
Abstract
Background and aims:
Despite the growing spread of schistosomiasis among preschool children (pre-SAC), evidence is scarce on caregivers’ knowledge, attitudes, and practices (KAP). The current study investigated the level and determinants of KAP of primary caregivers of pre-SAC towards Schistosoma mansoni (S. mansoni) infection in southern Ethiopia.
Design and methods:
A cross-sectional study was conducted among 887 primary caregivers of pre-SAC. A multistage sampling technique was applied, wherein study participants were selected through a simple random sampling technique. A pre-tested, structured questionnaire was used to collect data at the respondent’s home. Multivariable logistic regression with a cluster-robust variance estimation method was used.
Results:
The knowledge level of S. mansoni infection among respondents was 358 (37%). Only 486 (54.8%) of caregivers had a favorable attitude, while 513 (57.8%) of caregivers had good practices. Being from the poorest (AOR = 0.75, 95% CI: 0.57–0.99) and poorer (AOR = 0.55, 95% CI: 0.47–0.65) households were significant determinants of knowledge. The age range of 23–29 years, not having formal education, and being from the poorest households were significant determinants of attitude. Being unmarried (AOR = 0.57, 95% CI: 0.36–0.89) and not receiving information about the disease from any source (AOR = 0.40, 95% CI: 0.26–0.62) had a significant association with good practice.
Conclusion:
The present study revealed a low level of knowledge, unfavorable attitudes, and poor practices about S. mansoni among primary caregivers. To enhance caregivers’ KAP, tailored health education is recommended.
Introduction
Schistosomiasis is a poverty-related NTD caused by a parasite blood fluke or trematode of the genus Schistosoma. 1 It is the second most predominant and has enormous health, education, and socio-economic impacts following malaria. 2 Humans are the definitive host for adult Schistosoma parasites, while specific freshwater snails act as intermediate hosts.3,4 Globally, six species of schistosomes affect human beings. 1 S. mansoni, S. hematobium, and S. japonicium are the three main species of schistosomes that cause disease in humans, but S. mansoni and S. haematobium are widespread. 1 Among the two endemic species occurring in sub-Saharan Africa (SSA), S. mansoni is the most predominant species. 1 S. mansoni is widely distributed in Ethiopia, whereas S. hematobium is mainly restricted to the Rift Valley region (i.e., Somali region). 5
S. mansoni infection is associated with undesirable acute and chronic physical and cognitive outcomes.2,6 –8 The long-term effect of these infections may induce permanent disability or even death in some patients. 9 S. mansoni infection can be prevented using key approaches which include mass praziquantel administration; access to safe water, basic sanitation, and the promotion of hygiene practices (WASH), vector control, and health education.10,11 These interventions need to be integrated to play a critical role in the successful control or elimination of S. mansoni infection.12,13
The success of community-based control interventions depends on community acceptance of the program. 14 Programs should first intend to realize the community’s knowledge, attitude, and practices (KAP) toward schistosomiasis before the implementation of the program activities. 15 According to recent findings, primary caregivers are critical in the control of S. mansoni infection among preschool-aged children (pre-SAC). 10 A review conducted in sub-Saharan Africa (SSA) indicated the importance of caregivers’ involvement in the planning and implementation of control programs. 16 Nevertheless, lacking appropriate information and a favorable attitude, they may be involved in risky practices that predispose their young children to S. mansoni infections.17,18 A study from Nigeria 19 revealed that caregivers contributed to the spread of schistosomiasis among children through risky water-related practices.
