
Abstract
Background:
The fourth most common cancer in women worldwide is cervical cancer. Over 87% of deaths from cervical cancer occur in developing nations. One of the risks of developing cervical cancer is the use of oral contraceptives. However, there is limited evidence on the knowledge, attitude, and practice of cervical cancer screening among family planning service users in Ethiopia.
Objective:
To assess the knowledge, attitude, and practice toward cervical cancer screening and its associated factors among family planning service users.
Methods:
A facility-based cross-sectional study was conducted from January 1 to February 28, 2023. A total of 816 participants were selected using a systematic sampling technique. Data were collected using a pretested, structured, and interviewer-administered questionnaire. The collected data were entered into EPI Data 3.1 and exported to SPSS version 24 (IBM, Armonk, NY, USA) for analysis. Logistic regression was used to identify risk factors. An odds ratio with a 95% confidence interval and a p-value < 0.05 were used to declare statistical significance.
Results:
Overall, 42.5%, 36.6%, and 20.1% of the participants had good knowledge, a positive attitude, and practiced cervical cancer screening, respectively. Being single (adjusted odds ratio (AOR) = 3.39, 95% confidence intervals: 1.15–6.26), having college or university level of education (AOR = 8.03, 95% confidence intervals: 3.45–19.23), having a family history of cervical cancer (AOR = 3.14, 95% confidence intervals: 1.82–8.84), and having a source of information from the media (AOR = 1.74, 95% confidence intervals: 1.09–2.54) were significantly associated with good knowledge of cervical cancer screening. Women who were aged 15–23 years (AOR = 5.62, 95% confidence intervals: 2.76–14.56), had college- or university-level education (AOR = 3.69, 95% confidence intervals: 1.65–8.22), and had good knowledge of cervical cancer (AOR = 4.71, 95% confidence intervals: 3.08–7.55) were significantly associated with a positive attitude toward cervical cancer screening. An earlier age of first sexual intercourse (AOR = 5.0, 95% confidence intervals: 3.80–9.20) and good knowledge of cervical cancer (AOR = 1.52, 1.21–5.82) were positively associated with good practice of cervical cancer screening. Women who attended high school were negatively associated with good practice in cervical cancer screening (AOR = 0.46, 0.23–0.73).
Conclusion:
Knowledge, attitude, and practice toward cervical cancer screening were low. As a result, during patient visits for care delivery, healthcare providers should inform and educate patients about cervical cancer screening.
Introduction
Cervical cancer is a worldwide public health issue and a chronic noncommunicable disease caused mostly by persistent infection with particular forms of the human papillomavirus (HPV). 1 In all nations throughout the world, HPV strains 16 and 18 are responsible for over 70% of cervical cancer incidences. 2 Multiple sexual partners, young age at first sexual intercourse, young age at first delivery, parity, oral contraceptive pills, smoking, obesity, and genetic sensitivity are all risk factors. 3
Cervical cancer is the fourth most frequent malignancy in women worldwide, with 604,127 new cases and 341,831 deaths reported in 2020. 4 In 2025, the number of new cervical cancer cases and deaths is expected to rise to 720,415 and 394,905, respectively. 5 Because of poor healthcare infrastructure, low- and middle-income countries account for over 85% of new cases and 87% of cervical cancer-related deaths. 6 Eastern Africa has the highest burden, with age-standardized incidence rates of >30 per 100,000 women. 7 Every year, around 6294 new cases and 4884 deaths occur in Ethiopia, making it the second-highest cause of cancer-related death among women after breast cancer. 8 Cervical cancer is becoming more prevalent among women aged 30–65, who account for 79% of cases and 65.8% of annual deaths.8,9
The main problems related to cervical cancer screening were a lack of awareness about the disease process, unsatisfactory pap smear testing, and the client’s negative attitude toward the procedure. Lack of awareness of available screening methods, in addition to a lack of knowledge, can play a significant role in the failure to use cervical cancer screening programs.10,11 Cervical cancer screening is low in sub-Saharan Africa and other developing countries due to low levels of awareness, insufficient knowledge, and clients with inaccessible services. 12
Cervical cancer is a disease that can be prevented and treated, and early detection of precancerous lesions can help lower the disease’s incidence and death rate. The Papanicolaou smear, visual inspection with acetic acid, and HPV testing are the most commonly used screening procedures, with the latter two being reported to be cost-effective in low-resource nations. 13 All women between the ages of 30 and 49 years old should be checked for cervical cancer at least once, according to the World Health Organization. 2
