
Abstract
Background:
Stunting is a significant concern in Indonesia, but its detection currently relies on anthropometric measurements, lacking the integration of comprehensive evaluations of child development. Therefore, the Child Development Card (KKA) serves as a valuable instrument employed to assess the growth and developmental aspects of children.
Aim:
This research aimed to investigate the potential of KKA as a discriminative tool for distinguishing between stunted and normal children.
Methods:
The participants consisted of 159 and 88 normal and stunted children aged 13–24 and 25–60 months. The aspects of children’s development examined included passive communication, social behavior, gross motor skills, active communication, fine motor skills, intelligence, and self-help skills. Discriminant analysis was conducted to identify the developmental aspects differentiating stunted children from normal children.
Results:
The analysis using SPSS 25 showed that the discriminating aspects of children’s development between stunted and normal children were gross motor skills, fine motor skills, passive communication, and intelligence. For the age group of 13–24 months, the discriminant function is represented as D = − 0.276 + 0.197 K - 0.511 GK + 0.361 KP. Meanwhile, for the age group of 25–60 months, the discriminant function is expressed as D = − 2.586 + 0.151 GK – 0.081 GH.
Conclusion:
Stunted and normal children could be differentiated based on four key aspects of development: gross and fine motor skills, passive communication, and intelligence. These findings aid in the early detection of stunted children and emphasize the crucial role of parental stimulation across these four aspects.
Introduction
Stunting poses a significant national challenge presently encountered by Indonesia. It pertains to the phenomenon of malnutrition in infants within the initial 1000 days of their lives, resulting in enduring setbacks in child growth and development. 1 Malnutrition during early childhood can hinder physical and mental development and result in death. Stunted children are at risk of experiencing decreased intellectual ability, productivity, and potential degenerative diseases in the future. 2
According to the Indonesian Nutritional Status Study (SSGI) in 2021, the prevalence among Indonesian children is 24.4%. Even though there has been a decrease in this statistic compared to previous years, it remains considerably distant from the target established by the National Medium-Term Development Plan (RPJMN), which sets forth the objective of achieving a prevalence rate of 14% by 2024. 3
The causes and risk factors of stunting can be categorized into three factors, namely (1) poor caregiving practices, (2) limited awareness among the community in using healthcare services, and (3) lack of access to nutritious food. 4 The first factor includes mothers’ lack of knowledge, and failure to provide exclusive breastfeeding to infants aged 0–6 months as well as complementary feeding (MP-ASI) to infants. The second contributing factor encompasses pregnant women who fail to adhere to a 90-day iron tablet (Fe) consumption regimen and children aged 3–6 years who are not enrolled in Early Childhood Education (PAUD). Consequently, this leads to inadequate monitoring of their growth and development, and the third factor includes anemia in pregnant women and the high cost of nutritious food.
Stunting detection has been primarily conducted through anthropometric measurements, including height/length, weight, as well as arm and body circumference. 5 Even though the conventional anthropometric definition of stunting (height-for-age z-score below −2 standard deviations) was originally devised as a statistical indicator of the societal and economic deprivation experienced by children at the population level, it has become commonly employed to delineate cases of chronic malnutrition. 6 There is no biological basis for the −2 standard deviation (SD) cutoff to define stunting, making it a poor individual-level classification of malnutrition or disease. 7 Therefore, short stature does not necessarily indicate health or developmental issues in children. 8 Stunting measurements in children need to be complemented with other methods, such as assessing children’s development using a Child Development Card (KKA).
A small portion of stunted children are assessed based on their development and KKA is used to monitor parental caregiving activities and children’s development. It serves a dual function as a monitoring and communication tool for discussing child development between healthcare workers/community health volunteers and mothers/families of children. 9 In addition, KKA was developed by the National Population and Family Planning Board (BKKBN) in 1988, a usage guideline was published in 2010, and an online version was launched in 2021. KAA includes seven aspects of development, which are gross motor skills, fine motor skills, passive communication, active communication, intelligence, social behavior, and self-help skills. 9
KKA has been used in the field but lacks empirical evidence that shows a comparison between the development of stunted and normal children. This comparison is important to identify the distinctive developmental patterns of stunted children compared to normal. Furthermore, understanding the distinctive developmental patterns of stunted children can serve as a reference for optimizing the aspects of development. The measurement results can also be used as a basis for designing appropriate stimulation or therapy for both individuals and groups of stunted children. The prevention and management of stunting are not solely focused on nutrition intake but also on providing appropriate stimulation to children.10,11 Previous research 12 also showed that integrated programs involving stimulation successfully reduced the proportion of stunted children. Therefore, it is important to identify which aspects of development differentiate between normal and stunted children.