Lack of knowledge and misperceptions about S. mansoni infection among caregivers may contribute to risky contact with infested water bodies.20,21 Evidence shows that in endemic areas, women perform most of the water contact activities, putting themselves and their pre-SAC at high risk of infection.21,22 A report from Nigeria 23 revealed that 16.2% of the caregivers engaged in open defecation in surrounding bushes, 1.8% directly to the river, and 13.2% depended solely on water from the river for domestic usage. In Ethiopia, 24 27.8% of households practiced open defecation. Studies have also shown that the KAP of individuals regarding schistosomiasis is influenced by socio-demographic characteristics, as well as economic and behavioral factors. 25
In endemic countries, including Ethiopia, where S. mansoni26,27 is predominant, community-based KAP studies on schistosomiasis are scarce. These hinder the attainment and sustainability of the evidence-based control interventions targeted toward the elimination of schistosomiasis as a public health threat to at-risk population groups. 9 This study, therefore, assessed the level and determinants of KAP of pre-SAC toward S. mansoni infection in southern Ethiopia.
Materials and methods
Study design and setting
A cross-sectional community-based study was conducted from August to December 2021 among primary caregivers of pre-SAC (aged 4–7 years) in Hawella Tulla district, southern Ethiopia. The Neglected Tropical Diseases (NTDs) burden assessment conducted in Ethiopia between 2013 and 2014 revealed a 54.9% prevalence of S. mansoni infection in the study district. 28 The district is located 289 km south of Addis Ababa, the capital city of Ethiopia. It is situated at an altitude of 1800 m above sea level and has an annual rainfall of 1123 mm and a temperature of 13°C–27°C. Lake Hawassa is the water source of the residents of the district for domestic, agricultural, fishing, and other uses. A map of the study district is presented in Figure 1. 18

Map of the study site. The top left is the map of Ethiopia. The middle-left figure shows the map of the Sidama region where the study kebeles are located. The bottom-left figure indicates the map of Hawassa City administration, where the study district and kebeles are found. The figure on the right shows the map of Lake Hawassa and the kebeles where the study was conducted.
Study population
The study population was primary caregivers of pre-SAC aged 4–7 years.
Inclusion and exclusion criteria
Primary caregivers who had pre-SAC aged 4–7 years, residing in the study area permanently, and who gave written consent were included in the study. Primary caregivers who had health problems that hindered their involvement were excluded from the study due to the inability to conduct interviews.
Sample size and sampling technique
OpenEpi sample size calculation software was used to compute the sample size. The level of knowledge, attitude, and practice, and the significant determinants of KAP were considered during the sample size determination. The assumptions: the level of knowledge of at least one sign and/or symptom of schistosomiasis (54.4%), attitude of willingness to participate in praziquantel preventive chemotherapy campaigns (79.2%), and practice of washing in open water (61.2%) based on a previous study 29 ; absolute precision of 5%; and a design effect of 1.5. Accordingly, the total sample sizes calculated after adjusting for the anticipated non-response rate (10%) were 636, 423, and 609. The sample size desired was also calculated using variables significantly linked with KAP in a previous study, 30 setting the ratio of unexposed to exposed at 1%, the level of confidence at 95%, power at 90%, and the estimated non-response rate of 10%. The estimated sample sizes accordingly were 317, 910, and 127. Then, the largest sample size computed from the risk factors (n = 910) was used.
A multistage sampling technique was applied to select the study kebeles (the lowest executive units in Ethiopia). Out of the 12 kebeles of the district, 6 were designated based on the S. mansoni infection rate among SAC. 28 From the six kebeles, three (Tullo, Finchawa, and Chafe Kotijebessa) were chosen with the lottery technique. In the selected kebeles, the health extension workers prepared the list of community members eligible for the study through house-to-house enumeration before the study initiation. The sample size allocation was done proportionate to the population size of each kebele. Then, the study participants were selected using a simple random sampling method via a computer-generated random number. In cases where the chosen participant was not accessible at home during the initial visit, two repeated visits were made, after which the person was considered a non-respondent.
Data collection
A pre-tested, structured, face-to-face interviewer-administered questionnaire was used to collect data. The questionnaires prepared in the English language were translated into local languages (Amharic and Sidamu Afoo). The consistency of the tool was preserved by translating it back into English. The Amharic or Sidamu Afoo questionnaire was applied based on the language preference of the participants during the interview. The questionnaire covered such issues as socio-demographic features of the respondents; sources of information about S. mansoni infection, signs and symptoms, modes of transmission, prevention, treatment and control, severity, predisposing factors, and preventive measures. Eight public health experts for data collection and two senior experts for supervision were recruited from public health institutions. Then, the data collectors and supervisors were trained in data collection tools, interview techniques, and their roles and responsibilities for 2 days by the research team. Before the study initiation, the questionnaire was pre-tested on 5% of the entire sample size of caregivers in the Wondo Genet district. Based on the pre-test findings, the data collection tool has been revised.
