
Abstract
Keywords
Background
For research to effectively inform knowledge of how different people understand and experience dementia, one would need to understand the ethnicity and cultural backgrounds of the populations.1,2 For example, in Africa, knowledge about dementia can be informed by sociocultural factors such as occupation, education, gender roles, age, spirituality and religion, 3 and cultural contexts that are socially transmitted from one generation to another4,5 These sociocultural contexts, such as witchcraft 6 or spirituality and religion impacted African people’s understandings, meanings, and beliefs about dementia,7 -10 drawing upon values, customs, relationships, and practices that shape the way Africans communicate, think, and behave that characterize Black Africans, particularly with people with dementia and caregiving for dementia.11 -13
Thus, this current work is designed to understand and improve the health of BAME (defined as all ethnic groups except White ethnic groups) communities in the UK focused on dementia and the Black African populations to inform dementia practice and policy. Equal opportunity to access dementia services is a priority and essential for a racially and ethnically diverse population in the UK, including those conducting dementia research. 14 Dementia services in the UK require an understanding of lay dementia knowledge to provide patients, particularly Black African communities, with the dementia services needed. 15
Studies in the UK suggested that Black Africans lack dementia knowledge 16 and that African populations rely on religious support and are underrepresented in dementia specialist services. 17 When Black Africans in the UK use dementia specialist services, they usually do so later in the condition18,19 and are often at higher risk of not being diagnosed and prescribed the appropriate care and medication for dementia. 19
In the UK, about 25 000 BAME (Black, Asian and Minority Ethnic) population are living with dementia, and this has been projected to increase to about 172 000 by 2050.20,21 The African population represents a significant population in the UK. According to the 2021 Census, approximately 2.4 million Black individuals reside in the UK, which accounts for 4.2% of the population. Africans comprise more than half of this population, with 1.5 million people representing 2.5%, increasing from 1.8% in 2011. Black African people are the largest ethnic group within this population and are comprised mostly of Nigerians (0.5%), Somalis (0.3%), and Ghanaians (0.2%). 22 Thus, Black Africans can lead to increased dementia prevalence in the BAME in the UK.23,24
Moreover, average life expectancy has improved globally. 25 It has increased in Black African populations and was expected to rise above the average of 65 years in the UK due to improved quality of life and access to essential health services. 26 Therefore, we would expect dementia to rise among the Black African populations in the UK, underscoring the urgency of this current research to explore the lay knowledge and beliefs toward dementia among Black Africans informing dementia practice and policy.
This study systematically reviews the literature on lay knowledge and beliefs about dementia using evidence synthesis methodology.27,28 The research identifies the qualitative studies relevant in Africa and the UK and identifies gaps in the UK studies on dementia among the African population. This review excluded studies outside of the UK and Africa because the research is focused on the UK to inform the UK dementia services. Even though most of the qualitative studies on dementia are conducted in Africa, the UK, and the United States. The evidence provided in most studies in the United States was on Black Americans. 14 The data did not apply to the UK’s Black African context, which is the population of interest in this study. Therefore, research from the United States was excluded from the review to enable the current researcher to obtain the best evidence and reach the best conclusion. Nonetheless, the researcher ensured that the review process was robust. Further, it emphasizes the fact that context is essential in this study.
Research Context
Lay people from Black African communities may lack biomedical knowledge of dementia. However, Black Africans have lay knowledge and beliefs about dementia based on a shared sociocultural understanding of the dementia phenomenon in the Black African communities that frame or shape their dementia service use and non-use pattern within a broader sociocultural context.29,30 So, our working definition of lay knowledge and beliefs about the definition is the “general cultural stock of knowledge” 31 held by the local members of the Black African communities who are not medical or health practitioners. Of course, everyone has access to their own type of lay knowledge. 32
Review Question
The research used evidence synthesis to explore lay knowledge and beliefs about dementia among Black African populations in the UK and Africa. It aimed to identify gaps in UK studies and understand how dementia is constituted and constructed among Black Africans.
Review Question
What are the lay knowledge and beliefs toward dementia among the Black African populations in the UK and Africa?
Aim
The review aims to identify gaps in the UK literature.
Objective
The objective is to understand dementia services for the Black African populations in the UK by understanding how dementia is constituted and constructed among the Black African populations in the UK and African studies.
Methods
This study systematically reviews the qualitative studies on lay knowledge and beliefs about dementia using an evidence synthesis principle27,28 to address the research question.
