
Abstract
Increased emphasis on the child’s voice and point of view in care and treatment has led to an expansion in the development of methods to access and identify their perspectives. Drawing on our experiences in a study of children with leukemia in hospital, this article explains the challenges and opportunities that arise in the use of five commonly used methods in a study of hospitalized children’s experiences with health care professionals, including the “Draw and Write” technique, a sticker activity, a paper–person exercise, informal interviews, and participant observation. Each of these methods was examined with regard to ease of use, data generation, and utility of data for accessing children’s perspectives and development of initial clinical guidance.
Introduction
There is now a growing body of research, which recognizes that to better understand children, their experience trajectories and sociocultural engagements, they must be placed as competent participants at the center of the research process (Dell Clark, 2011). For this to happen, researchers need to facilitate children’s communication and participation in data collection (Harden, Scott, Backett-Milburn, & Jackson, 2000; Thomas & O’Kane, 1998). Recent literature highlights the need for researchers in health care to distinguish between having a child’s perspective and taking the child’s perspective (Coyne & Harder, 2011; Nilsson et al., 2015). The child’s perspective requires the researcher to capture the child’s own viewpoints and experiences, based on what the child regards as important. Subsequently “task-centered” participatory activities, such as drawing or diary writing, which build on children’s existing skills and interests, have been suggested as better approaches for capturing the child’s voice, rather than more traditional “talk-centered” methodologies (James, Jenks, & Prout, 1998). For example, a “toolbox,” encompassing examples of customizable interview techniques are known to be essential in finding ways beyond talk to seek children’s views (Lees et al., 2017; Lys, Gesink, Strike, & Larkin, 2018; Teachman & Gibson, 2013).Yet published work discussing the impact of using different participatory methods in health services research with children is lacking (Haijes & van Thiel, 2016).
Here, we take an opportunity to discuss the value and challenges using five qualitative data collection methods in a busy clinical context with children newly diagnosed with leukemia and evidence this discussion through a systematic evaluation of the data produced using each method. Particular attention is given to the relative contribution each method made to (a) elicit the child’s perspective in their interactions with clinicians and (b) the development of future clinical guidance concerning health care professional (HCP)–child interactions. Our remarks and reflections are based on data collected as part of the “Talking With Children Study.” The primary aim of this study was to gain an in-depth understanding of what children newly diagnosed with cancer knew about their disease and treatment, how they came to know, and what they wanted to know, as a first step in developing guidance for professionals for talking with children in the early phases of cancer treatment.
Method
Design
An ethnographic approach, comprising participant observation and informal interviews alongside participatory methods, was used by a researcher embedded in a clinical team. This researcher (G.B.) had extensive previous experience of working with children, had no prior affiliation with either the inpatient or outpatient units, and was not known to patients or their families prior to the study commencing. When meeting children eligible for recruitment into the study, the researcher was careful to tell children that she was not a nurse or a doctor and that she was a researcher who wanted to know “what they think about and talk about.” During data collection the researcher was mindful to distinguish herself from other hospital staff in her attire by dressing in casual clothes.
Setting
This study took place within the hematology and oncology service of a large tertiary children’s hospital in England.
Participants’ Consent and Assent
A purposive sample was selected to include children, boys and girls, across the range of childhood cancer diagnoses, and aged 4 years to 12 years old. Children were excluded if they were outside of these age ranges at the time of data collection, or if they were identified by clinical staff as too unwell to be asked to participate in a research study. In total, 13 families were approached and seven children, three girls and four boys, were recruited into the study. Reasons for refusal to participate were as follows: parent’s refusal to speak to the researcher, parents felt that it was not a good time, child refusal to assent to participate, and lack of available interpreters. In addition, one child was found to be ineligible for participation after being initially approached by the researcher as he or she did not meet the inclusion criteria. Two children had acute myeloid leukemia, whereas the remaining five had acute lymphatic leukemia. A child-centered approach was used to negotiating informed assent and consent (Dell Clark, 2011). This approach respected each child’s capacity to be involved in informed decision making while simultaneously recognizing the parents’ responsibility as protective gatekeepers (Lambert, Glacken, & McCarron, 2011): the detail of this process of obtaining child assent and written parental consent has been described in detail elsewhere (Vindrola-Padros, Bryan, Coyne, Martins, & Gibson, 2016).
Ethical Approval
This study was granted National Research Ethics Service (NRES) Committee (Reference: 10/H0801/56) and local approvals prior to the researcher entering the field. All names presented are pseudonyms.
Data Collection
Between May 2011 and May 2012, an embedded researcher (G.B.) was established in the clinical team to capture the events and conversations that took place in real time between children and their parents, children and HCPs, and between HCPs. The researcher spent approximately 3 days per week following families as they navigated the hospital and observing interactions between children, parents, and professionals; as well as among the professionals when the case study families were discussed on both the inpatient and outpatient wards. Participant observation and informal interviewing were used in accessing children’s visions of their worlds and their everyday interactions in the hospital setting.
