
Abstract
There are long-standing debates about the benefits of prostate cancer screening. Conflicting trial results and inconsistent recommendations regarding prostate cancer screening in clinical guidelines highlight the importance of patient factors that influence decision making in prostate cancer screening. Attitude is an important factor associated with cancer screening. However, attitudes toward prostate cancer screening among Chinese men are still poorly understood. The objective of the study was to evaluate attitudes toward prostate cancer screening and their association with prostate cancer screening intention among Chinese men. In this community-based study, 340 males were randomly recruited. Three distinct concepts related to prostate cancer screening attitudes were evaluated, including perceived consequences of screening, moral obligation, and anticipated regret. The intention to have prostate cancer screening was asked. Only 5.00% of the study participants had prostate cancer screening before, while 69.71% have an intention to undergo screening in the future. Participants with a high level of anticipated regret also had a high likelihood to have screening in the future, with an adjusted odds ratio (aOR) of 1.82. Participants who had favorable attitudes toward the consequence of participating in prostate cancer screening had a high likelihood to undergo screening, with an aOR of 1.22. Participants who were more concerned about pain and invasion of privacy were less likely to have an intention to have prostate cancer screening, with aORs of 0.53 and 0.57, respectively. To enhance screening intention, public health programs should include components related to anticipated regrets and perceived consequences.
Prostate cancer is one of the most principal and rising health concerns among older men, exhibiting an increasing trend in its incidence. According to the article “The Global Burden of Cancer 2013,” prostate cancer is the leading cause of cancer incidence for men (Fitzmaurice et al., 2015), imposing a very high burden and associated costs on the health system. Results from the Global Burden of Disease Study in 2015 also reported that the incident cases of prostate cancer increased 3.7-fold from 1990 to 2015 (Pishgar et al., 2018). During this period, age-standardized incidence rate also increased 1.7-fold and disability-adjusted life years attributable to prostate cancer increased by 90%. Despite the steady increase in incidence rate, the effectiveness of prostate cancer screening and improvements in therapeutic approaches, including surgery, radiation therapy, and hormonal and chemotherapy, have led to a decrease in prostate cancer mortality (Pishgar et al., 2018). Based on epidemiological data, the burden of prostate cancer is substantial in China. Prostate cancer is the sixth common malignancy and the tenth leading cause of cancer death in China (Bai et al., 2020). An epidemiological study reported that the incidence rates of prostate cancer for those aged ≥65 in Asian regions (i.e., Japan, Hong Kong, and mainland China) had increased progressively with time (Teoh et al., 2019). It is estimated that the incidence rate of prostate cancers will continue to rise in China in future decades due to the rise of the aging population (Tsoi et al., 2017). The Global Burden of Disease Study 2015 reported that most prostate cancer deaths occurred in China (Pishgar et al., 2018). A systematic review and meta-analysis published in 2020 reported that compared with other Asian countries, China has the lowest 1-year (64.1%) and 10-year (9.4%) survival rates of prostate cancer (Hassanipour et al., 2020). The impacts of prostate cancer on patients are detrimental. A study in Hong Kong reported that prostate cancer patients had poorer health-related quality of life than the general population, with lower scores in general health, vitality, and mental health domains of the Short Form-12 Health Survey version 2 (Choi et al., 2016). These data suggest that all primary, secondary, and tertiary prevention programs for prostate cancer in China should be strengthened.
The delayed diagnosis of prostate cancer leads to a more advanced disease presentation with higher mortality rate (Pishgar et al., 2018). Some debates have arisen about the benefits of routine prostate cancer screening because prostate-specific antigen (PSA) screening is associated with overdiagnosis and the detection of indolent cancer (Boyle & Brawley, 2009). The Prostate, Lung, Colorectal, and Ovarian Cancer Screening Trial also reported no evidence of a mortality benefit for organized annual prostate cancer screening (Andriole et al., 2012). By contrast, it was estimated that PSA screening accounts for 45%–70% of the reduction in prostate cancer mortality in the United States (Etzioni et al., 2008). The European Randomized Study of Screening for Prostate Cancer (ERSPC) confirmed a substantial reduction in prostate cancer mortality due to PSA screening, with a relative risk reduction of 21% in men randomized to screening (Schröder et al., 2014). A review summarized that undergoing PSA-based screening for prostate cancer annually to once every four years can significantly reduce the risks of metastatic prostate cancer development and death as a result of prostate cancer (Ito et al., 2019). The ERSPC also predicted that the annual screening of men between the ages of 55 and 69 years would result in a total of 73 life-years gained per 1000 men of all ages who were followed for their entire lifespan (Heijnsdijk et al., 2012).
