
Abstract
Introduction:
Recognizing and correcting inhaler technique faults are critical for pharmacists. This study assesses the inhaler usage practices, attitudes, and knowledge among pharmacists.
Methods:
This cross-sectional study was conducted among 200 pharmacists in 2 provinces (Karbala and Najaf) from October 1, 2022, to the end of December 2022.
Results:
Two hundred Iraqi pharmacists, aged 28.1 ± 4.6 years, and randomly selected from Najaf and Karbala, participated in the study. The use of inhalers was well-known to about one-third of the participants. Most participants felt that using inhalers properly impacts how well a patient responds to treatment and that pharmacists must take courses to improve their credentials as educators. About a third of the volunteers checked how inhalers were used and explained the inhale-hold technique.
Conclusion:
In conclusion, pharmacists in Iraq demonstrated a fair level of knowledge and practice regarding inhaler usage techniques, with a good attitude toward teaching patients how to use their inhalers. The training programs on how to use inhalers would be beneficial in improving their healthcare services.
Introduction
Chronic respiratory diseases, including chronic obstructive pulmonary disease (COPD) and asthma, significantly impact the respiratory system by narrowing the airways. This condition necessitates the use of bronchodilators to alleviate symptoms and improve airflow. These diseases represent considerable global health challenges, often resulting in severe morbidity and mortality. In 2019, COPD was attributed to 3.23 million deaths. Notably, in low- and middle-income countries, it accounts for approximately 90% of all deaths among individuals under the age of 70. 1 On the other hand, asthma is a prevalent chronic disease that affects individuals across all age groups. It is a significant non-communicable illness that has been responsible for more than 455,000 fatalities globally in 2019. According to estimates, approximately 262 million individuals worldwide are affected by this condition. 2 People with Asthma and COPD can control their symptoms by inhaling medication to lead a normal daily life. 3 Proper inhaler technique is essential for achieving maximum effectiveness. Recent research has indicated that, despite the prevalent use of inhalers, a significant number of patients are not using them correctly, and many patients request regular training to improve their inhalation technique. 4 Adherence to proper inhaler technique can significantly enhance patients’ respiratory function and overall quality of life.5–7 Furthermore, this can help prevent poor disease control, exacerbations, and increased healthcare costs. 8 It is imperative to note that there are only three significant categories of interventions for improving inhaler technique: technological adaptations, healthcare provider education, and patient or caregiver education. 9 Clinical guidelines recommend that healthcare professionals check their patients’ inhaler technique regularly. 10 However, it can be challenging for clinicians to provide effective intervention if they find a patient’s inhalation technique incorrect due to their busy schedule. The role of pharmacists encompasses a range of responsibilities, including, but not limited to, the dispensing and monitoring of medication use. Pharmacists play a crucial role in identifying and addressing errors associated with inhaler techniques, thereby significantly contributing to patient safety and optimal therapeutic outcomes.11–13 Pharmacists play a vital role in the healthcare system, serving as fundamental contributors to ensuring that patients use medications effectively for optimal outcomes. Proficiency in inhaler usage techniques is a key area of expertise for pharmacists, and their knowledge, attitudes, and practices in this domain are crucial for the success of patient care. To ensure the highest quality of care, comprehensive research has been conducted to evaluate the inhaler usage education provided by pharmacists. 14 This study aims to provide a comprehensive vision for the educational needs of healthcare professionals, thereby enhancing their knowledge and practice to achieve improved patient outcomes. By emphasizing the importance of inhaler usage education, pharmacists can substantially impact their patients’ lives and contribute to the overall enhancement of healthcare services. This study aims to evaluate pharmacists’ knowledge, attitudes, and practices regarding inhaler usage techniques.
