
Abstract
Background:
Prostate cancer (PCa) accounts for 21.6% of all cancers among men in Botswana, ranking as the fourth most common cancer (9%) across all age groups. This study aimed to assess the knowledge, attitudes and practices related to PCa screening among men aged 40 years and older in Ramotswa, Botswana.
Design and methods:
A cross-sectional survey was conducted involving a random sample of 362 males aged 40 years and older in Ramotswa. Logistics regression models were utilised to examine associations between socio-demographics, knowledge, attitudes, practices and PCa screening.
Results:
Of the 362 respondents, 105 (29%) men reported having undergone prostate screening tests either prostate-specific antigen (PSA) or digital rectal examination (DRE). Additionally, 221 (61%) had prior knowledge of PCa, with 114 (32%) receiving information from the radio while fewer than 20% learnt about it from health care providers. Single men were found to be 63% less likely to go for screening compared to married men (AOR = 0.37; [95% CI 0.22–0.61]). Men who were not afraid of the screening test results were twice as likely to go for screening compared to those who were afraid of a positive result for prostate test (AOR = 2.14; [95% CI 1.12–4.09]).
Conclusions:
While respondents demonstrated above-average knowledge of PCa, fewer than half had undergone a PSA test. Urgent and targeted interventions are needed to address predisposing factors such as fear of prostate screening. Furthermore, the low rates of PCa information dissemination by healthcare workers underscore the need for enhanced engagement of medical practitioners in educating men about PCa.
Significance of the study
The significance of this study is multifaceted, as it seeks to explore critical issues surrounding prostate cancer screening among men. This study provides valuable insights for policymakers and healthcare workers seeking to improve health outcomes for men at risk of prostate cancer. Understanding men’s knowledge of prostate cancer screening is a crucial determinant for wellness and self-care practices. Assessing men’s attitudes is important in determining if their attitudes are interfering with good health and how the attitudes can be changed. This is crucial for public health intervention that seeks to promote wellness behaviours among men. Furthermore, the study elucidates barriers that may hinder men from engaging in wellness and self-care practices regarding prostate cancer screening, thereby informing interventional programmes aimed at creating enabling factors and a positive cognitive state of men’s control over their wellness behaviours.
Introduction
Prostate cancer (PCa) is one of the most commonly diagnosed cancers and a leading cause of mortality globally in the adult male population. 1 PCa accounts for almost 10 million deaths globally. 2 In 2020, nearly 1.4 million new cases were reported, resulting in approximately 375,000 deaths globally. 1 The incidence and mortality rates of PCa are particularly high among black men, and developing regions such as Latin America, the Caribbean and Africa.3,4 For instance, Africa’s mortality from PCa is projected to rise significantly from around 55,744 deaths in 2022 to an estimated 107,435 cases per 1,044,996,089 annual population by 2040. In contrast, Europe’s mortality expected to increase by 15% over the same period. 5
Currently, prostate cancer constitutes 23% of all cancers in men. 6 PCa develops in the prostate, and the prostate gland is only found in males. 7 The prostate, a gland in the male reproductive system, typically enlarges with age, leading to benign prostatic hyperplasia (BPH), which can mimic prostate cancer symptoms.7,8 The median age of PCa presentation is 68 years 9 and while PCa is rare in men under 50, incidence among young men (<55) has risen notably from 5.6 to 32 cases per 100,000 between 1986 and 2008. Consequently, it is advised that black men aged 40 years and older consider undergoing screening for PCa.10 –12
PCa is often asymptomatic in its early stages, making it easily overlooked without proper screening. Therefore, men must undergo screening as early as 40 years of age.13,14 Early detection is crucial in preventing advanced disease, as highlighted by Anakwenze et al. 15 in their study from Botswana, which explored factors that lead to advanced cancer presentation.
