
Abstract
The aim of this review was to assess the association between occupational exposure to silicon dioxide and chronic respiratory symptoms among workers in the cement manufacturing industries. Approximately 60 articles published from 2010 to 2021 were found and four independent reviewers extracted the data from each eligible study using PubMed, Google scholar etc. The following terms were used: exposure to cement dust, exposure to silicon dioxide etc. Inclusion and exclusion criteria were considered while searching for the studies. In this review, a total of 14 articles were included in this study. Chronic cough was the most prevalence exposure symptoms (OR 1.90; CI 9.90, 0.78), with wheezing reported to be the least experienced symptom (OR 1.34; CI 11.5, 0.50). Two studies reported exposure concentration ranging from 0.026 to 0.044 mg/m3, and 0.27 mg/m3 was also reported in one study. The FEV1 and FVC was lower in exposed workers when compared to the control group. Studies reported the crystalline silica quartz to be 21.5% in limestone, 22.5% in bauxite, 21.22% in clinker, and 21.22% in raw cement. Chronic cough, phlegm, wheezing, and shortness of breath or dyspnea was found to be significantly prevalence among workers, particularly cleaning personnel, in the cement manufacturing industries.
Introduction
The demand for cement has been growing each year as the number of infrastructures in developing countries increase. Cement is an essential element or material used mainly in civil engineering and many construction processes. Since some of the operations in the cement factories require manual handlings, workers are potentially exposed to the raw materials used in production stages. 1 Stages such as the processing of raw material, burning of clinker and grinding are involved in the cement industry for production. The production process involves quarrying, crushing, grinding, blending, packaging, and shipping of the finished products. 2 However, throughout the entire processes, particles of silicon dioxide escape and become airborne. The level of occupational exposure to silica particles depends on the machinery used for production, and availability of systems to suppress airborne dust concentrations. 3 High airborne concentration and prolonged of exposure to silica particles can result in the development of chronic respiratory symptoms.
Cement can be natural or artificial. Materials that are natural such as those that have cement like features are used as natural cement, and hydraulic cement powder is provided by grinding and calcining only. 2 There are different types of artificial cements with different chemical composition, quality, and usage. 4 Portland cement is one of the artificial cement. Raw materials such as limestone, chalk, and argillaceous materials are mixed well, placed in a kiln to fire them, and then grounded to fine powder to make Portland cement. 5 The Portland process have two stages namely clinker manufacturing and clinker grinding. 5 Portland cement is a grayish powder that has fine particles with an aerodynamic diameter that ranges from 0.05 to 5.0 µm, and it has <1% crystalline structure. 5 This type of cement is composed of tricalcium silicate (3CaO SiO2), dicalcium silicate (2CaO SiO2), tricalcium aluminate (3CaO Al2O3), and a tetra-calcium aluminoferrite (4CaO Al2O3Fe2O3). The chemicals composition of cement include calcium oxide (62%–66%), silicon dioxide (19%–22%), aluminum trioxide (4%–8%), ferric oxide (2%–5%), magnesium oxide (1%–2%), minute selenium, thallium, and other elements. 1 Silicon dioxide is a public health concern as it was found to be associated with the development of several respiratory symptoms and high mortality rate during occupational exposure events. 6 Occupation exposure to silicon dioxide in both developing and developed countries is still an occupational risk factor for chronic respiratory symptoms. 6 This review aimed to evaluate the relationship between occupational exposure to silicon dioxide and prevalence of chronic respiratory symptoms among workers in cement manufacturing industries. Previously published studies were assessed to accomplish the aim of this study.
Methodology
Protocol registration
This systematic review has not been registered in the international prospective register of systematic reviews (PROSPERO).
Methods
This desktop study was conducted to evaluate the association between occupational exposure to silicon dioxide and the prevalence of chronic respiratory symptoms in cement industry. Approximately 60 full-text articles were found prior deciding on inclusion and exclusion criteria. The electronic scholarly databases such as PubMed, Google scholar, research gate, Publons etc., were used to search for full-text articles published in an English language between 2010 and 2021. Keywords such as “cement dust,” “crystalline silica,” “occupational exposure,” and “chronic respiratory symptoms” were used.
In this review, a Practitioners of Evidence-Based Practice (PICO) was used to facilitate literature search. (i) Population (P) was accounted for as workers in the cement industry or exposed to silicon dioxide, (ii) Exposure (E) was used instead of Intervention (I). Exposure was limited only to workers exposed to silicon dioxide, (iii) the exposed group was compared with the Control population (C) included in the reviewed studies, and (iv) Outcomes of interest were chronic respiratory symptoms.
Inclusion criteria
Type of participants—all studies that involved cement industry workers of all age groups and gender were considered. Those who were regarded as directly exposed and unexposed to silicon dioxide were also included. Furthermore, participants who were regarded as smokers, non-smokers, sensitive groups, or workers with underlying conditions formed part of the study.
Types of studies—all cross-sectional studies that used quantitative design were considered in this systematic review.
Search strategy
All peer-reviewed articles were searched. The following databases were used: PubMed, MEDLINE, BMC, BMJ, Africa Wide, Cambridge University Press, Science Direct, Springer Link, Oxford Journals, AMED, CINAHL, research gate, Google scholar, Publons, and WHO library database. Only full-text articles published between 2010 and 2021 were searched.
Exclusion criteria
This review excluded studies conducted before the year 2010 and those that used qualitative research designs. Gray literature from internet sources, newspapers and magazines were also excluded. Articles that were not available as open access and needed to be purchased, also those that were not published in English language were excluded.
Data collection
To ensure reliability of data collection process, four independent academic reviewers extracted data from each eligible study. Any disagreement that occurred between the reviewers was resolved through discussions, and if no consensus were reached, a fifth additional reviewer was invited as a referee. The variables that were extracted include the year of study commencement, the country of origin, types of chronic respiratory symptoms (wheezing, chronic cough, shortness of breath, chronic phlegm, and difficulties in breathing), silicon dioxide exposure levels, characteristics of participants (age, gender, smoker, non-smoker, vulnerable individuals), and the cause of death amongst cement industry workers. PRISMA flow diagram and sample tables were used. For each study, the following was extracted: location, publication year, author, number of workers for both exposed and unexposed, exposure levels of silica dust, and the prevalence of chronic respiratory symptoms.
Data analysis
Data were first recorded in the Microsoft Excel (2016) spreadsheet to identify and remove duplications. Data in the excel were used to identify the odd ratios of the four chronic respiratory symptoms using the 2 × 2 contingency table. Odds ratios were calculated for each article used to at 95% confidence intervals. Furthermore, the forest graph were plotted to demonstrate prevalence of chronic respiratory symptoms.
Results
As shown in Figure 1, 2560 articles were searched from multiple databases and 65 of them were reviewed based on eligibility. A total of 59 studies were left after the removal of duplications. There were 35 full-text articles that were excluded for the following criteria: non-specific to prevalence of chronic respiratory symptoms (21), deaths in the cement industries (1), no free full access (1), was a case study (1), prevalence of acute respiratory illnesses (2), non-cement industries (6), pulmonary health risks (2), and no chronic respiratory symptoms found (1). The number of studies used to assess the prevalence of chronic respiratory symptoms were nine, and five studies were compared for workers exposure to high concentration of silicon dioxide.