Ethiopia does not have a nationalized, organized cervical cancer screening program, but there is opportunistic screening, which is carried out when a patient requests a checkup or test from their doctor or other healthcare provider or when a doctor or other healthcare provider offers a checkup or test. Primary healthcare centers are located close to people and hence serve the majority of the world’s population. 14 Women of reproductive age use primary healthcare institutions for a variety of reproductive health needs, including prenatal care and contraception. As a result, primary healthcare centers can act as centers for a population-based cervical cancer screening program. One of the risks of developing cervical cancer is the use of oral contraceptives. However, there is limited evidence on the knowledge, attitude, and practice of cervical cancer screening among family planning service users in Ethiopia, particularly in the study area. Thus, this study was conducted in Debre Tabor town health facilities to investigate the knowledge, attitude, and practice of cervical cancer screening and associated risk factors among family planning service users for the prevention and control of cervical cancer.
Materials and methods
Study area
The research was carried out at Debre Tabor town health facilities. Debre Tabor is located 667 kilometers from Addis Ababa, Ethiopia’s capital city, in the South Gondar Zone of Amhara Regional State in North Central Ethiopia. According to the information from the Debre Tabor town administrative bureau, the town had a total population of 87,627 people; among these, 19,898 were in the reproductive age group. There is one hospital, three health centers, and six private clinics in the town. This study included only government-run healthcare facilities: the so-called Debre Tabor Comprehensive Specialized Hospital (DTCSH), Debre Tabor Health Center, Atse Seifeard Health Center, and Luel Alemayehu Health Center. All of the selected health facilities provide family planning services in the town.
Study design, period, and populations
A facility-based cross-sectional study was conducted from January 1 to February 28, 2023. The study population was reproductive-age women who attended family planning at the health facilities.
Eligibility criteria
All reproductive-age women (15–49 years old) who attended family planning at the selected health facilities and volunteered to give informed written consent were included in the study, whereas we excluded women with known mental illness and who were critically ill.
The sample size determination
Sample size was calculated using a single proportion formula with knowledge of cervical cancer screening at 59.3%, taken from the study done in Gondar, Ethiopia,
15
with the assumption of a 95% confidence interval (Z α/2 = 1.96), a margin of error of 5%, and a design effect of 2
Sampling procedure
In the town, family planning services were available in both public and private health facilities. For the purpose of this study, only government-run healthcare facilities were included; these are DTCSH, Debre Tabor Health Center, Atse Seifeard Health Center, and Luel Alemayehu Health Center. Based on the average daily client flow of the units during the preceding three consecutive months, which was determined by reviewing client registration log books, the calculated sample size was proportionally distributed to each healthcare institution. The DTCSH, Debre Tabor, Atse Seifeard, and Luel Alemayehu health centers saw an average monthly client flow of 1000, 700, 500, and 550, respectively. At all four of the health institutions chosen, there were an average of 2750 women sought family planning services each month. Thus, 297, 208, 148, and 163 sample sizes were allocated to DTCSH, Debre Tabor, Ginbot 20, and Luel Alemayehu health centers, respectively. A systematic random sampling approach was used to choose the study’s participants. A lottery method was used to choose the initial participant in each healthcare facility.
Data collection and quality control
Data were collected from each study participant using a pretested, structured, and interviewer-administered questionnaire. It was somewhat modified to fit the goals of this particular study and the local context after being adopted from related literature.1,11,16 The questionnaire is divided into five categories: sociodemographic characteristics, reproductive characteristics, knowledge of cervical cancer screening, attitudes toward cervical cancer screening, and cervical cancer screening practices. The questionnaire was initially written in English, then translated into Amharic, and finally back into English to ensure uniformity. To aid in the data collection procedure, four data collectors with BScs in nursing and two supervisors were engaged. Before beginning the actual data collection, the supervisor and data collectors received training on the methodology and purpose of the study, as well as on ethical issues.