Data on a household’s possession of particular assets such as radio, refrigerator, television, bicycle, motorbike, car, phone/cell phone; the household’s amenities such as water supply, toilet, flooring, walls/house, roof, electricity, and cooking fuel were considered to calculate the household wealth index. The household wealth index was computed using the principal component analysis (PCA). The sampled households were categorized into five quantiles using the scores, and each member of a household received that household’s quintile category. Regular supervision of data collectors was made to confirm the appropriate implementation of the study daily.
Variables of the study
Knowledge: The knowledge of respondents about S. mansoni infection was measured by asking a series of five closed-ended questions containing multiple options regarding signs and symptoms, prevention strategies, control and treatment methods, and modes of transmission. Participants who responded “NO” to the screening question were given a score of “0” and included in the knowledge level assessment. Questions related to knowledge were scored and pulled together, and the mean knowledge score was then calculated by dividing a scaled score by the number of respondents responding on the scale. Knowledge was recorded as high if more than or equal to the mean score, while low for a score less than the mean.
Attitude: The perception of participants regarding the severity of the disease, risk factors, signs and symptoms, mode of transmission, prevention strategies, treatment, and control of S. mansoni infection was assessed using closed-ended questions. It was measured using a questionnaire containing seven questions. The participant’s response and each question were ranked by a Likert scale using a numerical score ranging from 1 to 5. (Strongly disagree = 1, Disagree = 2, neutral = 3, Agree = 4, Strongly agree = 5). Reverse-coding for negatively phrased items was done. Higher scores show a more positive attitude. The overall attitude score of a participant was determined based on the mean scores computed by dividing on-scale scores by the number of participants responding on the scale. The attitude was delineated as a favorable attitude if the mean attitude score was more than or equal to the mean, and an unfavorable attitude for caregivers who had responded less than the mean attitude score.
Practice: The respondents’ practice with S. mansoni infection was evaluated by asking a single question that had nine major response options about where the study participants washed their clothing often. The response options listed were grouped into predisposing and protective practices. Respondents who reported at least one predisposing practice were categorized as having poor practice, while those who reported “No” for any predisposing practices were labeled as having good practice.
The exposure variables encompass age, educational level, marital status, occupation, wealth quintile, and source of information about S. mansoni infection.
Ethical considerations
The Institutional Review Board (IRB) of the College of Medicine and Health Sciences of Hawassa University (Ref. No: IRB/200/13) approved the study. It has been conducted as per the Declaration of Helsinki with the relevant guidelines and regulations. Written consent was obtained from the participants to participate in the study. Participants were informed about their right to withdraw from the study at any point without punishment, and that their withdrawal would not affect them.
Statistical analysis
Stata software version 14 (StataCorp LLC, College Station, TX, USA) was used to analyze data. Descriptive analyses were done by computing frequencies and proportions for categorical variables and means with standard deviations.
Multivariable logistic regression with cluster-robust variance estimation method was conducted to assess the effect of various background characteristics on knowledge, attitude, and practices about S. mansoni infection. The variables were included in the multivariable model using the purposeful variable selection technique as recommended in the literature. 31 Hence, variables with a p-value less than 0.25 on the bivariable model and those variables considered important in other literature were included in the multivariable model.
Results were reported as adjusted odds ratios (AOR) with their 95% confidence intervals (CI). A statistical significance level was set at a p-value of <0.05.
Results
Sociodemographic characteristics
Of the total 910 primary caregivers (all females) of pre-SAC recruited, 887 (97.5%) have participated. The majority, 438 (49.4%) of the caregivers were in the age group of greater than 29–39 years, while 25 (2.8%) of them were unmarried (Table 1). The mean (+ standard deviation (SD)) age of the primary caregivers was 31.4 (+0.2) years.
