
Abstract
Background:
This retrospective study aimed to evaluate our single-center experience with Magseed as a pre-operative localization system in a cohort of 47 patients with non-palpable breast lesions.
Design and methods:
Forty-seven patients with non-palpable breast lesions, who underwent Magseed pre-operative localization followed by breast-conserving surgery between November 2022 and June 2024 at our Breast Unit were enrolled in our study. The procedure involved percutaneous placement of the Magseed into the target lesion under ultrasound (66%) or stereotactic (34%) guidance. Data on patient demographics, lesion characteristics, Magseed localization and retrieval, surgical outcomes, and complications were collected and analyzed.
Results:
Magseed localization was successful in all cases, with no marker migration or dislodgment, and all seeds were retrieved (100%). Breast-conserving surgery was successful in 97.9% of patients, with only one requiring intraoperative widening. No significant complications were reported. Histopathology revealed predominantly invasive breast cancers, with “No Special Type” being the most common subtype (42.5%).
Conclusions:
The effectiveness of this technique is proven by our results, which reflect the data in the growing scientific literature on Magseed.
Keywords
Introduction
Breast cancer remains a worldwide public health dilemma and is currently the most common tumor in the globe. The approach to diagnosing and treating breast cancer is evolving from a uniform strategy to a new era of personalized medicine. 1
Breast cancer is typically identified either through routine screening or when symptoms such as pain or a detectable lump lead to a diagnostic test. Thanks to advancements in imaging technology and the implementation of screening programs that enable the early detection of breast lesions, the number of patients with non-palpable breast lesions has been steadily rising. 2
Moreover, screening healthy women often results in diagnosing tumors that are smaller, less likely to have spread, more suitable for breast-conserving surgery (BCS) and limited axillary procedures. This approach leads to fewer treatment-related complications and better survival rates. 3
Therapy concepts follow a curative intent and need to be decided in a multidisciplinary setting, taking molecular subtype and locoregional tumor load into account.
BCS combined with adjuvant radiotherapy, referred to as breast conservation therapy (BCT), has emerged as an alternative to mastectomy for early-stage breast cancer due to its comparable survival rates and reduced morbidity.4,5
Preoperative localization using imaging is essential for accurately guiding the surgery of non-palpable lesions or significant extensions of palpable lesions, thereby improving both oncological and cosmetic outcomes. 6
Wire-guided localization (WGL) was introduced in the 1970s and has served for many years as the only method for preoperative breast localization. 7
The established benefits of WGL include its widespread availability and moderate cost. Additionally, wires do not emit ionizing radiation and can be safely stored within the imaging department. However, this technique has several drawbacks.
Wires need to be placed a short time before surgery and patients must limit their movements to reduce the risk of wire displacement and migration, causing discomfort for the patient and surgical scheduling difficulties. Moreover, in some patients WGL has been associated with the development of hematomas and vasovagal reactions.
Another limitation is the site of wire insertion, which is normally placed where it is easier for the radiologist and does not consider the surgeon’s cosmetic surgical approach, potentially resulting in increased breast volume resection.
For surgeons, wires pose a significant disadvantage in the operating room, as they have to mentally plan the surgical approach by visualizing the mammogram with the consequent breast tissue compression, since it is not possible to localize the wire prior to opening the skin. 8
The surgeon must follow the wire tip through the breast tissue to locate the lesion, which can result in the excessive removal of healthy tissue, and it must remain in place until the surgery, potentially causing discomfort and pain. The wire may migrate, be transected, or become displaced, necessitating possible repositioning under image guidance.9,10
Magnetic seed (Magseed® (Endomagnetics, Cambridge, UK)) is a novel localization technique approved by the FDA in 2016. This technique shares many similarities with radioactive seed localization as it consists in seed placement under sonographic or tomosynthesis guidance, however it does not involve radioactivity. 11
Magseed is an inducible non-wire non-radioactive paramagnetic seed which is made of surgical grade stainless steel. The seed can be placed inside the breast lesion at any time prior to surgery. The detector probe temporarily magnetizes the iron in the seed, generating a magnetic field. It then detects this magnetization to provide real-time localization. While detection is reliably effective up to a depth of 4 cm from the skin’s surface, the manufacturer has reported successful detection up to 12 cm through palpation if the patient is in a supine position. 12
The use of Magseed to guide the resection of non-palpable breast lesions presents many advantages compared to WGL: precise surgical guiding, less discomfort for patients, and the facilitation of surgical scheduling, as the seed can be placed any time before surgery.