Men who are informed about prostate health are more likely to participate in screening. 16 There are two primary screening methods for PCa: the measurement of serum prostate-specific antigen (PSA) and the digital rectal examination (DRE). PSA is a protein produced by both normal and cancerous prostate cells; an elevated PSA levels may suggest prostate issues, although it does not necessarily confirm cancer. DRE involves a healthcare provider assessing the prostate through the rectum to evaluate its condition. 17 These screening tests aim to enhance quality of life by reducing morbidity and mortality, providing an opportunity for early treatment. 18
Risk factors for PCa include genetic predisposition, high dihydrotestosterone (DHT), levels, ethnicity, obesity, lifestyle choices, diabetes and poor nutrition. 16 In Botswana, PCa represents 22% of all cancers diagnosed in men and accounts for 9% of all cancers across all age groups. 2 Additionally, PCa contributes to 8% of all cancer-related deaths in the country. A study done several years ago showed that many patients in Botswana, including those with prostate cancer, present with advanced disease, resulting in over a 70% 19 mortality rate among cancer patients. Another study done in Botswana revealed that men face a heightened risk of advanced cancers due to delays in diagnosis and treatment, misdiagnosis, system barriers, understaffed facilities and poor referral communication.20,21
In Sub-Saharan Africa, low education levels contribute to a lack of understanding about prostate cancer, resulting in mistrust of prostate cancer screening processes. 22 Currently, knowledge, attitudes and screening behaviour regarding prostate cancer among adult males in Botswana remain unstudied. 23 Assessing men’s knowledge, practice and attitudes towards PCa screening among at-risk men is paramount to improving screening practices, early detection, and prognosis among men. Targeted evidence-based interventions are considered more effective in improving men’s health-seeking behaviours, attitudes and knowledge. 24 Therefore, this study aimed to assess the knowledge, attitudes, and practices of males aged 40 years and above in Ramotswa regarding PCa screening.
Methods and materials
Study design
The study employed a cross-sectional study design. Structured self-administered questionnaires were used to collect data on knowledge, attitudes and practices regarding PCa screening from a sample of men in Ramotswa, Botswana, between January and March 2023.
Study site and setting
This study was conducted in Ramotswa, an urban village located 32 km from Gaborone, the capital city of Botswana. Ramotswa is found in the South-East District of Botswana, and has an estimated population of 33,271, according to the 2022 census. 25
Study population, inclusion and exclusion criteria
All men aged 40 years and older were included in the study.
Measures
The questionnaire assessed the knowledge, attitude and practice of males aged 40 years and older in Ramotswa, Botswana, regarding PCa screening. The questionnaire was developed by the researchers based on existing literature.26,27 Face validation was performed to ensure that the questionnaire accurately measured the intended variables. This involved pre-testing it with five men from Gaborone who met the inclusion criteria, along with an expert panel of three public health specialists. The assessment focused on ambiguity, readability, clarity, the time required for survey completion and overall flow to ensure the items were appropriate and comprehensible, Reliability analysis of the questionnaire, conducted using Cronbach’s alpha, indicated acceptable internal consistency with scores of 0.79, 0.87 and 0,89 for practices, attitudes, and knowledge, respectively. The questionnaire was initially prepared in Setswana, translated into English and then back translated into Setswana to ensure accuracy and cultural relevance.
The questionnaire comprised four sections: socio-demographic characteristics, knowledge levels, attitudes and practices towards prostate cancer screening. Socio-demographic characteristics were evaluated using four questions: age, marital status, educational status and employment status. Practices towards the PCa screening were assessed with two questions: ‘Have you undergone a prostate-specific antigen test?’ with responses No and Yes; ‘Have you undergone a digital rectal examination test?’ with responses No and Yes.
Attitudes towards PCa screening were assessed through six questions using a 4-point Likert scale ranging from 1 (strongly agree,) to 4 (strongly disagree). Examples of some of the questions included ‘I believe men who have PCa screening will have more problems than men who do not go for screening’ and ‘I am bothered by the possibility that Digital Rectal Examination might be physically uncomfortable’.
Knowledge was assessed by asking respondents about their awareness of prostate cancer. Their familiarity with PCa screening, the source of their knowledge and their ability to accurately identify risk factors associated with PCa.
Sample size and sampling method
The sample size was calculated using a single proportion formula, considering a 95% confidence interval and a 5% margin of error. No previous studies were conducted in Botswana to establish the proportion of men who had been screened for PCa, and the population size of men aged 40 years and older was unknown; we used the Cochran formula
28
to ensure that the sample is a true representation of the entire population. This was calculated using the equation,
A multi-stage sampling technique was employed to select research participants. The first stage involved random selection of 4 of the 16 wards in Ramotswa using a lottery sampling technique. In the second stage three minor wards were chosen from each of the four selected wards. The third stage involved selecting every third house using systematic random sampling from the three selected minor wards. A household was randomly selected from multi-residential properties for each identified residential area. From each selected household, a male participant aged 40 years and older who consented to participate was chosen.