Sociodemographic characteristics of primary caregivers of preschool children (N = 887).

Note. N: the total number of participants within each category.
Schistosoma mansoni infection knowledge among primary caregivers
Most of the study participants, 655 (73.8%), reported having previously heard of S. mansoni infection. Overall, 409 (46.1%) of the respondents knew the signs and symptoms, while 356 (40.1%) of the participants stated the prevention measures of S. mansoni infection. Moreover, 331 (37.3%) of the primary caregivers knew about the mode of transmission, whereas only 87 (9.8%) knew about the treatment and control of the disease (Figure 2). The overall knowledge level of S. mansoni infection among the respondents was 358 (37%; 95% CI: 33.8%–40.2%).

Knowledge of signs and symptoms, mode of transmission, prevention, and treatment of S. mansoni infection among primary caregivers of preschool children.
Main source of information about S. mansoni infection among primary caregivers
In the present study, health extension workers were identified as the most common sources of information reported by 181 (20.4%) of participants, followed by research institutions cited by 104 (11.7%) of participants, while community meetings were distinguished as the least information source reported by 41 (4.6%) of participants (Figure 3). The knowledge score among caregivers ranged from 0 to 14 (the maximum possible score was 22). The mean knowledge score of the caregivers was 4.08.

Main source of information about S. mansoni infection among primary caregivers of preschool children.
Determinants of knowledge level about S. mansoni infection
According to the wealth index, the poorest (AOR = 0.75, 95% CI: 0.57–0.99) and poorer (AOR = 0.55, 95% CI: 0.47–0.65) households exhibited reduced odds of reporting good knowledge of S. mansoni infection relative to those from the richest wealth households. No significant association was observed with other variables (Table 2).
Determinants of knowledge level toward Schistosoma mansoni infection among primary caregivers of preschool children (N = 887).

AOR: adjusted odds ratio; CI: confidence interval; COR: crude odds ratio; N: entire number of participants within each category.
OR: odds ratio could not be estimated because it predicts failure perfectly.
p-value < 0.05 means statistically significant.
Attitude of primary caregivers of pre-SAC about S. mansoni infection
A total of 486 (54.8%) primary caregivers had a favorable attitude about the mode of transmission of S. mansoni infection, prevention, treatment, and control methods (Table 3). The attitude score among caregivers ranged from 16 to 34 (maximum possible score, 35). The mean attitude score of the caregivers was 3.54.
