March 6, 2021, to October 3, 2021. The process was concurrent, and he transcribed the interviews verbatim. Observations were recorded in his field notes. 47 The data employed a reflexive thematic analysis,35,38,39,48 informed by a grounded theory approach,20,21,49,50 which guided the coding, memoing and constant comparative analysis of the data to achieve theoretical saturation while adhering to the CGT principles.23,51 RM conducted the initial interview, data coding, and analysis and collected subsequent data. He modified and refined the emerging open and focussed codes through monthly meetings with senior academics (WM, HN, MN), who supervised the study to ensure the codes accounted for all the data related to answering the research questions and meeting the study’s objectives. This method employed a data-reduction process.20,21,23,51 The codes were sorted into categories and themes, as shown in Table 2. RM used inductive reasoning to assign concepts that explained the data (see Table 2). As part of the theoretical sampling/constant comparative method.20,21 RM kept track of his ideas in theoretical memos. He maintained memos and field notes, which allowed data to evolve (see Figure 1) into higher-level concepts and constructionist ideas23,42,51,52 The field notes were written records of observational data produced by fieldwork, 53 which consisted of descriptions of social interactions and their contexts. The theoretical memos were records of the researcher’s developing ideas and thought processes rather than a description of the social context. 49 RM stopped recruiting when theoretical saturation was achieved. The data collection and analysis were carried out concurrently (see Figure 1). The study achieved theoretical saturation when new data and analysis did not provide additional insights to the existing theoretical codes and categories, as the data and themes emerged. The researcher used a realist tale 54 to present the data, theories, and their interactions. Microsoft Excel was used to organise and manage the data. The findings demonstrated an understanding of the data and how the theories were illuminated in the Black African community in London.
Thematic analysis (examples of codes and themes – the participants’ names are pseudonyms).
A representative schematic approach for the data coding and comparative analysis. It shows the iterative flow and explains how the qualitative data were coded and reflexively analysed.
Codes and themes
Reflexivity
The vignette mitigated the power relationship between the researcher and the participants, 34 generating a rapport and relationship of trust throughout the research. Memoing helped the researcher document insights, thoughts, and sentiments about the data collection and analysis. 49 It allowed data to evolve to a higher interpretative level and constructionist ideas.23,42,51,52 The theoretical memos were records of the researcher’s developing ideas and thought processes rather than a description of the social context. 49 The researcher’s position presented a methodological challenge. He positioned himself as an insider and an outsider, 55 illuminating his ontological and epistemological perspectives. 56 Each position has advantages and disadvantages. 57 The researcher was considered ‘one of us’ 58 Indeed, the researcher is a Black African male, and some respondents called him a ‘brother’, which was an advantage in the study as it helped build positive rapport and relationships.
Epistemology delineates that lay knowledge of dementia exists. Therefore, epistemologically, the researcher presented information more meaningfully based on his insider position.56,59 An interpretive and constructionist stance based on inductive reasoning that illuminated the lay concepts of dementia/theoretical constructs. Ontologically, the insider perspective highlighted the ‘emic account’ of the dementia phenomenon 60 and was situated within a cultural relativist position. It also recognised dementia knowledge as relative to the group culture and the context in which the dementia knowledge and beliefs were subjectively rational and meaningful within the Black African culture, 61 which made sense to the respondents. The outsider perspective was the ‘etic account’ of dementia, positioned within the spectrum of positivism and objectivism, a realist perspective. 60 It highlighted the cultural difference regarding an external standard and from an ontological position that assumes a predefined biomedical concept of dementia as a neurological disease or pathology.62,63 This context refers to medical culture. The researcher, a trained medical doctor and applied medical anthropologist, is also a Black African. This highlights his positionality in the study and the potential impact on his objectivity and biases.
Results
Four key themes, each with its subthemes, emerged and were developed.
The results suggest that participants have a good understanding of dementia. The group’s perception of dementia has evolved from traditional views to a more medical perspective. Lay and biomedical concepts intersect and interact in delivering dementia services.
Traditional views
The findings suggest that the group, who are Black Africans from West African countries, hold traditional beliefs about dementia. These views reflect the respondents’ inherited or deeply ingrained thought patterns, behaviours, and actions. Participants associate dementia with witchcraft or madness, emphasising the socio-cultural heritage of Black African society. Such beliefs influence the attitudes and behaviours of the group towards dementia in the UK. However, a noticeable shift in traditional views has emerged amongst the participants. Most respondents recognise that their beliefs about dementia have evolved. For example: People in my community used to think dementia was madness or witchcraft, but things have started to change a bit. . . .you know before [interjection] Dementia is forbidden. . .[laugh] once you have dementia, they will say “obu oye ala” [meaning mad person] (Nwanne).
