
Abstract
Background:
Ethiopia is a country with a high endemicity of the hepatitis B virus, and the primary mode of transmission for this virus is mother-to-child transmission. However, the country lacks a comprehensive plan for viral hepatitis surveillance, prevention, and control.
Objectives:
To assess the knowledge, attitudes, and practices toward preventing and controlling hepatitis B virus infection among pregnant women attending antenatal care at a University Hospital in Central Ethiopia.
Design:
A hospital-based cross-sectional study was conducted among pregnant women from October to November 2023 at a University Hospital in Central Ethiopia.
Methods:
A total of 412 pregnant women were selected and included in the study using a systematic random sampling technique. An interviewer-administered questionnaire was used to collect the data. The collected data were imported into Epi-data version 3.1 and then exported to the Statistical Package for Social Sciences version 25 for analysis. In the bivariate analysis, variables with a p-value less than 0.25 were included in the multivariate analysis. A logistic regression model was used. A p-value <0.05 indicated statistical significance.
Results:
The overall response rate was 94.1%. Of the total 412 respondents, 37.6% exhibited good practices. Notably, pregnant women within the age categories of 29–39 years (adjusted odds ratio (AOR): 0.31; 95% confidence interval (CI): 0.15, 0.64) and ⩾40 years (AOR: 0.17; 95% CI: 0.06, 0.50), residing in rural areas (AOR: 0.35; 95% CI: 0.17, 0.70), with smaller family sizes (AOR: 0.13; 95% CI: 0.07, 0.25), lacking information about hepatitis B virus infection (AOR: 5.15; 95% CI: 2.91, 9.13), having a positive attitude (AOR: 0.03; 95% CI: 0.02, 0.06), and possessing good knowledge (AOR: 0.38; 95% CI: 0.20, 0.71) were significantly associated with poor practice.
Conclusion:
This study revealed that pregnant women had a low level of knowledge, attitudes, and practices related to hepatitis B virus infection prevention and control. A greater understanding is necessary to effectively prevent and control the spread of infection through prioritized health education programs targeting pregnant women. These programs must focus on raising awareness through campaigns that promote knowledge and immunization for their children.
Introduction
Hepatitis is a medical condition characterized by liver inflammation.1,2 The liver is essential for processing nutrients, filtering the blood, and combating infections. 2 Numerous virus families can impact this process. 3 Hepatitis B virus (HBV) infection is a significant global public health concern, affecting an estimated 2 billion individuals worldwide. This infectious disease poses a risk of acute and chronic conditions because it affects the liver.4–7 Globally, it affects one out of every 15 people. 7
Its prevalence is high, predominantly in resource-limited countries. 8 This disease is more common and is responsible for millions of people in Africa.1,4 Its prevalence in sub-Saharan Africa (SSA) ranges from 9% to 20%. The prevalence in the general population is estimated to be between 5% and 30%, while among pregnant women, the prevalence is approximately 9.4%.7,9,10
In Ethiopia, HBV has remained a significant public health problem, with an estimated incidence of 8%–12%.11,12 The country lacks a comprehensive plan for viral hepatitis surveillance and has no periodic national surveys,13,14 with insufficient infection prevention and control strategies.15,16 The country is developing an elimination strategy and implementing various interventions to halt transmission while caring for and treating hepatitis patients.17,18
Mother-to-child transmission of HBV infection is the primary mode of transmission in Ethiopia, accounting for 35%–50% of HBV carriers.19–22 The process of perinatal transmission, which occurs when infected women give birth to their newborns, can adversely affect the cognitive and physical development of future children. 23 The virus can survive outside the body for more than 7 days. 7
Contact with infected body fluids, such as blood, saliva, semen or vaginal fluid, can result in the spread of the virus.4,7 In addition, common routes of HBV transmission include needle stick injuries, circumcisions, tattoos, piercings, intravenous drug use, sharp objects, transfusion of infected blood or blood products, unprotected sexual intercourse, and hemodialysis.24–28 In addition, frequent intercourse, drinking alcohol, and chewing khat are behavioral factors that can increase the risk of transmission. 27
Globally, 90% of cases of HBV transmission are transmitted from mother to child and occur predominantly in SSA countries. 8 All member states support the World Health Organization (WHO). The WHO is a global hepatitis strategy that attempts to treat 80% of patients with these disorders and reduce new hepatitis infections by 90% and deaths by 65% between 2016 and 2030. 29 However, global progress toward reaching elimination goals has been slow, particularly in SSA, where the burden of HBV is high. 30
Preventing mother-to-child transmission (MTCT) of HBV to halt its spread necessitates enhanced screening, disease awareness, and timely vaccination. 8 Ethiopian infants receive the pentavalent HBV vaccine, which is usually available in most hospitals and healthcare facilities. However, only a few private clinics nationwide offer adult HBV immunization. 4 Nonetheless, coverage challenges are still prevalent in numerous regions of Ethiopia. 8
Very little is known about the practices, attitudes, and knowledge regarding the prevention and control of HBV infection in pregnant women in Ethiopia. 6 Most studies have been conducted on medical and health science students31–33 and healthcare professionals.34,3 Pregnant women, therefore, require more screening and education about their condition. However, in the study setup, there is no research on knowledge, attitudes, and practices (KAP) related to preventing and controlling HBV infection among pregnant women attending antenatal care (ANC). Therefore, this study aimed to assess the KAP toward preventing and controlling HBV infection among pregnant women attending ANC at a University Hospital in Central Ethiopia.