Conflicting trial results about PSA screening, potential risks associated with screening, and inconsistent recommendations regarding PSA screening in clinical practice guidelines highlight the paramount importance of patient factors that influence decision-making on PSA screening (James et al., 2017). For many health behavior models and theories, such as theory of reasoned action and theory of planned behavior (Fazio & Zanna, 1981; Madden et al., 1992; Sheppard et al., 1988), attitude is an important determinant of an individual’s behavior. In the contexts of cancer screening, a systematic review and meta-synthesis of qualitative studies about colorectal cancer screening reported that attitude toward screening is an important factor associated with participation in colorectal cancer screening (Honein-AbouHaidar et al., 2016). A review about the barriers to prostate cancer screening in sub-Saharan Africa also reported that attitudes toward prostate cancer screening play an important role in influencing the uptake of prostate cancer screening (Baratedi et al., 2020). A greater understanding of the attitudes toward prostate cancer screening is needed so that an appropriate health promotion program can be developed to aid people in making informed choices.
Attitude is a complex concept. With respect to cancer screening, Lechner et al. (1997) suggested that attitudes toward cancer screening could be divided into several domains, including (a) perceived consequences of screening, (b) moral obligation, and (c) anticipated regret. Lechner and colleagues have used this conceptual framework to explore factors associated with breast cancer screening behaviors (Lechner et al., 1997). First, people are concerned about the possible consequences of cancer screening. The long-term outcomes of cancer screening might be very positive because they may lengthen a healthy life. However, people might also be worried about the immediate outcomes of cancer screening, such as pain and fear of the results. Second, by participating in cancer screening, people might feel that they are fulfilling a moral obligation. The concept of moral obligation has also been studied in relation to screening for cervical cancer (Tacken et al., 2007), breast cancer (Griffiths et al., 2010), and colorectal cancer (Ward et al., 2015). Third, anticipated regret is another possible outcome related to cancer screening. People might think that not attending the screening would leave them with feelings of regret if cancer is detected at a later date. A study reported that anticipated regret could lead to a significant increase in colorectal cancer screening update (O’Carroll et al., 2015). Another study also reported that anticipated regret was a significant predictor of intention to attend for a cervical smear test (Walsh, 2005). However, based on a review by Koch, current evidence about the role of anticipated regret in medical screening is still conflicting, suggesting that additional research is necessary (Koch, 2014). Compared with other cancer types, such as breast cancer and colorectal cancer, there is a dearth of research about attitudes toward prostate cancer screening. The conceptual framework proposed by Lechner et al. (1997) has not been used to understand prostate cancer screening behavior. Besides, most existing studies about attitudes toward prostate cancer screening also do not consider the multidimensional nature of attitude (Gift et al., 2020; Miller et al., 2020), thereby hindering our comprehensive understanding of attitudes toward prostate cancer screening among men.
To the best of our knowledge, no study has explored the attitudes toward prostate cancer screening among Chinese men. Study findings obtained from other populations might be quite specific and cannot be easily generalized to Chinese populations because attitudes toward cancer screening vary across cultures (Kolahdooz et al., 2014; Tay et al., 2013). In addition, cancer screening, including prostate cancer screening, is affected by cultural factors (Curry et al., 2003; Ma et al., 2012). Therefore, to address these research gaps and provide additional information about prostate cancer screening in Chinese populations, the present study aimed to evaluate attitudes toward prostate cancer screening and their association with prostate cancer screening intention among Chinese men in Hong Kong.
Material and Methods
Study Design
This community-based household survey study was conducted in Hong Kong.
