
Abstract
Introduction:
Numerous studies have reported respiratory impairment by exposure to fine particulate matter (PM2.5). However, limited studies investigated its effects on fiber cement roof workers. Thus, our study evaluated the impact of PM2.5 on pulmonary impairments among workers and its risk factors.
Design and Method:
A total of 131 fiber cement roof workers have been chosen based on the inclusive criteria. Size-segregated particles were measured in the workplace of workers. Interview and spirometry tests were obtained to determine the respiratory impairments.
Result:
The results showed the mean concentrations of PM2.5 had exceeded the WHO and US-EPA standards. A quarter of workers had lung restriction, lung obstruction, and mixed. Workers are most likely to have shortness of breath and wheezing. A significant correlation was found between smoking, production workers, and a long work period with abnormal lung function. Fiber cement roof workers are significantly at risk of exposure to PM2.5. They are most likely to acquire abnormal lung function due to PM2.5 exposure.
Conclusion:
Our study recommended the industry constantly maintain its programs. The industry should keep using the wet process to prevent dust generation and water suppression from preventing dust spread, as well as to wear respiratory protection for workers to avoid PM2.5 exposure. We recommended as well to the industry to implement follow-up programs for workers with abnormal lung function. Further action is needed to protect the workers’ occupational health in the fiber cement roof industry.
Introduction
Air pollution by particulate matter (PM) has been considered the five highest contributors to the global burden of disease. 1 Human health effects associated with exposure to PM were significantly affected by the size distribution, concentrations, components, and toxicities.2,3 Between 2000 and 2019, a large portion of the world’s metropolitan populace lived in regions exposed to the high level of PM with a diameter ≤2.5 µm (PM2.5), prompting significant numbers of non-communicable disease burdens. 4 PM2.5 is characterized by its small particle size, large surface area, and toxin absorption ability; hence, it can infiltrate the smallest airways, including alveolar tissue, with various toxic substances (such as metals and heavy metal ions, organic and inorganic compounds, allergens, many microbial compounds, and Polycyclic Aromatic Hydrocarbons).5,6 Epidemiological studies have consistently linked short-term exposure to gaseous air pollution and ambient particulate matter (PM) with increased hospitalization and mortality from respiratory disease. 7
Globally, PM2.5 has contributed to 7.8% of total deaths and 4.2% of disability-adjusted life years (DALYs). 8 Numerous epidemiological studies have reported morbidity and mortality by respiratory impairments related to inhalation of PM2.5, such as pulmonary inflammation,7,9,10 the decline in pulmonary function, asthma,11–13 and chronic obstructive pulmonary diseases (COPD).14,15 In addition, a study has revealed that every 10 μg/m3 increment of PM2.5 concentration will increase the mortality by respiratory illness by more than 1.68%. 16
These particulates come from numerous sources, including traffic, industries, trade activities, and home heating and cooking. Moreover, it is associated with health and well-being, ventilation/air velocity, 17 and improper indoor air quality in an environment, which can severely affect the occupants and workers at the workplace. Increasing industrial activities and urbanization also have consequences, notably in increasing pollution. 18 Inward contamination, reaction products within the indoor environment, and penetration of outdoor pollutants are great examples of sources of indoor air pollutants. PM2.5 has been reported as the primary pollutant from industrial sites in many countries such as China,18–21 Germany, 22 France, 23 Italy, 24 India, 25 and Pakistan. 10 Furthermore, respiratory health effects have also been reported among workers related to exposure to industrial PM2.5. 25 In the roofing fiber-cement industry, cement dust is generated in numerous processes, such as blending and pouring, racking and curing, and de-palleting and skid. 26
To date, there have been limited studies in Indonesia regarding the effect of PM2.5 on workers. Specifically, no study has been conducted on fiber cement roof industry workers in Indonesia. In response to this problem, this study investigates the relationship between PM2.5 exposure and lung impairment in workers working in the fiber-cement industry in Indonesia.