Methods and materials
Study design, area, and period
This cross-sectional study was conducted in a University Hospital from October to November 2023. The town is 232 km from Addis Ababa, the capital city of Ethiopia. 35 The total population of the town is 112,860, with 55,933 (49.56%) men, 56,927 (50.44%) women, 13,264 (23.3%) women of childbearing age, 3905 (3.46%) pregnant women, and 17,606 (15.6%) children under 5 years of age. The hospital provides various services, including an operating room, ANC, an intensive care unit, different wards, and inpatient and outpatient departments. It has 300 beds and serves as a center of excellence for training undergraduate and postgraduate students in health-related disciplines. The outpatient service includes a hospital pharmacy, general ambulatory care, an emergency department, and antiretroviral therapy clinics for the community. 36
Sample size determination
Using the single population proportion formula, the sample size was determined with the following considerations: P = 10.4% (where P represents the prevalence study conducted among pregnant women to assess their knowledge in tertiary hospitals in the Amhara Region, northwestern Ethiopia, to maximize the sample size), 5 Z1-α/2 = 1.96 (where Z1-α/2 refers to the critical value at a 95% confidence level), d = 3% (indicating the margin of error), and a 10% nonresponse rate. The intended sample size was n = (1.96) 2 0.104 (1 − 0.104)/(0.03)2 = 398. Finally, considering a 10% nonresponse rate during the study, the total sample size was 438 (n = 398 +10% of 398, which was 40).
Sampling procedure
Considering that the ANC clinic at a University Hospital receives an average of 20 pregnant women per day and that the data collection period was scheduled for one month, 438 pregnant women were chosen using a systematic random sampling technique with a skip interval of every “ninth.” As a result, pregnant women aged 18–49 were interviewed.
Population
The study population included pregnant women in their second and third trimesters who visited the ANC clinic at a University Hospital during the study period. The study unit comprised all selected and sampled pregnant women from a University Hospital during the study period.
Inclusion and exclusion criteria
Pregnant women in their second and third trimesters, aged 18–49 years, with confirmed pregnancy through clinical history and obstetric ultrasound scan examination, and who did not have any medical or obstetric disorders, were eligible to participate in the study. Exclusions consisted of pregnant women who had not yet attended any antenatal visits, were attending their first antenatal visit, or were experiencing severe illness and unable to communicate effectively.
Measurement of variables
This study assessed KAP regarding the prevention and control of HBV infection among pregnant women attending ANC. The primary dependent variable in this study was practices, but knowledge and attitudes toward preventing and controlling HBV infection among pregnant women were also considered secondary dependent variables. Knowledge: This study assessed pregnant women’s knowledge through 18 yes-or-no-response questions focused on preventing and controlling HBV infection. A correct response was assigned a value of one, while an incorrect response was assigned a value of zero. The scores for each item were tallied, and those who scored higher than or equal to 11 out of 18 yes-or-no questions were classified as having good knowledge, while those who scored lower were classified as having poor knowledge.4–6
Attitude
This study evaluated respondents’ attitudes regarding preventing and controlling HBV infection among pregnant women. The final score was determined by 14 yes-or-no questions focused on preventing and controlling HBV infection. Each correct response received a score of 1, while each incorrect response received a score of 0. The scores of all the questions were added together, and respondents who scored nine or more out of the 14 questions were categorized as having a positive attitude. In contrast, those who scored lower than or equal to nine points were categorized as having a negative attitude.4–6
Practice
The assessment of pregnant women’s practices in preventing and controlling HBV was conducted using a set of up to 10 yes-or-no questions. A score greater than or equal to 6 out of 10 was categorized as good practice, whereas a score less than six was categorized as poor practice.4–6
Household income/wealth index
Utilizing principal component analysis (PCA), the household’s wealth index and income level were examined. Factor extraction was performed using PCA with varimax rotation. The suitability of the PCA was assessed using the Kaiser–Meyer–Olkin (KMO) measure of sampling adequacy, which is greater than 0.5 for individuals and the entire collection of items. Finally, households are divided into five wealth quintiles by the Demographic and Health Surveys wealth index: lowest, poor, medium, rich, and richest. 37
Data collection and quality assurance procedures
The data were collected using an interviewer-administered questionnaire. The questionnaire contains questions developed and adapted from various types of literature.4–8 The necessary permission was obtained from the owner of the original questionnaire. The questionnaire developed by the investigators contained the following four sections: (1) basic demographic characteristics (age, residence, marital status, educational status, occupational status, religion, family size, ethnicity, sources of information on HBV, and household income/wealth index of households of pregnant women for preventing and controlling HBV infection); (2) knowledge; (3) attitude; and (4) practice-related factors related to HBV infection prevention and control in pregnant women. The questionnaire was written in English, translated into Amharic, the common language in Ethiopia, and translated back to English by another person who can speak both languages to ensure consistency. To ensure consistency, the questionnaire was pretested on a sample size of 5% (n = 22) at Worabe University Comprehensive Specialized Hospital, Silte, Ethiopia. Two trained supervisors checked the data’s validity and completeness daily. The reliability of the data collection tool was evaluated in terms of knowledge, attitudes, and practice-related items on the questionnaires. To ensure the quality of the data, emphasis was placed on the design of the data collection instrument for its simplicity. Standardized community rating scales, validity, and reliability were considered.