Study Participants
The eligibility criteria included Chinese men aged 40–70 years and residing in Hong Kong. Those who could not understand Chinese, refused to join the study, or were too ill to give consent were excluded from the study.
Sampling and Recruitment Procedures
To enhance the representativeness of the study sample and the generalizability of the study findings, households across all districts in Hong Kong were randomly sampled to form a list of addresses. The randomization and sampling procedures were conducted independently by a local research firm in Hong Kong. An invitation letter about the aims and objectives of the household survey study and the personal interview arrangements was sent to the sampled households before each household visit. An enquiry hotline telephone number and the name of a contact person were also included to enable the participants to clarify any questions they might have had on the interview or to make an appointment at a preferred interview time. Once the participants accepted the invitation, trained interviewers visited the sampled addresses on the scheduled date and time. The eligibility criteria of the study participants were checked before the face-to-face interviews were conducted.
Study Instruments
The attitudes toward prostate cancer screening were evaluated using the questionnaire developed by Lechner et al. (Lechner et al., 1997). The following concepts related to attitudes toward prostate cancer were measured.
Perceived consequences of screening were assessed by 11 items. Of this number, seven items consisted of positive consequences of screening, while four items consisted of negative consequences of screening (Cronbach’s alpha: 0.74 in the current study).
The moral obligation men feel to participate in prostate cancer screening was assessed by two items (Cronbach’s alpha: 0.80 in the current study).
Anticipated regret of not participating in prostate cancer screening was assessed by two items (Cronbach’s alpha: 0.73 in the current study).
Participants were asked to rate the items on a four-point Likert scale (3 = strongly agree, 2 = agree, 1 = disagree, 0 = strongly disagree). After the scores of negatively phrased items were recoded, the scores of the individual items of each subscale were added to obtain a subscale score. A higher score indicated a more positive (favorable) attitude/ higher moral obligation/ higher anticipated regret toward prostate cancer screening.
Regarding prostate cancer screening history, participants were asked if they had undergone prostate cancer screening (either PSA or DRE) before. The response options included “yes,” “no,” and “not sure.” Participants were also asked to indicate on a six-point Likert scale (3 = extremely likely, 2 = very likely, 1 = somewhat likely, –1 = somewhat unlikely, –2 = very unlikely, –3 = extremely unlikely) their intention to participate in prostate cancer screening in the future (Lechner et al., 1997). For subsequent analysis, we dichotomized the responses into “yes” and “no.” Data on age, marital status, employment status, and monthly personal income were also collected.
Analysis
First, descriptive statistics were used to summarize the distribution of response options of each individual item of attitudes toward prostate cancer screening. Second, independent t-test was used to compare the mean attitude scores (a) between participants who intended to have prostate cancer screening in the future and those who did not; and (b) between participants who had prostate cancer screening before and those who did not/were not sure. We also calculated Cohen’s d effect sizes, which were interpreted as either trivial (<0.2), small (≥0.2 and <0.5), moderate (≥0.5 and <0.8), or large (≥0.8) (Sullivan & Feinn, 2012). Third, multiple logistic regression was conducted to explore the association between attitudes toward prostate cancer screening and screening intention, controlling for sociodemographic factors.
Ethics
The study protocol was approved by the institutional review board of the University of Hong Kong/Hospital Authority Hong Kong West Cluster (reference number: UW 20-324). All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. Written informed consent was obtained from each study participant.
Results
Sample Characteristics
A total of 860 households across all the districts in Hong Kong was randomly selected. Among the selected households, 275 (31.98%) were not eligible, 89 (10.35%) refused to join the study, and 156 (18.14%) could not be reached after five attempts, resulting in a final total of 340 (39.53%) households. Finally, 340 males (one from each household) were successfully interviewed and included in the analysis of this study.
The mean age was 54.43 years (SD 9.35). Among the participants, 232 men (68.24%) were between 40 and 60 years old, and 108 men (31.76%) were over 60 years old. Regarding marital status, 286 men (84.12%) were married. Further, 222 men (65.29%) had a full-time job, and 206 men (60.59%) had a monthly personal income ≤HKD$20,000. Only 17 men (5.00%) had prostate cancer screening before, while 237 men (69.71%) intended to have prostate cancer screening in the future. Table 1 shows the characteristics of the participants.