Search Strategy
The research strategy covers 2 areas of literature search. Firstly, a comprehensive literature search on the research topic was performed using Google Scholar to overview the research topic. Google Scholar is a part of the popular WWW search engine, which means there were no limits on the languages covered, keywords allowed per search, and the list of covered journals. 33 Given the vast amount of literature, most papers were outside this study’s scope, and it was impossible to review them systematically. Nevertheless, most of the studies on dementia in the African population were conducted in Africa, the UK, and America. However, the researcher excluded studies conducted in the United States on the grounds of transferability since the focus was on Black Africans and the UK. Dementia studies in the United States were mainly conducted on African Americans 14 and not within the context of Black Africans.
A systematic literature search was conducted in the second search to identify relevant studies.27,28 Four databases were used to find peer-reviewed articles and provide literature on the topic. The databases were selected to enable a search strategy for research published in a broad disciplinary tradition. The search was conducted from 3 September 2017 to 17 October 2022. Five years of searching databases and reporting ensured the robustness of the review process. This added rigor and quality to the study and helped the researcher achieve trustworthiness. It also helped the researcher learn and appreciate the breadth and depth of dementia knowledge and access current studies on the topic. The researcher used search words as identified inductively from the literature, and were “dementia,” “Alzheimer’s,” “culture,” “religion,” “anthropology,” “belief,” “perception,” “knowledge,” “lay,” “view,” “stigma,” “attitude,” “constructionism,” “Africa,” and “UK.” Each keyword and the phrase were initially used singly and combined using the Boolean operators “AND” and “OR.” Thus, the researcher undertook the search and launched the literature quality appraisal. A set of the combined search terms is as indicated and was used in each database.
(Dementia OR Alzheimer*) AND (Cultur* OR Relig* OR Anthropol*) AND (Belief* OR Perception* OR Knowledge OR Lay OR View* OR Attitude* OR Stigma OR Constructionism) AND (Africa OR UK).
The researcher searched 4 databases: Scopus, Web of Science, Medline, and PubMed. Scopus was used because of the interdisciplinary nature of the study topic. Scopus delivers the world’s research output in medicine and social sciences. It covers life sciences, social science, and health science and covers a broader journal range in keyword searching and citation analysis. 33 Web of Science was used because the database supports various scientific tasks across diverse knowledge domains. It covers the oldest publications, indexes, and archived records dating to 1900. 33 Hence, the researcher used PubMed and Medline because of the study topic’s relation to clinical medicine and health science. PubMed focuses on medicine and biomedical sciences, 33 although PubMed has an interface that searches Medline.
The 4 databases were selected to enable a search strategy for research published in various disciplinary traditions, including broader social sciences, clinical medicine, and health sciences. These combined characteristics of databases enhanced the utility of medical literature and social sciences in meeting this study’s academic and professional needs. In each database, date limits were not applied to the search to consider a broader perspective. The set of papers on return was screened for eligibility to be included in the review. Nonetheless, this study literarily used only 3 electronic databases (see Table 1) because PubMed was an interface that searched Medline. So, Medline is the same as PubMed. The researcher used Google Scholar to overview the research topic. The review augmented the electronic search with backward and forward reference searching of included articles and carried out grey and manual book searches.
Search Strategy and Results.

Eligibility Criteria
To be included in the review, papers needed to meet the eligibility criteria for inclusion27,28 and papers that did not meet the eligibility criteria were excluded from the research (see Table 2). The papers included in the review were published peer-reviewed articles with available abstracts and full text written in English. The review excluded studies outside the UK and Africa. The focus of this study is to identify gaps in the UK. As noted, some of the few studies on African populations were conducted in the United States among African Americans rather than Black Africans. 14 Therefore, this study excluded papers conducted in the United States on the grounds of transferability and confirmability. 34 The evidence provided in the studies conducted in the United States does apply to the UK context using the trustworthiness discourse.34 -36
Eligibility Criteria for Inclusion and Exclusion Using the APSO Framework.

Furthermore, this study included only research reporting qualitative studies as this was the methodology appropriate to the review question. 37 Therefore, quantitative studies are excluded. However, quantitative analysis can consist of expressions of attitude and epidemiology, and often close-ended and expressed numerically to ensure statistical representation 38 rather than decisions gathered through contextualized inquiries or interviews to learn about feelings, meanings, attitudes, behaviors, and experiences39 -41 of dementia. Therefore, the review included mixed-method studies 38 of dementia because when mixed studies are used, the data can gather the target audience’s demographic experiences, attitudes, feelings, behaviors, and meanings of dementia. 42
In addition, the inclusion and exclusion criteria are used when screening results from the initial database to ensure relevance to the review question. The researcher utilized the APSO checklist, which he developed inductively from the papers, and further, the study used the CASP qualitative checklist. 43 The tools were an initial practical framework to appraise the evidence and ensure relevance to answering the review question. Finally, the researcher uses the trustworthiness criteria (EOR) to evaluate the qualitative studies.34,44 The APSO checklist is as demonstrated.