The PRISMA flow diagram used for eligibility.
Eligibly articles for this systematic review were obtained from 14 studies published from 2010 to 2021. Nine studies with a total of 2091 study participants were used to extract data to find the association between the exposure to cement dust and the prevalence of chronic respiratory symptoms. Table 1 show studies that associated cement dust exposure with chronic respiratory symptoms. A comparison is made between the exposed populations and less exposed. The sample size ranges from 123 to 404. Two studies were conducted in Ethiopia, one study in Kongo, one study in Iran, one study in Indonesia, two study in Egypt, one study in Iraq, one in Nepal, and one study in Tamil Nadu. Five studies were eligible for the meta-analysis of chronic cough, nine studies for wheezing, six studies for phlegm, and eight studies for shortness of breath. Seven studies were cross sectional studies, one study included both a cross sectional and an analytical design and one study was a longitudinal study. The results of the aforementioned studies are demonstrated in tables below. Table 1 outline all studies that reported chronic respiratory symptoms within the cement mining industry.
Studies showing the prevalence of chronic respiratory symptoms.

Three study measured personal exposure levels to silica among 978 study participants. Table 2 outline the measured exposure levels of silica among the exposed and referent population in different occupational settings. Samples were taken in each department of the cement industry to determine the mean and standard deviation of airborne silica concentration.
Occupational exposure to silica dust in different departments in the cement manufacturing industry.