The researcher purposely visited the units at different times of the day: early mornings, late evenings, and weekends, to ensure that a comprehensive picture of children’s everyday activities were captured (Lambert, Glacken, & McCarron, 2011). The researcher was present in as many clinical locations as possible where care and treatment took place, including multidisciplinary team (MDT) meetings, clinical ward rounds, during consultations, while children were waiting for procedures and during the administration of therapy. The researcher also spent time at the nurses’ stations, in the corridors, and in playrooms to capture the more informal spaces in which HCPs and children interacted. At various time points during data collection, informal unscripted interviews were conducted with or without props including toys to elicit the child’s perspective on their experiences and interactions. Informal interviews were also conducted with parents and HCPs.
Extensive field notes were maintained following a modified data collection framework proposed by Spradley (1980). Where possible, interactions were audio recorded and transcribed verbatim. The researcher asked the child’s permission to audio record at the beginning of each interaction. One child was initially resistant to the use of the audio recorder but allowed the researcher to audio record their last interaction. Between five and 26 observations were carried out with each family recruited into the study over the period of data collection (a total of 87 interactions). As indicated by Nightingale, Sinha, and Swallow (2014) data collection was organized within the confines of what was achievable with one researcher within the 12-month time period of the “Talking With Children Study.”
In addition to participant observation and informal interviews, three child-centered methods were used to capture children’s knowledge about their disease and treatment and their interactions with professionals: (a) the “Draw and Write” technique (Aldiss, Horstman, O’Leary, Richardson, & Gibson, 2008; Gonzalez-Rivera & Bauermeister, 2007; Horstman, Aldiss, Richardson, & Gibson, 2008), (b) a sticker activity (Lambert, Glacken, & McCarron, 2008), and (c) a paper–person (a method developed by the field researcher; G.B.).
Each of these three methods was selected with an eye to the context of the research setting. The sequence of methods employed was not prescriptive, rather they contributed to a “toolbox” of resources and child-centered activities brought to the ward by the researcher each day. Each technique was flexible, allowing the researcher to make adjustments as necessary to the activity depending on the child’s age or physical condition. Children were presented with a variety of options during each interaction and asked to select the activity. If the child chose to complete an activity they did so only once.
The “Draw and Write” technique was chosen as a method for accessing children’s experiences, and their associated thoughts and feelings in a nonthreatening and open-ended manner (Horstman et al., 2008; Knighting, Rowa-Dewar, Malcolm, Kearney, & Gibson, 2011). Children were given a single sheet of A4 paper and felt tip pens. It was left up to the child whether to use the paper in portrait or landscape (Horstman et al., 2008). The researcher used the drawing prompt: “Draw a picture of someone like you who is in hospital and what they are thinking and what they are feeling.” The phrasing of the prompt was not directing children in what to draw but rather aimed to help frame his or her thoughts toward providing information about a specific topic (Horstman et al., 2008). Children were reassured that the task was not a test, and that there was no “correct” response (Horstman et al., 2008; Knighting et al., 2011). If they were able, children were encouraged to write on their drawing, to add emphasis. For children who were too young or too unwell to write, the researcher acted as a scribe. The child’s drawing was then used as the focus of a short semistructured interview about their picture (Horstman et al., 2008). During this interview, the researcher first focused on any items in the picture that needed elucidating, before exploring with the child what they had drawn to gain the child’s explanations of the meaning (Driessnack, 2006).
To provide some structured guidance and focus to conversations about professionals and the amount of information doctors and nurses gave to children, a sticker-based activity was employed (Lambert et al., 2008). The sticker chart was modified from Lambert et al.’s (2008) “stick a star quiz,” by adding four questions about doctors and nurses allowing time for children to ask questions and answering children’s questions. Children were asked 14 open-ended questions about their experiences of communicating with doctors and nurses (for example, “How much information do the nurses give you?,” “How much time do nurses spend answering your questions?”), and asked to respond by placing a sticker in either the “never,” “a little” “sometimes,” or “a lot” boxes on the chart. Children were asked short clarifying questions by the researcher about their response prior to the next question.
The paper–person activity was developed by the researcher as a “prop” for the children to use while reflecting on their past treatment and was employed only with the children approaching the end of treatment. Children were given a large paper cut out in the shape of a person and a box of pens and given the prompt: “Think about everything that has happened to you since you were diagnosed and what treatment and procedures have been done to you and draw them on the person.” The task usually started with the child drawing the person’s face and giving the person a name. The researcher used prompts (such as: “what kind of line did you have?”) if the child appeared to be having trouble with recall. This task was completed in conjunction with verbal interviewing, which helped to sustain the child’s involvement (Dell Clark, 2011).
In addition to these activities, the researcher interacted with the children recruited into the study and their families while playing games, doing arts and crafts, and watching television (Bluebond-Langner, 1980). These informal interactions provided a context for observing interactions between children and professionals and later for exploring the meaning of such interactions with the children and their parents (Lambert et al., 2008).
