
Abstract
Objective
This study was designed to compare the margin clearance and re-excision rates of ultrasound (US)- and wire-guided excision in a large number of patients with nonpalpable breast cancer.
Methods
In total, 520 women who were histologically diagnosed with nonpalpable breast cancer were recruited in this study. All nonpalpable lesions were visible by US. The patients were randomly divided into two groups: those who underwent wire-guided breast-conserving surgery (BCS) and those who underwent US-guided BCS. Re-excision rates and positive surgical margins were recorded.
Results
A total of 262 patients underwent US-guided excision and 258 patients underwent wire-guided excision. No differences were found in tumor or patient characteristics. The positive margin rate was 4.6% in the US-guided group and 19.4% in the wire-guided group with a significant difference. Age, menopausal status, excision volume, histological grade, and tumor type significantly influenced the positive surgical margin rate. The intraoperative re-excision rate was significantly lower in the US-guided group than wire-guided group (11.1% vs. 24.0%, respectively).
Conclusions
US-guided BCS seems to be more effective than wire-guided BCS for treatment of nonpalpable breast cancers in terms of the margin clearance and re-excision rates. Patients can avoid the discomfort caused by preoperative wire placement.
Keywords
Introduction
With the introduction of screening programs for breast cancer, the median tumor size has greatly decreased. More than one-third of breast cancers are estimated to be nonpalpable in surgical practice. 1 Breast-conserving surgery (BCS), which is as safe and effective as mastectomy, has become a common surgical modality for early breast cancer. 2 The incidence of inadequate (close or positive) excision margins ranges from 5% to 60%. 3 Patients sometimes agree to undergo re-excision to reduce the recurrence rate of ipsilateral breast cancer and obtain clear pathologic margins.
Various localization methods are used to obtain adequate surgical margins, including wire-guided, palpation-guided, and radio-guided excision. 4 Wire-guided excision is the current treatment method for nonpalpable breast cancers. The surgeon’s experience and the radiologist’s accuracy in guidewire placement will influence the resection of nonpalpable breast cancer. Wire-guided excision is frequently inadequate; approximately 20% of patients still need to undergo a second surgical treatment despite the breast cancer being diagnosed before surgery. 5 Additionally, preoperative placement of a guidewire is uncomfortable for the patient, which increases the patient’s anxiety about the operation. 6
Ultrasound (US) has been extensively applied to image-guided breast biopsy procedures.7,8 Intraoperative US was first used as an alternative means to detect nonpalpable breast cancers in BCS in the late 1980s. 9 The surgeon can use US to visually remove the nonpalpable malignancy and obtain adequate margins. 10 The security and feasibility of this method have been tested by several groups, but only a few patients were included, and the advantages of US-guided BCS remain controversial.11,12 The aim of this study was to compare the margin clearance and re-excision rates of wire- and US-guided BCS in a large number of patients with nonpalpable breast cancer.