The questionnaire was pretested on 5% (41) of the sample size before the actual data were collected in another health center, called Addis Zemen Health Center, to ensure the correctness and consistency of the questionnaire. Each night after the collection of data, the supervisors and the principal investigator checked over all of the data to make sure they were accurate, clear, and consistent. The data were thoroughly cleansed before analysis, and there was double data entry and validation.
Operational definitions
Knowledge
The participants’ cumulative mean score for knowledge about cervical cancer was determined using the mean score. Accordingly, those who received a score below the mean on the questions related to cervical cancer screening services had poor knowledge, while those who had received a score above or equal to the mean had good knowledge. 11
Attitude
We used a Likert scale for assessing the attitude. Strongly disagree = 1, disagree = 2, neutral = 3, agree = 4, and strongly agree = 5 were the scoring scales that were employed. The responses were added up to get a final score. The mean score was then determined. Women with scores above the mean were thought to have a positive attitude toward cervical cancer screening, whereas those with scores below the mean were considered to have a negative attitude. 1
Practice
Cervical cancer screening was not practiced among respondents who had never undergone the procedure. However, it was determined that individuals who had undergone at least one cervical cancer screening were practicing cervical cancer screening. 17
Data processing and analysis
The coded data were cleaned, corrected, and double-checked for accuracy, then entered into EPI Data 3.1 and exported to SPSS version 24 for analysis. Categorical variables were presented using frequency and percentages. For continuous variables, the mean and standard deviation were employed. The associations between independent and outcome variables were studied using bivariate and multivariate logistic regression. To control the effect of confounding variables, variables with a p-value of 0.2 in the bivariable analysis were kept in the multivariable model. The model’s fitness was determined using the Hosmer and Lemeshow Goodness of Fit test. The strength of the associations between factors was assessed using crude and adjusted odds ratios, as well as their respective 95% confidence intervals (CI). Statistical significance was defined as a p-value of less than 0.05.
Ethical consideration
Debre Tabor University’s Research and Ethical Review Committee granted ethical approval; the letter’s reference number was CHS/1674/2022. Additionally, the permission letter was obtained from the Debre Tabor town health office and selected health facilities. After getting written informed consent from all literate and legally authorized representatives of all illiterate and under-18-year-old participants, the data were collected. The study was conducted per the Declaration of Helsinki. The participants in the study received no financial compensation or benefit whatsoever. The study participants were identified using codes to protect data confidentiality, and no unauthorized individuals had access to the information obtained.
Results
Sociodemographic characteristics of the study participants
A total of 816 women participated in the study, making the response rate 100%. The participants’ ages ranged from 15 to 49, and the mean (±SD) age of the participants was 28.8 (±5.43) years. The majority of the participants, 369 (45.2%), were within the age range of 24–32 years. Most of the participants, 760 (93.1%), were Orthodox followers, and more than half of them, 567 (69.5%), were married. Among the study participants, 317 (38.8%) were educated up to the college level or above, and the majority of the participants, 268 (32.8%), were housewives. The three-fourth of the participants, 626 (76.7%), had a monthly household income above 1500 Ethiopian Birr (Table 1).
Sociodemographic characteristics of the study participants attending Debre Tabor town health facilities, North Central Ethiopia, 2023 (n = 816).