Methods
Study design and setting: This cross-sectional study was conducted among 200 pharmacists in 2 provinces (Karbala and Najaf). The researcher developed a new tool, the “Questionnaire,” to evaluate pharmacists’ knowledge, attitudes, and practices regarding inhaler usage techniques. Participants: Pharmacists were surveyed regarding their willingness to participate in the study, which employed a convenient sampling methodology. They completed the questionnaire independently as a self-administered questionnaire. The researcher distributed the questionnaire to pharmacists while they were engaged in their professional duties within their respective pharmacies. The questionnaire was rigorously validated for use in the study, which focused on pharmacists, regardless of whether they were employed in community pharmacies, hospital pharmacies, or both. According to the Iraqi Code of Ethics, pharmacists are permitted to work in both the private and public sectors. 15
Validity and reliability: To ensure face and content validity, the questionnaire was reviewed by six specialized pharmacists, five of whom were faculty members with experience and expertise in survey instrument development and research. Modifications suggested were considered, and changes were made accordingly. Reliability analysis of the questionnaire using Cronbach’s alpha showed an internal consistency reliability of 0.9. The estimated time required for participants to complete the questionnaire was approximately 10 min.
Demographic information was settled, a few questions related to the pharmacist’s knowledge, attitude, and practice regarding proper inhaler usage technique were adapted and rephrased according to the aim of the study from the literature review.16,17 Some suggestions were made by the experts who reviewed the questionnaire.
The questionnaire was evaluated and translated according to the Translation and Cultural Adaptation—Principles of Good Practice. 18 After preparing the questions, the researcher started forwarding translation to the Arabic language, reconciliation, back translation, back translation review, harmonization, cognitive debriefing, review of cognitive debriefing results, finalization, proofreading, and the final report was prepared. 18
Study size: The sample size needed for the study was calculated using the equation below 19 :

Where n = the sample size; Z = the statistic for the 95% level of confidence used in the power analyses, which was 1.96; p = the expected prevalence or the proportion used, which was (7%) = 0.07 according to the World Bank, Iraq population about 42,000,000. 20 The number of Iraqi pharmacists is about 31,000 21 ; and d = the precision used, which was 0.036 (according to Niang d = 1/2 p. 22 By applying these values in the equation, the sample size will be equal to 192, by adding an extra population to avoid bias and missing data, it will be 200 pharmacists.
The criteria for inclusion in this study primarily involved the enrollment of licensed pharmacists who were actively employed in private and/or public sectors settings at the time of the research.
Ethics approval and consent to participate
This study was approved by the Institutional Review Board of Al-Zahrawi University College (ZUC 014 on 01-06-2022). All participants provided informed consent and signed a form upon participation in the study. All methods followed relevant guidelines and regulations in compliance with the STROBE Statement.
Statistical analyses and variables
The data were analyzed using the SPSS (version 20) software package (SPSS Inc., Chicago, IL, USA); the age of the participants and the duration of their work as community pharmacists were presented as mean ± SD. Other variables were categorical variables and were presented as numbers and percentages. Respondents who participated in the pilot study were excluded from the final study analyses. Knowledge, attitude and practice variables were categorized using Bloom’s cut-off point. In the knowledge section, which consists of 5 questions with a total possible score of 10, correct answers (yes) received a score of 2 points each. Incorrect answers (no) received a score of 0 points, while partially correct answers were assigned a score of 1 point. Participants’ overall knowledge scores were categorized according to Bloom’s cut-off points: a score between 8 and 10 points was considered “good,” a score between 4 and 7 points was classified as “fair,” and a score of less than 4 points was deemed “poor.” In the attitude section, which consists of 3 questions with a total possible score of 6 points, responses were scored as follows: each correct response (answered “yes”) received 2 points, incorrect responses (answered “no”) received 0 points, and responses where participants answered “I don’t know” received 1 point. Participants’ overall attitude scores were categorized using Bloom’s cut-off points: a score between 5 and 6 points was considered “good,” a score between 3 and 4 points was deemed “fair,” and a score of less than 3 points was classified as “poor.”