Patients and methods
Patients
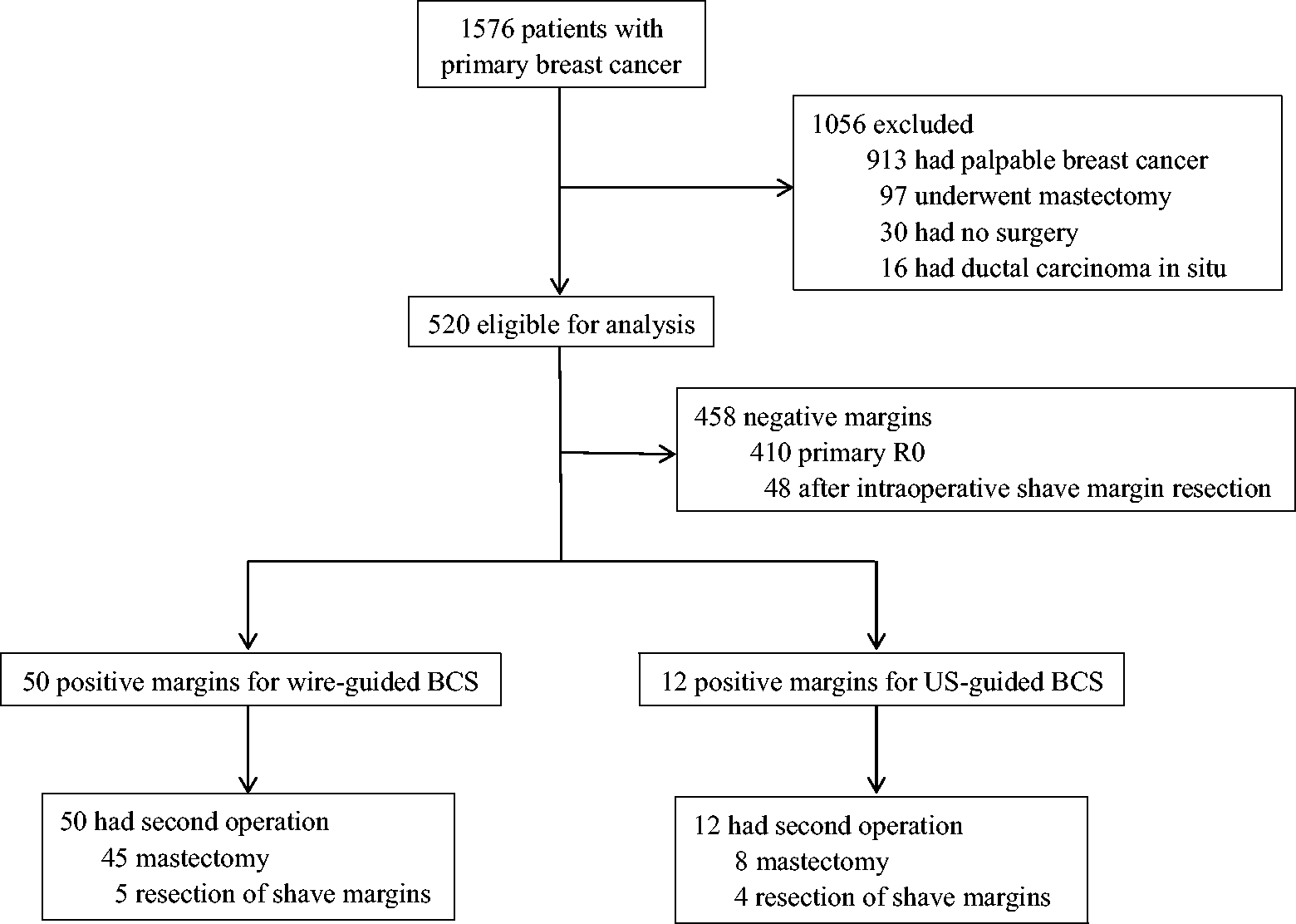
This study was designed according to the Declaration of Helsinki and was approved by the Ethics Committee of the Affiliated Tumor Hospital of Guangxi Medical University (IRB number: 2017-151). Patients who were diagnosed with and treated for primary breast cancer from June 2010 to January 2015 at the Affiliated Tumor Hospital were included in this study. Patients with an established diagnosis of nonpalpable breast cancer willing to undergo BCS were eligible for analysis. The patients were enrolled in the study only when US clearly displayed nonpalpable breast cancer. We excluded patients with palpable tumors, patients undergoing mastectomy, patients with ductal carcinoma in situ, and patients treated without surgery. These patients were randomized into two groups: those who underwent standard wire-guided BCS and those who underwent US-guided tumor excision. The patients were randomized based on a random number table. All patients were informed of the US- and wire-guided procedures in detail, and all provided written informed consent to participate in the study. The details of the study design are shown in Figure 1.
Study design. BCS, breast-conserving surgery; US, ultrasound.
Surgery
Five surgeons and three radiologists from the Affiliated Tumor Hospital of Guangxi Medical University participated in the study. The patients were grouped into US- and wire-guided excision groups according to the localization method. In the wire-guided group, a dedicated radiologist used US to place wires the day before surgery (Figure 2). Repeat mammography was used to verify all wire positions. The operation was performed by an experienced oncological breast surgeon. During the operation, the tumor was excised using the wire for localization. After tumor resection, all specimens were sent to the radiology department for mammographic confirmation (Figure 3). When suspicious surgical margins were found in the specimen radiographic examination, additional intraoperative resection of the shave margins was performed from the excision cavity.

Ultrasound guidance was used to place wires.

Mammographic confirmation of the specimen.
In the US group, the surgeon used a portable 14-MHz US probe (Toshiba Viamo; Toshiba, Tokyo, Japan). The location of the tumor was observed by US before the operation began (Figure 4). A sterile skin marker was used to mark the excision borders. The distance from the tumor to the muscular layer and depth from the skin was detected by US to evaluate the extent of surgical resection. The tissue was then resected perpendicularly to the chest wall in a cylindrical manner. During surgery, palpation and US examination of the cavity and remaining breast were performed to exclude further tumor foci. After tumor removal, ex vivo US examination of the specimen was immediately performed to confirm the presence of the tumor in the resected specimen. The specimen was also examined by X-ray after surgical excision. The surgeon measured the distance between the lump and the resection margin in all directions. If a suspicious surgical margin was observed, re-excision of the shave margins was immediately performed.