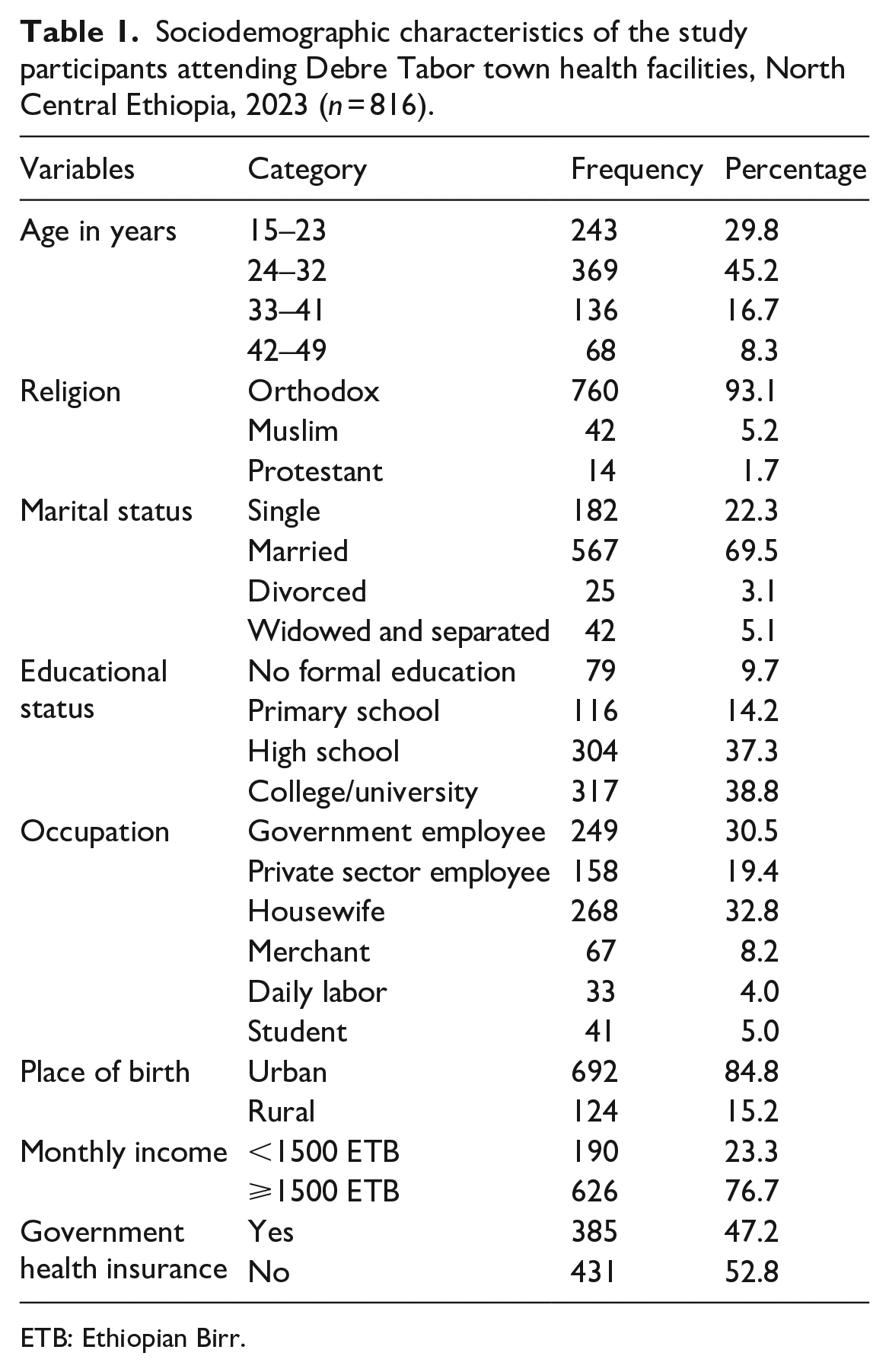
ETB: Ethiopian Birr.
Reproductive characteristics of the study participants
More than two-thirds (586, or 71.8%) of the participants had started sexual intercourse at an age group of less than 18 years. Among the participants, 16.5% had a history of casual sex; 67% had a history of pregnancy; 9.9% had a history of abortion; and 8.3% had a family history of cervical cancer. Of all the participants, 87 (10.7%) used oral contraceptives (Table 2).
Reproductive characteristics of the study participants attending Debre Tabor town health facilities, North Central Ethiopia, 2023 (n = 816).