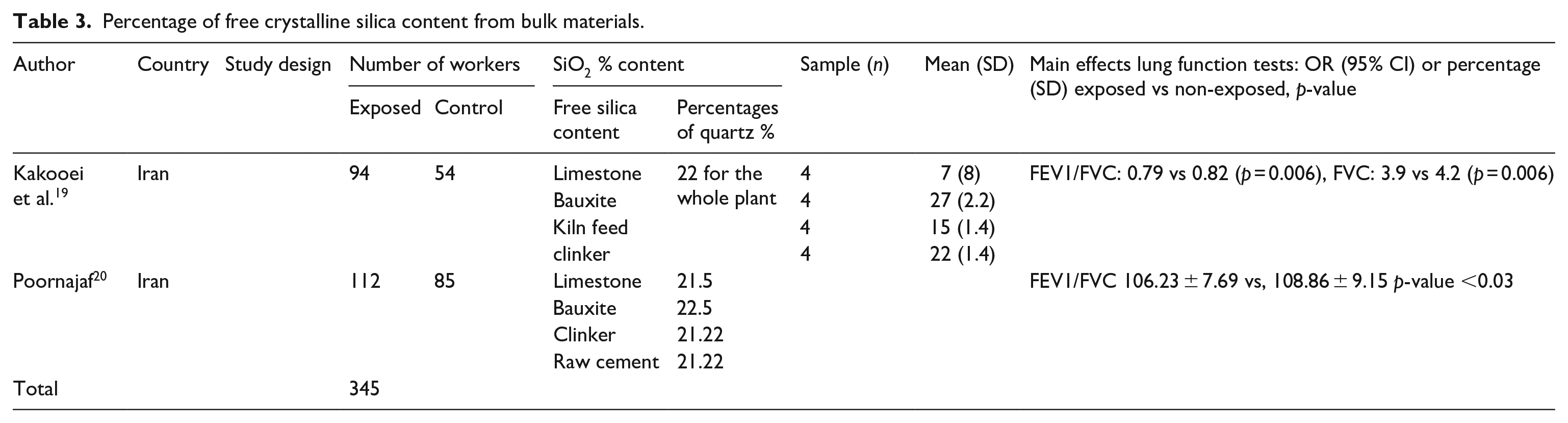
Table 3 shows two studies with 345 study participants measured the silica content in percentages as well as the comparison of lung functions between the exposed workers and referent group.
Percentage of free crystalline silica content from bulk materials.
Odd ratios were calculated using 95% CI for all eight studies that reported chronic cough from each study reported in Table 1. The results of each study are shown in Table 4 below.
The odd ratio and 95% confidence interval of chronic cough of each study.

The reported cases of chronic wheezing between exposed and referent groups were used to calculate odd ratios as shown in Table 5 below.
The odd ratio and 95% confidence interval of chronic wheezing of each study.

Forest plot was used to graphically demonstrate chronic cough from a total of five studies reported in Table 4.
Odds of reported chronic wheezing from nine studies shown in Table 5, are outlined below using forest plot.
Nine studies were used to calculate odd ratios for reported chronic phlegm, and the six of those studies are projected below in Figure 4.
Eight studies reported in Table 7 were used to illustrate the odds of shortness of breath among the exposed and referent groups in Figure 5 below.
Table 6 below indicate all the studies that reported chronic phlegm, and odd ratios were calculated at 95% CI.
Shows the odd ratio and 95% confidence interval of chronic phlegm of each study.

Shortness of breath was also reported as one of the chronic respiratory symptoms associated with cement dust exposure, and the results of calculated odd ratios are shown in Table 7 below.
Shows the odd ratio and 95% confidence interval of chronic dyspnea of each study.