In the practice section, which contains 7 questions with a total possible score of 14 points, responses were scored as follows: each correct response (answered “always”) received 2 points, incorrect responses (answered “never”) received 0 points, and responses where participants answered “sometimes” received 1 point. Participants’ overall practice scores were classified based on Bloom’s cut-off criteria: a score ranging from 10 to 14 points was categorized as good, a score from 5 to 9 points as fair, and a score of less than 5 points as poor. In the barriers section, which consisted of 5 questions with a total possible score of 10 points, each response indicating “always” was assigned a score of 2, responses indicating “never” received a score of 0, and responses indicating “sometimes” were awarded a score of 1. Participants’ overall barriers scores were also categorized following Bloom’s cut-off criteria: a score between 7 and 10 points was deemed good, a score between 4 and 6 points was classified as fair, and a score of less than 4 points was considered poor. The score for each knowledge, attitude, practice, and barrier was calculated, and all the results were presented in tables as appropriate.
Results
Two hundred Iraqi pharmacists participated in the study randomly from two provinces (Karbala and Najaf). Their mean age was 28.1 ± 4.6 years, and the mean duration of their work as community pharmacists was 5.3 ± 3.6 years. Table 1 illustrates demographic data of the participants. The male participants outnumbered the female participants (56.5%), and the majority of participants held a bachelor’s degree in pharmaceutical science (88%). More than two-thirds of them work in both hospital and community pharmacies.
Demographic data of the participants.

Table 2 illustrates participants’ knowledge regarding inhaler usage technique. About one-third of the participants reported good knowledge of inhaler usage techniques (Table 2).
Participants knowledge regarding inhalers usage techniques.
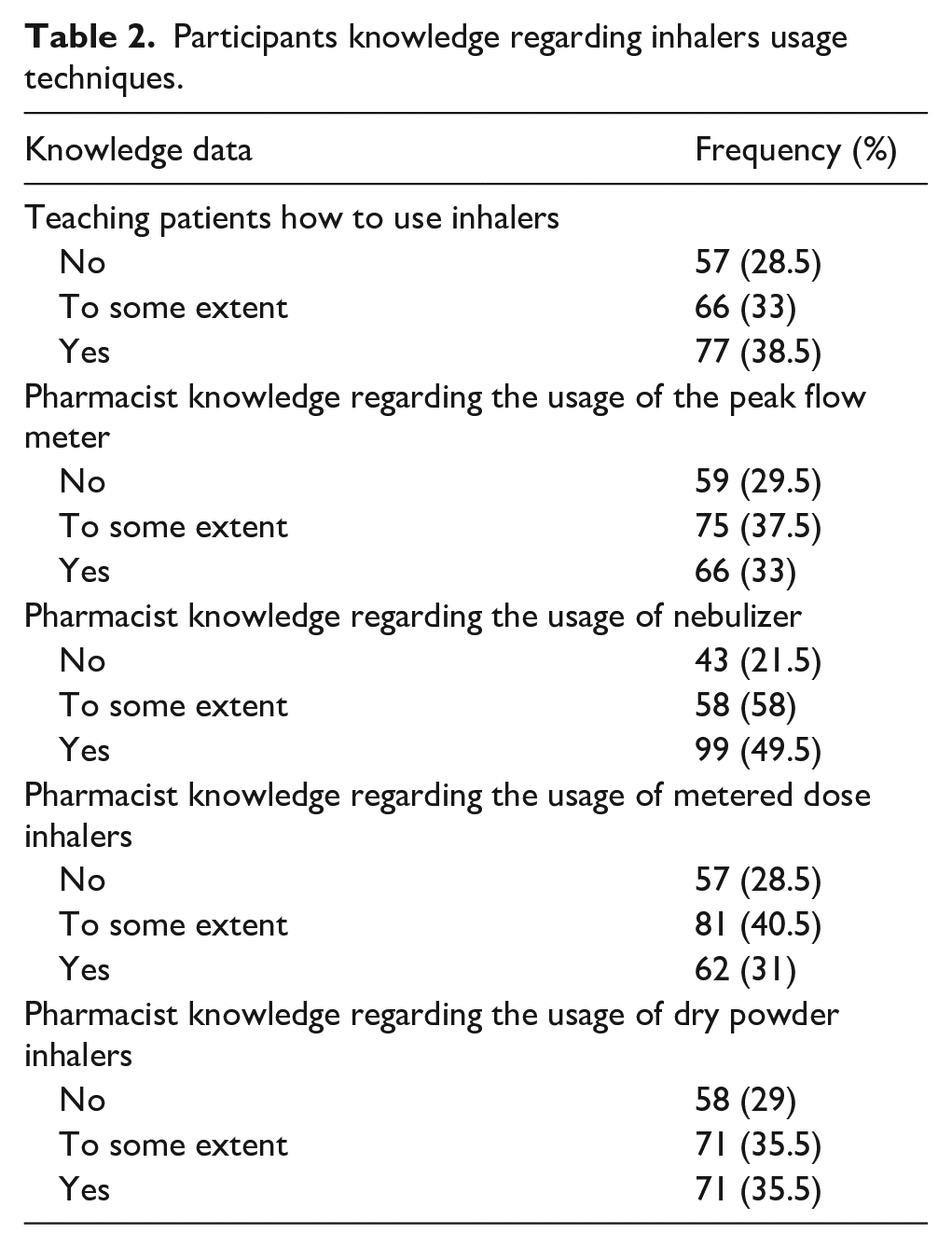
Table 3 shows participants’ attitudes regarding inhaler usage techniques. The majority of participants agreed that proper inhaler usage techniques significantly affect treatment success, and pharmacists should attend courses to become more qualified educators.
Participants’ attitude regarding inhaler usage techniques.