Therefore, the group’s understanding of dementia seems to be evolving, as most respondents appear to have moved away from beliefs in dementia-related witchcraft and madness due to their experience of living in the UK, as demonstrated.
Before I came to the UK, I thought dementia was “were” [madness] (Sesan). They would say it is either they are into witchcraft or that they are crazy . . . But a person from this society [London] would see it from a different perspective (Yemi).
However, some respondents shared accounts of the group’s lay expertise in their countries of origin but acknowledged that the practice is either invalid or in transition in London.
In Liberia, they [people with dementia] use many things like holy water and holy oil, burn incense, and use local roots and plants. But here in London, they [people with dementia] use proper medicine (Finda).
Nevertheless, some respondents believe that the practice has not been entirely abandoned, suggesting that members of the group migrated to the UK with some of their dementia-related cultural practices to preserve their cultural identities, including traditional practices for dementia treatments. For example: In Ghana, the indigenous people know how to mix the herbs and roots of plants to obtain a mixture that might aid recovery from different sicknesses. It is a practice well known to them, and they still practice it. You can even get some of these herbs and roots in some shops in London (Yoofi).
Nonetheless, most participants seem to have moved away from their community’s beliefs and traditional practices regarding dementia. However, all respondents were regular churchgoers in London, engaging in worship and prayer, which highlights their religiosity and spirituality. This, in turn, enhances their sense of belonging, socialisation, self-esteem, and overall well-being as reflected in the data.
The church is a place of worship. People with dementia can go to church, pray and worship. . .(Ben). Churches are places of worship and reverence for God. . . Churches may also be considered “hospitals” where sins, evils, and deviance can be dealt with (Seyi).
Indeed, the church is a tangible and communal expression of spirituality and religion that can collectively provide individuals with a sense of cultural identity and a framework for understanding illness, misfortune, and its treatment within the group, often involving the Black African community and a higher power. Just as a hospital offers care for people with dementia, the church can be seen as a place where those with dementia and their carers can find spiritual healing, support, comfort, and renewal. Regardless of the group’s spiritual and religious beliefs about dementia associated with sin, some participants view dementia as a disability.
Dementia is a form of disability. . . (Bello). They [people with dementia] usually lack the ability to coordinate daily activities due to cognitive impairment (Yoofi).
Similarly, regarding disability, older age and the ageing process are common factors associated with cognitive decline and difficulties in managing daily tasks. Ageing is a natural process; however, it can affect a person’s ability to carry out everyday activities, which may then be considered a disability. In line with the data, most participants associated dementia with older age and the ageing process, thus integrating it into their social identity.
Dementia comes with older age. . .(Seyi). It [dementia] is part of ageing. . .(Eze).
Furthermore, according to the data, many participants viewed dementia as a sickness, which aligns with the literature on social identity, a part of a person’s self-concept that stems from their perceived belonging to a community, influencing how individuals perceive themselves and how others might perceive them. For example: . . .Bola [the person with dementia] is sick, and her children are not happy with her sickness (Ngozi).
Therefore, most respondents associated dementia with social identity and linked it to relationships, as well as related factors such as ethnicity, religion, spirituality, immigration, socioeconomic status, disability, and occupation. Similarly, some participants also connected dementia to gender, as demonstrated in the excerpts.
I am here from Nigeria to work. Although I am a Black British national. . .Our generation is made up of immigrants in the UK (Kunle). I am a carer, and I have seen many cases of dementia, and they are mainly women. . .they are mostly women than men (Bimbo).
Indeed, most group members were caregivers and viewed dementia through a gendered lens. Traditional gender roles appeared to shape their ideas about appropriate practices in dementia care.
When I was a male carer, I was not allowed to provide care for women [with dementia] because it was inappropriate to do so (Tunde). I will say, man to man and woman to woman, out of respect for privacy. . .But naturally, women are better carers [for people with dementia] than men (Okafor).
Nevertheless, traditional gender roles, which are norms that specify how men and women should behave, can restrict and limit individual skills and choices in dementia care. However, the data showed that most participants believed their understanding of dementia and caregiving had improved during their stay in the UK.