APSO Checklist
The APSO checklist is developed inductively by considering the papers and is like the PICO strategy.45,46 The researcher wanted to ensure that the studies considered for this review contained the right populations (see Table 2). This review is not about dementia intervention but about dementia knowledge. Indeed, many UK papers were on BAME. However, only a few had Black Africans as respondents or participants, and the researcher wanted to ensure the study’s outcome was based on dementia services. Using the APSO checklist ensures the appropriateness of the articles, population, study design, and outcome of the research and offers rigor and the ability to synthesize the evidence needed for the review using this criterion as highlighted:
• Is it a published journal article?
• Is the abstract available?
• Is the full text available?
• Is the article written in English?
• Is the study conducted in Africa with African populations?
• Is the study conducted in the UK with African populations?
• Is it a qualitative study?
• Is it a quantitative study?
• Is it a mixed-methods study?
• What is the outcome of the study?
• Is the outcome relevant to the current study?
The Identification of Studies to be Included or Excluded
The study identification process is divided into 2-stage operations:
(i) Level 1 screening, and
(ii) Level 2 screening process.
Level 1 was done using the publication modality, whilst the level 2 process was done using the APSO checklist as illuminated above, and then the CASP 43 qualitative checklist for quality appraisal of the selected articles.
In the level 1 screening, the papers identified from the 3 central databases were assessed using the APSO checklist, for example, based on peer-reviewed journals, available abstracts, available full text, and establishing that the papers were written in English (as illustrated in Tables 2 and 3).
Screening of the Included Papers Using the APSO Checklist.

In the level 2 screening, the researcher removed the duplicates, and the remaining papers were screened based on relevance to the study using the APSO checklist (please refer to Table 3). The use of the APSO checklist by the researcher was essential because the evidence synthesis needs to be directly relevant to the population of study and phrased in such a way as to facilitate answering the research question. Therefore, the APSO checklist made the literature review process more transparent and provided quality and rigor in the review process. It focused the evidence synthesis on peer-reviewed articles with African people as respondents or participants in the qualitative studies and excluded studies outside of the UK and Africa. More so, the researcher was interested in the outcome of the dementia services. The researcher’s professional and personal experiences of providing care for a family member with dementia, his clinical background, and being a Black African in the UK situated his positionality47,48 and biases in the review and met his interest as an insider and outsider in the review and evaluation process.49,50
So, the inclusion and exclusion criteria were used when screening results from the initial database. In addition to the search and ensuring relevance to the research question, the researcher used the APSO checklist (see Table 3) when reading titles and abstracts and the full article to ensure relevance and the ability to answer the research question. The included articles were then appraised using the qualitative checklist of the Critical Appraisal Skills Programme 43 (see Table 4). The researcher used these checklists to screen and appraise the papers methodologically and evaluate the quality of the included articles.
Quality Assessment of Included Studies Using the Critical Appraisal Skills Programme: Qualitative Checklist.

Indeed, 22 papers were included in the review (n = 22), although Armstrong et al’s 51 study and Mkhonto and Hassen’s 8 paper were problematic. Armstrong et al’s 51 study explored the perspectives of Black and Asian people living with dementia and their carers in the UK. Of the 15 participants, 7 were of Black ethnicity, and all were Caribbean. Some participants reported birth in African countries such as Kenya and Uganda, but all those who reported birth from the African countries defined themselves as South Asians. Nevertheless, the researcher included the UK study in the review because the paper contains Black Caribbean respondents, and the findings were relevant to the current study. Whilst Mkhonto and Hassen’s 8 paper involved 19 nurses; even though this current review excluded studies with a health professional, the researcher included the paper because the study involved 18 family members; 2 of the 18 family members were of Black African background and were not health professionals.
Quality Appraisal
The included studies were assessed against the Critical Appraisal Skills Programme. 43 The CASP systematic review qualitative checklist highlighted ten questions to help make sense of the review papers as a quality measure. The appropriateness of the methodology, for example, research design, research methods, and findings were considered. 43 For instance, 3 broad issues were considered when appraising the included studies:
(i) Were the results of the study valid?