Knowledge of cervical cancer screening
Overall, 347 (42.5%) (95% CI: 38.5–46.4) of the participants had good knowledge of cervical cancer screening, that is, scored greater than or equal to the mean, and the rest (57.5%) had poor knowledge. The mean score and standard deviation of respondents’ knowledge about cervical cancer screening were 5.99 and ±5.23, respectively. More than two-thirds (574, or 70.3%) of participants had heard about cervical cancer. Of those who had heard about cervical cancer, the largest number, 261 (45.5%), had heard about it in the mass media. About 42.7% of the participants did not know any symptoms of cervical cancer. About 47.8% of the respondents did not know about cervical cancer screening. The majority (71.8%) of the participants did not know any of the procedures used in screening for cervical cancer. More than two-fifth of the participants, 340 (41.7%), had no idea what factors raised the chance of getting cervical cancer. Regarding prevention, about two-fifth of the participants, 328 (40.2%), did not know the prevention methods for cervical cancer. Regarding treatment, more than half (51.7%) of the respondents did not know the treatment for cervical cancer (Table 3).
Cervical cancer screening knowledge level among family planning service users at Debre Tabor town health facilities, North Central Ethiopia, 2023 (n = 816).

HPV: human papillomavirus; OCPs: Oral contraceptive pills.
Attitude toward cervical cancer and its screening
Overall, 300 (36.6%) (95% CI: 32.9–39.8) of the participants had a positive attitude toward cervical cancer and its screening. The mean score and standard deviation of respondents’ attitudes toward cervical cancer and its screening were 18.03 and ±6.16, respectively. Of all the respondents, 232 (28.4%) agreed that cervical cancer is becoming a problem in Ethiopia. About 284 (34.8%) of the respondents agreed that anyone, including themselves, could have the chance of acquiring cervical cancer. More than one-quarter of the respondents (242, or 29.7%) agreed that cervical carcinoma is transmitted from person-to-person. More than one-third (326, or 39.9%) of the respondents thought that screening helped prevent cervical cancer. Two-fifths of the participants (325, or 39.8%) were willing to undergo cervical cancer screening (Table 4).
Attitudes toward cervical cancer among family planning service users at Debre Tabor town health facilities, North Central Ethiopia, 2023 (n = 816).

The practice of cervical cancer screening
Of all the participants, only 164 (20.1%) (95% CI: 17.2–22.3) had been screened for cervical cancer before the survey. Of those who had been screened, all had been screened in hospitals, and the majority of them (58.5%) were screened at the initiation of a health professional (Table 5).
Practices toward cervical cancer among family planning service users at Debre Tabor town health facilities, North Central Ethiopia, 2023 (n = 816).

Among the reasons mentioned for non-screening, 66.2% were because of inadequate information, 46% absence of symptoms, 32.2% attitude toward the screening process, 31.7% absence of readiness, 21.4% absence of screening services, 18.6% mentioned expensive service costs, and 13.8% because of embarrassment (Figure 1).

Major reasons not to screen for cervical cancer among family planning service users at Debre Tabor town health facilities, North Central Ethiopia, 2023, (n = 816).
Factors associated with knowledge of cervical cancer screening
Age, marital status, educational status, monthly income, age of first sex, family history of cervical cancer, and source of information from the media were all found to be significantly associated with having adequate knowledge of cervical cancer screening in a bivariate logistic regression analysis. However, in the multivariable logistic regression analysis, marital status, educational status, family history of cervical cancer, and source of information from the media were independently associated with adequate knowledge of cervical cancer screening.
As a result, single women were three times more likely to have good knowledge about cervical cancer screening than their counterparts (AOR = 3.39, 95% CI: 1.15–6.26). In addition, women who attended a college or university were eight times more likely to have good knowledge about cervical cancer screening than those who did not attend formal education (AOR = 8.03, 95% CI: 3.45–19.23). Similarly, women who had a family history of cervical cancer were three times more likely to be knowledgeable about cervical cancer screening compared with those who did not have a family history of the disease (AOR = 3.14, 95% CI: 1.82–8.84). Furthermore, participants who had a source of information from the media were two times more likely to have good knowledge of their cervical cancer screening when compared to those who had not had a source of information from the media (AOR = 1.74, 95% CI: 1.09–2.54; Table 6).
Factors associated with knowledge of cervical cancer screening among family planning service users at Debre Tabor town health facilities, North Central Ethiopia, 2023 (n = 816).

COR: Crude odds ratio; ETB: Ethiopian Birr; FH-CC: Family history of cervical cancer.