My experience here in the UK is that the way they see dementia is not the way we see dementia in Africa. (Kaku).
Therefore, it can be inferred that many Black Africans in London are increasingly becoming aware of dementia through education, practice, and training. The participants primarily migrated from West African countries, with the majority being Nigerians, and they were predominantly caregivers.
Africans are becoming increasingly aware of dementia, as they now have access to education, information, and the internet (Nkem).
As a result, most participants in the group experienced a significant change in their understanding of dementia, shifting away from traditional views such as witchcraft and madness towards a more medical perspective. Their exposure to and extended stay in the UK played a crucial role in this transition. Most respondents, who were caregivers in the UK, highlighted the importance of professional development. They adopted a biomedical understanding of dementia through their education, practices, and training, enabling them to be more effective in their roles as caregivers.
Disease and illness
The transition from a traditional view of dementia to a more medical perspective within the group emphasised dementia as both a neurological disease and an illness. Most participants understood dementia in these two ways. While ‘disease’ and ‘illness’ are often used interchangeably in the group, ‘disease’ refers to an objective diagnosis linked to organic pathology, whereas ‘illness’ relates to a person’s subjective experiences or perceptions of feeling physically or mentally unwell.
Dementia is a disease that affects the brain (Fatou). Dementia is a disease of the brain (Remi).
The data indicates that dementia is a neurodegenerative condition, which aligns with medical literature. However, a few respondents noted that dementia is not a specific disease but rather an illness.
Dementia is not a specific disease but an impaired ability or illness (Efe).
Of course, some respondents regarded dementia as a mental illness that can significantly impact daily life and relationships within the group.
I think dementia is a terrible mental illness (Ben).
Indeed, members of the group may face mental health challenges, and practitioners must recognise and not overlook how mental illness presents, especially in cases of dementia within these communities. While the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) may influence some healthcare practitioners to argue that dementia is a mental illness, medical doctors generally do not classify it as such. Nonetheless, individuals with dementia can experience mood and behaviour changes, including aggression, depression, manic disorder, anxiety, post-traumatic stress disorder (PTSD), or psychosis. Therefore, a holistic approach to dementia in the Black African community is essential, particularly when it affects a person’s behaviour and cognitive functions. For instance, some respondents associated dementia with forgetfulness.
People with dementia usually forget things, and they usually find it difficult to remember things (Bimbo). They forget things, forget their flat, forget their family, forget their friends, and can’t remember things. Then, you could tell, hay, they have got dementia (Merida).
However, forgetfulness in daily life is a complex phenomenon, and recognising when it becomes a cause for concern is essential. Many respondents perceived it as a sign of dementia.
If the person is showing signs like forgetfulness. . .these things would point me towards a dementia condition (Kofi).
Nevertheless, it is common to forget things occasionally, and a certain degree of memory loss can occur in specific situations. However, forgetfulness is a risk factor for dementia and is associated with brain function in medical literature. Likewise, many participants described dementia as brain damage that causes memory loss, as shown in the excerpt: Dementia is a disease that affects a person’s brain, leading to memory loss. . . It is associated with the deposition of proteins in the brain cells, eventually leading to dead cells in the brain (Seyi).
Indeed, participants regarded dementia as a neurodegenerative disease, indicating that it is a neurological disorder capable of causing cognitive decline and memory loss. Consequently, dementia was viewed as a pathology and aligns with medical literature.
Dementia is a pathology. . .(Yemi).
Of course, most respondents were caregivers and, unsurprisingly, adopted the biomedical understanding of dementia. Like some others, Ngozi mentioned that chronic conditions can cause dementia.
. . .HIV and TB can cause dementia (Ngozi). Diabetes [interjection]can cause dementia (Kelechi).
Some participants considered genetics a risk factor for dementia.
I think one of the causes of dementia is hereditary (Zubby).
Furthermore, most participants considered sociocultural factors as a risk for dementia. These factors can negatively affect health, well-being, and individual behaviour and attitudes. For example, the data highlight these sociocultural influencing factors.
Older age and ageing: Older age is a risk for dementia, and we cannot prevent growing old (Ejiro).
Alcohol and smoking cigarettes: Alcohol and smoking are not good for our well-being. . .it causes dementia (Bimbo).
Environmental factors: Other things like noise and air pollution can cause dementia (Nwanne).