(ii) What are the findings?
(iii) Will the findings help understand dementia phenomena?
Subsequently, the articles were judged as high, moderate, or low quality. No low-quality papers were identified in the studies (see Table 4).
CASP (2018) Checklist
Was there a clear statement of the aims of the research?
Is a qualitative methodology appropriate?
Was the research design appropriate to address the aims of the research?
Was the recruitment strategy appropriate to the aims of the research?
Was the data collected in a way that addressed the research issue?
Has the relationship between the researcher and participants been adequately considered?
Has the ethical issue been taken into consideration?
Was the data analysis sufficiently rigorous?
Is there a clear statement of findings?
How valuable is the research?
Quality Assessment
The CASP checklist is designed to be used as a scoring system. However, the researcher adapted the scores by assigning a maximum of 1 point per item, 14 with a possible score ranging from 0 to 10 (lowest to highest quality, respectively). He gave a partial point (0.5) if the study population was not entirely Africans but a multi-modeling of ethnicity and if the data analysis failed to provide separate findings for the African people in the study. Therefore, a score of 7 to 10 was judged as a high-quality study, 5 to 6 was evaluated as a moderate-quality study, and a score below 5 was considered a low-quality study. Still, no low-quality paper was identified in the study. Seventeen papers (n = 17) were regarded as high quality, and 5 (n = 5) papers were considered moderate-quality studies. Baghirathan et al’s 52 paper was the only study that assessed the relationship between participants and the researcher’s biases. Therefore, all the papers needed more positionality and reflexivity. Concerning the Armstrong et al’s 51 and Mkhonto and Hassen’s 8 studies, although the papers were problematic, the studies were included, and their findings were significant in answering the research questions.
Evaluation Discourse (EOR)
The studies were evaluated further by drawing on philosophical and evaluation discourses,53 -55 based on the research, epistemological and ontological concepts, 56 and mainly used trustworthiness criteria.34,44 The criterion has been generally accepted as the platform for evaluating qualitative studies. It offered sufficient flexibility to accommodate the best evidence and practices for achieving rigor and trustworthiness within the qualitative paradigm. It advocates for 5 key concepts:
Credibility
Transferability
Dependability
Confirmability
Authenticity
These 5 key concepts are used to evaluate the included literature, assess whether the studies were guided by theory, methods, and empirical data, and assess their outcomes and relevance.
Overall, twenty-two studies (n = 22) met the eligibility criteria and were appraised and included in the review (Table 4). All the UK papers were a multi-modeling of ethnicity in the study. Nine studies (n = 9)16 -18,51,52,57 -60 are research conducted in the UK. Thirteen studies (n = 13)7 -13,61 -66 are research conducted in Africa (5 [n = 5] studies from South Africa, 2 [n = 2] studies from Tanzania, 1 [n = 1] study from Congo, 2 [n = 2] studies from Uganda, 2 [n = 2] studies from Nigeria, and 1 [n = 1] study from Ghana].
All the studies were valuable based on the topic, research design and methods, and the outcome of the studies, offering essential insights into dementia services in Africa and the UK with African populations. However, they were limited in methodology and lacked the researcher’s positionality and biases (see Table 5). All the UK papers were multi-ethnic studies, and the studies did not separate the findings of the Africans from the Caribbean people. Therefore, based on the discourse criterion, the findings were valuable but unreliable. Nevertheless, Berwald et al 16 suggested that Black Africans lacked dementia knowledge. This finding is invalid as the study had no separate data for the Black African population. Thus, the conclusion drawn from the study is not credible and lacks authenticity for the Black African community in the UK (Table 6).
Identified Gaps in the Literature and Plans for an Empirical Study in the UK.

Extracted Data From the Included Papers.