Methodology
The participants consisted of 159 normal children and 88 stunted children aged 13–24 and 25–60 months from three regencies in West Java: Sumedang, Tasikmalaya, and Ciamis regencies. Within these three regencies, one sub-district serving as the locus of stunting was selected, resulting in the identification of the sub-districts Jatigede, Ciawi, and Sindangkasih. Data collection was randomly conducted from these three sub-districts, which are the focal points for stunting.
The KKA is fundamentally structured according to developmental stages: 0–6, 7–12, 13–24, and 25–60 months. However, the categorization into two groups, specifically 13–24 and 25–60 months, is implemented because children under 13 months have not yet displayed all the intended measured abilities. Details of participant’ characteristics can be seen in Table 1. Therefore, measurements are only taken within the age ranges of 13–24 and 25–60 months because within these age ranges, all aspects of abilities are evident. Consequently, the sample only comprises children aged 13–24 and 25–60 months.
Participants’ characteristics.
Each participant’s growth and development were measured using KKA 9 , which consisted of 46 items as listed in Table 2, measuring seven aspects, namely:
Gross motor skills (six items) refer to the aspect of development where children perform movements involving large muscle groups and require energy.
Fine motor skills (six items) are movements performed by specific body parts and involved small muscle groups. Children do not require much energy for these movements.
Intelligence (11 items) refers to the ability to comprehend, think, remember, and solve problems.
Passive communication (five items) is the ability to understand signals and speech from others.
Active communication (nine items) is the ability to express feelings, desires, and thoughts through crying, body movements, or speaking.
Social behavior (three items) refers to the ability to interact and socialize. This includes interacting and behaving with family members and others in their environment.
Self-help skills (six items) refer to the ability and skills to perform simple tasks related to their daily life.
Child Development Card (KKA) items.

KKA was measured by directly observing children in their developmental aspects. This research used KKA, which has been categorized based on the developmental aspects, and uses an observation guide. The guide consisted of instructions to be given to mothers and children, success indicators, targeted behaviors, operational behaviors, required equipment, and measurement procedures for each behavior. 13 The guide was developed according to the developmental aspects based on children’s age.
Children are given a score of 1 when the targeted behavior can be performed and a score of 0 when it cannot. Subsequently, the dataset underwent discriminant function analysis, a statistical technique used to determine the variables that differentiate or separate between two or more groups. This technique aims to find the best linear combination of variables that distinguishes between these groups. The goal is to identify which variables contribute the most to the classification or discrimination between different groups. 14 In this research context, discriminant analysis was conducted to determine the developmental aspects differentiating stunted children from normal children.
Results
Tables 3 and 4 illustrate the overview of growth and development in stunted and normal children aged 13–24 and 25–60 months based on univariate analysis. In the 13–24 months age group, aspects of social behavior and intelligence exhibit significant values. Meanwhile, in the 25–60 month age group, all aspects show significant values. However, after conducting a discriminant function analysis, a discriminant function was discovered for the 13–24 month age group as D = −0.276 + 0.197 K−0.511 GK + 0.361 KP. While for the 25–60 month age group, it was found as D = −2.586 + 0.151 GK–0.081 GH. This implies that the growth and development aspects predicting a child’s tendency toward stunted are intelligence, gross motor skills, and passive communication in the 13–24 month group, and gross motor skills as well as fine motor skills in the 25–60 month group.
Growth and development of stunted and normal children 13–24 month.