Methods
Study design and data collection
Study design
This cross-sectional study determines the relationship between PM2.5 and lung impairment among fiber roof industry workers. The collection of data was conducted from April to July 2019.
Location of study
The selected industry location is in Cikarang-Karawang, West Java, Indonesia. It is an industrial region area and one of the largest and most important fiber roof industries based on data from the Ministry of Industry of the Republic of Indonesia. The administrative workers are distributed on 8 h work shifts per day. Before the research was carried out, permission was sought from the company of the respective fiber cement roof industry, and ethical clearance was obtained from the Ethical Committee of the Ministry of Health of the Republic of Indonesia. Informed consent was acquired from each respondent in the study. The respondents were explained the measurement and evaluation process before agreeing to participate in this research. All the information and identities used in this study remain classified. based on on-site observation of the industry, the factory uses enclosed ventilation, filtered cabins, and a local exhaust ventilation system. It uses wet processes to prevent dust generation and water suppression from preventing dust spread. In addition, the workers also wear respiratory protection.
Participants
We recruited all workers of the selected industry with at least 10 years of seniority and still working when this study was conducted and collected personal data through a questionnaire administered in April−May 2019. A total of 131 respondents participated in this study. Data collection included interviews using a questionnaire, direct observation, and measurement of characteristics (gender, age, height, weight, Body Mass Index (BMI), education level, smoking status, duration of work, type of job, spirometry test), and concentration of PM.
Measurement of particulate matter
PM concentrations were measured following the previous method 27 in the environmental workplace (n = 14). The particulate matter measurement was collected in the same day. Briefly, four Sioutas cascade impactor (SKC Inc.) stages were attached to the Leland Legacy pump (SKC Inc.) and operated at 9 L/min flow rate for 2 h. Quartz filters (25 and 37 mm) were installed in each impactor stage to catch the PM in different sizes. The first, second, third, and fourth stages of impactor cached the particulate in diameter less than 0.25 μm (PM0.25), 0.25–0.5 μm (PM0.5), 0.5–1 μm (PM1.0), and 1–2.5 μm (PM2.5), respectively. The levels of each PM were finally measured by gravimetric analysis using MT5 Microbalance (METTLER TOLEDO Inc.) after being conditioned in the balance room for at least 24 h.
Identification of respiratory health symptoms
Information on the presence of respiratory health symptoms (coughing, sputum expectoration, shortness of breath, wheezing, and chest-related complaints) within the last 3 months was identified using ST. George’s Respiratory Questionnaire 28 by the interview.
Lung function test (Spirometry)
Lung function tests (spirometry) have been widely used to detect deterioration in respiratory function. The test was performed by a trained researcher using a Portable Spirometer BTL-08 Spiro. The minimum expiration time is 3 s until the flow volume graph peaks. Respondents were given enough time to understand the test procedure and provide the required flows. A pulmonologist’s doctor further interpreted the results to identify lung function abnormalities. The lung function abnormalities were classified into lung restriction, obstruction, and mixed symptoms.
Statistical analysis
The statistical analysis used a chi-square test to analyze the association of lung impairment with respiratory health symptoms and risk factors. The statistical significance was defined as a p-value < 0.05. The t-test was to analyze the differences of concentration of PM2.5. The logistic regression analysis was conducted to determine the significant risk factors.
Results
Characteristics of the respondents
The general characteristics of respondents are shown in Table 1. All respondents are male workers. Most workers (81.7%) completed high school or upper level at the education level. Almost half of the respondents (43.5%) were actively smoking based on their smoking status. The workers were predominantly >40 years old, had been working <20 years in the production section, and had BMI < 25. Most workers had normal results in a spirometry test, but 13.7% had lung restrictions.
General characteristics of fiber cement roof workers. Indonesia, 2019.

Particulate matter distributions
Table 2. shows the concentrations of PM0.25, PM0.5, PM1.0, and PM2.5 from eight measurement spots in the workplace divided into production and non-production area. The highest mean concentration both in the production and non-production area was PM2.5. There was a significant difference in mean concentrations between the production and non-production area.