Sociodemographics and Study Outcomes Among 340 Participants.

Note. SD = standard deviation.
Attitudes Toward Prostate Cancer Screening
Regarding attitudes toward the perceived consequences of prostate cancer screening, more than 80% of the participants endorsed that if they participate in prostate cancer screening, they will feel considerably more certain about their health (n = 291, 85.59%); they will have a lot of reassurance (n = 290, 85.29%), will be able to detect an abnormality a great deal earlier (n = 289, 85.00%), and get a very clear explanation of the screening (n = 275, 80.88%). Furthermore, 277 men (81.47%) agreed that attending prostate cancer screening will show that they care for their health very much. However, regarding the negative consequences of prostate cancer screening, more than 40% of the participants expressed that undergoing prostate cancer screening will involve a significant amount of time (n = 152, 44.71%), and they will experience a lot of fear of the screening results (n = 142, 41.76%). In particular, 119 men (35.00%) were worried that they will experience immense pain. Additionally, 100 men (29.41%) are concerned about the privacy issue. Concerning moral obligation, about 80% of the study participants agreed that by participating in prostate cancer screening, they will fulfill a very great obligation to themselves (n = 271, 79.71%) and their family (n = 280, 82.35%). With respect to anticipated regret, 244 men (71.76%) agreed that if they did not participate in the screening but prostate cancer was detected at a later date, then they would feel very regretful. Table 2 presents the descriptive statistics.
Descriptive Statistics About Attitude Toward Prostate Cancer Screening.

Note. Likert scale: 3 = strongly agree, 2 = agree, 1 = disagree, 0 = strongly disagree.
reversed items.
After the scores of reversed items were recoded, the scores of the individual items were added to obtain a subscale score.
Association Between Attitude Toward Prostate Cancer Screening and Screening Intention
There were statistically significant differences in attitude between participants who intended to have screening in the future and those who did not. Compared with those who did not intend to have screening in the future, those who did intend to have screening had a more favorable attitude toward the consequence of participating in prostate cancer screening (Cohen’s d effect size: 0.80), a higher level of moral obligation (Cohen’s d effect size: 0.65), and a higher level of anticipated regret (Cohen’s d effect size: 0.82). Table 3 presents the results of independent t-test. Multiple logistic regression analysis found that participants who had a more favorable attitude toward the consequence of participating in prostate cancer screening had a higher likelihood of having the screening in the future, with an adjusted odds ratio of 1.22, 95% CI [1.12, 1.34], while those who had a higher level of anticipated regret also had a higher likelihood to have screening in the future, with an adjusted odds ratio of 1.82, 95% CI [1.38, 2.39]. However, the association between moral obligation and screening intention became statistically insignificant in the logistic regression model. Table 4 presents the results of the logistic regression model.
Attitude Toward Prostate Cancer Screening and Prostate Cancer Screening Intention and History.

Note. SD = standard deviation.
A higher score indicated a more positive (favorable) attitude toward prostate cancer screening.
For outcome “yes,” we combined “extremely likely,” “very likely,” and “somewhat likely.”
For outcome “no,” we combined “extremely unlikely,” “very unlikely,” and “somewhat unlikely.”
p value was obtained using independent t-test.
Results of Multiple Logistic Regression to Explore Factors Associated With Prostate Cancer Screening Intention.