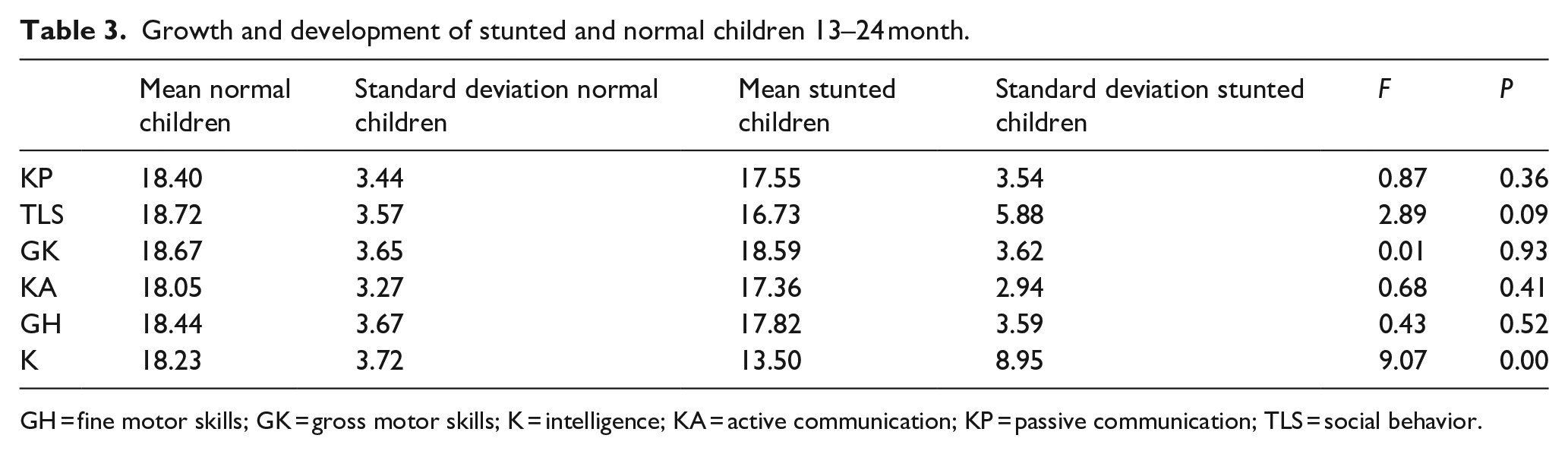
GH = fine motor skills; GK = gross motor skills; K = intelligence; KA = active communication; KP = passive communication; TLS = social behavior.
Growth and development of stunted and normal children 25–60 month.

GH = fine motor skills; GK = gross motor skills; K = intelligence; KA = active communication; KP = passive communication; MDS = self help; TLS = social behavior.
Discussion
Discriminant factors in growth and development of stunted and normal children aged 13–24 months
The discriminant analysis indicated that the discriminating factors for stunted children are gross motor skills, passive communication, and intelligence. This aligns with WHO 15 where stunting can cause developmental impairments in gross and fine motor skills, language abilities, and social skills.
The findings show that gross motor skills are the most distinguishing aspect of development in identifying stunted children. The specific skills referred to are walking independently and kicking a ball without support. Furthermore, they are associated with compromised growth potential in children, usually caused by insufficient nutrition. In cases of children from low socioeconomic backgrounds, the frequency of breastfeeding and the provision of breast milk substitutes tends to be low, and the incidence of infectious diseases is high. 16
Passive communication is also a differentiating aspect of development in identifying stunted children. The abilities in question encompass the identification of three body parts, as well as the recognition and naming of three pictures. This observation aligns with the findings of Nahar et al., 17 where stunted children exhibit inferior communication skills in comparison to their non-stunted counterparts.
Intelligence is also an aspect of development that can distinguish stunted children. The aspects include the ability to pour a drink using a spoon, providing three objects and correctly naming them, and successfully stacking five objects without toppling. The findings are in line with previous research, 18 indicating that children experiencing stunting demonstrate lower intelligence scores compared to non-stunted children. This leads to the conclusion that stunting adversely affects children’s cognitive abilities.