Discussion
In this study, the main aim was to assess the association between occupational exposure to silicon dioxide and the prevalence of chronic respiratory symptoms amongst employees in cement plants. However, studies that focused on cement dust, total and respirable dust exposures were also included since there were few articles on occupational exposure and silicon dioxide. This study did not take into account the duration of exposure and work shift. In Table 5, a greater association between occupational exposure to silicon dioxide and prevalence of chronic cough (OR 1.90; CI 9.90, 0.78) was observed. This supports the findings of a case report by Matar et al. 21 where a worker presented chronic cough and was diagnosed with complicated silicosis from exposure to silicon dioxide. Similarly, 2011 in Spain countertops manufacturing industries, 295 cases of silicosis were reported, and approximately 82% of workers developed chronic respiratory symptoms from exposure to silicon dioxide. 22 There was also a greater risk of chronic wheezing (OR 1.34, CI 11.50, 0.50) among occupationally exposed workers to silicon dioxide. Approximately seven studies had an odd ratio <1, suggesting lower risk of chronic wheezing among workers exposed, while two studies (OR > 1) indicating greater association between occupational exposure and chronic wheezing. A study by Tsuchiya et al. 23 showed a chronic wheezing and other chronic respiratory symptoms in an 85-year-old non-smoker male who was exposed to silica dust from sand mold casting in motorcycle manufacturing industry for four decades. Eight studies suggested an association between occupational exposure and development of chronic phlegm (OR 1.16; CI 19.4, 0.22). Only one study indicated an equal probability for chronic phlegm in both exposed and control group. There was almost two-threshold risk of developing shortness of breath/dyspnea among workers exposed to silicon dioxide (OR 1.93; CI 22.43, 0.73), when eight studies were compared. Australian scholars reported exertional dyspnea from three cases that had chronic exposure (15, 20, and 23 years) to silicon dioxide from manufacturing artificial stone benchtops. 24 Only four studies suggested lower probability for the prevalence of shortness of breath/dyspnea, while one study indicated no association between exposure and shortness of breath/dyspnea. The non-association could be explained by possible pulmonary hypertension. Yeo et al. 25 found progressive exertional dyspnea as an early diagnosis of pulmonary capillary hemangiomatosis in a 29-year-old female exposed to silica from a bathtub-manufacturing factory. Chronic cough was the most prevalent exposure-related respiratory symptom. Dagnew et al. 26 reported the highest number of chronic respiratory symptoms amongst the workers. In the said study, workers were subjected to different working conditions and job description, and both exposed and control groups were assessed. Cough was found to be the most common prevalent chronic respiratory symptom. This accords well with the finding of the current study and suggests a higher probability for development of chronic cough among workers exposed to silicon dioxide. Hakim et al. 11 showed that experiencing chronic respiratory symptoms was mostly attributed to improper trainings on job tasks and standard operating procedures for mitigation, prevention and control of health hazards or risks arising from the workplace.
Figures 2–5 (forest plot graphs) suggest statistically significant difference in some of the studies that were recorded for each four chronic respiratory symptoms. Figure 2 shows that the results of one study were statistically significant different. Other studies suggest development of chronic cough among the exposed group. These studies provide a compelling evidence that there is an association between occupational exposure to silica and prevalence of chronic respiratory symptoms in the cement manufacturing industries. Table 3 shows the amount of concentration of crystalline silica that cement industry workers are exposed in different work units. Most studies that assessed the association between occupational exposure to crystalline silica in cement manufacturing industries indicates that the exposure level is above the recommended threshold limit values. High levels of particulate matter (PM2.5 and 10) were reported in different sections of the cement manufacturing industry. A mean concentration of 0.87 mg/m3 was measured in the cement mill with 0.50 mg/m3 in the parking section, and 1.80 mg/m3 in a crusher. 27 In a study conducted by Omidianidost et al. 16 and another study conducted by Gharavandi, 28 exposure to crystalline silica was in the range of 0.026–0.044 mg/m3 and 0.027–0.044 mg/m3 respectively. The highest and lowest crystalline silica exposure was experienced in the raw mill and the packaging unit. Similar high exposure events were noted in a study by Mirzaee et al., 29 where cement dust concentration was 4.5 mg/m3 near the packing machine, 4.2 mg/m3 during loading, 23 mg/m3 for crushing, and 43–47.6 mg/m3 in a raw mill. Thai et al., 30 suggest that the concentration levels of respirable cement dust concentration fluctuate significantly in different sections of the cement manufacturing industries, and such is dependent on the availability and levels of control mechanisms. A study by Couture et al., 31 in construction industry, showed high exposure levels of silica dust among crusher operators (0.08 mg/m3) and concrete truck operators (0.01 mg/m3), exceeding occupational exposure limits by more than 30 threshold.

Prevalence of chronic cough.