Statistically significant association at p-value 0.001–0.05.
p Value < 0.001.
Factors associated with the attitude toward cervical cancer screening
Age, educational status, occupational status, monthly income, and knowledge of cervical cancer were associated with a positive attitude toward cervical cancer screening in a bivariate logistic regression analysis. However, in the multivariable logistic regression analysis, age, educational status, and knowledge of cervical cancer were found to be significantly associated with a positive attitude toward cervical cancer screening. Thus, those participants who were aged 15–23 years were six times more likely to have a positive attitude toward cervical cancer screening compared with women of 42–49 years of age (AOR = 5.62, 95% CI: 2.76–14.56). Similarly, participants who had a college or university education were four times more likely to have a positive attitude toward cervical cancer screening than those who did not attend formal education (AOR = 3.69, 95% CI: 1.65–8.22). Moreover, women with good knowledge of cervical cancer were five times more likely to have a positive attitude toward cervical cancer screening than those with poor knowledge (AOR = 4.71, 95% CI: 3.08–7.55; Table 7).
Factors associated with the attitude toward cervical cancer screening among family planning service users at Debre Tabor town health facilities, North Central Ethiopia, 2023 (n = 816).

CC: Cervical Cancer; ETB: Ethiopian Birr.
Statistically significant association at p-value 0.001–0.05.
p Value < 0.001.
Factors associated with cervical cancer screening practice
In the bivariate logistic regression analysis, age of first sex, marital status, educational status, type of family planning used, history of pregnancy, and knowledge of cervical cancer were found to be associated with good practice in cervical cancer screening. But, in multivariate analysis, age of the first sex, educational status, and knowledge of cervical cancer were independently associated with good cervical cancer screening practice. Therefore, women whose age of first sexual intercourse was less than 18 years were five times more likely to have good practice with cervical cancer screening than those whose age of first sexual intercourse was greater than 18 years (AOR = 5.0, 95% CI: 3.80–9.20). On the other hand, women who attended high school were 54% less likely to have good practice with cervical cancer screening than those who did not attend formal education (AOR = 0.46, 0.23–0.73). Women with good knowledge of cervical cancer were 1.5 times more likely to have good practice with cervical cancer screening than those with poor knowledge (AOR = 1.52, 95% CI: 1.21–5.82; Table 8).
Factors associated with the practice of cervical cancer screening among family planning service users at Debre Tabor town health facilities, North Central Ethiopia, 2023 (n = 816).

CC: Cervical Cancer.
Statistically significant association at p-value 0.001–0.05.
p Value < 0.001.
Discussion
This study was conducted to assess the knowledge, attitude, and practice of cervical cancer screening and its associated factors among family planning users at Debre Tabor town health facilities. The present study revealed that 70.3% of women have heard about cervical cancer. This finding was consistent with the study that has been conducted in Ambo, Central Ethiopia (68.8%), 17 and Ghana (68.4%). 18 However, the finding of the current study was higher than the studies conducted in Gondar town, northwest Ethiopia (65.1%); 19 Finote Selam, northwest Ethiopia (34.3%); 20 Dessie town, northeast Ethiopia (57.7%); 21 Addis Ababa, Ethiopia (42.7%); 16 Wollega, western Ethiopia (54.4%); 22 and India (65.5%). 23 This disparity could be due to a variety of factors, including differences in the study setting, study population, sample size, and study period. On the contrary, our finding was lower than a similar study conducted in Gondar (90%), 15 Gurage Zone, Southern Ethiopia (83.8%), 11 Dire Dawa, Eastern Ethiopia (84.4%), 24 Adigrat Town, Northern Ethiopia (79.6%), 25 Gabon (91.6%), 26 and Uganda (88.2%). 27 This discrepancy could be due to differences in the study setting and study population.
In the current study, mass media was the major source of information (45.5%). This finding was in line with those of studies conducted in Gondar (41.1%) 19 and Finote Selam (41.7%). 20 However, our finding was lower than other similar studies.11,17,21,24,25,27 This difference might be due to differences in media coverage among the countries and towns.