Data analysis
Data were entered and analysed using SPSS version 28. Binary Logistic regression models were employed to predict PCa screening test and socio-demographic characteristics such as age, marital status, educational status, knowledge levels, practices and attitudes. The association between socio-demographic factors and knowledge of prostate cancer was tested using the Pearson Chi-square test, with a p-value of < 5% considered statistically significant. Descriptive statistics including the mean age and standard deviation for age frequencies related to knowledge levels about Pca, are presented in Table 1. We presented crude odd ratios (COR) and adjusted odds ratios (AOR) with their corresponding 95% confidence intervals to estimate the effects of socio-demographic factors mentioned earlier. A p-value of < 5% was considered statistically significant.
Socio-demographic characteristics.

Mean ± standard deviation (range).
Results
Three hundred sixty-two men participated in the study (94% response rate), with an age range of 40–82 years and a mean age of 48 years (standard deviation (SD) = 7.6 years; Table 1). Most of the participants were aged 40–51 years (77%) and were not married 226 (62%). Almost two-fifths (38%) had completed secondary education, while (17%) had primary and no formal education. More than half of the men (68%) were employed.
Table 2 shows that 61% of participants had heard of PCa. Among the men surveyed, over a third (114) learnt about PCa from the radio, whilst (70%) from a doctor. More than three-quarters (278) of respondents believed that PCa is associated with infertility and sexual dysfunction. Possible risk factors for PCa were identified as smoking (76%) followed by sexually transmitted infections (74%) and a high-fat diet (50%).
Men’s knowledge and practices regarding PCa (N = 362).

One hundred five (29%) were tested for prostate cancer, 19% had undergone PSA and 36 (10%) had undergone a DRE, respectively. In addition, over 90% of participants indicated that they intended to be screened in the future (Table 3).
Men’s practices towards prostate cancer (N = 362).

The association between demographic factors and PCa screening is summarized in Table 4. Marital status was the only factor significantly associated with PCa screening. Specifically single men were 63% less likely to go for screening compared to their married counterparts (AOR = 0.37; (95% CI 0.22–0.61)).
Demographic factors and PCa screening (N = 362).
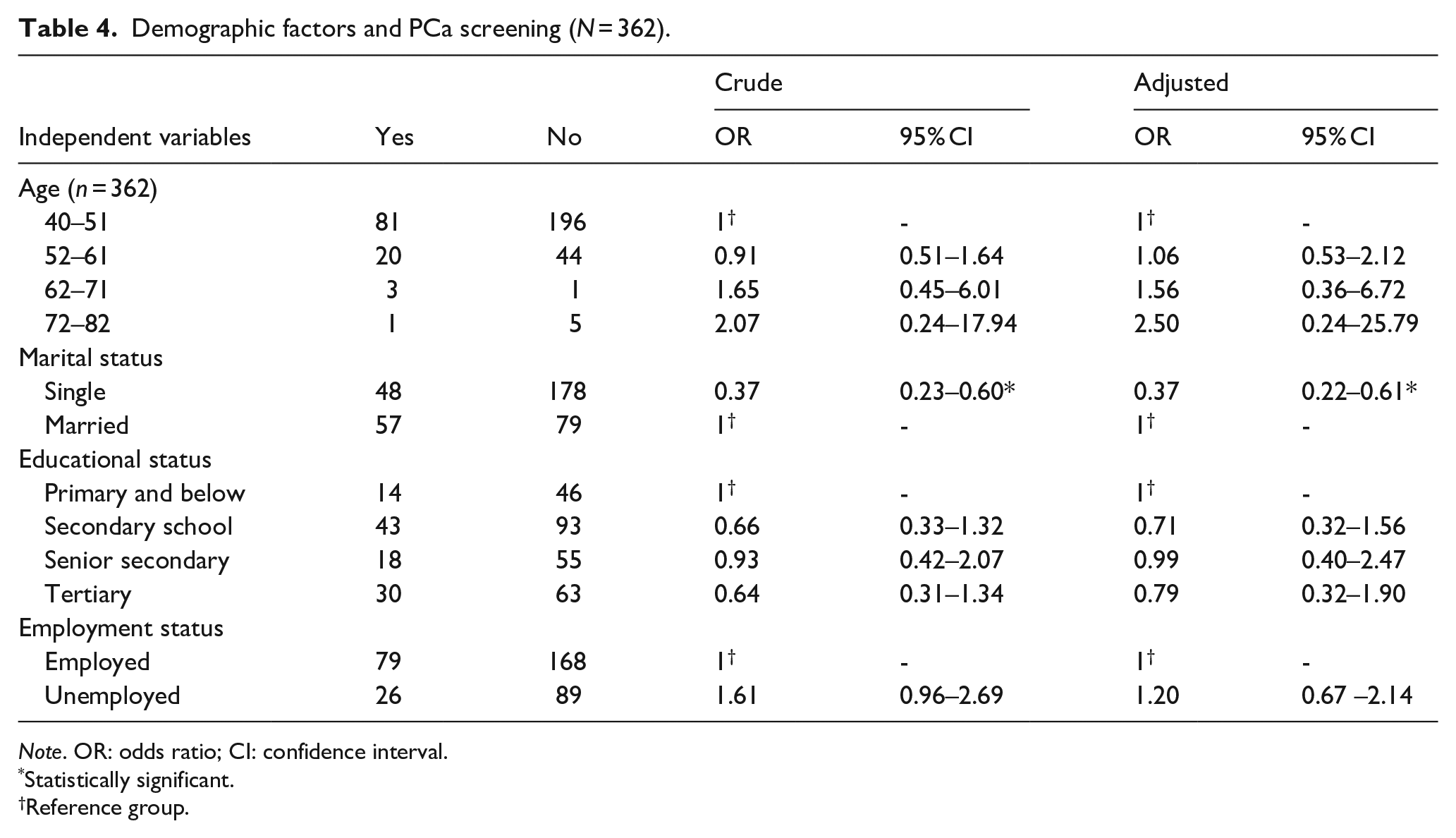
Note. OR: odds ratio; CI: confidence interval.
Statistically significant.
Reference group.
Most men had a positive attitude towards PCa screening with 342 (95%), and more than half having expressed a positive attitude towards the DRE exam (196; 54%; Table 5). However, one hundred forty-seven men (41%) agreed that digital rectal examination was embarrassing. However, 342 (94%) believed having a PCa test was important.
Men’s attitudes towards PCa (N = 362).

The association between attitudes towards PCa and screening is summarised in Table 6. Men not afraid of the prostate screening results were twice as likely to go for screening compared to men who feared that the screening test might be positive (AOR = 2.14; (95% CI 1.12–4.09)).
Attitudes towards PCa and PCa screening (N = 362).

Note. OR: odds ratio; CI: confidence interval.