Data processing and analysis
Epi-Data version 3.1 was utilized to input the coded data, which were subsequently exported to the Statistical Package for Social Sciences (SPSS) version 25 for analysis. The data were entered under the purview of the principal investigator. Tables, graphs, and charts were used to conduct descriptive research, and the results were frequently reported. Variables from the bivariate analysis with p values less than 0.25 were added to the multivariate analysis.
The variables for the multivariable analysis were selected using bivariate analysis. Nonetheless, multivariate statistical significance was tested at the 5% level. Adjusted odds ratios (AORs) and 95% confidence intervals (CIs) were calculated in conjunction with logistic regression to verify the existence and strength of the relationships between the independent and dependent variables. The household’s wealth index and income level were examined by utilizing PCA. The Hosmer and Lemeshow test was used to evaluate the model’s fitness; the results showed that the knowledge, attitude, and practice-related predictor variables had values of 0.515, 0.116, and 0.138, respectively. The variance inflation factor was used to determine whether there was any multicollinearity among the independently associated variables; it should be less than 2.173.
Results
Sociodemographic characteristics of the study respondents
Of the 438 eligible pregnant women who participated in the study, 26 were excluded (26 datasets were incomplete and were not considered for analysis), resulting in a response rate of 94.1%. Out of the 412 pregnant women included in the study, all 412 (100%) were married, and nearly two-thirds of the respondents, 252 (61.2%), were aged 18–28 years. The study respondents’ ages varied from 18 to 49 years, with pregnant women’s mean age being 29 years and their standard deviation being ±7.98 years. Nearly three-fourths, 297 (72.1%), of the respondents identified as Protestant in religion, while 337 (81.5%) resided in urban areas (Table 1).
Sociodemographic-related characteristics of the study respondents toward preventing and controlling hepatitis B virus infection among pregnant women attending antenatal care at a University Hospital in Central Ethiopia, 2023 (n = 412).

ETB, Ethiopian Birr; HBV, hepatitis B virus; TV, Television.
Knowledge of pregnant women toward preventing and controlling HBV infection
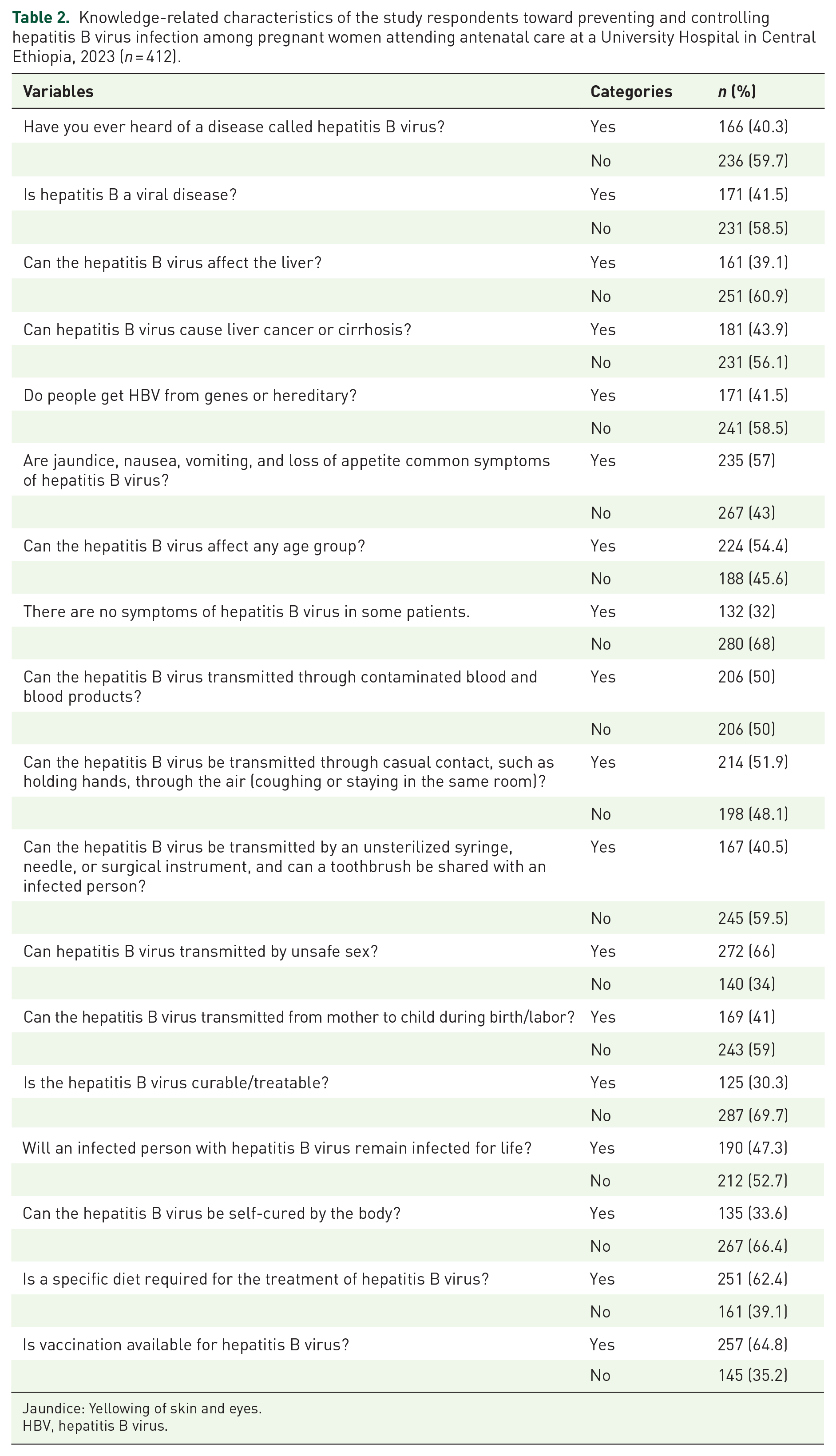
Of the 412 study respondents, one-quarter, 103 (25%), exhibited strong knowledge, with a mean of 8.3544 and a standard deviation of ±3.02072 (95% CI: 20.6, 29.4) (Figure 1). Nearly 166 (40.3%) of the respondents were aware of HBV, a viral disease. Additionally, 161 (39.1%) knew that HBV affects the liver. Furthermore, 181 (43.9%) patients were aware that HBV could lead to liver cancer or cirrhosis (Table 2).

Knowledge-related characteristics of the study respondents toward preventing and controlling hepatitis B virus infection among pregnant women attending antenatal care at a University Hospital in Central Ethiopia, 2023 (n = 412).