Furthermore, the studies show that the African populations used religious and spiritual support from churches and relied on friends and family for dementia advice, support and care.16,17 This suggests that the respondents have knowledge and beliefs about dementia that frame or shape their dementia service use and non-use within a broader sociocultural context. So, the current researcher considers that the participants have lay knowledge and beliefs about dementia, which the authors did not consider. Indeed, dementia can be transcendental, 67 and the lay concepts of dementia are holistic.5,29,30
However, the data illuminated a perceived lack of cultural sensitivity from GPs, and the respondents perceived that GPs lacked dementia knowledge. 17 This suggests epistemic tensions between biomedical and lay knowledge 68 about dementia in the Black African community and that medical doctors and laypeople could view dementia from different frames of reference and thus provide the reason why participants may have had negative interactions with their GPs. 17 Indeed, Black Africans in London presented late to the inner London memory services. 19 Nonetheless, the current researcher is a medical doctor and an applied medical anthropologist, which defines his positionality and biases in this study, and he believes the biomedical and lay concepts can interact as delineated by the concept of intersectionality. 69 Let us note that researchers’ backgrounds, positionality, and biases can impact their research approach and outcome and determine whose voices are heard. 70
Furthermore, the included literature was not confirmable in the study with demographic data across the entire research. Most studies lacked demographics such as occupation, gender, age, religion, education, and socioeconomic status. We expect the knowledge of dementia to vary with demographics, and nonconformity may be rare. Although, some studies (eg, Nwakasi et al, 10 Jacobs et al, 13 Mukadam et al, 18 Armstrong et al, 51 Kehoua et al, 63 Kakongi et al, 64 Mahomed and Pretorius,65,66) provided some vital demographic data. However, it was difficult to draw a separate conclusion for Black African populations in the study. Of course, in the UK, one would expect dementia knowledge among Black African populations to vary depending on educational level, occupation, age, gender, and immigration status.
In addition, 5 UK studies (n = 5) were conducted more than 10 years ago,18,57 -60 suggesting that the data is undependable and may lack credibility for the current Black African populations in the UK because dementia knowledge may have evolved. 17 This suggests an essential need for further research on the topic. It appears as if dementia knowledge is embedded in the respondents’ culture, and the Black Africans in the UK may have languages, narratives or metaphors for dementia that need further exploration.
Finally, the total number of respondents (n = 222) in all the UK studies added together was 222, with only 38 participants (n = 38) fluidly defined as Africans, constituting just about 17% of the total respondents in the UK study. However, all the African studies were of African background, comprising 465 Black African participants (n = 465) for the qualitative data. Therefore, 17% is a meager percentage, so this study considers the UK data not robust and lacks credibility for Black African populations. Thus, the UK studies’ findings are undependable and do not wholly inform us about the Black African population’s lay knowledge and beliefs toward dementia. Indeed, the UK literature lacks confirmability and authenticity for the Black African communities in the UK (Figure 1).

PRISMA diagram of the selection of studies.
Thematic Analysis
Data analysis was guided by Braun and Clarke’s 39 recommendations on synthesizing qualitative research using thematic analysis. The researcher used the reflexive thematic analysis,39 -41,71,72 informed by a grounded theory approach.73,74 The analysis is conducted to answer the review question thematically. The procedure was drawn upon in the thematic coding and analysis of the included studies and in identifying the themes and patterns or meanings across the data.41,72,73 The researcher analyzed vital empirical data that was accessible in the included papers. The analysis was driven by the participants’ own words rather than the researcher’s interpretation of the data. 41 Hence, the researcher included direct quotations from the UK and African studies in his analysis and coded the extracted data line by line and between as necessary to answer the review question. Braun and Clarke’s thematic analysis method is an iterative and reflexive process consisting of 6 steps: (i) Familiarization, (ii) Coding, (iii) Generating themes, (iv) Reviewing themes, (v) Defining themes, (vi) Writing up.
The method was further enhanced by a similar process of identifying theories through analyzing the data,74,75 which involved familiarizing with the data, focus coding, theoretical coding, categorizing, and thematic coding through inductive reasoning. 74 Indeed, as the researcher coded the included studies’ empirical data, embedded concepts became apparent and emerged from the data. Then, the researcher deductively assigned theories to the data. 76
This grounded approach provided a means of constructing methods77,78 to better understand how dementia is constituted and constructed by Black Africans in the included studies. The process enabled the researcher to understand the socially shared constructions that underline the individual’s or group’s behavior and the dementia reality of the participants across the papers. The researcher coded the participants’ words as evidence using colors and managed the data using Excel.
Step-by-Step Guide to the Thematic Analysis Informed by Grounded Theory Approach
Through an iterative and reflexive process of comparing the empirical data from the studies39 -41,71,72 informed by the grounded theory approach,74,75 the researcher produced codes inductively, identified and refined the themes based on the empirical evidence as demonstrated in the steps:
Step A: Open Coding
The researcher reviewed all the included studies to identify emerging codes, patterns, and themes. The process involved “familiarisation” and “constant comparative” analytical processes, which allowed the reviewer to move back and forth constantly across the studies and ensure that the complexity of the data was represented in the analysis. The step was fast and loose.