Statistically significant.
Reference group.
Table 7 shows that participants aged 40–51 years were more knowledgeable about PCa screening than those aged 52 years and older (
Demographic factors and the knowledge of prostate cancer (N = 362).

p < 0.05. **p < 0.001.
Discussion
This study examined men’s knowledge, attitudes and practices regarding PCa screening in Ramotswa, Botswana. Our findings indicated that respondents demonstrated a high level of awareness about prostate cancer compared to similar studies conducted in various regions of Sub-Saharan Africa. The increased knowledge could be attributed to the initiatives by the Men for Health and Gender Justice organisation and the Ministry of Health, which include an annual awareness campaign every November, the provision of free screening services and educational activities at various social gatherings in Botswana. 29 These efforts emphasise the relationship between diet, exercise, hypertension and diabetes in relation to PCa. 30
The findings of our study align closely with a study conducted in Saudi Arabia, where 65% of men reported having heard about prostate cancer. 31 In contrast, a significantly higher percentage, 82%, of men in Italy were aware of PCa. 26 Furthermore, our findings sharply contrast with two separate studies conducted in Limpopo and Free State Province, South Africa, where over 60% of the men reported that they had not heard about PCa.32,33 These disparities underscore the variation in awareness and educational outreach regarding prostate cancer across different regions, highlighting the need for continued efforts to improve awareness and access to information about prostate cancer in areas with lower knowledge levels.
In our study, we found that men primarily learnt about prostate cancer from sources such as the radio, medical doctors, television, the internet, and friends. These findings are consistent with research conducted by Asare and Ackumey in 2021 among men in Ghana. 34 However, our findings differ from those of a study in Saudi Arabia, where social media was identified as the main source of information, followed by the internet, friends/family and healthcare providers among men aged 40 years and older. 31 Additionally, a study from South Africa indicated that family and friends as well as physicians, are the most common sources of information for men in the same age group. 32 In contrast, our study revealed that less than 20% of participants reported information on PCa from medical doctors. These results suggest that in Botswana, radio serves as a significant medium for disseminating health information and promoting the role of healthcare providers, particularly doctors and other healthcare workers, who appear less impactful in raising awareness about PCa. In our study, compared to those in South Africa, this gap highlights the need for healthcare professionals to proactively educate patients about prostate cancer and the importance of screening. It is also important to note that the dynamics of health information dissemination may vary in urban settings. Therefore, further research is necessary to explore awareness and information sources related to prostate cancer among men in urban areas. This would provide a more comprehensive understanding of knowledge and practices regarding prostate cancer screening across different demographics.