Ultrasound image of the tumor.
In both groups, titanium clips were placed at the lumpectomy site for radiotherapy treatment. The specimen was examined by an experienced pathologist after excision. Repeat excision was performed in a second operation when the initial surgical specimen was found to have positive surgical margins. The total resection volume was obtained by summing the volume of the original surgical resection specimen and the margin of intraoperative re-excision, which was measured by the pathologist.
Pathology
All specimens were sent to the pathologist and measured in the pathology department. The size of the tumor was first measured after the specimens were carefully inked and cut. The surgical margins were evaluated based on current Dutch breast cancer guidelines: negative, margin distance of ≥4 mm; positive, margin distance of <4 mm or tumor cells present at the inked edge of the specimen.
Statistical analysis
SPSS 17.0 (SPSS Inc., Chicago, IL, USA) was used for the statistical calculations. The different pathological variables between the two groups were compared using Fisher’s exact test or the chi-square test. The mean of nonparametric variables was compared by variance analysis. A P value of <0.05 was taken to indicate statistical significance in all analyses.
Results
Patient and tumor characteristics
From June 2010 to January 2015, 1576 patients with primary breast cancer at our hospital were enrolled in this study. A total of 1056 patients were excluded because they had palpable breast cancer (n = 913), underwent mastectomy for nonpalpable breast cancer (n = 97), did not undergo surgery (n = 30), or had ductal carcinoma in situ (n = 16) (Figure 1). The remaining 520 patients were randomly assigned to undergo either wire-guided BCS (n = 258) or US-guided BCS (n = 262).
The patient and tumor characteristics are shown in Table 1. The mean age of the patients was 59 years in the wire-guided group (range, 38–72 years) and 63 years in the US-guided group (range, 27–74 years). The median tumor size was similar in the two groups. The mean excision volume was 96 mm3 in the wire-guided group and 92 mm3 in the US-guided group, with no statistically significant difference. No screening items showed a significant difference between the two groups.
Patient and tumor characteristics.

Data are presented as mean ± standard deviation or n (%).
US, ultrasound; ER, estrogen receptor; PR, progesterone receptor; HER-2, human epidermal growth factor receptor 2.
Tumor margins
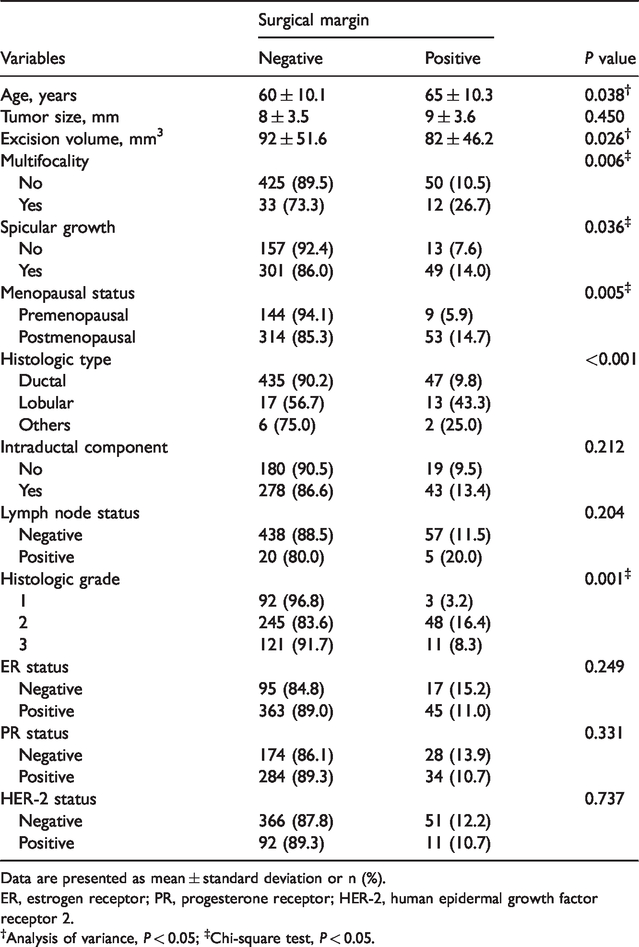
The influence of the patient and tumor characteristics on the surgical margins was first studied by US examination. The margin state is summarized in Table 2. Most tumors (88.1%) had a negative surgical margin. Age, menopausal status, excision volume, histological grade, and tumor type significantly affected the positive surgical margin rate (Table 2). Positive surgical margins were more likely to occur in postmenopausal women of advanced age (P = 0.005). Multifocality (P = 0.006) and spicular growth (P = 0.036) were more closely associated with positive surgical margins. The excision volume (P = 0.026), tumors with intermediate-grade differentiation (P = 0.001), and tumors of lobular histologic type (P < 0.001) were also associated with a higher risk of positive resection margins.