Knowledge-related characteristics of the study respondents toward preventing and controlling hepatitis B virus infection among pregnant women attending antenatal care at a University Hospital in Central Ethiopia, 2023 (n = 412).
Jaundice: Yellowing of skin and eyes.
HBV, hepatitis B virus.
Attitudes of pregnant women toward preventing and controlling HBV infection
Of the 412 study respondents, 180 (43.7%) with a (95% CI: 39.6, 49.2) had positive attitudes, with a mean of 6.9733 and a standard deviation of ±4.41869 (Figure 2). More than a quarter, 140 (34%), of the women who responded expressed the belief that they had never thought they could get HBV. The majority, 327 (79.4%), of the respondent women stated that they would inform others if they were diagnosed with HBV. Additionally, out of the total respondents, 226 (54.9%) of the surveyed women preferred seeking treatment at a healthcare facility until there was no improvement in the signs and symptoms of HBV infection. Less than half, specifically 175 (42.5%) of the respondent women, sought medical attention at a health facility after experiencing symptoms for a month. Furthermore, only 276 (67%) of these women reported consulting physicians. Similarly, 215 (52.2%) of the respondents expressed the need for HBV vaccination. Moreover, less than half, 182 (44.2%), of the respondent women believed that children under 2 years of age should be vaccinated. Additionally, 207 (50.2%) of the respondents were willing to return to the clinic after birth for HBV screening. Less than half (170, 41.3%) of the respondent women knew where to obtain HBV immunizations. Conversely, 256 (62.1%) of the respondent women believed that vaccinations could be obtained for free or at a reduced cost. The majority, 162 (87.9%), of the respondent women expressed the need for HBV vaccinations. Furthermore, 207 (50.2%) respondents were willing to undergo HBV screening. Less than half, 182 (44.2%), of the respondents were aware of the availability of laboratory tests for HBV. However, 214 (51.9%) widespread misconceptions were identified regarding treating HBV with antibodies in the case of an HBV infection in infants (Table 3).

Attitude-related characteristics of the study respondents toward preventing and controlling hepatitis B virus infection among pregnant women attending antenatal care at a University Hospital in Central Ethiopia, 2023 (n = 412).
Attitude-related characteristics of the study respondents toward preventing and controlling hepatitis B virus infection among pregnant women attending antenatal care at a University Hospital in Central Ethiopia, 2023 (n = 412).

3 Sadness, 2 Shame. **30 if you know you have been exposed to HBV.
HBV, hepatitis B virus.
The study respondents were worried about preventing and controlling HBV infection among pregnant women attending ANC at a University Hospital in Central Ethiopia (Figure 3).