Item-by-item attitude distribution of primary caregivers of preschool children toward Schistosoma mansoni infection (N = 887).
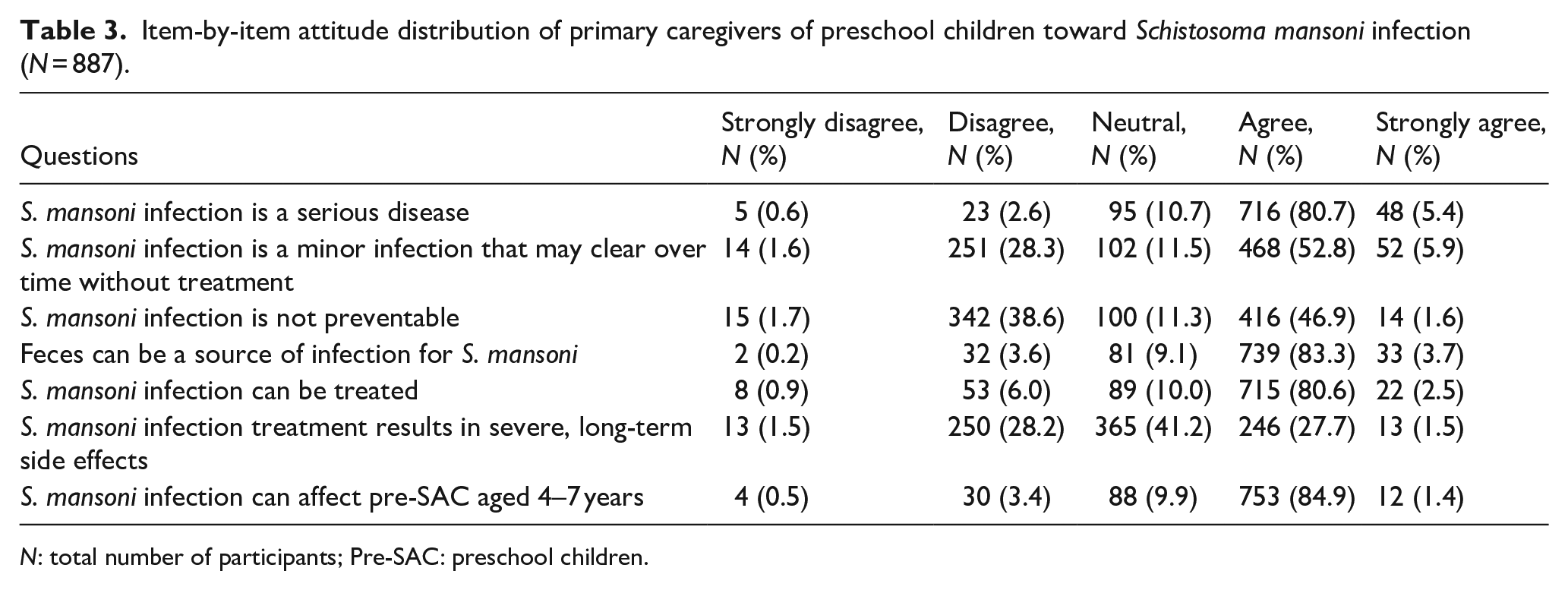
N: total number of participants; Pre-SAC: preschool children.
Determinants of attitude toward S. mansoni infection
Being in the age group of 23–29 years (AOR = 1.18, 95% CI: 1.01–1.37) increased the odds of reporting a favorable attitude towards S. mansoni infection relative to those in the age group of >40 years. A significant association was detected between not having formal education (AOR = 0.80, 95% CI: 0.65–0.98) and reporting favorable attitudes among primary caregivers compared to those having higher education levels. Being from the poorest wealth households (AOR = 0.42, 95% CI: 0.28–0.62) was also a significant determinant of reporting a favorable attitude among primary caregivers compared to those from the richest counterparts (Table 4).
Determinants of attitude status toward Schistosoma mansoni infection among primary caregivers of preschool children (N = 887).

AOR: adjusted odds ratio; CI: confidence interval; COR: crude odds ratio; N: overall number of participants within each category.
p-value < 0.05 means statistically significant.
The practice of primary caregivers of pre-SAC about S. mansoni infection
513 (57.8%) of primary caregivers had good practice related to predisposing factors of S. mansoni infection. Out of the remaining 374 (42.2%) of caregivers who engaged in predisposing practices, the majority used pond 159 (17.9%) or lake 137 (15.5%) water for washing clothes commonly (Table 5).
The level and distribution of practices among primary caregivers of preschool children towards Schistosoma mansoni infection (N = 887).

N: total number of participants; Pre-SAC: preschool children.
Determinants of practice status toward S. mansoni infection
A significant association was detected between being unmarried (AOR = 0.57, 95% CI: 0.36–0.89) and reporting good practice about predisposing factors among caregivers compared to married. Primary caregivers who did not receive any information had 60% (AOR = 0.40, 95% CI: 0.26–0.62) lesser odds of reporting good practices about the disease relative to those who acknowledged the health extension workers as the information source (Table 6).
Determinants of practice toward Schistosoma mansoni infection among primary caregivers of preschool children (N = 887).

AOR: adjusted odds ratio; CI: confidence interval; COR: crude odds ratio; N: total number of participants within each category.
p-value < 0.05 means statistically significant.