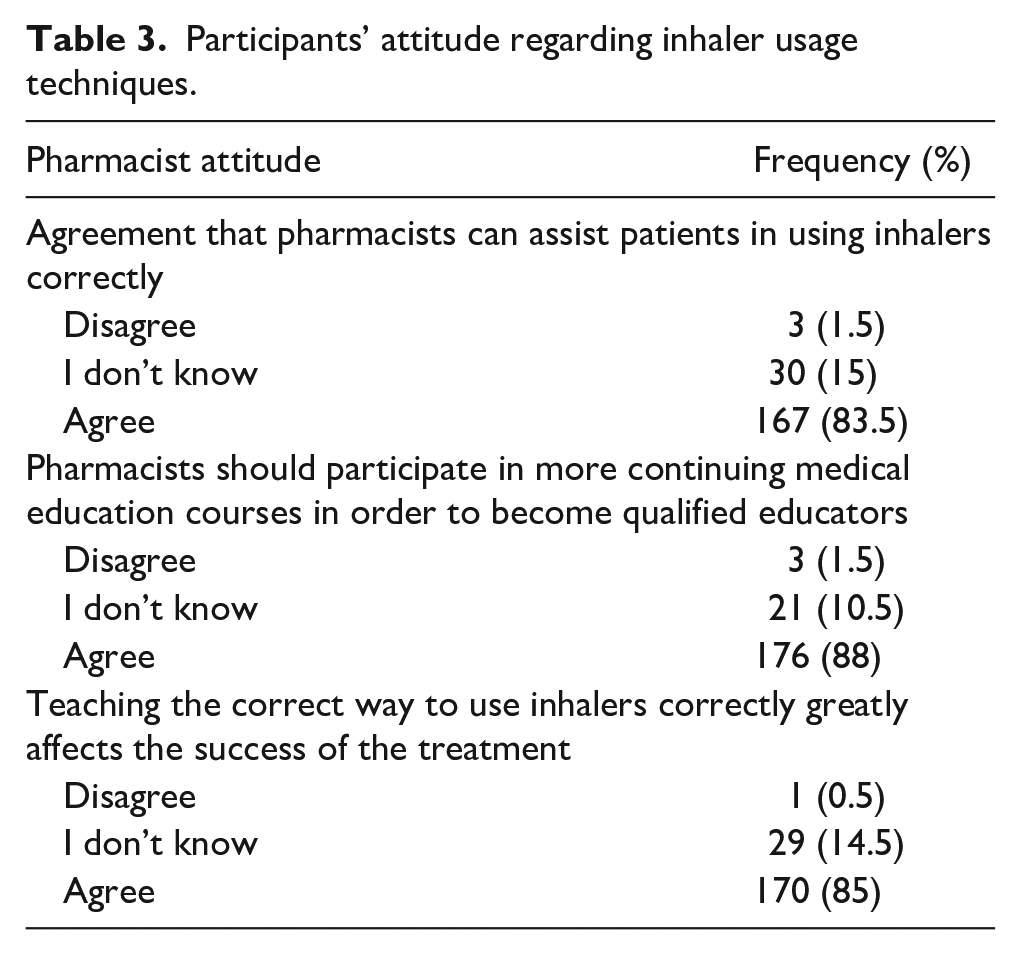
Table 4 shows participants’ practice regarding inhaler usage techniques. Approximately one-third of the participants reviewed inhaler usage techniques and explained how to take a breath and hold it. About half of the participants always give time for discussion with the patients.
Participants practice regarding inhalers usage techniques.

Table 5 illustrates the barriers that pharmacists face and refrain from teaching patients how to use inhalers correctly. Approximately 25% of the participants reported a shortage of time, either in their own time or in patients’ time. About one-third of them said that a lack of confidence and skills prevents them from counseling.
Participants’ barriers to teaching inhaler usage techniques.

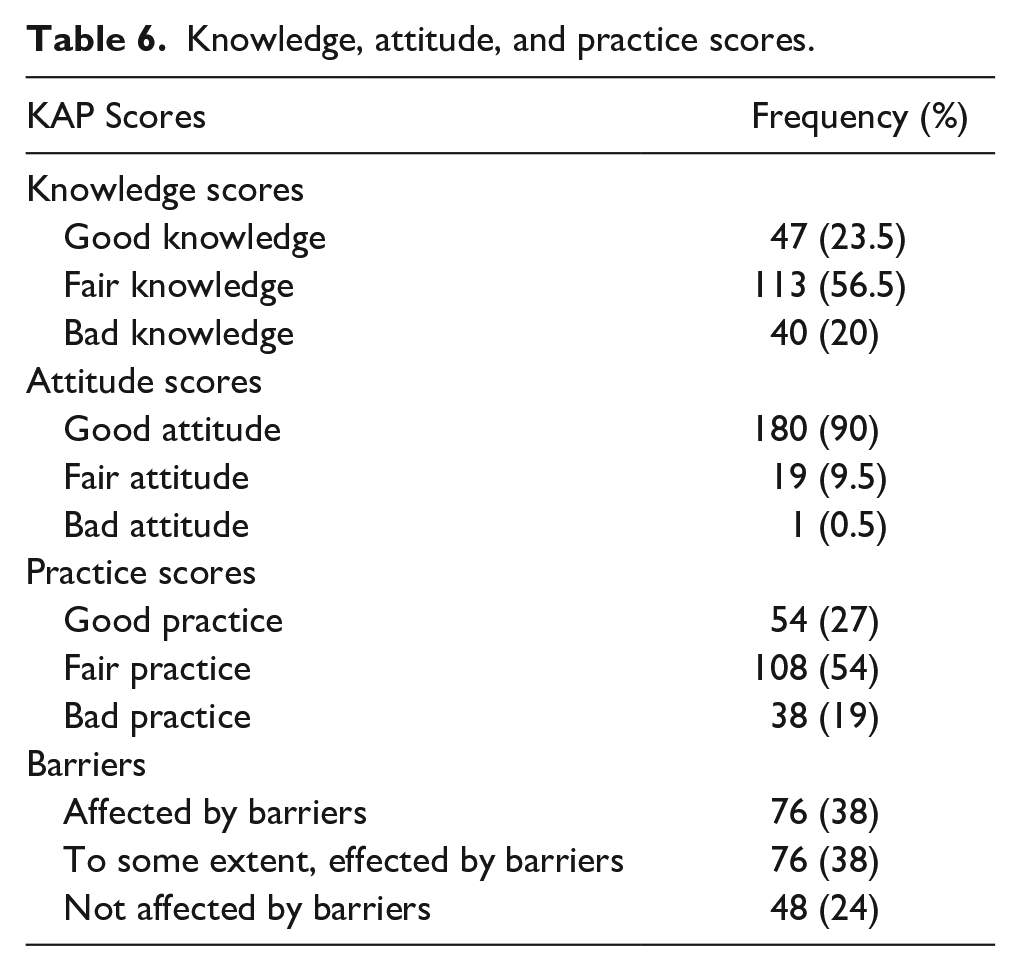
Table 6 illustrates KAP scores for the study participants; about half had fair knowledge and practice regarding inhaler usage techniques. The majority of the participants had good attitude regarding teaching their patients inhaler usage techniques. Half of the participants were not affected by the barriers to teaching their patients inhaler usage techniques.
Knowledge, attitude, and practice scores.
There was a significant association between the fair knowledge scores and each participant’s age and the pharmacist specialization area (who had both hospital and community practice); p < 0.026 and p < 0.03, respectively.
Discussion
The knowledge of pharmacists regarding inhaler usage techniques has a significant impact on the effectiveness of patient treatment. Pharmacists who have a thorough understanding of the various types of inhalers and proper inhalation techniques can guide patients on how to use their inhalers correctly. This can improve treatment outcomes, such as better symptom control and a reduced risk of adverse effects.
Knowledge and attitude: The study indicated that slightly over 50% of the participants had a fair understanding of how to use inhalers correctly. Among those with good knowledge, only half had knowledge of how to use nebulizers correctly. A study conducted in Portugal revealed that as many as 87% of patients commit at least one error while using inhalers, and Portuguese community pharmacies make efforts to review and correct their inhaler usage during every visit. 