Data Analysis
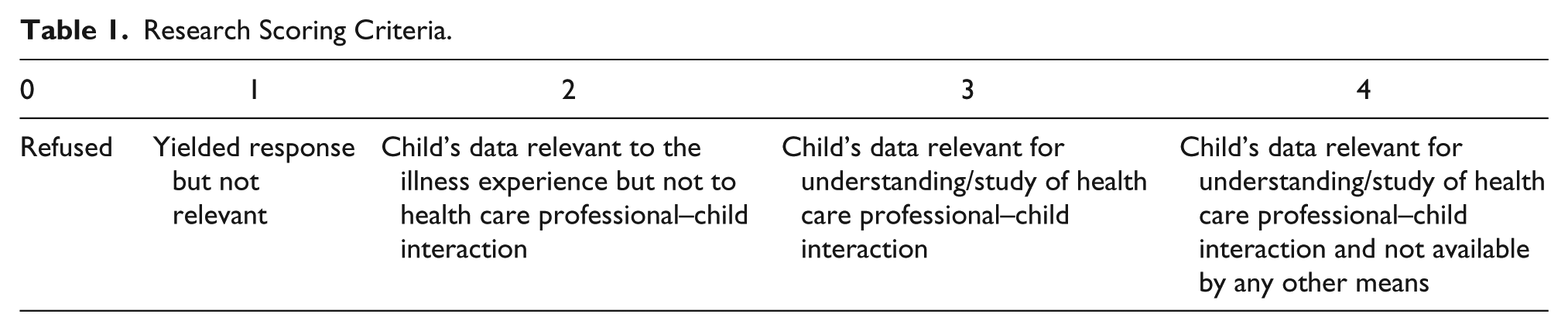
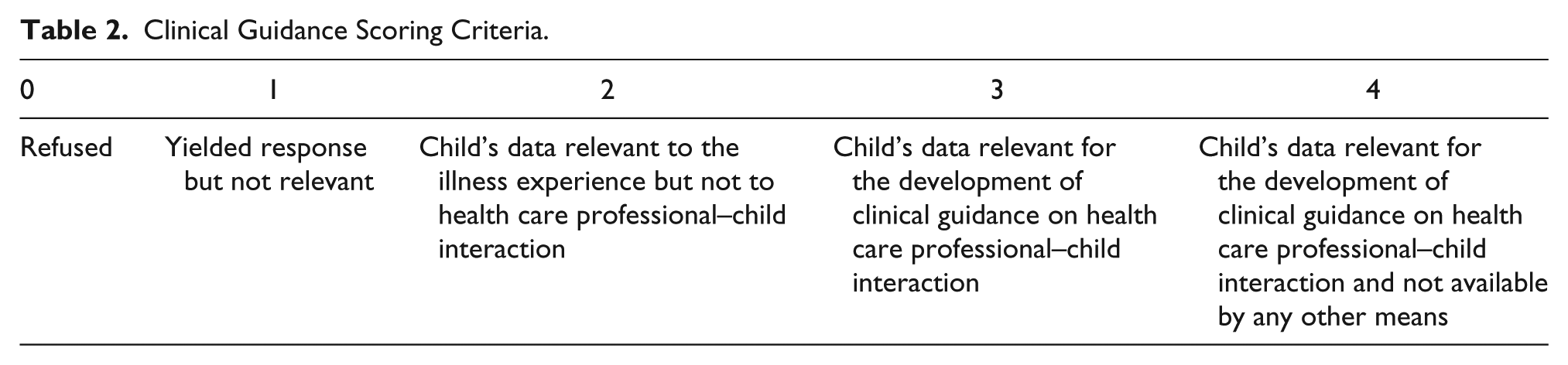
To explore the merits and the relative contribution of each method used to inform our understanding of HCP–child interaction with a view toward the development of clinical guidance for talking with children, data from the HCP–child communication domain from the “Talking With Children Study” were reviewed per child per data collection method. The further exploratory questions used to clarify children’s responses were presented separately from the “Draw and Write” and sticker activities to draw out the value of these specific components. Two numerical scoring systems were developed by M.B.L. and further revised by G.B. Three authors, M.B.L., G.B, and F.G., scored all data generated from each of the methods used in the study. Data were scored (a) for utility of understanding of HCP–child interaction (Table 1) and (b) in relevance for developing clinical guidance for HCP–child interaction (Table 2). Both scoring systems used a 0–4 scale, with the lowest score indicating the child refused the activity, and the highest score indicating the production of data that was relevant to the project goals and available by that method only for that child. For example, child’s utterances, which were not related to either the understanding of HCP–child interaction or the development of clinical guidance received a score of 1; a score of 2 was given to data that while relevant to understanding the child’s illness experience did not include their relations or interaction with HCPs; a score of 3 was given to child’s data that were relevant for either the study/understanding of HCP–child interaction or for the development of clinical guidelines into HCP–child interaction; while a score of 4 was given to data relevant for the study of/understanding of HCP–child interaction or the development of clinical guidance on HCP–child interaction and not available by any other means.
Research Scoring Criteria.
Clinical Guidance Scoring Criteria.