Step B: Theoretical Coding
The researcher then developed codes that went beyond the explicit content of the data by comparing findings across the studies. The latent codes invoke a conceptual/theoretical framework identifying the assumptions underpinning the data.
Step C: Focus Coding
This step allowed the reviewer to perform a second coding round, providing an interpretative lens to the participants’ own words or excerpts. The process involved finding patterns, renaming the codes, continuously comparing data, and refining and getting codes closer to forming a category or a new theme.
Step D: Category Coding
The researcher turned the focus code into a category/theme by charting and grouping similar codes.
Step E: Thematic Coding
This is the step in which the reviewer defines the themes and patterns across the dataset (unifying/mapping codes) and ensures that the excerpts point to the same underlying idea or meaning, with the intent of a continuous analysis within the structure.
Step F: Managing the Data and Writing the Report
Excel was used to manage the data and facilitated the data analysis, as illuminated in the audit trail:
1.
The empirical data presented in the literature is a subsample of the whole dataset used in the included articles (see Table 7).
Thematic Analysis (Codes and Themes).

Codes and Themes
Strengths and Limitations
The study provided a greater description of methods and higher-order interpretation of the dementia phenomenon, illuminating a lay conceptual understanding of dementia among Black African populations. The reviewer used the evidence synthesis methods to transcend the individual studies’ findings developed by the authors of the primary qualitative studies to create higher-order themes. However, the methods were subject to selection biases, and the findings underrepresented the Black African populations as the reviewer developed analytical rather than individual descriptive analyses of the culture. Synthesizing qualitative data across studies from diverse African cultural contexts can be challenging as culture is a complex whole rather than just an analytical simplification.
Results
A: The Main Study Findings
B: Themes (Findings From the Current Review)
The reviewer developed higher-order themes. Four themes emerged from the current research constituting dementia.
Summary of Each Main Study’s Findings.

Themes (Higher-Order Themes).
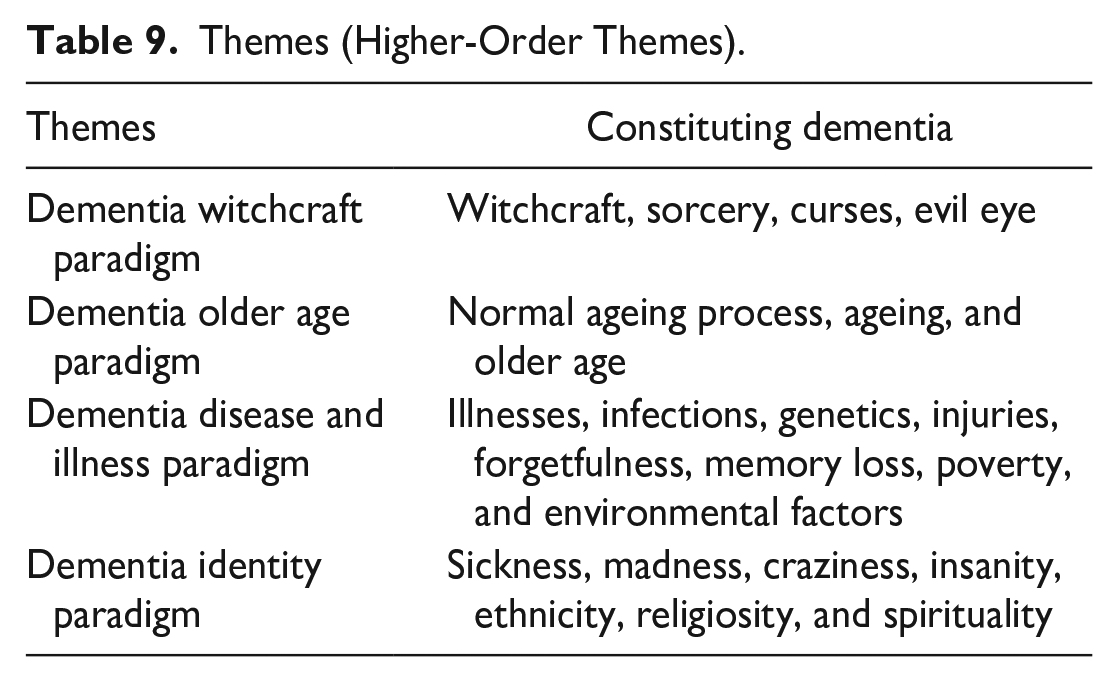
Dementia Witchcraft Paradigm
The findings highlighted the dementia witchcraft paradigm theme, which illuminated how dementia was constituted as sorcery, curses, and evil eye but broadly as witchcraft among the Black African populations, as demonstrated in the excerpts. For example,
You know in the village; they will think that somebody is bewitching [or casting evil spell on] that person [with dementia] . . .