23 A cross-sectional study found that nurses and doctors had poor knowledge of how to use the metered dose inhaler and spacer device. 24 A survey conducted in Iraq revealed insufficient knowledge among pharmacists regarding inhalation aerosol device techniques and therapies. 25 An online survey found that slightly over half of COPD patients preferred using a small-volume nebulizer over an MDI or DPI due to its ease of use, convenience, and fast-acting nature. 26
Based on this study, it was found that most participants had a positive attitude toward educating their patients about inhaler use and improving their own skills. Similarly, a study by Akram et al. 27 suggested that asthma patients should be provided with counseling on asthma management and education. Significant changes in the level of agreement with certain beliefs and attitudes were observed after an educational intervention. These changes included an increased understanding of the importance of regularly assessing and educating patients, as well as an improvement in the confidence and comfort levels of healthcare professionals when considering and educating patients. It was also noted that educating patients is not solely the responsibility of physicians. 28
Practice: Approximately one-third of the participants in the study demonstrated good practice in checking their patients’ inhalation technique. However, despite this, half of them were found to have only fair practice scores. The findings align with those of a prior study that indicated healthcare professionals possess a moderate level of knowledge and practical experience concerning inhaler devices. 29 The significance of pharmacist-led interventions and their positive impact on inhaler usage techniques has been highlighted through a study conducted in Nepal. In this study, pharmacists delivered interventions that resulted in an improvement in the quality of life, asthma management, and inhalation techniques among patients with asthma. 30 A study conducted in Iraq involved pharmacist-led education sessions with an average counselling time of 15 min, which resulted in a significant improvement in inhalation technique. 31 In an uncontrolled pre-post Norwegian study, it was found that the Inhalation Technique Assessment Service provided by trained pharmacists resulted in significant improvement in the inhalation technique of both new and experienced users. Furthermore, this improvement was sustained through two follow-ups across all assessed devices, demonstrating the effectiveness of the service. 