Materials and methods
A single center retrospective analysis was conducted on 37 patients who underwent Magseed localization followed by BCS between November 2022 and June 2024 at our Breast Unit.
All patients enrolled in this study had non-palpable breast lesions identified on imaging at our institute by screening mammography followed by digital tomosynthesis and ultrasound examination or preventive examinations with combined mammography and ultrasound scan.
The utilization of Magseed localizers was determined through multidisciplinary meetings between radiologists and surgeons of the Breast Unit.
The localization procedure involved percutaneous placement of the Magseed into the target lesion after skin disinfection and administration of local anesthetic.
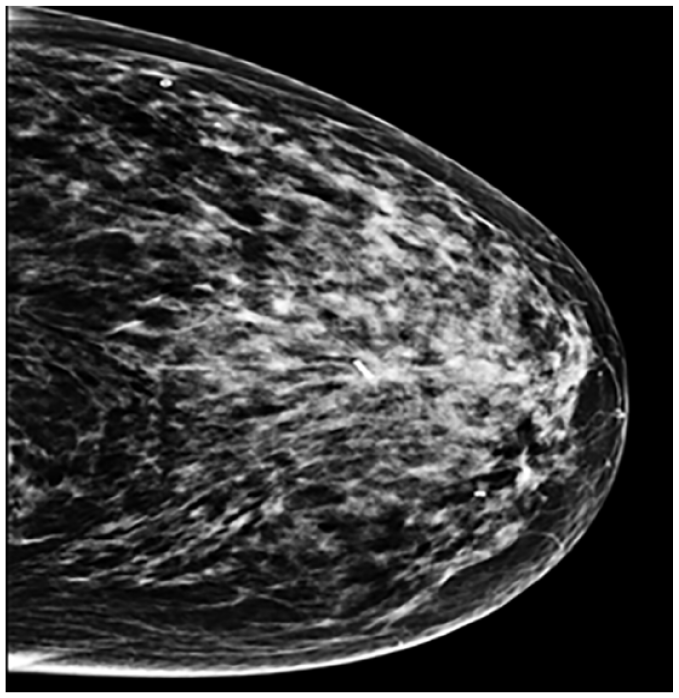
Magseed localization was performed under ultrasound (66%) Figure 1 or stereotactic (34%) guidance by one of our four qualified breast radiologists with more than 15 years of experience.

Ultrasound guided Magseed pre-operative localization.
Correct positioning of the marker was assessed immediately after its introduction by mammography Figure 2 with two projections (cranio-caudal and mid-lateral oblique).
Sentimag probe.
The surgical procedure employed the SentiMag probe Figure 3, which uses an audio signal that varies in intensity based on the distance between the marker and the probe, as well as the strength of the magnetic field, to precisely locate the non-palpable lesion for removal.

Correct positioning on pre-operative Mammography.
At the conclusion of the surgical procedure, a mammogram on the surgical specimen was performed to confirm the presence of the Magseed in the excised tissue Figure 4 and to measure the distance between the lesion and the surgical margins. Intraoperative widening was considered if the lesion was detected at the margin of the surgical specimen by breast radiologists.
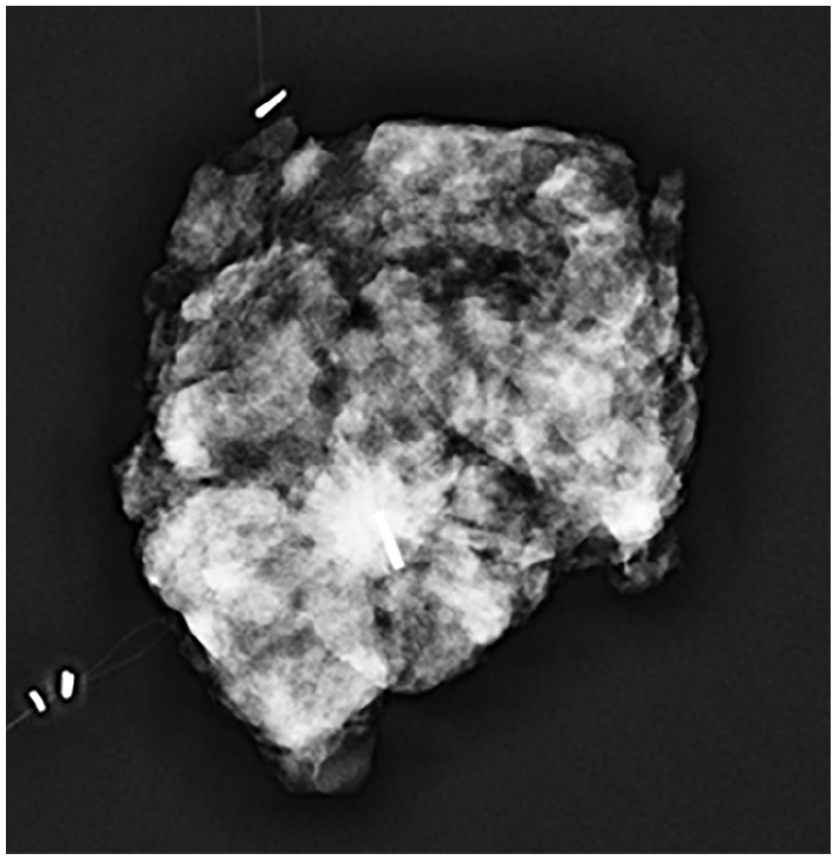
Centered magseed on surgical specimen.