Discussion
The present cross-sectional study assessed the level of knowledge, attitude, and practices about S. mansoni infection among primary caregivers of pre-SAC aged 4–7 years residing in three rural districts in southern Ethiopia. The main results of the current study revealed a low level of knowledge, unfavorable attitude, and poor practices of S. mansoni infection among primary caregivers of pre-SAC, with significant variation across signs and symptoms, prevention measures, means of transmission, and treatment and control (ranging from 87 (9.8%) for the treatment and control to 409 (46.1%) for the signs and symptoms.
The knowledge level was low among primary caregivers from the poorest and poorer households. The age range of 23–29 years, not having a formal education, and being from the poorest households were significant determinants of attitude. Moreover, being unmarried and not receiving information from any source were significant determinants of practices of S. mansoni infection.
The present study’s findings revealed that 358 (37%) of the primary caregivers knew about the disease, with significant differences across signs and symptoms, prevention measures, modes of transmission, treatment, and control. Studies conducted in South Africa, 27 Kenya, 32 and a systematic review in SSA 16 also reported similar findings. The knowledge level remained low partly due to weaknesses in the health education structures and a deficiency of community members’ experiences on the health and social effects of S. mansoni infection among respondents. However, knowledge was relatively high, 409 (46.1%) on signs and symptoms, while the least 87 (9.8%) on control and treatment. The observed difference in the knowledge level of some key aspects of S. mansoni infection control and treatment demonstrates the neglect of the health education intervention component in the morbidity control strategy in Ethiopia. Thus, contextual circumstances should be acknowledged when framing health education intervention as a key component of the program to attain and sustain the interruption of disease transmission, particularly in rural settings. Besides, in the current study, the magnitude of favorable attitude about S. mansoni infection was 486 (54.8%). A comparable finding was reported in other studies elsewhere.33,34 Most of the caregivers recognized that the disease could be treated, as was also reported in Tanzania. 35 The overall perception of the primary caregivers is not in favor of breaking the chain of disease transmission.
The study findings indicate that 513 (57.8%) of the primary caregivers had good practices about S. mansoni infection. The present finding is lower than the report from Uganda 36 that indicated 253 (65.7%) of parents/guardians had appropriate practices towards urogenital schistosomiasis among under-five children. The justification for the inadequate good practices could be that, in Ethiopia, S. mansoni infection-related robust interventions such as mass praziquantel administration, health education, WASH, and vector control that channel the information dissemination for the required behavioral change were overlooked caregivers of pre-SAC considering their young children to be safe from the infection due to the presumed reduced interaction with contaminated water sources. However, in our study, risky water-related practices were observed, especially among participants who rely on Lake Hawassa and other infested water sources due to scarce knowledge and unfavorable attitudes about the disease.
In the present study, the poorest wealth index categories exhibited 25% reduced odds of reporting good knowledge, while the poorer showed a 45% reduction compared to the richest wealth category. The possible reason for this might be linked to the lower likelihood of having access to diverse information sources among household members in the lower wealth quantiles than those in higher wealth quantiles. Often, higher wealth quantiles are taken as a proxy for improved health services and health message access. 30
The current study revealed that the younger age group (23–29 years) had increased odds of reporting a favorable attitude relative to the older age group (>40 years). The factor that has accounted for the observed higher odds of reporting a favorable attitude might be that younger people are more likely to recognize the importance of avoiding contact with lake water by considering the long-lasting health impacts of persistent infested water contact relative to their older counterparts.
In the study region, not having formal education decreased the odds of reporting a favorable attitude by 20% relative to those in the higher education level. In Ethiopia, caregivers having lower education have a lower chance of employment. Also, having lower education decreased the chance of active involvement in formal health information dissemination channels and frequent contact with health extension workers, which might have contributed to the reported unfavorable attitude relative to those who have diverse information sources due to their higher education level. 30
The present study has also revealed that the poorest wealth quintile had 58% lower odds of reporting a favorable attitude relative to the richest households. The justification for this association may be that the respondents with lower wealth quintiles had more attachment to lake water to obtain their living relative to those with higher wealth quintiles. 30
The present study has found that being unmarried leads to 43% lesser odds of good practice compared to married caregivers. The possible explanation for this finding might be attributed to the reduced access to resources that may affect health information access among unmarried caregivers compared to married and may be involved in riskier health-related behaviors. 37 Furthermore, the current study revealed that 60% lesser odds of reporting good practice were observed among caregivers who did not receive any information about S. mansoni infection from any source, relative to health extension workers as a source of information. The gap in understanding a disease process and recommended prevention measures related to low health literacy accounted for this finding.