Loneliness and insomnia (difficulty getting to sleep): . . .And when a person is lonesome and lonely, lacking social events, that could lead to dementia. My dad has been lonely. He does not get involved in social events. . .My dad finds it difficult to sleep at night (Yemi).
Moreover, some participants associated poverty with risk factors for dementia, linking it to suffering.
When I say hard life, I mean living a difficult life full of stress, unemployment, financial distress. . . (Nonye).
Some participants perceived falls and head injuries as risks for dementia: . . .Falls and head injuries can cause dementia (Kunle).
Likewise, the idea of preventing dementia resonated deeply with the group. Most participants mentioned resilience, healthy behaviour, and lifestyle as preventative measures.
. . .being free from stress by being resilient, socialising and being in a safe and good environment that is not noisy and dirty can prevent dementia (Kelechi). Eating healthy food. . . can also help us to maintain good health. In short, keeping a healthy lifestyle is the key to preventing dementia (Yetunde).
Furthermore, many respondents viewed mental agility as a preventative measure against dementia, as explained in the data.
Keep yourself busy, play games, and read papers or magazines regularly to keep your mind stimulated [interjection]. These things can prevent dementia (Fatou).
Moreover, most respondents emphasised the importance of exercise in preventing dementia. In line with the existing literature, exercise can enhance memory and cognitive skills, as well as boost mental well-being. More importantly, Yemi notably provided an exercise prescription.
As I said, the most important thing is to prevent, provide support if a person has dementia [cough] and partake in bodily exercise. You don’t have to be a member of a gym before you can do exercise. You can sit up, you can do stretches, you know, you can watch videos and do some small exercises. This helps as much as possible to improve blood flow through all parts of the body, including the brain and all the other parts of your body. It keeps you healthy (Yemi).
Additionally, participants viewed routine medical checks, including neurological tests, brain scans, and blood tests, as a way to prevent dementia within the group.
. . .Particularly, Black people should learn to monitor their vital signs, such as blood pressure and pulse rate, or they could go for a medical check-up as needed (Seyi).
Indeed, some participants described dementia as a consequence of stroke and high blood pressure, which aligns with the medical literature.
My mother was diagnosed with a stroke [interjection] and high BP. Before she died, the doctors said she had vascular dementia (Marie).
However, for most respondents, the strategy for preventing and managing dementia in the Black African community should focus on green and blue spaces. The idea of preventing dementia through nurturing rather than nature resonated strongly with the group, as exemplified in the excerpt: But you also have to create open spaces and gardens [Interjection]. . .Take the person with dementia to the park. The person should have a 1 to 2 km walk [Interjection], listen to music, watch television, and life will go on. . . Give people a comfortable house and let them have fresh air (Okafor).
Reflecting on the data, nurture encompasses all the sociocultural and environmental factors that shape the group’s behaviour, while nature can refer to the group’s innate, individual, pathological, and genetic characteristics. Regardless, most participants have adopted person-centred care and biomedical concepts of dementia due to their prolonged stay in the UK. However, a key challenge in dementia care and prevention within Black African communities will involve preserving the personhood of individuals with dementia in sociocultural terms. Dementia encompasses more than just an individual’s organic pathology, as indicated by the risk factors. Nonetheless, the shift from a traditional view of dementia within the group to a more medical perspective represents positive progress. This transition in understanding has positively influenced the group’s willingness to seek medical assistance for dementia.
Help-seeking
The findings show that the concept of help-seeking revealed that the Black African population followed predictable steps when seeking assistance for dementia, involving a complex decision-making process shaped by both traditional and medical perspectives. Help-seeking behaviour naturally resonated with the attitudes and stigma within the group. Most respondents believed that stigma impacted help-seeking for dementia.
The only problem with dementia in the Black community is that Black people do not get to accept the condition as quickly as they should because of the stigma associated with it (Obiora).
Certainly, stigma can lead to discrimination, prejudice, and social exclusion. Respondents explained how families in the Black African community tend not to discuss dementia and how people with dementia often feel isolated within their communities. For example: . . .Some would not discuss it. They [people with dementia] feel isolated and isolate themselves from the community (Eze).
Indeed, stigma leads to marginalisation within the group. However, most participants had access to the internet. They recognised that it influences their help-seeking behaviour for dementia, as most respondents used computers or devices to access dementia information, as shown in the excerpt: Normally, the first thing to do is to [Interjection] thank God for Google; people Google up a lot of [dementia] information (Yemi).