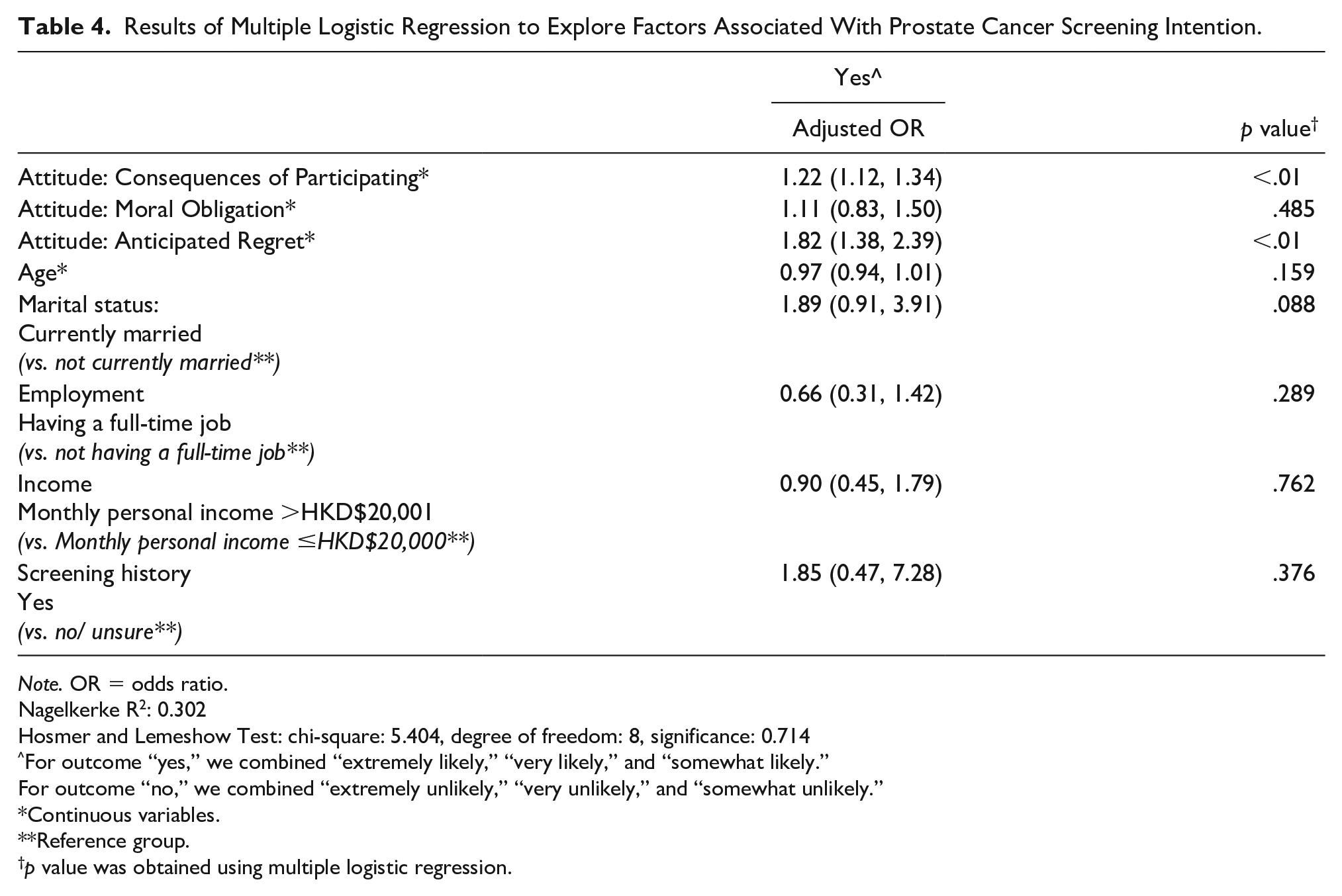
Note. OR = odds ratio.
Nagelkerke R2: 0.302
Hosmer and Lemeshow Test: chi-square: 5.404, degree of freedom: 8, significance: 0.714
For outcome “yes,” we combined “extremely likely,” “very likely,” and “somewhat likely.”
For outcome “no,” we combined “extremely unlikely,” “very unlikely,” and “somewhat unlikely.”
Continuous variables.
Reference group.
p value was obtained using multiple logistic regression.
To further understand which specific areas of attitude associated with screening intention, we put individual items in the regression model. We found that participants who were more concerned about pain and invasion of privacy were less likely to have an intention to undergo prostate cancer screening in the future, with adjusted odds ratios of 0.53, 95% CI [0.32, 0.87] and 0.57, 95% CI [0.34, 0.93], respectively. Both individual items of anticipated regret were associated with an intention to have prostate cancer screening in the future, with adjusted odds ratios of 2.68, 95% CI [1.49, 4.82] (item 14) and 1.80, 95% CI [1.06, 3.07] (item 15), respectively. The results are presented in Table 5.