Prevalence of chronic wheezing.
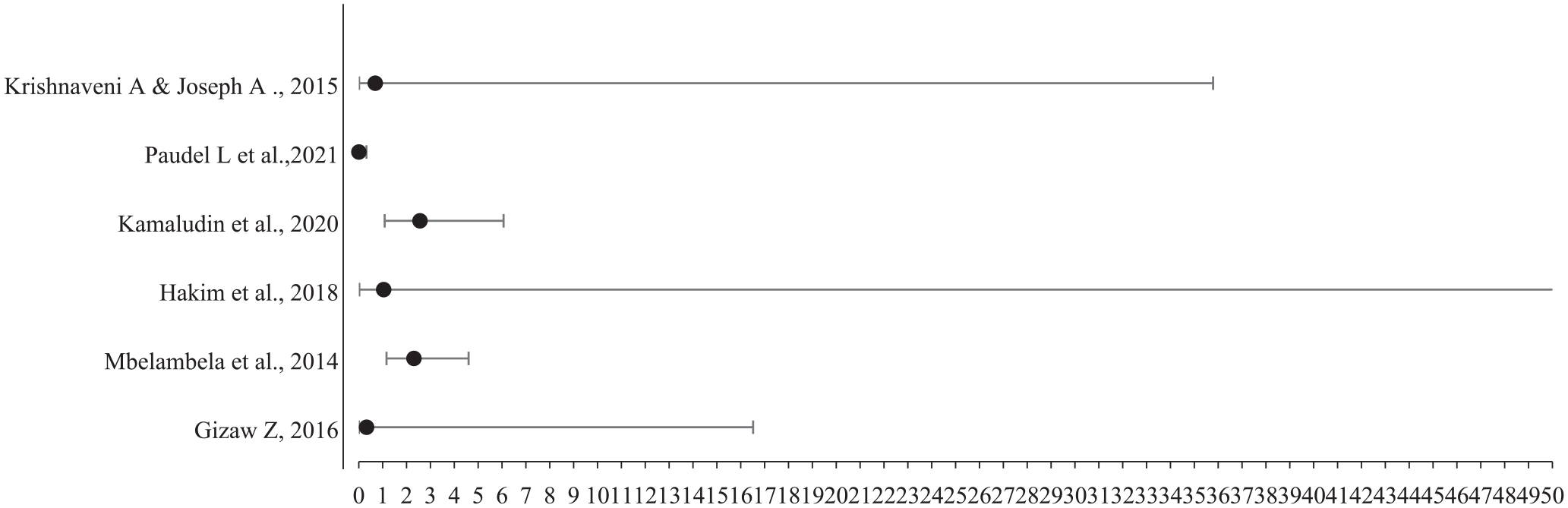
Prevalence of chronic phlegm.

Prevalence of chronic dyspnea/ shortness of breath.
According to Anderson et al., 32 workers in cement industry are exposed to high levels of PM cement dust fraction, ranging between 10 and 2.5 µm, and are more likely to suffer from chronic respiratory symptoms since this fraction can penetrate upper and deeper regions of the respiratory tract. A study conducted by Kakooei et al. 19 show that 16 bulk samples were collected to estimate the SiO2 content of bulk materials. Crystalline silica was found to contribute 22% of the cement dust produced. Also, Poornajaf 20 reported the composition of crystalline silica quartz to be 21.5% (limestone), 22.5% bauxite, 21.22% (clinker) and 21.22% (raw cement). The FEV1 and FVC in both studies was remarkably lower in exposed group. This suggested that exposed workers are likely to develop chronic respiratory symptoms.
Methodological strength and weaknesses
This review focused on cross-sectional studies, and included only one longitudinal study by Zeleke et al.2,14 This might have invited the exposure-effect misclassification bias since cross-sectional studies do not determine the cause and effect. Majority of studies included in this review, compared the exposed with the referent groups, and used exposure concentration to associate with health risks. Although the limited number of reviewed studies might have underrepresented the exposure scenario of silicon dioxide, this review also included studies that quantified the symptoms from different departments in the cement industries and exposures from bulk materials. Studies that focused on the extent to which chronic respiratory symptoms might have affected the lung function among workers were not reviewed. To eliminate this, only studies that collected personal exposure samples were included.
Potential biases
Since this review did not account for the symptoms per smokers and non-smokers, this might have invited reporting bias. Also, second-hand smoking which tend to be classified under non-smoking in many studies, could have led to misclassification of study groups, leading to under-reporting of chronic respiratory symptoms.
Future research
Many studies including this review have demonstrated the association between exposure to silicon dioxide in cement industries, bulk material processing and chronic respiratory symptoms. Given the limitations in the literature regarding health risk assessments in addressing lungs functionality, specific exposure symptoms, and clinical implications among the exposed occupations, hazard quotient determination studies are urgently needed. Firstly, it is important for future studies to explore the association between chronic respiratory symptoms among the exposed workers, classifying symptoms per job category. Dosimetry studies on particles settlement of silicon dioxide in various regions of the respiratory symptoms would assist in determining specific exposure symptoms. Furthermore, there is a need for future studies to determine the clinical cost implications for the treatment of silicon dioxide related exposure symptoms in order to inform improved controls in dusty occupational settings.
Conclusion
There is an association between occupational exposure to silica dust and prevalence of chronic respiratory symptoms amongst workers in the cement industries. This review demonstrated that occupational group exposed to silica dust, are more likely to experience chronic respiratory symptoms. Programs for workplace safety measures should be adopted and implemented with an aim of reduction risk of health hazard. Chronic cough was noted to be the most prevalent chronic respiratory symptoms and chronic wheezing to be the least.
Footnotes
Availability of data and material
Not applicable.
Code availability
Not applicable.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical clearance
This review study was submitted to the Research Ethics Committee of the University of Johannesburg (2021), and an ethical waiver was granted.