To be considered relevant for a score of 3 or above for the utility of understanding HCP–child interaction criteria, data had to concern children or HCP’s communication practices or preferences. Some of the data with this score detailed, for example, why children chose to ask questions of certain health professionals, and not others; children’s reasons for providing information to only certain members of staff; and children’s explanations for choosing to talk or not talk during interactions.
To be considered relevant for a score of 3 or above for relevance in developing clinical guidance for HCP–child interaction, data had to be applicable to the development of guidelines on HCP–child interaction. This included data that, for example, detailed children’s communication preferences on how involved they would like to be in conversations about their disease and therapy; and showed examples of good or poor communication practices, such as HCP use of inappropriate analogies or HCPs supporting children in participation in dressing changes.
Scores were then compared and a very small number of disagreements were resolved through dialogue. The results for each method are presented by child in Table 3. Results are discussed by the method used.
Methods Used with Each Child and Score for Health Care Professional-Child Interaction and Relevance for the Development of Clinical Guidance on Health Care Professional-Child Interaction
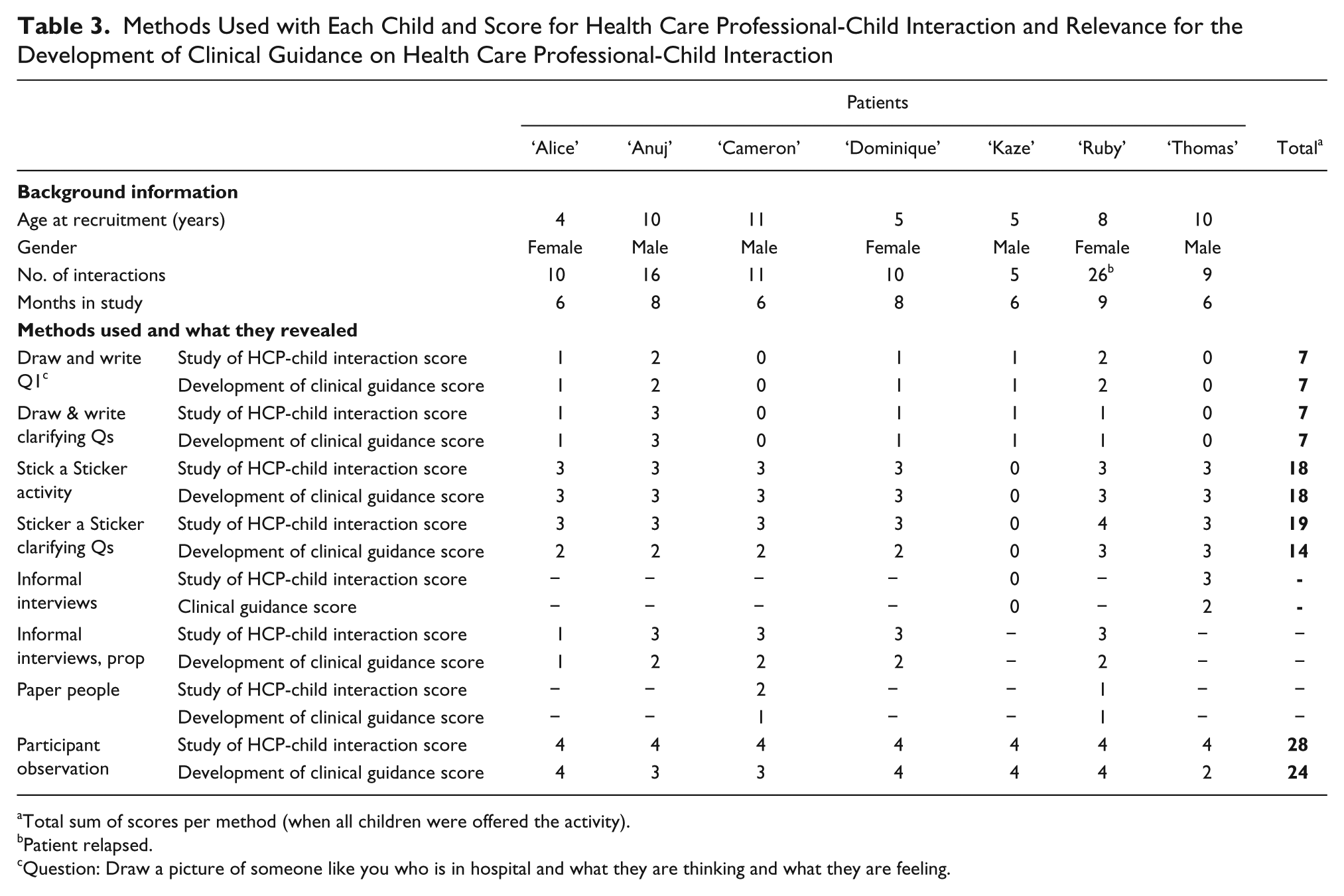
Total sum of scores per method (when all children were offered the activity).
Patient relapsed.
Question: Draw a picture of someone like you who is in hospital and what they are thinking and what they are feeling.