Worries of the study respondents toward preventing and controlling hepatitis B virus infection among pregnant women attending antenatal care at a University Hospital in Central Ethiopia, 2023 (n = 412).
Practice of pregnant women in preventing and controlling HBV infection
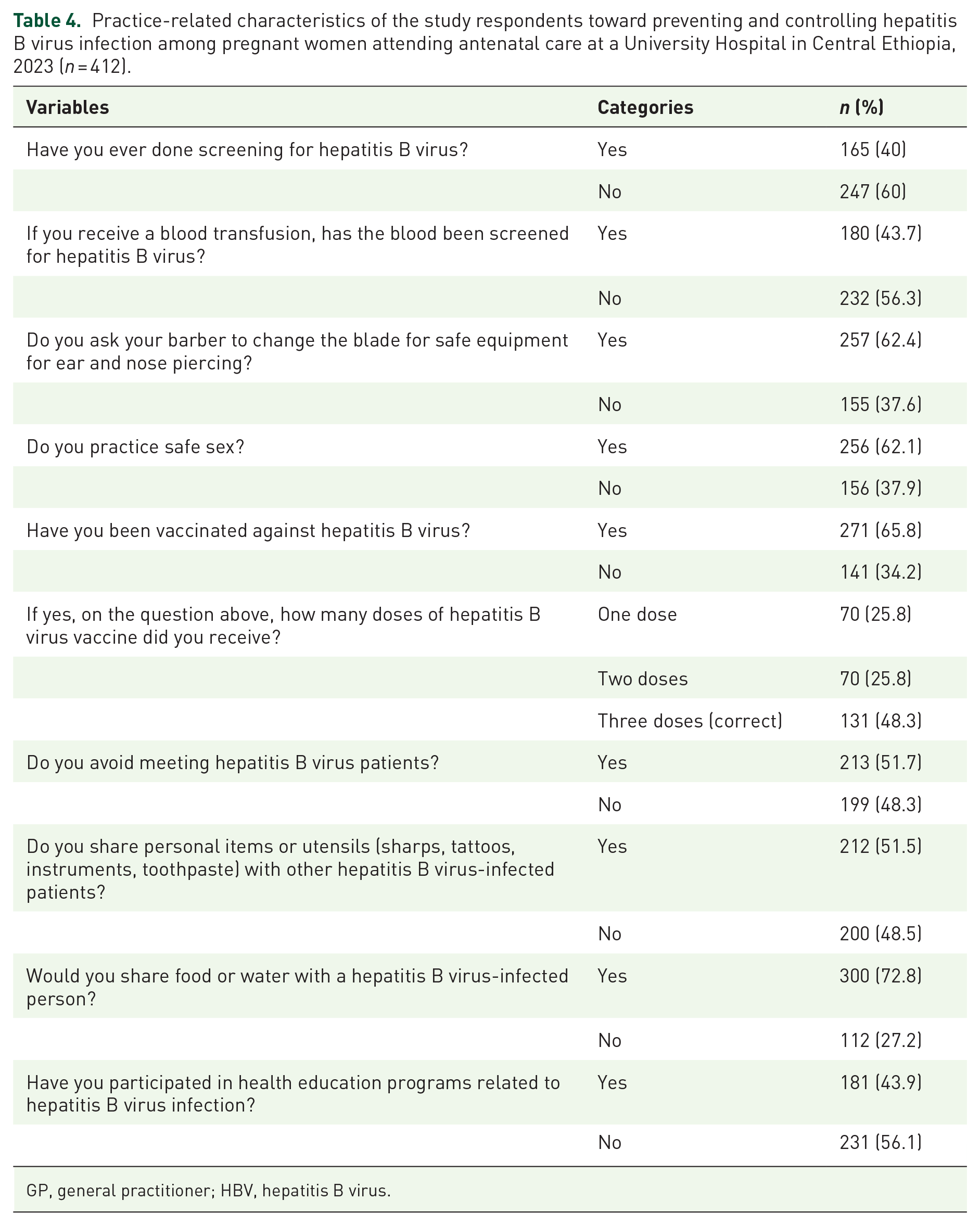
Of the 412 study respondents, 155 (37.6%) with a (95% CI: 32.8, 42.2) had good practices, with a mean of 5.1092 and a standard deviation of ±2.15804 (Figure 4). Less than half, 165 (40%) of the respondent women, had ever undergone screening for HBV. Two-thirds, 257 (62.4%) of the respondent women, asked the barber to change the ear and nose-piercing blades. A total of 256 (62.1%) of the respondent women practiced safe sex, and 271 (65.8%) of the respondent women were vaccinated against HBV. Almost half (131, 48.3%) of the respondents had taken three doses of the HBV vaccine. Three-fourths of the respondents (300, 72.8%) shared food or water with a person infected with HBV. Almost half, 213 (51.7%) of the respondent women, avoided meeting with HBV patients. In comparison, 212 (51.5%) of the respondent women shared personal information or utensils (sharps, tattoos, instruments, and toothpaste) with another person infected with HBV. Less than half, 181 (43.9%) of the respondent women, had participated in health education programs related to HBV infection (Table 4).