Results of Multiple Logistic Regression to Explore Factors Associated With Prostate Cancer Screening Intention (Individual Items).

Note. OR = odds ratio.
Nagelkerke R2: 0.360.
Hosmer and Lemeshow Test: chi-square: 3.668, degree of freedom: 8, significance: 0.886.
Age, marital status, employment status, income, and screening history were controlled in the regression model.
For outcome “yes,” we combined “extremely likely,” “very likely,” and “somewhat likely.”
For outcome “no,” we combined “extremely unlikely,” “very unlikely,” and “somewhat unlikely.”
p value was obtained using multiple logistic regression.
Association Between Attitude Toward Prostate Cancer Screening and Screening History
The results of independent t-test found no statistically significant difference in attitude between those who had prostate cancer screening before and those who did not. Table 3 presents the results of the independent t-test. Multiple logistic regression analysis only found that participants who were older were more like to have prostate cancer screening before (Supplementary Table S1).
Discussion
The study found a low prevalence of prostate cancer screening in Hong Kong: only 5%. This figure is significantly lower than that that reported in previous studies in Western populations. For example, a study in Portugal reported that the lifetime prevalence of having prostate cancer screening at least once was 44.2% (Braga et al., 2020). Another study in the United States reported that 62.4% of the participants reported that they had prostate cancer screening in the last 2 years (Ogunsanya et al., 2016). A study in Brazil reported that the prevalence of prostate cancer screening among men who utilized private health insurance-related services was 63.3%, while it was 41.6% among men who utilized the publicly funded health-care system (Soares et al., 2019). Previous studies in Hong Kong reported that the rate of cancer screening update in Hong Kong is relatively low. For instance, a study of 430 women recruited from a well women clinic reported that 59% of the respondents reported having a pap smear test, and 28% reported having a mammogram (Abdullah et al., 2001). These figures are indeed lower than those reported in other countries, such as the United States (prevalence of having a pap smear test: 79.9%; prevalence of having a mammogram: 66.9%) (Breen et al., 2001). There are some possible explanations for the low prostate cancer screening in Hong Kong. First, there is no population-based approach screening for prostate cancer in Hong Kong. Second, it was reported that misconceptions about cancer screening and a lack of knowledge about prostate cancer screening are common in Hong Kong, leading to a low uptake rate (Mo et al., 2014; So et al., 2014).
In line with the study by Lechner et al. (1997), we found that perceived consequence of cancer screening is associated with intention to have prostate cancer screening in the future. Previous studies reported that having a favorable attitude toward cancer screening is a facilitator to cancer screening (James et al., 2017). A systematic review of qualitative studies reported that the idea that early detection of cancer can improve cancer survival motivated men to undergo prostate cancer screening (James et al., 2017). Men who are more health conscious are more likely to attend prostate cancer screening. Furthermore, some men strive to maintain a sense of control of their body and are therefore inclined to participate in prostate cancer screening (James et al., 2017). The current study provided further evidence that attitude is an important determinant of cancer screening (Schoenborn et al., 2019), implying that improving public attitude toward cancer screening is an important component in health promotion programs and public campaigns that aim to improve cancer screening uptake.
People who are more concerned about pain and invasion of privacy are less likely to have an intention to undergo prostate cancer screening in the future. A study in the Netherlands reported that anticipated pain or discomfort is one of the major reasons to refuse prostate cancer screening (Nijs et al., 2000). A systematic review of qualitative studies summarized that some men have a vague understanding of prostate cancer screening, which causes them to feel concerned and anxious about undergoing screening (James et al., 2017). They thought that prostate cancer screening is invasive and painful (James et al., 2017). Some men felt a loss of personal dignity after undergoing the invasive procedure of screening and were thus unwilling to complete the screening again (James et al., 2017). This phenomenon is not unique to prostate cancer screening. A study about colorectal cancer screening in the United States reported that fear the examination might be painful is positively associated with the unwillingness to participate in colorectal cancer screening, with an adjusted odds ratio of 3.43 (Bynum et al., 2012). Concerns about invasion of privacy in screening have also been documented in the context of cervical cancer and breast cancer screening (Bukirwa et al., 2015; Ndukwe et al., 2013).