Nevertheless, for some participants, family members and relatives were the primary sources of support and information about dementia and related issues. Families dealing with dementia can seek support from specialised organisations and support groups.
I will discuss it [dementia] with my family and close friends (Ben).
Furthermore, most respondents indicated they would prefer to seek help from their GP instead.
I would make an appointment to see the GP as a priority (Bello).
However, some participants were sceptical about seeking help from their GP due to the associated stigma. They preferred to keep the dementia diagnosis secret, implying that dementia is linked with shame, as illustrated in the excerpt: But the point is that as a man, I may be worried about the stigma and may not want to see a doctor. Because as a man, when you start losing your mind, you might become a laughingstock, and your wife and children might also want to keep it secret (Kaku).
Reflecting further on the data, shame can be defined by a negative self-assessment, often arising from perceived failure to meet personal or societal standards, which leads to a desire to hide or withdraw. Shame can significantly impact mental well-being. However, as participants continued their stay in the UK, these evolving perspectives, particularly the shift from a more traditional view to a more medical approach, had a positive effect on help-seeking behaviour. Nonetheless, the concept of sin may have negatively influenced help-seeking for dementia within the group. For example: If I am worried about dementia, I would, first of all, consult with God to find out what the problem is. It could be due to my sins. . .If it is not due to my sins, I will seek help from the doctors (Ade).
Of course, while the concept of sin is not a defining characteristic of Black African communities, it is a traditional view that may impact the pursuit of medical assistance in the group. Some participants associated dementia with morality and divine punishment, possibly leading them to seek divine forgiveness. Dementia is a relative phenomenon, and feelings of guilt, stigma, and shame influence help-seeking behaviours within this group. Yemi suggested that anthropologists could play a crucial role, emphasising the need for cultural competence in dementia services.
. . .Anthropologists will know what all this is about and put things together (Yemi).
Indeed, clinical anthropologists or anthropologists in public health can apply anthropological perspectives to understand dementia-related issues, especially within Black African communities and dementia services in the UK. Applied medical anthropologists play a crucial role in promoting health equity by utilising their specialised knowledge to improve dementia practices and address health disparities related to dementia, alongside other critical health issues affecting Black African communities in London.
Caregiving and treatment
The data indicates that the model of dementia care and treatment strongly resonated with the group. Caregiving involves assisting and supporting someone with dementia, while treatment refers to the medical or therapeutic interventions used to manage the condition. Most participants believe that there is no treatment or cure for dementia.
There is no treatment for dementia. I have not seen anybody cured of dementia (Okafor).
However, most respondents believe that medicine is used to treat dementia solely for palliative purposes, which aligns with medical literature.
. . .but some medications for dementia may help you sleep or relax (Yemi).
In accordance with existing medical literature, various medications such as cholinesterase inhibitors, NMDA receptor antagonists, and antipsychotics are used to manage symptoms and improve the quality of life for individuals with dementia. Therefore, dementia is mainly treated symptomatically, as the group suggests, meaning that care should focus on alleviating symptoms and stress related to the illness to enhance the well-being of those living with dementia and their carers. However, further literature indicates that some newer medications have shown evidence of slowing the progression of Alzheimer’s disease in its early stages. Additionally, most respondents believe that Black Africans with dementia predominantly receive domiciliary care rather than residential care.
If you visit a care home, you will see less than 5% of Black people in there, maybe not even up to 2%, because most Black people with dementia stay in their homes (Eze).
Nonetheless, the decision between residential and domiciliary care depended on the individual’s needs, costs, and affordability, as indicated in the excerpt: Dementia care can be expensive, and it is usually tailored to the individual’s need [interjection] the need of the person with dementia. . . (Fatou).
Therefore, dementia is a personal and relative phenomenon. The group’s approach to dementia care emphasised individualism and pragmatism, with most participants expressing a need for therapy.
The person taking care of a person with dementia needs therapy. They need therapy for themselves because the labour is so much, and they are watching their loved ones change over time (Yemi).
Reflecting on the data, various therapies can offer vital support and a safe environment for individuals with dementia and their carers to express their feelings and concerns, as well as to learn and develop coping strategies. Therefore, dementia carers must be equally involved and central to the dementia care and treatment process within the Black African community. For example, the group regarded prayer and music as beneficial forms of therapy.
We can pray to God for help and healing [for dementia] (Obiora).