10
(p. 1452)
Indeed, dementia perceived as witchcraft was also linked to spirituality and religiosity:
I have already heard of dementia . . . but there are demons in all dementia: Matthew 17 verse 21: This type of demon comes out only through prayer and fasting.
63
(p. 170) They use to give sacrifice to the ancestors so due to her age she cannot afford to give sacrifice to them so they get annoyed and cause all these problems.
11
(p. 133)
Dementia Older Age Paradigm
The findings illuminated the dementia older age paradigm theme, which highlights how dementia was constituted as a normal ageing process, ageing, and older age as showcased in the excepts. For example,
Where I come from there’s no definition of dementia, an old person is starting to forget, it’s part of growing old.
16
(p. 5) I know age is one [cause] of dementia, and I believe we all know that the older we become, the more our mind becomes stale.
62
(p. 271)
Dementia Disease and Illness Paradigm
The results also illuminated the dementia disease and illness theme, widely drawn as infections, genetics, injuries, forgetfulness, memory loss, poverty, and environmental conditions, as can be seen in the showcased excerpts. For example,
People with dementia were HIV-positive and epileptic . . .
63
(p. 171) The majority get the disease of forgetfulness . . .
9
(p. 6)
Moreover, the findings illuminated dementia as an organic pathology:
Dying of brain cells’
17
(p. 737)
Dementia was also narrated as an illness:
Then, when I was allowed, I was told, “he is ill” . . .
51
(p. 9)
Dementia Identity Paradigm
Finally, the findings highlighted the dementia identity paradigm theme, illuminating that dementia was constituted through a process of differences defined in social relationships and behavior, such as sickness, madness, craziness, insanity, ethnicity, disability, religiosity, and spirituality, as showcased in the excerpts. For example,
Had it not been that he is old we will say he is mad
12
(p. 909) . . . she is having such sickness
10
(p. 1453)
Ethnicity/race resonated strongly in the studies:
When you talk about dementia . . . this is a White, old White people’s disease, it’s not seen as Black people have dementia
16
(p. 7)
Comparison of the Findings in Africa and the UK
The evidence synthesis shows that the findings from the UK and Africa differ and are similar. The UK findings lack authenticity for Black Africans and, therefore, are invalid for Black African populations compared to the findings of the studies in Africa. However, the lay knowledge of dementia as older age and ageing, as well as dementia as a disease and illness, were reciprocally translated in both the UK and studies in Africa with similar logic and meanings that explained the dementia phenomenon among the Black African populations, and intersected with biomedical knowledge and understanding about dementia.
However, there were inconsistencies in the dementia witchcraft paradigm as the findings in Africa refute the UK studies due to the modeling of Black African and Caribbean people in the UK studies, and the research provided no separate findings for the Black African populations in the UK. Black Africans and the Caribbean people are distinct from each other, suggesting a need for further empirical study in the UK. Nonetheless, the dementia identity paradigm theme is an emerging concept in both studies, related to social relationships that lead to dementia stigma in both Africa and the UK. The dementia identity paradigm provides a line of argument synthesis, considering dementia a social identity and a new interpretation of the dementia phenomenon among Black Africans.
Consequentially, dementia perceived as witchcraft influenced help-seeking for dementia in Africa, and in any case, dementia perceived as witchcraft in the UK by Black Africans would equally impact help-seeking for dementia. It is more likely that Black Africans will resort to seeking help for dementia in churches rather than dementia specialist services, and this can lead to stigma and abuse. So, the reviewer argues for tailored educational and training programs aimed at reducing the stigma associated with dementia and improving outreach efforts to better support the Black African communities in dealing with dementia-related issues and preventing the abuse of people with dementia.
Discussion
Dementia is a public health burden in the UK. 20 The high prevalence of dementia among Black Africans, coupled with their lower engagement with dementia specialist services in the UK,16,17 is a public health concern. The findings in this study showcased how dementia was constituted and constructed among the Black African populations. Generally, lay people’s knowledge and beliefs about dementia are not limited to biomedical constructs. People can draw on their own meaning and interpretation of their experiences of dementia in everyday life.29,30 Different populations can draw on dementia as defined by representations79 -81 and can also be based on their own beliefs and culture. 5 The evidence synthesis shows that the lay knowledge and beliefs about dementia among Black African populations were foregrounded in sociocultural distinctiveness, constituting mainly as witchcraft (eg, studies7,9,10), older age (eg, studies11,12), disease and illness (eg, studies16,17,63), and with social identity based on relationships (eg, studies12,13).