Results
“Draw and Write”
Of the seven children in the study, five completed this activity. Two children, both older boys aged 10 years and 11 years, respectively, refused: “Thomas” said that he was “rubbish at drawing” and would rather just read his book, whereas no reason was recorded for “Cameron’s” refusal. Of the five drawings produced at the children’s bedsides, two were completed while the child was an inpatient and were being nursed in their own room. The other three were completed on the outpatient day unit, two of these while the child was allocated a bed in a bay with other families present, and one in a private side bay. It is possible that the presence of family members or other patients may have affected the child’s choice of drawing. Although observing her daughter talk through her drawing with the researcher, “Alice’s” mother commented that “Alice” had drawn “a very optimistic view” of being in hospital, and instead of the drawing she had produced of her playing, she thought that “Alice” would have drawn herself attached to her drip stand. At her next appointment, “Alice” presented the researcher with a drawing done at home, in which a figure was depicted exactly as her mother described. This drawing was kept by the researcher, with “Alice’s” permission, but excluded from the analysis.
Three children produced drawings that, while interesting contributions to our understanding of children’s presentation of their experiences, were not immediately relevant to our understanding of HCP–child interaction (hence a score of 1 for relevance for study of HCP–child interaction and for the development of clinical guidance). “Kaze” first wrote his name and then drew himself, his family, and the toys he played with, whereas “Alice” drew herself playing with another female patient. “Dominique” was adamant that she did not want to draw a picture of someone who was “in hospital” and instead drew someone walking in the countryside. Although “Dominique’s” drawing could be argued to possibly show the way she coped with her treatment, it was judged not to be relevant for understanding HCP–child interaction.
The drawings produced by the other two children were judged to be “relevant to the illness experience but not to the research question” (a score of 2) for both research and clinical guidance purposes. Both children drew pictures of figures lying in bed. One child “Ruby” annotated her drawing with a thought bubble, which stated: “I feel a bit sick, I should go to the playroom and take my mind off.” The “Draw and Write” activity alone generated no data deemed relevant for study of HCP–child interaction or for the development of clinical guidance (required for a score of 3 or above).
After completing their drawings, as per the method, children were asked to talk about their picture with the researcher, who gently asked additional clarifying questions where required. One of the children, “Anuj” who drew a figure lying supine on a bed explained that the stick figure standing over him was a doctor who was saying “you’re going to get better, don’t worry.” This was given a score of 3 and considered relevant for both study of HCP–child interaction and the development of clinical guidance. The responses of the other four children were judged to have only “yielded a response but not relevant” for both domains (a score of 1). No data generated using the “Draw and Write” technique was scored as being solely available using this method across the seven participants (a score of 4).
Sticker Activity
The sticker activity was offered to all participants. One child, “Kaze” refused, choosing instead to play. The other children did the task at the bedside. Five of the children completed the task on the outpatient day unit, three of these while in bays with other families present, and one child completed the task on the ward in her own room. Of the six children who started the task, one child, “Anuj,” did not complete it as he was called for treatment. Notably, the task was interrupted by clinical activities in another three children, only two of whom chose to resume the activity postinterruption.
This activity was time-consuming, particularly with the younger children (those aged 4 years and 5 years). Children took a long time to navigate all 14 questions and some put the stickers in the wrong box after making their decision, resulting in the researcher having to verify and then revise these responses. The repetitiveness of the question format, which asked seven questions about the doctors and then the same seven questions about the nursing staff was observed to be tedious for some of the younger children. It was initially planned that children would be asked to place different numbers of stickers in the boxes depending on their response; however, this was quickly abandoned with these children, as it proved too time-consuming in a busy clinical environment. The activity terminology also had to be clarified for some of the younger children. For example, “Alice” did not understand the word information and so an explanation was provided.
One child, “Ruby” aged 9 years, who took part in the study almost entirely as an inpatient, furtively looked about while completing the questions about the nurses. She was obviously uncomfortable despite the activity taking place in her room with the door closed and only the researcher present. Ruby apologized aloud to the nurses even though none were there when she placed a sticker indicating that the nurses “never” spent time answering her questions. She told the researcher “Don’t ask me questions about why. Please don’t ask me the question about why.” “Ruby” also chose to distinguish between members of the nursing staff, telling the researcher about her favorite nurse separately from the rest of the nursing staff when answering the question about how much the nurses allowed her to speak and have her say. “Thomas” adapted the activity to better suit his responses, placing stickers on the line between the “some” and “a lot” box for four of the questions. This activity was scored as relevant for both study of HCP–child interaction and the development of clinical guidance for all children (a score of 3). However, none of the data generated by the participants was considered to be only available using this method across any participants (a score of 4).
After completing each question on the sticker activity, the researcher asked further exploratory questions to clarify the child’s responses. This questioning was curtailed for one child, “Dominique,” who was notably distracted by the television during the later parts of the task but when asked by the researcher if she wanted to stop, told the researcher to continue. Mindful of the child–researcher power balance, the researcher continued with the task, but stopped asking the clarifying questions. The data generated from clarifying questions (before discontinuing), were given a score of 4 for study of HCP–child interaction for “Ruby,” as this activity was the only method that revealed that “Ruby” did not like the doctor’s use of the term “blood cancer” when interacting with her as it gave her a “funny feeling” to hear her disease described as such.