Indeed, most respondents believed that prayer and music can be comforting and uplifting, and may therefore benefit individuals with dementia and their carers, evoking memories and enhancing overall well-being, as expressed in the excerpts: The prayer was very comforting and encouraging. . .(Marie). Singing gospel songs can be good. It could help to improve their [people with dementia] memory and thinking (Ben).
Therefore, as indicated by the data, prayer and music can offer comfort, routine, and spiritual connection, fostering a sense of belonging in dementia care. Consequently, providing holistic and practical support that is familiar to people with dementia and their caregivers is crucial for managing the challenges of dementia. The sociocultural model of dementia services within the Black African community in the UK signifies a significant transition. This shift recognises the unique needs and challenges faced by individuals with dementia and their caregivers in this community. It emphasises the importance of addressing personal needs, preferences, prevention, and community resources for support. This approach, which considers dementia beyond just a medical condition, can help reduce stigma and promote the overall well-being of individuals with dementia and their caregivers within the group, including their spiritual needs. It highlights person-centred care and the vital role of caregivers, ensuring they feel valued and are central to the care and treatment process.
Discussion
Four main themes, each with its subthemes, emerged and were developed. The main themes included (i) Traditional views, (ii) Disease and illness, (iii) Help-seeking, and (iv) Caregiving and treatment. Findings show that witchcraft and dementia-related beliefs are consistent with the broader dementia literature on Black African populations. 64 This study added witchcraft to the broader dementia literature on BAME in the UK, specifically on Black African populations. 2 However, the research is limited to first-generation migrants from West Africa and church populations. Furthermore, the findings indicate that respondents evaluated dementia according to what they considered reasonable given their age, gender, education, occupation, religion and spirituality, ethnicity, socioeconomic status, and migration status, thus situating social identity. 65 The participants were primarily carers, and most respondents identified as Nigerian. Religion significantly influenced the group’s understanding of dementia. Some respondents perceived sin as a cause of dementia and viewed it as a punishment from God, linking dementia with morality and guilt. Some would instead seek divine forgiveness, 66 thus delaying seeking help from doctors. The dementia knowledge and beliefs in the group were transcendental and associated with metaphysical properties. 67 The dementia identity theory was situated in the mind/brain68–70 and on the social relationships with others. 65 Hence, some respondents perceived dementia as madness/craziness. 71
Nevertheless, the findings show that these traditional views about dementia appear to be transitioning within the group, as the results demonstrated that the majority of respondents experienced a significant shift in their understanding of dementia. They are moving away from traditional beliefs such as witchcraft, madness, curses, sin, and spirituality towards a more medical perspective that emphasises disease and illness, highlighted by risk factors including genetics, chronic medical conditions like strokes, diabetes, infections such as HIV and TB, and trauma from falls and head injuries. The group emphasised the importance of diagnosing dementia through medical tests, including brain scans, neurological assessments, and blood tests. Exposure to and prolonged stay in the UK played a pivotal role in this transition. In addition, most participants viewed dementia as forgetfulness and associated being forgetful with memory loss and older age. However, forgetfulness in everyday life is a complex phenomenon. 72 Age is a biological marker and a fundamental prognostic index in diagnosing, preventing and treating dementia. 73 Many respondents, mainly carers, identified older age, poverty, insomnia, alcohol use, smoking, loneliness, and environmental factors as risks, which aligned with the existing literature. All participants perceived no medical cure for dementia and emphasised that the medications used for treatment are merely for palliative purposes. Prevention of dementia focuses on reducing risk factors through lifestyle changes, including a balanced diet, access to green/blue spaces, and regular awareness of dementia, as well as managing underlying health conditions through routine medical tests and check-ups.
However, reflecting on the findings, relativism 74 holds that there is no absolute knowledge and beliefs about dementia, suggesting that every community in the UK will have a different experience of dementia2,3,18 dependent on sociocultural factors. The primary task in dementia services is maintaining the personhood of the person with dementia, necessitating the perception of personhood in sociocultural rather than individual terms 75 as the findings suggested that dementia can also be medically stigmatised. Health practitioners may hold negative attitudes towards dementia within Black African communities. Nevertheless, prevention and management of dementia via nurture, including green and blue spaces and comfortable housing, resonated strongly in the group 76
Therefore, the results indicate that community dementia services must be designed and tailored more appropriately to the sociocultural needs of the person.75,77 Some respondents conceptualised dementia as a disability 78 and perceived gender as a risk factor. Dementia as a disability is not an individual’s pathological characteristic but an outcome shaped by sociocultural and environmental factors. 79 The lay and biomedical concepts of dementia intersected in the provision of dementia services within the group. Most of the respondents were carers who had assimilated the biomedical ideas of dementia through education, training and learning,62,63 to be effective in their caregiving roles in the UK.