Margin status.
Data are presented as mean ± standard deviation or n (%).
ER, estrogen receptor; PR, progesterone receptor; HER-2, human epidermal growth factor receptor 2.
†Analysis of variance, P < 0.05; ‡Chi-square test, P < 0.05.
Margins after US-guided versus wire-guided resection
Of all 262 US-guided resections, 12 (4.6%) tumors had positive margins and 250 (95.4%) had negative margins. These rates for wire-guided resections were 50 (19.4%) and 208 (80.6%), respectively (Table 3). Therefore, the effect of US-guided resection was significantly better than that of wire-guided resection (95.4% vs. 80.6%, respectively; P < 0.001).
Margins after US-guided versus wire-guided resections.

Data are presented as n (%).
US, ultrasound.
Tumor localization
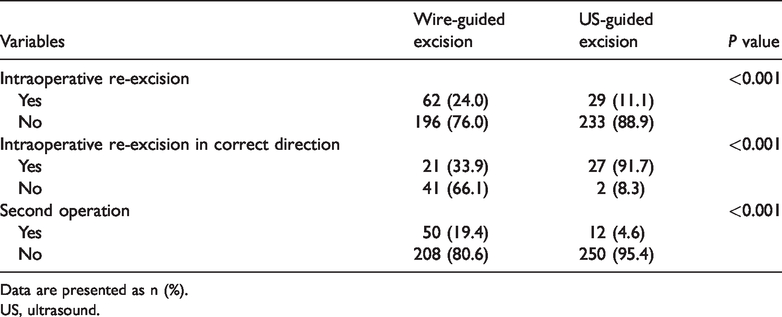
The shaving rate (intraoperative re-excision) was significantly higher in the wire-guided than US-guided BCS group (24.0% vs. 11.1%, respectively; P < 0.001). The shave margins were removed under the guidance of US or specimen radiography, respectively. Among patients who underwent additional shave margins, histologic examination of the shave margins showed that the problematic margin was correctly identified by intraoperative US-guided re-excision in 27 (91.7%) of 29 cases. In the wire-guided BCS re-excision group, the shave margins were able to be excised in the correct direction in only 21 (33.9%) of 62 cases (P < 0.001). There was also a significant difference in the re-excision rate via a second operation between the two groups (P < 0.001) (Table 4). Twelve (4.6%) of 262 patients in the US-guided group and 50 (19.4%) of 258 patients in the wire-guided group underwent a second operation. In the US-guided BCS group, four women underwent re-excision during the second operation and eight women underwent a mastectomy. In the wire-guided BCS group, five women underwent re-excision during the second operation and 45 women required a mastectomy to prevent recurrence (Figure 1).
Tumor localization and re-excision rates.
Data are presented as n (%).
US, ultrasound.
Discussion
BCS combined with adjuvant radiation is a common treatment method for early breast cancer and is as effective and safe as mastectomy. 2 However, the main difficulty facing surgeons is still the achievement of clear surgical margins. Research has proven that positive resection margins are closely associated with local recurrence. 13 If the surgical margin is positive, mastectomy or re-excision must be performed, which is uncomfortable for patients and increases the cost of hospitalization.14,15 Therefore, to reduce the risk of local recurrence and the re-excision rate, it is particularly important to obtain a clear surgical margin intraoperatively.
US-guided breast surgery is a promising method of obtaining clear surgical margins.16–18 US can be used as a localization method before BCS or after mastectomy to confirm the existence of tumors in the specimen.19,20 However, many of these studies have been limited by a small sample size or a retrospective design with the potential risk of recall bias. Therefore, the effect of US-guided BCS has been controversial. In a randomized controlled study, Krekel et al. 21 demonstrated the effect of US-guided breast surgery in the treatment of palpable breast cancer. In total, 134 patients with palpable breast cancer were recruited in their study and randomly assigned to either palpation- or US-guided BCS. Of the 69 patients in the palpation-guided group, 12 (17%) had positive resection margins; in contrast, of the 65 patients in the US-guided group, only 2 (3%) had positive margins (P = 0.009). The results of US-guided resection in the present study were similar to these.