The majority of the sticker activities took place in the presence of the child’s parents. When “Alice” completed the sticker activity, her mother and older sister both interjected during both the task and the clarifying questions to give their views on “Alice’s” level of interaction with staff. “Alice’s” mother subsequently took over responding to the clarifying questions on behalf of her daughter, resulting in the child’s perspective in this activity being relatively limited. However, as Alice spoke about her interactions with medical professionals during this activity, these data were given a score of 3 for HCP–child interaction. The data from the other children who completed this task was considered relevant for the study of HCP–child interaction (a score of 3). Data from two children were given a score of 3, whereas the remaining four children provided no information scored as relevant for the development of clinical guidance (Table 3).
Paper–Person Activity
Two children choose to complete the “paper person” task. Both activities took place in the outpatient day unit at the end of treatment while waiting for the child to have their central line removed. In the case of “Ruby,” the activity took place in a six-bed bay with two other families present. One young patient, who was not part of the study, continually interrupted the task to ask what “Ruby” and the researcher were doing, and to tell them that they were not allowed to use the tray table to draw. When the researcher offered the child his own person to complete, the offer was rejected by the child’s father who subsequently told him to stop interrupting the activity. This activity engaged both participants. Although “Cameron” completed the activity, his younger brother was told off by his parents for trying to involve himself in the task. The researcher was able to satisfy everybody by offering the sibling his own pens and “paper person.”
Although the task produced useful data about the children’s illness experience, none of it was considered relevant for either the study of HCP–child interaction or the development of clinical guidance.
Informal Interviews
Informal interviews took place with six of the seven children as one child refused to answer questions about his disease or treatment, instead telling the researcher that he had come to the hospital to “play and build puzzles.” The other six children all took part in at least one informal interview. Interviews with two older boys took place while playing with Lego®. These interviews took place while the children were inpatients in their own rooms. Interviews with “Alice” and “Dominique” were conducted using a toy, a rabbit and a sock monkey respectively, as a “prop” and took place in the outpatient bays. Using the monkey in this manner proved to be very successful with “Dominique,” who had previously been resistant to discussing treatment and who had denied being sick in earlier conversations with the researcher. However, when introduced to the toy and asked to explain to the monkey why she had come to the hospital, Dominique grabbed it, squeezed it tightly, and then proceeded to discuss an extensive list of disease and treatment-related topics, including her views on the nursing staff. Informal interviews were given a score of 3 for study of HCP–child interaction for “Dominique” and four other children. The interview with “Alice” was determined to have elicited a response but this was not relevant for study of HCP–child interaction. Informal interviews were found to produce no data scored as relevant for the development of clinical guidance on HCP–child interaction.
Participant Observation
Participant observation was the only method with universal engagement from the children and as such provided the majority of the data for the HCP–child communication domain of the “Talking With Children Study.” This method generated some of the most illustrative examples for both study of HCP–child interaction and for the development of clinical guidance. Data collection using participant observation in a busy clinical environment proved feasible albeit challenging. Staff were initially wary of being observed, particularly, when the interaction was audio recorded, although such reservations appeared to diminish over time as they grew accustomed to the researcher’s presence.
Most children quickly grew comfortable with the researcher’s presence, scolding her when she had not seen them in a while, or when they knew she had spent longer that day with other children on the unit. However, the researcher found she had some difficultly developing a rapport with two of the older boys in the study, who were both 10 years old. “Anuj” and his family were quiet, extremely reserved, and spoke English as a second language. Although the family continually verbally consented to the researcher’s presence, the researcher did not feel comfortable just turning up and “hanging-out” with this family in the way she did with other families in the study. This became particularly apparent when “Anuj” became very unwell and appeared to retreat under his blankets and withdraw from the world during treatment. “Thomas,” a 10 year old boy, was often monosyllabic and did not make eye contact while talking, which made conversation difficult. As both children provided written assent at the beginning of the study and continual verbal assent during the study, the researcher was confident that these issues were not subtle signs of refusal to take part in the study, rather issues with building rapport with research participants.
Data generated using this method were scored as “relevant for study of HCP-child interaction and unavailable by any other means” (a score of 4) for all seven children. “Kaze” was observed as being happy and chatty prior to a consultation and subsequently curled into a ball and became mute when his medical consultant appeared at his bedside leading the consultant to ask him: “why is your head stuck to your knee?” As the consultant conversed with “Kaze’s” parents, “Kaze” gradually resumed his previous activity. As “Kaze” was unwilling to complete the sticker activity and was unresponsive during the researcher’s attempts to ask him questions about his experiences, this hesitation to interact with professionals may not have been identified without participant observation. Likewise, observation of “Thomas’s” interactions with professionals indicated that he was at times highly anxious while in the hospital, excusing himself to go to the bathroom multiple times prior to treatment or procedures, much to the exasperation of his father; and visibly concerned about the meaning of test results, even supposedly routine results such as blood pressure and oxygen saturations. This was not identified using any other methods employed during the study.