32 Based on a prospective multi-center intervention study, it is evident that community pharmacy-based pharmacists are well-suited to provide significant supplementation to doctor-based education in inhalation technique for asthma and COPD patients with poor inhalation technique. 33 On the other hand, in 2015 a cross-sectional study in Abu Dhabi found a good practice with regard to the use of an inhaler. 34 A questionnaire was administered to 365 parents of children, which revealed that a minority of participants demonstrated a satisfactory level of knowledge regarding inhaler use. Nevertheless, those who exhibited this knowledge tended to show positive attitudes and engage in effective practices related to inhaler usage. 34
Barriers: Based on the study’s findings, it is evident that time poses a significant barrier for both patients and pharmacists, as reported by 25% of the participants. Furthermore, a considerable number of participants expressed a lack of responsibility in teaching patients how to use inhalers, while many others cited insufficient skills as the main obstacle. The results are consistent with those of another study, which reported that healthcare professionals often face a shortage of time to assess and educate patients using MDIs. 28 In alignment with our findings, the Malaysian study demonstrated that most Malaysian pharmacists (over 95%) lack the time to provide specific asthma services, according to a study, while the majority agreed to participate in seminars, courses, conferences, and workshops. 27 Patients’ attitudes indicated that low levels of pharmacist knowledge and skills were barriers to implementing pharmacy-led asthma care in the literature reviews. 35
Implications for practice and policy: Pharmacists have a unique opportunity to enhance patient care by improving inhaler technique and adherence. By leveraging their accessibility and expertise, pharmacists can play a critical role in promoting optimal disease control and better outcomes for patients and healthcare providers alike. 