The study found that the level of knowledge about cervical cancer screening was 42.5% (95% CI: 38.5–46.4). This finding was concordant with the studies conducted in Wolaita, Southern Ethiopia (43.1%) 1 and Adigrat (46.4%). 25 However, our report was higher than the studies done in Addis Ababa (27.7%), 16 Gondar town (19.9%), 19 Finote Selam (30.3%), 20 Gurage Zone (26.2%), 11 Dire Dawa (9.3%), 24 Nepal (13%), 28 Cameroon (3.6%), 29 Perambalur (36.5%), 30 and India (11%). 23 This variation might be due to differences in time, sample size, and sociodemographic features of study participants. In addition, this difference might be due to the different study settings. Our study was a health facility-based study, meaning that participants might have better health-seeking behavior and may have had contact with health professionals, exposing them to information about cervical screening, whereas Gondar, Finote Selam, and Gurage Zone studies were conducted in the community. In contrast, our finding was lower than the report from Gondar (59.3%), 15 Dessie (51%), 21 Addis Ababa (60.8%), 31 Ambo (50.7%), 17 Rwanda (50.1%), 32 and China (51.9%). 33 This difference might be because of the variation in study setting and population, as well as the socioeconomic and demographic variation.
Nearly one-third, or 36.6% (95% CI: 32.9–39.8), of the respondents had a positive attitude toward cervical cancer screening. This finding was lower than the report in the two Gondar studies (67.7%, 58.2%),15,19 Finote Selam (58.1%), 20 Wolaita (45.5%), 1 Wollega (44.1%), 22 Ambo (46.1%), 17 Dira Dawa (60.1%), 24 Adigrat (53.3%), 25 China (96%), 33 Perambalur (83.8%), 30 and Nepal (85%). 28 This discrepancy might be due to socioeconomic, demographic, study setting, and study population differences.
Almost one-fifth, or 20.1% (95% CI: 17.2–22.3), of the study participants had done cervical cancer screening. This finding was in line with the studies done in Wolaita (22.9%) 1 and Cameroon (20%). 29 However, this finding was higher than the studies conducted in Gondar (0.5%), 15 Ambo (6.3%), 17 Gurage Zone (3.8%), 11 Dire Dawa (2.5%), 24 Ghana (0.8%), 18 Nepal (13.6%), 28 Perambalur (2.7%), 30 and India (9.5%). 23 On the other hand, the findings of the present study were lower than those reported in Addis Ababa (25%), 16 Adigrat (38.1%), 25 Rwanda (28.3%), 32 Gabon (65.1%), 26 and China (63.7%). 33 This difference might be due to time variation, differences in study setting, study population, or sociodemographic variables.
In the present study, being single was significantly associated with good knowledge of cervical cancer screening. This finding was in line with the previous study done in Addis Ababa. 16 The result can be explained by the fact that single women are more likely to be younger and have had more exposure to sexual education. The current study also found an association between educational status and good knowledge of cervical cancer screening. Similar findings were obtained in other studies.1,17,20,21,25,31,33 People who are more educated read more, heed the advice of medical professionals, and learn more about their health conditions, which may give them better knowledge about cervical cancer screening. According to our findings, a family history of cervical cancer was independently associated with good knowledge of cervical cancer screening. This result was similar to that of previous investigations.11,31 This might be because those families who had exposure to cervical cancer can easily inform their family of any clinical signs, symptoms, or adverse effect-related condition of the disease. In addition, the source of information from the media was significantly associated with knowledge of cervical cancer screening. The use of various mass media outlets has increased recently. Information can be quickly and easily disseminated to a large audience by using mass media. One method for increasing cervical screening awareness is the use of the media.
In the current study, the younger age group (15–23 years) was significantly associated with a positive attitude toward cervical cancer screening. This finding was consistent with the study conducted in Wollega, Western Ethiopia. 22 This might be because younger women have obtained more sexual education and knowing the importance of screening increases women’s attitudes toward screening services. Similarly, educational status was significantly associated with a positive attitude toward cervical cancer screening. This finding was consistent with earlier studies.20,25,33 Women with higher levels of education have greater abilities to communicate and an increased capacity for knowledge retention, which may help them comprehend the nature of the disease and have a favorable attitude toward cervical cancer screening. Moreover, good knowledge of cervical cancer was significantly associated with a positive attitude toward cervical cancer screening. This finding was in line with the reports from other studies.1,20 This could be explained by participants becoming more motivated to seek healthcare as a result of acquiring knowledge regarding the importance of cervical cancer screening.