The data from four children were judged to be “relevant for the development of clinical guidance and unavailable/not available by any other means” (a score of 4). Data from two children were deemed to be “relevant for the development of clinical guidance” (a score of 3) and one was classified as “relevant to the illness experience but not to the research question” (a score of 2).
Participant observation highlighted professionals’ interactional strategies such as the use of rhetorical questions when examining patients and completing clinical observations. For example, on the outpatient unit, a health care assistant (HCA, unqualified nurse) was observed asking children’s permission to record their weight, height, and blood pressure as part of the admissions procedure but then was repeatedly observed inserting an in-ear thermometer into children’s ears without permission, explanation, or forewarning. In one instance, when the HCA asked a child’s permission, she had moved to insert the thermometer before the child had a chance to respond.
Secondarily, the way children were addressed during the ward round was identified through participant observation. Observing the ward round from the child’s perspective, whereby the researcher sat with the child and waited for the MDT to visit, revealed that the consultant did not actually enter the room when asking “Ruby” a question during the ward round. Observations revealed that the majority of the consultant’s body remained outside of the room, instead they put their head around the door and rested their weight on the door handle, and did not take their hand off the handle during this entire interaction. Without participant observation this nuance of practice would not have been identified.
Discussion
We have now reached the point in research, practice and policy in child health where including the voice and perspective of the child is de rigueur. However, which is the best way to capture children’s voices, to identify their perspectives, or to utilize our findings for clinical practice? In this study, we focused on HCP–child interactions, and we found that participant observation provided the richest and most robust data in comparison with other techniques for understanding relations with children undergoing treatment for cancer. This method was scored highest for both the study of HCP–child interaction and the development of clinical guidance. As Carnevale, Macdonald, Bluebond-Langner, and McKeever (2008), have discussed previously, the use of participant observation provided understanding, which could not have been obtained utilizing other methods. O’Kane (2000), however, has suggested that participatory methods can be utilized as an alternative to ethnographic methodologies, yet our data suggest that this may not be the case. In our study the data produced differed by the methods used, with some participatory methods such as the “Draw and Write” revealing comparatively less about HCP–child interaction. That said, the use of some of these participatory methods, such as the “Draw and Write,” did offer the opportunity for the researcher to build rapport with the child and family in a relatively short time frame as well as to remain in the room to observe encounters with professionals (Coad, 2007; Dell Clark, 2011). The use of a mixture of participatory and observational methods may, therefore, be advantageous in clinical environments with similar patient populations (Coyne & Carter, 2018).
The children’s hospital environment is undoubtedly a clinical space, where children reside but which is organized for “medical care.” Privacy is an issue for children in hospital (Ekra & Gjengedal, 2012; Pelander & Leino-Kilpi, 2009), not just those taking part in research, with bathrooms often being the only truly private space (Schalkers, Dedding, & Bunders, 2015). Although the researcher was mindful of not asking children to complete activities, such as the sticker activity “rating” the nurses and doctors in public spaces, such as the playroom, this was not always possible and many children ended up completing the activities in the busy outpatient area, as it was seldom possible to secure a private space for data collection. It is possible, therefore, that the clinical environment may have affected some of the children’s responses when using the participatory methods. For example, “Ruby” was made notably uncomfortable during the sticker activity when asked for her views on the nurses despite the door of her private room being closed. However, in hospital, such “private” rooms are not really private, and during the study, private spaces were frequently entered by other people: nurses administrating medicines and performing observations, doctors either by themselves or on the ward round, social workers, psychologists, play staff, staff from the hospital school, orderlies, cleaners, other patients, not to mention the child’s family and friends.
It has been suggested that flexible and informal environments are important when using participatory methods with children (Carter & Ford, 2013) and as such that researchers should allow participants to choose the space in which the interview is to be conducted (Darlington & Scott, 2002; MacDonald & Greggans, 2008; Stevens, Lord, Proctor, Nagy, & O’Riordan, 2010). The environment in which data were collected in our study was neither flexible nor informal, and children were afforded very little venue choice. The majority of the data were collected in rooms that accommodated six beds for children who were in hospital for the day receiving outpatient treatment and their families. Although these beds were equipped with curtains, these were seldom used and most interactions were visible to the entire room. Collecting data in such an environment is challenging for both the researcher and the child.
Constant interruptions for clinical tasks, while obviously necessary, disturb the flow of data collection, and can be particularly problematic with children who have a short attention span. The data generated in our study using the clarifying questions in the “Draw and Write” and sticker activity illustrates the importance of accompanying activities with discussion. However, such questions after or during an activity substantially increases the length of the activity, and in a clinical environment with young children, limited time and a high likelihood of being interrupted, this can be problematic. The frequent presence of a child’s family during data collection and their interjections should not necessarily be seen as negative; as maternal “scaffolding” can result in the child producing a more complete and richer narrative than with a child who is unprompted (Clarke-Stewart & Beck, 1999; Irwin & Johnson, 2005). Nevertheless, it can be a challenge for the researcher to ensure that the child’s “voice” is heard, and that the child is not simply narrating the parent’s story (Carter & Ford, 2013).