Practice-related characteristics of the study respondents toward preventing and controlling hepatitis B virus infection among pregnant women attending antenatal care at a University Hospital in Central Ethiopia, 2023 (n = 412).
Practice-related characteristics of the study respondents toward preventing and controlling hepatitis B virus infection among pregnant women attending antenatal care at a University Hospital in Central Ethiopia, 2023 (n = 412).
GP, general practitioner; HBV, hepatitis B virus.
Factors associated with the KAP of pregnant women toward preventing and controlling HBV infection
Factors associated with the knowledge of pregnant women regarding the prevention and control of HBV infection
We employed multivariable analysis to account for potential confounders. Our findings indicate that having a rural residence, having a small or large family size, lacking information about HBV infection, and having a medium household income were significantly associated with poor knowledge among pregnant women regarding HBV infection prevention and control, with p values < 0.05 (Table 5).
Factors associated with pregnant women’s knowledge toward preventing and controlling HBV infection while attending antenatal care at a University Hospital in Central Ethiopia, 2023 (n = 412).

Variable significance at a p-value < 0.05 in the multivariate analysis.
AOR, adjusted odds ratio, COR, crude odds ratio, HBV, hepatitis B virus, 1 is the reference.
Factors associated with the attitudes of pregnant women toward preventing and controlling HBV infection
Rural residence, small or large family size, and lacking information about HBV infection were significantly associated with negative attitudes toward preventing and controlling HBV infection, with a p-value < 0.05 (Table 6).
Factors associated with the attitudes of pregnant women toward preventing and controlling HBV infection attending antenatal care at a University Hospital in Central Ethiopia, 2023 (n = 412).

Variable significance at a p-value < 0.05 in the multivariate analysis.
AOR, adjusted odds ratio, COR, crude odds ratio, HBV, hepatitis B virus, 1 is the reference.
Factors associated with practices of pregnant women toward preventing and controlling HBV infection
Pregnant women aged 29–39 years and ⩾40 years, residing in a rural residence, having a small family size, lacking information about HBV infection, having a positive attitude, and possessing good knowledge were identified as having a significant correlation with poor practices concerning the prevention and control of HBV infection, with a p-value < 0.05 (Table 7).
Factors associated with the practices of pregnant women in preventing and controlling HBV infection by attending antenatal care at a University Hospital in Central Ethiopia, 2023 (n = 412).

Variable significance at a p-value < 0.05 in the multivariate analysis.
AOR, adjusted odds ratio, COR, crude odds ratio, HBV, hepatitis B virus, 1 is the reference.
Discussion
This research aimed to assess pregnant women’s KAP regarding the prevention and control of HBV infection at the ANC clinic of a University Hospital in Central Ethiopia. Pregnant women living with HBV can transmit the virus to both the general population and their unborn children. 38 Inadequate knowledge may influence pregnant women’s attitudes and practices concerning the risk of HBV infection for both the public and their unborn children. 6
The findings of our study revealed that only 25% of pregnant women had good knowledge about preventing and controlling HBV infection. This finding was greater than those of studies conducted in the Amhara Region, Northwest Ethiopia, 5 Guangdong Province, China, 39 Buea Health District, Cameroon, 40 and Ningo-Prampram District, Ghana. 41 However, this number was lower than that reported in studies conducted at the University of Gondar Comprehensive Specialized Hospital in Northwest Ethiopia, 6 Benha University Hospital, 7 Eastern Ghana, 42 Aden Hospital in Hargeisa, Somaliland, 4 Arua Regional Referral Hospital in Arua, Uganda, 43 and Kumasi, the capital city of Ghana, 44 Addis Ababa, Ethiopia, 45 and the West Region of Ghana. 46
Additionally, this study indicated that pregnant women have poor knowledge about HBV transmission from mother to child, transmission mechanisms, and preventive measures. This knowledge gap can lead to a greater incidence of MTCT of HBV, complicating efforts to prevent and eliminate HBV in the Ethiopian context. One reason for this limited understanding could be the lower education level among the study participants, with fewer than half (201, 48.8%) having completed primary and secondary education. Additionally, the lack of awareness may stem from insufficient initiatives targeting HBV infection and its impact on mothers and children, as well as a lack of guidance from healthcare providers on HBV during pregnancy.
The study’s findings emphasize the need for more knowledge regarding HBV prevention and control among the surveyed women, who would benefit from additional education on various aspects of the virus, including its origin, symptoms, transmission, management, and prevention. Specifically, 236 (59.7%) pregnant women were unaware of HBV, 251 (60.9%) lacked knowledge about its impact on the liver, and 245 (59.5%) did not know that HBV could be transmitted via unsterilized syringes, needles, surgical instruments, or sharing a toothbrush with someone who has HBV. 47 Additionally, 243 (59%) were unaware of MTCT during birth or labor. These knowledge gaps can be attributed to inadequate and inconsistent ANC education regarding the different modes of HBV transmission. Therefore, it is essential to prioritize targeted health education and promotion efforts to prevent and control the spread of HBV effectively.