36 By providing pharmacists with the necessary time and resources, improving patient education materials, and investing in pharmacist training, we have the potential to significantly enhance inhaler education and improve treatment outcomes. Collaborate to guarantee that patients receive the utmost quality of care attainable. It is essential for future research to broaden its scope to encompass the entire country, as the current study is confined to only two governorates, thereby presenting a substantial gap in our understanding of the issue. To gain a more comprehensive understanding of the subject matter, it is essential to incorporate a diverse range of samples in future studies, which will lead to the generation of accurate and reliable results. Immediate action must be taken to ensure a thorough evaluation of the prevailing situation.
Conclusion
Research findings indicate that pharmacists in Iraq demonstrate a fair level of knowledge and practical skills regarding inhaler usage techniques. Additionally, there is a positive inclination among pharmacists toward educating patients on the correct use of inhalers. The implementation of training programs for pharmacists may enhance the quality of healthcare services delivered.
Supplemental Material
sj-docx-1-phj-10.1177_22799036251368440 – Supplemental material for Pharmacist’s knowledge, attitude, and practice toward proper inhaler technique
Supplemental material, sj-docx-1-phj-10.1177_22799036251368440 for Pharmacist’s knowledge, attitude, and practice toward proper inhaler technique by Khansaa A. Ibrahim Albaroodi in Journal of Public Health Research
Footnotes
Acknowledgements
The author thank all the pharmacists who participated in and facilitated our work.
Ethical considerations
This study was approved by the Institutional Review Board of Al-Zahrawi University College (ZUC 014 on 01-06-2022).
Consent to participate
All participants agreed to participate and signed an informed consent form upon participation in the study. All methods followed relevant guidelines and regulations in compliance with the STROBE Statement.
Author contributions
KAI Albaroodi set the study design, data collection, data analyses, reporting results, preparing the manuscript, and reading and approving the final manuscript.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
This article file includes all data generated during this study; raw data is available upon request.
Data access statement
The author had complete access to the study data.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.