With the development of technology, nonpalpable breast cancer can be detected increasingly earlier. Early detection was achieved in 520 patients in this study. The use of intraoperative US is an alternative way to detect nonpalpable breast tumors. 22 In previous studies, the re-excision rate of US-guided surgery for nonpalpable breast cancer ranged from 3% to 9%.23,24 The use of intraoperative US provides a significant benefit for the surgeon because it facilitates immediate assessment of the resection margins. 25 A recent retrospective study showed that in 85.7% of patients, US-guided BCS had sufficient surgical margins, which was in accordance with our study. 3 The shave margins were re-excised using US in 27 patients. Therefore, these 27 patients were able to avoid reoperation because of the use of intraoperative US. The positive margin rate was thus reduced from 14.9% (39/262 cases) to 4.6% (12/262 cases). Similar results have also been obtained in retrospective 21 and prospective studies.20,26 Multifocality, spicular growth, a small resection volume, and postmenopausal status increase the risk of positive resection margins.
One of the major issues discussed in the current study was the comparison of wire-guided BCS with other methods, including US-guided BCS or radio-guided localization of occult lesions. The effect of US- and wire-guided BCS on resection margins has been evaluated in three similar studies.27–29 James et al. 29 demonstrated a statistically significant difference in the positive surgical margin rate between wire- and US-guided surgery (17% vs. 6%, respectively; P = 0.030). Other studies showed that the clear surgical margin rate in US-guided surgery was 90.0%, while that in wire-guided surgery was 78.2%;28,30 this is in agreement with our data. Notably, the rate of a second operation to achieve adequate margins was also significantly different between the two techniques, which is consistent with our results. 31
It can be speculated that surgeons must excise more tissue to obtain a clear surgical margin. Interestingly, this hypothesis was overturned in our study. US-guided BCS had more adequate resection margins, but the mean excision volume was not significantly different from that of wire-guided BCS (92 vs. 96 mm3, respectively). This not only facilitates the surgery but also improves the cosmetic effect of BCS. The resected tissue volume has been shown to be inversely related to the cosmetic results. 32
One study confirmed that US-guided BCS has the advantage of a low re-excision rate for patients with nonpalpable breast cancer, but the sample size was small. 11 In the present study, intraoperative re-excision was performed in 24.0% of wire-guided resections, which was higher than that of US-guided excisions (11.1%). The surgeon could properly identify the problematic margin with US in 91.7% of cases. Only 33.9% of cases were properly resected in the wire-guided BCS group. These findings are similar to the results of US-guided BCS for palpable breast cancer in terms of the margin status and re-excision rate. 33 Therefore, intraoperative US can be used to detect positive surgical margins and is a safe and sensitive method.
Another advantage of more exact resection is that patients need not undergo a second surgery. In such cases, the patient’s health condition can be improved and the hospital costs will be reduced. In one study, the rate of pathologically adequate surgical margins was improved when the distance between the resection margin and tumor edge was measured. 22
The design of US-guided BCS is to achieve the current trend of BCS. According to the present study and literature review, US-guided BCS is a feasible, effective, and reproducible procedure with good sensitivity. It is also easy to perform and can reduce hospital costs.34–36 US-guided localization had lower costs than and a shorter preoperative wait time than wire-guided localization. It could be used as an alternative to wire-guided localization in preoperative marking of nonpalpable breast lesions. 37
A limitation of our study is that we did not perform a logistic regression analysis to determine the relative contributions of various risk factors to positive margins. Another is that we did not evaluate the cosmetic outcome, the rate of tumor recurrence, or patient satisfaction with these procedures. However, a major advantage of this study is that the tumor characteristics and patients were equally distributed between the two groups, which helps to avoid selection bias. The large number of patients recruited in our research could improve the external validity of this study.
In conclusion, when nonpalpable lesions are visible by US in patients with breast cancer, it seems that US-guided lumpectomy is superior to wire-guided resection with respect to margin clearance. This will reduce the rate of a second operation for re-excision. In addition, patients can avoid undergoing unpleasant wire placement before surgery. Finally, US-guided BCS allows the surgeon to be independent of the pathologist or radiologist and may become a standard surgical procedure.