An earlier age of first sexual intercourse was significantly associated with the practice of cervical cancer screening. This result was similar to the study conducted in the Gurage Zone, Southern Ethiopia. 11 In addition, good knowledge of cervical cancer was positively associated with good practice of cervical cancer screening. This finding was consistent with the study conducted in the Gurage Zone, Southern Ethiopia, 11 and Tanzania. 34 This could be because those respondents who were aware of cervical screening were more likely to attend health facilities. Understanding the significance of screening gives women a compelling reason to seek this service. On the other hand, women who attended high school were negatively associated with the good practice of cervical cancer screening. Women who attended high school were 54% less likely to have good practice with cervical cancer screening than those who did not attend formal education. This finding differs from the previous finding, 25 where women who attended high school were positively associated with good practice in cervical cancer screening. This might be due to the differences in the respondents’ socioeconomic and demographic factors.
Limitation of the study
Firstly, this study was a cross-sectional study and therefore was not able to establish a causal relationship between dependent and independent variables. Secondly, the study is a health facility-based study, which may limit the generalizability of the findings to all women in Ethiopia. Thirdly, the potential role of men in improving cervical cancer screening rates was not investigated in this study.
Conclusion
The overall knowledge, positive attitude, and practice toward cervical cancer screening were low. Being single, educational status, family history of cervical cancer, and the media as the source of information were significantly associated with knowledge of cervical cancer screening. Women who were aged 15–23 years, educational status, and knowledge of cervical cancer were significantly associated with attitudes toward cervical cancer screening. Early age at the first sex and knowledge of cervical cancer were positively associated with the practice of cervical cancer screening, whereas women who attended high school were negatively associated with the practice of cervical cancer screening. Healthcare facilities should implement health education and awareness-raising campaigns regarding cervical cancer. At the community level, additional research with a qualitative component is recommended.
Supplemental Material
sj-docx-1-smo-10.1177_20503121231208654 – Supplemental material for Knowledge, attitude, and practice of cervical cancer screening and its associated risk factors among family planning service users at Debre Tabor town health facilities, North Central Ethiopia: A cross-sectional study
Supplemental material, sj-docx-1-smo-10.1177_20503121231208654 for Knowledge, attitude, and practice of cervical cancer screening and its associated risk factors among family planning service users at Debre Tabor town health facilities, North Central Ethiopia: A cross-sectional study by Shewaneh Damtie, Biruk Legese, Ayenew Berhan, Teklehaimanot Kiros, Tahir Eyayu, Kefiyalew Mihrete and Wubet Taklual in SAGE Open Medicine
Footnotes
Acknowledgements
The authors would like to acknowledge Debre Tabor University, College of Health Science. We would also like to thank all study participants and data collectors for their cooperation.
Authors’ contributions
SD was the primary investigator who was involved in conceptualization, data curation, formal analysis, methodology, laboratory investigation, results in interpretation, involved in execution, acquisition of data, data statistical analysis, drafting of the article, and engagement in critically revising of the article. BL, AB, TT, TE, KM, and WT were involved in the execution, acquisition of data, data statistical analysis, results in interpretation, drafting of the article, and engaged in critically revising of the article. All authors read and approved the final article.
Availability of data and materials
All data generated or analyzed during this study are included in this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval and informed consent
Debre Tabor University’s Research and Ethical Review Committee granted ethical approval; the letter’s reference number was CHS/1674/2022. Additionally, the permission letter was obtained from the Debre Tabor town health office and selected health facilities. After getting written informed consent from all literate and legally authorized representatives of all illiterate and under-18-year-old participants, the data were collected. The study was conducted as per the Declaration of Helsinki. The participants in the study received no financial compensation or benefit whatsoever. The study participants were identified using codes to protect data confidentiality, and no unauthorized individuals had access to the information obtained.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Trial registration
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.