This study revealed that pregnant women in rural areas were 5.85 times more likely to have poor knowledge than those in urban areas (AOR: 5.85; 95% CI: 2.82, 12.14). This finding was in agreement with a study conducted in the Ningo-Prampram District, Ghana, which showed that most pregnant women who demonstrated poor knowledge lived in rural areas 41 but contrasted with a study conducted at Gondar Comprehensive Specialized Hospital, Northwest Ethiopia, 6 which showed that poor knowledge was prevalent among pregnant urban residents. This is not acceptable. This could be because women who lived in urban areas were more likely to have access to resources such as well-stocked libraries, schools, and health facilities. Rural areas also lack access to media such as television and radio that provide information on preventing and controlling HBV infection.
Pregnant women with smaller family sizes had a 2.05-fold greater likelihood of developing poor knowledge about HBV infection prevention and control than did those with medium family sizes (AOR: 2.05; 95% CI: 1.20, 3.50); no studies have reported the relationship between small family size and poor knowledge. The poor knowledge among individuals from smaller families may be attributed to a need for more effective communication concerning the prevention and control of HBV infection within these households, resulting in reduced knowledge of HBV infection among such families. In contrast, pregnant women with a large family size were 75% less likely to have poor knowledge regarding the prevention and control of HBV infection than were those with a medium family size (AOR: 0.25; 95% CI: 0.06, 0.71). This observation could be attributed to the increased level of communication within larger family sizes compared to medium-sized families.
Pregnant women who lacked information about HBV infection were 3.57 times more likely to have poor knowledge than those who were well informed about HBV infection (AOR: 3.57; 95% CI: 2.11, 6.06). This finding contrasted with a study conducted in the Tigray Region, Northern Ethiopia, where 16.4% of respondents were unaware of their HBV status. 38 This knowledge gap may be attributed to a need for more comprehensive information regarding HBV infection prevention and control, the growing prevalence of HBV infection in our country, and the imperative to strengthen prevention and monitoring measures for HBV infection in alignment with national health policy.
Pregnant women with a medium household income had a 2.14 times greater likelihood of having poor knowledge of the prevention and control of HBV infection than those with a low household income (AOR: 2.14; 95% CI: 1.18, 3.89). This finding contradicts a study conducted in tertiary hospitals in the Amhara Region, Northwest Ethiopia, 5 and Gondar Comprehensive Specialized Hospital, Northwest Ethiopia. 6 These could be women from households with moderate income who may engage in risky behaviors such as alcohol consumption, chewing khats, and cigarette smoking. These behaviors have been associated with unsafe sex, acts of violence, and impaired decision-making.48–50 Compared with women from low-income households, those from moderate-income households may be more prone to experiencing heightened sexual and physical violence. 51 These factors collectively place pregnant women at risk of HBV infection.
The findings revealed that only 43.7% of pregnant women had a positive attitude toward preventing and controlling HBV infection. This finding was lower than those of studies conducted at the University of Gondar Comprehensive Specialized Hospital in Northwest Ethiopia, 6 the Amhara Region in Northwest Ethiopia, 5 the Kumasi metropolis in Ghana, 44 and the Guangdong Province in China. 39 However, this finding was consistent with that of a study conducted at Aden Hospital in Hargeisa, Somaliland. 4
This study revealed that negative attitudes among pregnant women may be attributable to a prevailing trend. Approximately 272 (66%) respondents indicated that they had never considered contracting HBV. Moreover, 85 (20.6%) of the respondents expressed reluctance to disclose their HBV diagnosis to others. Additionally, 245 (59.5%) of the respondents were unaware of the recommended age for vaccination, and 242 (58.7%) needed to be made aware of the locations where HBV immunizations are available. Another concerning finding is that 230 (55.8%) of the respondents needed to perform laboratory tests for HBV. All of these factors can facilitate disease transmission.
The disparity in attitudes toward preventing and controlling HBV infection among pregnant women may be due to variations in knowledge and practices among those who received ANC clinic services at hospitals. This may be a result of decreasing awareness about HBV infection, which can lead to negative attitudes. Additionally, this discrepancy may be attributed to differences in study locations, low socioeconomic status, and challenges communicating with physicians. Notably, 276 (67%) of the respondents in the study sought medical consultation only when they were infected, likely due to limited healthcare access, insufficient availability of health facilities, and a low level of education.