The current study found that anticipated regret is associated with an intention to have prostate cancer screening in the future. Similarly, Lechner et al. (1997) reported that anticipated regret could predict an intention to participate in breast cancer screening in the future. The study reported that anticipated regret explains 33% of the variance in intention (Lechner et al., 1997). A meta-analysis about anticipated regret and health behavior reported that anticipated inaction regret (i.e., anticipated regret from not engaging in a behavior, such as cancer screening) is associated with a higher intention of engaging in health behavior, with a pooled effect size of 0.52, and being more likely to engage in the behavior, with a pooled effect size of 0.29 (Brewer et al., 2016). An important clinical implication of this finding is that emphasizing the consequences of inaction (i.e., not having cancer screening) may benefit interventions that focus on anticipated regret as a way to change health behavior (Brewer et al., 2016). An experimental study in the United Kingdom reported that simply asking questions about anticipated regret could increase cervical cancer screening update (Sandberg & Conner, 2009).
Our results are contrary to previous studies that reported past behavior (attending screening before) to be a strong predictor of participating in future screening for breast cancer (Lechner et al., 1997) and cervical cancer (Roncancio et al., 2013). One possible explanation is that the sample size of people who had prostate cancer screening was small, leading to the insignificant results found in the study. A further study with a larger sample size is needed to confirm our findings. Another possible explanation is that, given the absence of symptoms or perceptible health problems, people might think prostate cancer screening is not really necessary (James et al., 2017). Therefore, even though they had prostate cancer screening before, they were not too eager to have it again in the future.
Strengths and Limitations of the Study
This study has several strengths. First, as random sampling was used to recruit study participants across Hong Kong, the sampling bias could be minimized. Second, the study questionnaires were administered by trained interviewers using a face-to-face interview. Accordingly, interviewers could clarify the questions and answer questions raised by the study participants, thus ensuring data quality. Third, instead of considering attitude as a single concept, we evaluated attitudes toward perceived consequence, moral obligation, and anticipated regret, enhancing our understanding about the relationship between attitude and prostate cancer screening intention. Some limitations of the study should be noted as well. First, all study outcomes were self-reported by the study participants. It was difficult to obtain clinical records about the prostate cancer screening history of the study participants in a community-based survey. Therefore, recall bias and social disability bias should be taken into consideration. Second, the causality of the study variables could not be provided in this cross-sectional study. Third, the study findings might not be generalizable to other populations given that attitude is a culturally specific concept while cancer screening behaviors are affected by many other factors, such as health-care systems.
Conclusion
Prostate cancer screening was not common in our study sample, with only 5% of the participants having been screened before, while 69.71% of the participants intended to have prostate cancer screening in the future. Attitude about the perceived consequence of screening was associated with prostate cancer screening intention in the future. Specifically, people who were concerned about pain and invasion of privacy were less likely to have screening intention. Anticipated regret was another important factor associated with prostate cancer screening intention in the future. To enhance prostate cancer screening intention, public health campaigns and health promotion programs should include components related to anticipated regrets and perceived consequences.
Supplemental Material
sj-docx-1-jmh-10.1177_15579883211051442 – Supplemental material for Attitude Toward Prostate Cancer Screening in Hong Kong: The Importance of Perceived Consequence and Anticipated Regret
Supplemental material, sj-docx-1-jmh-10.1177_15579883211051442 for Attitude Toward Prostate Cancer Screening in Hong Kong: The Importance of Perceived Consequence and Anticipated Regret by Edmond P.H. Choi and Eric Y.F. Wan in American Journal of Men’s Health
Footnotes
Acknowledgements
We would like to thank Professor Lilian Lechner for her advice on the study instrument and Social Policy Research Limited for data collection.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Seed Fund for Basic Research, the University of Hong Kong (Reference: 201811159199).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.