Concentrations of PM in the environmental workplace of a fiber cement roof factory. Indonesia, 2019.

PM: particulate matter.
The fiber cement roof industry has distribution concentrations (mean ± SD) of PM 0.25, PM 0.5, PM 1.0, and PM 2.5.
Significant at <0.05 for an independent t-test.
Lung function impairment with respiratory health symptoms
The abnormal group reported more wheezing (66.67% vs 33.33%) and almost the same shortness of breath (43.75% vs 56.25%) than the normal group. It also showed a significant correlation between lung function impairment and respiratory health symptoms (wheezing and shortness of breath), demonstrating an 8.61-times and 3.29-times more significant risk of suffering lung function impairment compared to the respondents with normal lung function (Table 3).
Prevalence of respiratory health symptoms by lung impairment group among fiber cement roof workers. Indonesia, 2019.
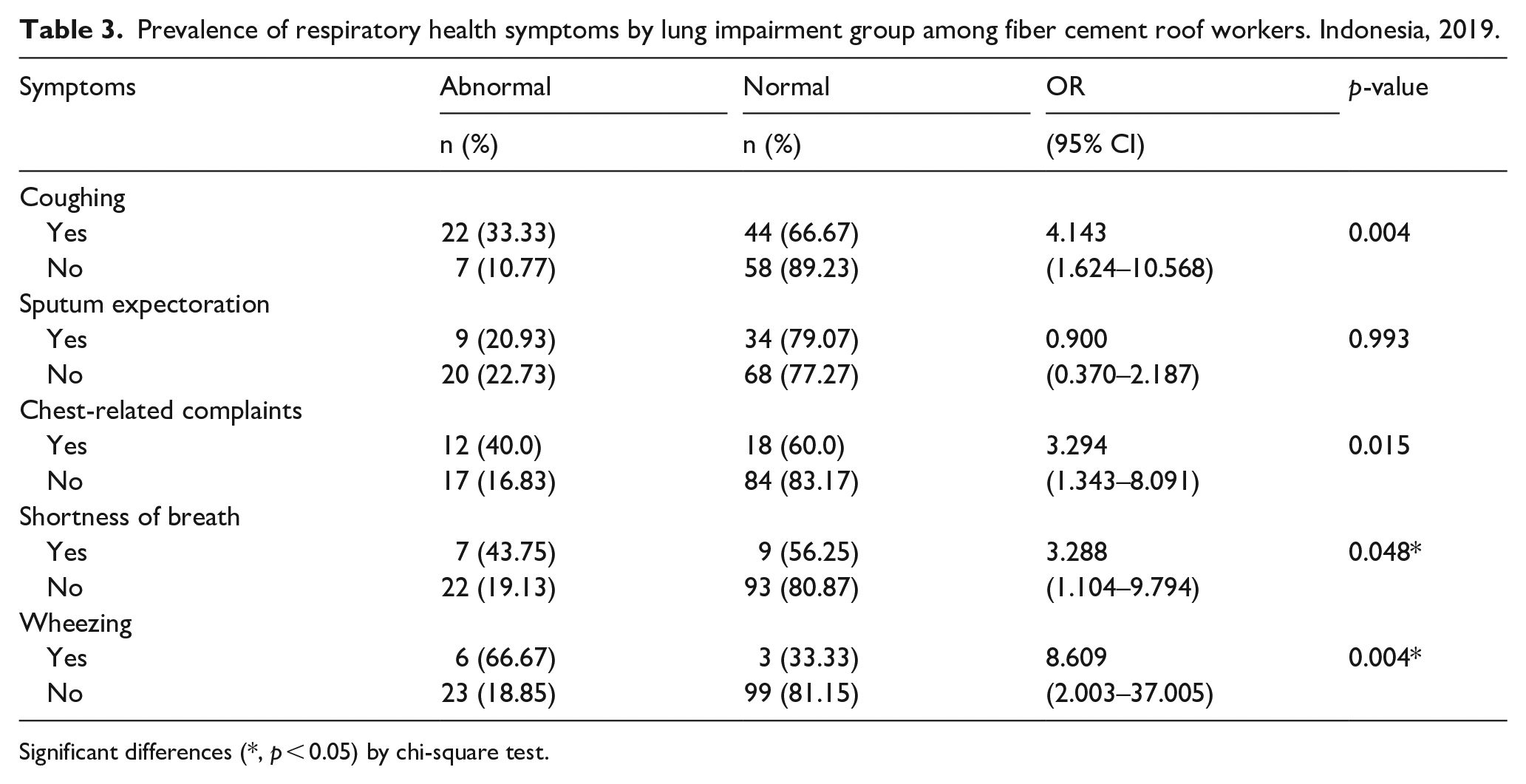
Significant differences (*, p < 0.05) by chi-square test.