Although the results show that traditional views on dementia are shifting within the group, the findings suggest that the dichotomy between lay and biomedical knowledge of dementia may be false (see Table 3). This proposition can be crucial for the destigmatisation of dementia. 5 The lay and biomedical concepts are interconnected, interactive, dependent, and not mutually exclusive, as demonstrated in the sociocultural model (see Figure 2). Most respondents described dementia as both a neurodegenerative disease and a mental illness, with some linking it to genetics. Therefore, the association of mental illness with dementia in the group should be acknowledged and considered in the context of the whole person, especially when it impacts their behaviour, cognition, and ability to perform daily tasks. It may also be crucial to thoroughly explore the connections between genetics and dementia in Black African populations. 80
Themes.


Sociocultural model.
Furthermore, the findings highlighted that the association of dementia with witchcraft is linked to stigma and abuse.81–83 This perception can negatively impact help-seeking for dementia in the UK. It also presents a pressing need to safeguard people with dementia in the Black African community from abuse. However, knowledge and beliefs about dementia in this group are not static; they continually evolve due to the participants’ ongoing stay in the UK and advancements in media technology, such as the internet 84 and increasing access to education and training. Still, prayer 85 and music 86 provide a sense of healing and comfort, which could serve as therapy for dementia in the group. Finally, the sociocultural model is illuminated:
The sociocultural model is a three-dimensional representation of lay concepts and dementia services in the Black African community
Holism suggests that the lay concept of dementia is holistic87,88 and a sociocultural approach that encompasses the whole person. It includes the evolving traditional views and medical perspectives on dementia. Individualism advocates for maintaining the personhood of the person with dementia within sociocultural contexts rather than solely in individual pathological terms, 75 ensuring that dementia care is tailored to the people’s needs, preferences, and circumstances. Pragmatism suggests that person-centred care and cultural competence in dementia practice and services are essential. 89 Dementia is a relative phenomenon dependent on sociocultural contexts, illuminating the need for a community-based dementia care strategy. 90 Applied medical anthropologists can be valuable in dementia services in the UK.
Strengths and limitations
The study has a solid methodological and theoretical underpinning. It involved lay respondents from all walks of life, including carers, thus ensuring adequate data to develop a robust and valid understanding of dementia and achieve credibility and theoretical saturation. This study is a rich and authentic dataset. However, the research is limited to first-generation immigrants from West Africa and the church population. This means that the study is not generalisable to all Black African populations. All the participants had a formal education. A setting where the participants have no formal education can limit the degree of transferability. Additionally, the study excluded people aged 85 and older, which limits the generalisability of the research.
Recommendations
The study recommends dementia outreach as an intervention in educating and training the Black African population in the UK on dementia to reduce stigma and enhance dementia awareness.
Implications for policy and practice
Health practitioners and policymakers must be more aware of and consider lay belief systems when interacting with community patients, service users, and caregivers.
Conclusions
The study concluded that the group does not lack knowledge of dementia. Their understanding and beliefs about dementia are evolving, and further efforts are needed to enhance awareness through education, training, and outreach to support individuals with dementia and their families within the Black African community.
Footnotes
Acknowledgements
The author would like to acknowledge the support of Dr. Wendy Martin, Professor Holly Nelson-Becker, and Professor Meriel Norris for their exceptional guidance and encouragement throughout this study. The author would also like to thank all the respondents who participated in the study. All names used are pseudonyms and do not represent the actual names of the participants.
Ethical considerations
The research received ethical approval from the Research Ethics Committee of the College of Health, Medicine and Life Sciences at Brunel University London. Approval was granted to conduct the research from December 1, 2020, to September 1, 2022, under reference number 25440-MHR-Dec/2020-28887-2.
Consent to participate
All enrolled participants gave verbal consent and signed informed consent forms during their participation interviews.
Consent for publication
Each community church provided written informed consent before the research ethics committee approved the study and prior to the enrolment of participants.
Author contributions
Raphael Chinedu Mokwenye is the sole author of the research paper and is responsible for the overall content, including conceptualisation, participant recruitment, data collection and analysis, writing the initial draft, and reviewing and editing.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.