A “toolbox” of participatory and other activities was employed in our study. This approach also included a range of toys and non-research-based resources, which were useful when breaking the ice and establishing a rapport with the child (Carter & Ford, 2013; Woodgate & Kristjanson, 1996). This gave the children choice over the tasks. When asked what activities they wanted to do, two of the older male children refused to take part in the “Draw and Write” activity, with one child telling the researcher his refusal was due to his perceived inadequacies at drawing. The use of drawing activities in research may be advantageous as unlike interviews, which can require more immediate forms of response and may be perceived to be intrusive by some children (Carnevale et al., 2008); the “Draw and Write” technique gives children flexibility, time to think about what they want to depict, and to amend and add to their response (Punch, 2002). However, not all children like to draw (Carter & Ford, 2013; Dell Clark, 2011): Older children may be worried about their level of artistic competence and not consider drawing to be fun (Punch, 2002).
The use of the audio recorder in our study initially appeared to concern some hospital staff and proved difficult in busy clinical environments, especially with young children, people with regional accents or people who spoke quietly. Individual bedside televisions started to be placed in the outpatients bays during the course of the study, which considerably raised the background noise level in these rooms and were a potential for distraction. To overcome background noise, the researcher appointed children “disk jockey” asking them to speak directly into the audio recorder like a microphone. However, this technique was only partially successful.
Researchers need to be mindful of both the demands of the clinical setting and their population when choosing research methods and consider such diverse factors as infection control measures (Carter & Ford, 2013), age, children’s attention spans, potential for interruptions, privacy, background noise levels, and whether the activity can be completed when the child is attached to a drip stand, lying down, or with an intravenous cannula in place. In addition, the importance of relational skills, tenacity, and attention to detail on the part of the researcher while utilizing these methods in clinical environments cannot be overstated. The “toolbox” of activities utilized in this study empowered children to select which participatory activities they wanted to complete without making children feel awkward or coerced to complete any particular activity.
Limitations
The “Talking With Children Study,” which recruited seven families over 1 year of data collection, with the researcher only in the field approximately 3 days a week, is a relatively small study. However, given the nature of the data collected, utilizing participant observation with only one researcher carrying out the observations, recruitment of more families would have meant missing crucial data from those families already in the study. The frequent presence of parents during data collection means that the possibility of mutual pretense in children’s responses should not be overlooked (Bluebond-Langner, Belasco, DeMesquita, & Wander, 2010).
In addition, data collection was ward-based and did not take place away from the clinical setting. Even with good quality equipment, there were challenges associated with the noise of the clinical environment. The study took place in a single specialist setting, and families were not followed into the “shared care” local hospital, where some children can spend the majority of the early phases of treatment, or at home. However, each of the children was met by the researcher on multiple occasions during their time in the study, with between five and 26 interactions with each child. Many of these interactions encompassed the entire duration of the outpatient visit, as the researcher arrived at the beginning of the appointment and left the unit with the family, which allowed considerable time for the families to share their experiences. Our approaches allowed the collection of data from all three perspectives in HCP–child interaction: those of the child, the HCP, and the parent.
For this article, two scoring systems were applied to the data generated from the “Talking With Children Study” and used as aids to analysis when sorting and classifying data. That these scoring systems were not validated prior to use is a limitation of the narrative presented here. However, these scoring systems were applied independently by three of the authors and differences between scores although infrequent, were discussed and resolved, which introduced rigor to the process.
Conclusion
The use of participatory methods in a busy clinical environment with children undergoing treatment for leukemia is challenging, but possible, albeit not without limitations. Participant observation provided much of the data from the HCP–child communication domain from the “Talking With Children Study” and proved a particularly useful method for studying HCP–child interaction. The methods utilized in this study were complementary and in combination produced rich data. However, the use of participatory methods requires considerable forethought and planning on the part of researchers to collect meaningful data. All these methods can be time-consuming, and researchers need to utilize them flexibly to avoid fatiguing participants. More accounts of the effective use of participatory methods in different contexts should be shared so that researchers can learn from the experiences of others, in particular what works and what does not and in which contexts. Researchers need to think carefully about the patient population and the clinical context when choosing which methods to utilize in future studies. This is particularly important when children are extremely ill during data collection. The use of a methods “toolbox” empowers children to select which participatory activity they would like to complete and can avoid children being made to feel awkward or coerced into taking part.
Footnotes
Acknowledgements
The authors are enormously grateful to the children, their families, and staff who took part in the “Talking With Children Study.”
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The “Talking With Children Study” was funded by the Olivia Hodson Cancer Fund. G.B.’s post was supported by the Olivia Hodson at the time of the study and thereafter, during completion of analysis and writing period, by the Great Ormond Street Children’s Charity’s core grant to Louis Dundas Center for Children’s Palliative Care. M.B.L.’s post is supported by funding from True Colors Trust. Acknowledged by the relevant authors is support received from the NIHR Great Ormond Street Hospital Biomedical Research Center.