Data on patient demographics, lesion characteristics, Magseed localization and retrieval, surgical outcomes and complications were collected and analyzed.
Results
The study included a total of 47 patients, with a mean age of 58.4 years (range 35–85).
The average size of the breast lesions before surgery was 10.3 mm (range 5–28).
Magseed localization was successful in all cases, with no instances of migration or dislodgment of the marker.
All magnetic seeds were successfully retrieved from the surgical specimens (100%).
Almost all patients (97.9%) underwent successful BCS with clear margins on final pathological assessment. Only one patient (2.1%) required re-excision due to close margins.
No significant complications related to Magseed localization or surgical intervention were reported.
Postoperative histopathological analysis revealed predominantly invasive breast cancers, with No special type (NST) being the most common histological subtype (42.5%), followed by B3 lesions (21.2%), ductal carcinoma in situ (DCIS) (19.1%), invasive ductal carcinoma (IDC) (8.5%) and invasive lobular carcinoma (ILC) (8.5%).

Discussion
Our single experience with Magseed localization demonstrates its effectiveness and reliability as a localization technique for guiding BCS and our results reflect the data in the scientific literature on Magseed.
The high success rate of complete tumor excision with clear margins (97.4%) reflects the accuracy and precision afforded by Magseed localization.
Gera et al. demonstrated the effectiveness of localization of non-palpable breast lesions with Magseed through a systematic review and pool analysis of 1559 procedures from 16 studies. The successful localization rate was 99.86% and the re-excision rate was 11.19%. 12
D’Angelo et al performed a retrospective single-center study to evaluate efficacy and accuracy for preoperative localization of non-palpable lesions using Magseed with a cohort of 45 patients.
Their data demonstrate a highly successful placement rate (97.8%) with a re-excision rate for positive margins of 0%. Only one procedure experienced clip migration. 13
In our study, with a similar cohort of patients, we did not encounter any migration, but we had one case of intraoperative widening due to positive margins.
Crèvecoeur et al performed a retrospective study on a cohort of 100 patients with localized breast lesions using the Magseed system. Five patients had multiple lesions for which more than one Magseed was introduced into the breast.
Their results on the placement rate and re-excision rate are also in line with existing data from the literature, additionally they demonstrated the feasibility of targeting multiple lesions in the same breast. 14
Compared to traditional WGL, Magseed offers several advantages including improved patient comfort, reduced logistical challenges, and enhanced accuracy in identifying and excising non-palpable breast lesions.15–17
Although our study has limitations due to the single-center experience and the small cohort of patients, the low rate of re-excision in our study further underscores the clinical utility of Magseed in achieving oncologically sound surgical outcomes.
Conclusion
In conclusion, Magseed localization represents a valuable addition to the armamentarium of techniques for guiding BCS in patients with non-palpable breast lesions. Our experience highlights the efficacy, safety, and feasibility of Magseed as a preoperative localization method, with excellent surgical outcomes.
Further studies with larger cohorts and longer follow-up periods are warranted to validate and establish Magseed as a standard practice in BCS. Nonetheless, our initial experience supports the integration of Magseed into clinical practice as a reliable localization technique for optimizing surgical management of non-palpable breast lesions.
Footnotes
Author contributions
Conceptualization, S.C. and A.C.L.G.; formal analysis, L.G. and M.C.G.; investigation, A.C.L.G, L.G and M.C.G; data curation, L.G. and M.C.G; writing—original draft preparation, L.G. and M.C.G.; writing—review and editing, S.C, L.G and M.C.G; visualization, A.C.L.G and M.C.G; supervision, S.C and A.C.L.G. All authors have read and agreed to the published version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Informed consent was collected for every participant.