Discriminant factors in growth and development of stunted and normal children aged 25–60 months
The discriminant analysis indicates that the discriminating factors for stunting are gross and fine motor skills. These results show that gross motor skills in children aged 25–60 months are the most distinguishing aspect of development in identifying stunting cases. The specific skills are standing on the tips of both feet and dancing to music. This is consistent with research findings on children aged 3–65 months, where acute nutritional disorders are associated with delayed development of gross motor skills, fine motor skills, social interaction abilities, and language development. 19
Additionally, fine motor skills are a differentiating aspect of development in identifying stunting. The skills referred to are inserting and removing small objects. These results align with the research on 525 children, showing a significant relationship between stunting and impaired fine motor skills in under 5 years old. 20 In a similar finding, stunted children have poorer fine motor skills. This research shows that stunting can have a negative impact on the fine motor skills of young children, affecting their future development.21,22
Based on the explanation, gross motor skills are a strong discriminant factor for distinguishing stunted children in the age groups of 13–24 and 25–60 months. The skills are directly influenced by anthropometric factors, which determine stunting. This is a foundational aspect of development that contributes to other aspects, such as play activities and socialization. Furthermore, gross motor skills build self-confidence while engaging in environmental activities. Kartika et al. 23 also reported a relationship between stunting and gross motor development. Stunted children are likely to have 5.02 times the risk of experiencing impaired gross motor development compared to normal children. This is often due to the presence of malnutrition, which affects the development of the cerebellum, the area of the brain responsible for motor control. This phenomenon also hinders the formation and maturation of muscle tissue, resulting in stunted children having slower acquisition of motor skills and weaker muscles.
Children aged 0–5 years learn and acquire abstract concepts through physical exploration involving gross and fine motor skills. Therefore, impaired gross motor skills hinder the development of fine motor skills, as well as the exploration of the environment in children. This limits experiences, such as feeling textures, comparing sizes, and planning movements. The limited development of environmental experiences restricts thinking abilities, which ultimately affects passive communication. In line with previous research, stunted children experience delays in language development, making it difficult to express their desires, needs, thoughts, and ideas. Consequently, they interact with others through body movements or passive communication. 17
Conclusion
Based on the discriminant function analysis and the discussion presented, four aspects of development can distinguish stunted children. These aspects are gross motor skills, fine motor skills, passive communication, and intelligence. These findings serve as valuable tools for early identification of a child’s susceptibility to stunting. Consequently, parental stimulation in these four areas is paramount for the developmental progress of stunted children, commencing from their birth.
Recommendations
To optimize the development of stunted children, it is recommended to promptly provide stimulation for the enhancement of their gross motor skills, fine motor skills, passive communication, and intelligence. Examples of stimulation that can be provided to enhance gross and fine motor skills include facilitating head support by placing children on their stomachs and engaging them with toys, promoting body tilting by producing sounds with a toy to prompt leaning, and allowing grasping and holding of objects in front. After children have acquired the fundamental abilities within the 0–6 month age range, they will progress to developing additional skills, including sitting, standing, walking, and gaining control over their body movements to maintain balance. Examples of stimulation for passive communication and intelligence include engaging in contact by following a toy with their eye gaze and attributing meaning to simple movements, such as waving, saying goodbye, and clapping hands.
Footnotes
Acknowledgements
We would like to extend our gratitude to all the study participants and the organizations that help us, namely Matching Fund Kedaireka, in collaboration with the Directorate General of Higher Education, Ministry of Education and Culture with the National Population and Family Planning Agency (BKKBN).
Author contributions
Ratna Jatnika: Manuscript writing, method, data analysis, and research management.
Hendriati Agustiani: Theoretical concept, data collection, and research management.
Fitri Ariyanti Abidin: Theoretical concept and data collection.
Fitriani Yustikasari Lubis: Theoretical concept and data collection.
Kustimah Kustimah: Theoretical concept and data collection.
Lucia Voni Febriani: Theoretical concept and data collection.
Syauqiyyah Syahlaa: Manuscript writing.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Matching Fund Kedaireka, in collaboration with the Directorate General of Higher Education, Ministry of Education and Culture with the National Population and Family Planning Agency (BKKBN).
Ethical approval
The study was approved by The Research Ethics Committee Universitas Padjadjaran Bandung (registration number: 973/UN6.KEP/EC/2022).