The current evidence on the level of KAP towards S. mansoni infection among primary caregivers of pre-SAC shapes the health and well-being of marginalized populations infected or affected by S. mansoni infection. Thus, our research makes substantial contributions to knowledge, policy, practice, and future research by broadening the scope of school-age children-focused interventions toward extensive commitments to the inclusion of the overlooked at-risk populations to tackle S. mansoni infection in Ethiopia and other similar endemic settings.
As a portion of the limitations, the current study didn’t determine the level of S. mansoni infection among primary caregivers that may benefit the infected participants and accelerate the information dissemination, which enhances the improvement of KAP among women in a high-risk population in highly endemic communities. The other limitation is that we did not exhaust all the prevailing potential behavioral practices with effects on the desired behavior change among primary caregivers, which may overestimate the level of practice as an outcome. However, our results provide insight into the general situation of KAP toward S. mansoni infection among primary caregivers of pre-SAC in Ethiopia.
Conclusions
Our study revealed the low level of knowledge, unfavorable attitudes, and poor practices that indicated critical gaps in integrated intervention strategies for S. mansoni infection. Hence, S. mansoni infection elimination efforts should ensure the involvement of primary caregivers during the planning, execution, monitoring, and evaluation activities of the interventions in endemic settings. Moreover, health education should be combined with other strategies to effectively enhance caregivers’ KAP in endemic communities.
Supplemental Material
sj-pdf-1-phj-10.1177_22799036251361622 – Supplemental material for Knowledge, Attitudes, and Practices of Primary caregivers of Preschool children towards Schistosoma mansoni infection in Southern Ethiopia: A community-based cross-sectional study
Supplemental material, sj-pdf-1-phj-10.1177_22799036251361622 for Knowledge, Attitudes, and Practices of Primary caregivers of Preschool children towards Schistosoma mansoni infection in Southern Ethiopia: A community-based cross-sectional study by Tafese Tadele, Ayalew Astatkie, Birkneh Tilahun Tadesse, Eyasu Makonnen, Solomon Mequanente Abay and Eleni Aklillu in Journal of Public Health Research
Footnotes
Acknowledgements
We are grateful to the health extension workers of the three study kebeles for their assistance. We also acknowledge the primary caregivers of Pre-SAC who participated in the study.
ORCID iDs
Ethical considerations
The Institutional Review Board (IRB) of the College of Medicine and Health Sciences of Hawassa University (Ref. No: IRB/200/13) approved the study. It has been conducted as per the Declaration of Helsinki with the relevant guidelines and regulations.
Consent to participate
Written consent was obtained from the participants to participate in the study. Participants were informed about their right to withdraw from the study at any point without punishment, and that their withdrawal would not affect them.
Authors contributions
TT, AA, BTT, SMA, EM, and EA: conceptualization, data curation, and methodology. TT, AA, BTT, SMA, EM, and EA: formal analysis and investigation. SMA, EM, and EA: funding acquisition, EA, and project administration. TT: drafted an original manuscript. TT, AA, BTT, SMA, EM, and EA: writing; review and editing. All authors approved of the final version of the article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The data collection work of this study was funded by the European and Developing Countries Clinical Trials Partnership (EDCTP) 2 program through pharmacovigilance infrastructure and post-marketing surveillance system capacity building for regional medicine regulatory harmonization in East Africa (PROFORMA; Grant number CSA2016S-1618) and PrazOpt (Grant number TMA2018CDF-2345) projects.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
All the required supplementary material can be supplied by the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.