Belief in witches’ crafts is widespread in Africa. 6 They are part of a complex body of inherited folklore, 4 and dementia identity is constituted through differences in social identity based on relationships with others in the Black African community. 82 In addition, dementia identity theory is situated with the mind/brain and body constructions. 83 Hence, the identity theory of the mind/brain and body holds that the processes of the mind are identical to the state of the brain and the physical body.83 -85 So, dementia was associated with “madness” and “craziness” in Black African communities. 12
Being mad/crazy or witches’ crafts can be viewed as a more comprehensive cultural socialization and unique dementia constructions/constructs or identifiers, 86 passed across the Black African community members and shaped their dementia help-seeking attitudes and behavior in the UK 19 and across Sub-Saharan Africa. 63 Most studies reported pluralistic behaviors (eg, study 13 ) in seeking help due to labeling and stigma.87,88
All the studies in Africa with Black African populations associated dementia with witchcraft. However, the association with witchcraft is inconsistent with the wider UK literature on Black African populations in the UK as reviewed. The studies on BAME in the UK suggested that Black Africans in the UK lacked knowledge of dementia. 16 It further suggested that Black African populations in the UK rely on community, friends, and families for dementia support and advice. Black African populations are underrepresented in UK dementia specialist services and use churches for dementia support. 17 Indeed, religion and spirituality are integral parts of Black African culture, and it is more likely for Black African populations in the UK to fall back on those services with which they are more familiar. 19
Nevertheless, the suggestion that Black Africans in the UK lacked dementia knowledge 16 is unreliable as the studies had no separate data for the Black African population. Thus, the conclusion drawn from the study is not credible, invalid, and lacks authenticity for the Black African community in the UK. However, we expect dementia knowledge among the Black African populations in the UK to vary based on demographics such as educational level, occupation, age, gender, and immigration status. Most importantly, dementia knowledge may have evolved in the Black African community in the UK.
Therefore, to address these gaps, this study recommends further empirical research to explore the lay knowledge toward dementia among Black African populations in the UK. The study must focus on methodological adaptations in order to continually make the research culturally sensitive. 89 Incorporating the views, experiences, perspectives, and practices of the Black African populations in the UK in all stages of the research process is essential because studies that ignore or do not account for the cultural perspectives of participants are invalid. 89 Indeed, future studies must be informed by a grounded theory approach. More importantly, longitudinal studies among Black African populations are needed to track changes in dementia perceptions over time.
Conclusion
The evidence synthesis shows that dementia is culturally embedded among the Black African populations and associated with stigma and abuse. However, the UK studies do not wholly inform us about the lay knowledge and beliefs about dementia among Black African populations in the UK. Previous studies in the UK lack authenticity for Black African populations and, therefore, are invalid. Moreover, most of the UK studies are outdated. There is an essential need for future studies among the Black African populations in the UK and a need for a longitudinal study to track changes in dementia perceptions in the group over time.
Recommendations
There is a need for culturally tailored educational and training programs aimed at reducing the stigma associated with dementia and improving community outreach efforts to better support Black African populations in dealing with dementia-related issues. Thus, this study recommends strong partnership or collaboration between medical doctors, community leaders, and applied medical anthropologists in dementia practice to help resolve the dementia stigma and prevent the abuse of people with dementia in Black African communities.
Implications for Policy and Practice
The study has broad implications for dementia policy and practice. A better understanding of the lay knowledge and beliefs about dementia held by Black Africans can improve dementia help-seeking and care, help prevent the stigma and abuse associated with certain beliefs about dementia, and provide culturally sensitive and tailored support for Black African communities. This study contributes to the evidence base for dementia practice in the Black African communities in the UK and Africa.
Footnotes
Acknowledgements
The author would like to acknowledge the support of Dr Wendy Martin, Professor Holly Nelson-Becker, and Professor Meriel Norris for their exceptional guidance and encouragement throughout this study. The author would also like to thank Professor Claire Donovan, Professor Christina Victor, Professor Nana Anokye, and Professor Subhash Pokhrel for their additional guidance in this study.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
No ethical approval was required for this research.