The findings revealed that only 37.6% of pregnant women had positive practices for preventing and controlling HBV infection. This finding was greater than that of studies conducted at the University of Gondar Comprehensive Specialized Hospital in Northwest Ethiopia, 6 Aden Hospital in Hargeisa, Somaliland, 4 and Bangladesh. 52 However, this value was lower than that reported in studies conducted in Kumasi metropolis, Ghana, 44 and Addis Ababa, Ethiopia. 45
This inconsistency can be attributed to various factors, including limited accessibility to healthcare services, a lack of awareness about the importance of HBV screening for prevention and control, and the educational background of the women surveyed. The findings of this study are concerning, as they indicate a lack of adherence to HBV-related practices among the survey respondents. A total of 232 (56.3%) of the women had yet to undergo HBV screening before transfusion. Additionally, 212 (51.5%) reported sharing personal items or utensils, such as sharps, tattoos, instruments, and toothpaste, with others. Furthermore, 231 (56.1%) participants had not participated in health education programs on HBV infection. 47
In this study, pregnant women between the ages of 29 and 39 years had a significantly lower likelihood (AOR: 0.31; 95% CI: 0.15, 0.64) of developing poor practices in the prevention and control of HBV infection than those between the ages of 18 and 28 years. Furthermore, respondents who were women aged 40 years and older were also found to be 83% less likely (AOR: 0.17; 95% CI: 0.06, 0.50) to develop poor practices in the prevention and control of HBV infection. This might be because as age increases, pregnant women’s awareness of the prevention and control of HBV infection increases.
Pregnant women residing in rural areas exhibited significantly lower rates of negative attitudes (AOR: 0.12; 95% CI: 0.06, 0.26). This finding was in contrast with a previous study conducted in the Amhara Region, Northwest Ethiopia 5 ; similarly, pregnant women residing in rural areas exhibited significantly lower rates of poor practices (AOR: 0.35; 95% CI: 0.17, 0.70). This finding agreed with a previous study at the University of Gondar Comprehensive Specialized Hospital, Northwest Ethiopia. 6
For pregnant women with smaller family sizes (AOR: 0.52; 95% CI: 0.33, 0.84), no studies were to be reported, and the majority, 93.9% of respondent women, did not tell others if they had HBV, and having a large family size (AOR: 0.32; 95% CI: 0.15, 0.67), exhibited markedly reduced rates of negative attitudes. Compared with families of medium size, families of smaller sizes were poorly practiced (AOR: 0.13; 95% CI: 0.07, 0.25) at preventing and controlling HBV infection; however, no studies have supported these findings. This could result from the lower viral transmission rates observed among medium-sized families of HBV-infected patients.
Pregnant women who lack information about HBV infection demonstrate significantly greater rates of negative attitudes (AOR: 1.78; 95% CI: 1.09, 2.91) and poor practices (AOR: 5.15; 95% CI: 2.91, 9.13) in the prevention and control of HBV infection than those who are knowledgeable about HBV infection. The lack of awareness could be attributed to insufficient information on HBV infection, the increasing prevalence of HBV infection in our country, and the absence of preventive measures and monitoring, resulting in increased transmission rates. Moreover, negative attitudes toward prevention and control measures for HBV infection exacerbate this situation. However, no studies have examined the association between pregnant women’s lack of information about HBV infection and their poor practices. This may be because pregnant women who are not well informed about HBV infection are less likely to be aware of effective measures to control and prevent transmission.
Pregnant women with good knowledge were 62% less likely to develop poor HBV infection prevention and control practices than those with poor knowledge (AOR: 0.38; 95% CI: 0.20, 0.71). This result is consistent with research from the University of Gondar Comprehensive Specialized Hospital, Northwest Ethiopia, which reported poor knowledge and limited practices. 6 Pregnant women with a positive attitude were 97% less likely to develop poor HBV infection prevention and control practices than those with a negative attitude (AOR: 0.03; 95% CI: 0.02, 0.06). However, in fact, pregnant women who have good knowledge should have a positive attitude and good practices. This overall discrepancy may be explained by differences in pregnant women’s practices, attitudes, knowledge, and allocation of resources.
Limitations
The study was conducted in a single antenatal clinic, thus limiting the generalizability of the research findings to all pregnant women in the study setting. Additionally, only one risk factor, the study respondent’s gender, was considered. HBsAb tests were not conducted to identify vaccinated or previously exposed women among the respondents. Furthermore, the survey on KAP documents was only carried out on a limited scale among pregnant Ethiopian women.
Conclusion
This study revealed that pregnant women had a low level of KAP related to HBV infection prevention and control. The study revealed significant associations between observed poor practices and factors such as being aged 29–39 years and ⩾40 years, residing in a rural residence, having a small family size, lacking information about HBV infection, having a positive attitude, and possessing good knowledge. Greater understanding is necessary to effectively prevent and control the spread of infection through prioritized health education programs targeting pregnant women. These programs must focus on raising awareness through campaigns that promote knowledge and immunization for their children.
Footnotes
Acknowledgements
We extend our deepest gratitude to the Central University of Tamil Nadu (CUTN) and the Department of Epidemiology and Public Health (EPH) for their invaluable support throughout this research endeavor. Our sincere thanks also go to the Indian government for sponsoring the Indian Council for Cultural Relations Scholarship Program, which played a pivotal role in facilitating this research. We are immensely grateful to the data collectors, supervisors, and staff at Wachemo University Hospital for their indispensable contributions. Finally, we would like to acknowledge the unwavering support and encouragement of our family and friends, whose valuable information and motivation made the completion of this thesis research possible.