In this study, married men were more likely to undergo PCa screening and exhibited greater knowledge about PCa screening compared to unmarried men. This aligns with findings from the PRACTICAL consortium, 35 which highlighted that social support from a spouse could promote health-seeking behaviours. Additionally, a Kenyan study on determinants of PCa screening among men aged 40 and older showed that married and educated men were more likely to go for screening compared to unmarried or uneducated men. 36
Another significant finding in our study was the positive attitudes towards the PSA test, which could influence men’s intentions for screening.24,37 In this study, more than half of the men did not find the DRE embarrassing; this aligns with findings from a study done in Brazil on barriers to prostate cancer screening in which only 26% of men felt ashamed of DRE. 38 Our findings are contrary to a Nigerian study in which 52% of men felt that DRE was embarrassing. 39 In addition, more than half of the men had a positive attitude towards the DRE exam, similar to findings from a study done in Trinidad among men aged 40 years and above. 40 However, our study findings are contrary to studies done in Nigeria. 39 In our study, almost all the respondents believed that it was important to have a PCa screening test, which is encouraging. Similar results were observed in a study in Zambia in which 99% of the men had positive attitudes towards PCa screening. 41
Almost all respondents in this study intended to undergo PCa screening. This finding was higher than those reported in other countries such as Italy, Spain, Nigeria and South Africa, where the intention to go for screening was 60%, 58%, 83% and 68%, respectively.26,32,42,43 These differences may be attributed to increased awareness of PCa and better access to screening services. The high intention of men in Ramotswa to undergo a PSA test is a critical precursor to engaging in preventive health behaviour: screening.44 –46
About a third of men had undergone a PCa test in this study. Similarly, a study in Italy found that 30% of men had received a PCa test. 26 PCa screening among men in most Southern African countries was much lower than our study finding; for example, in Zambia and Tanzania, the percentages of men who had undergone PCa screening were 13% and 17%, respectively.27,41 The region with the least number of men having been screened for PCa was Limpopo province in South Africa, with only 3% because of a lack of awareness about PCa. 32 Although the intention to go for screening was high, not many men were screened, suggesting a lack of reinforcing and enabling factors towards screening behaviour. 47
One limitation of this study is its focus on a single urban village, which may limit the generalisability of the findings to the broader Batswana population. Further research should be conducted in various urban and rural villages across Botswana to gain a more comprehensive understanding.
Fear of PCa screening was prevalent among participants, posing a significant barrier to screening uptake. Future interventions should prioritise addressing these fears by effectively communicating the benefits of early testing and detection. Additionally, exploring the sources of these fears may provide valuable insights for future research.
In conclusion, while men demonstrated above-average knowledge regarding prostate cancer and exhibited positive attitudes towards cancer screening, this did not directly translate into increased participation in PCa screening. Future interventions should focus on addressing predisposing factors, such as inculcating positive attitudes towards health screening behaviours, enhancing knowledge of symptoms and dispelling myths and misconceptions. Additionally, it is critical to facilitate enabling factors such as confidence, availability, accessibility of screening facilities and finally, reinforcements from family and partners of men. These elements can significantly bolster men’s confidence in enganging in healthy seeking behaviours. 24
Footnotes
Acknowledgements
We want to thank the Ministry of Health, Research and Development Division for permitting us to conduct the study. We also want to acknowledge all research participants who participated in our study.
Ethical considerations
Permission was obtained from the Ministry of Health, Health Research and Development Division, to conduct the study (HPRD 6/14/1). Written informed consent was obtained from the men in Ramotswa. The collected data were kept in a password-protected computer and were accessible only to the researcher.
Consent to participate
All study participants provided written consent to participate in the survey.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors received financial support from the Department of Tertiary Education Financing, Ministry of Tertiary Education, Research, Science & Technology, Botswana for data collection, not for authorship and publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.