Lung function impairment with risk factors
The workers who were actively smoking worked in the production section, and had been working for more than 20 years, had a significant correlation with lung function impairment, demonstrating a 6.0-times, 2.7-times, and 2.7-times greater risk of suffering lung function impairment (Table 4).
Prevalence of risk factors by lung impairment group among fiber cement roof workers. Indonesia, 2019.

Significant differences (*, p < 0.05) by chi-square test.
Multiple logistic regression analysis took PM2.5 exposure, education, smoking, age, BMI, job, and duration of work. Table 5 confirmed the abnormal lung function associated with smoking of OR 5.83 (95% CI: 2.14–15.87) and duration of work of OR 4.93 (95% CI: 1.20–20.24). However, smoking and PM2.5 exposure did not show any interaction.
Multiple logistic regression analysis among fiber cement roof workers in Indonesia, 2019.

Statistical significance at p < 0.05.
Discussion
This study figured that 22.1% of the workers acquire abnormal results in detail 13.7% lung restriction, 6.9% obstruction, and 1.5% both. This fraction may correlate with the interview result where the abnormal group reported more wheezing (66.67% vs 33.33%) and almost the same shortness of breath (43.75% vs 56.25%). It is also presented 8.61-times and 3.29-times more significant risk of suffering lung function impairment compared to the respondents with normal lung function. Decreased forced vital capacity (FVC) and FEV1 have also been associated with increasing concentrations of PM2.5 (PM with aerodynamic diameter <2.5 μm) in chronic obstructive pulmonary disease (COPD) patients who are ex-smokers or sustained quitters. Nonetheless, the effects of elemental components of PM among individuals not selected based on respiratory disease are under-investigated. 29 Similar to our results, the previous study has shown the association between PM2.5 exposure and lung function decline. 30
Our results showed high concentrations of PM2.5 in the workplace area. The concentrations of PM2.5 (127.46 µg/m3) were 8.5-fold higher than the WHO standard for the 24 h mean (15 µg/m3). It was 3.6-fold higher than the US-EPA standard 31 for a 24 h mean (35 µg/m3). Even though the mean concentrations of PM2.5 are the highest, the results still meet the required environmental quality standards of the Ministerial Decree of the Ministry of Health, Republic of Indonesia No. 70/2016 regarding Standards and Requirements for Industrial Work Environment, which is 10 mg/m3. Studies on respiratory symptoms among cement workers showed a higher risk of pulmonary dysfunction, pneumoconiosis, bronchitis, emphysema, and other disorders. 32
Regarding the smaller fractions (PM0.25, PM0.5, and PM1.0), our results demonstrated that the mean concentrations were not as high as PM2.5. Moreover, PM2.5 and heavy metals are found easily on the low-level floor in indoor air environments closer to the ground. 33 A previous study reported that the Brownian diffusion-controlled smaller particles, while the larger particle was affected by the gravitational sedimentation. 34 Since the smaller PM fractions have higher toxicities,35,36 more interest is needed, although the standards have not been established. Prior research by Mekasha et al. presented that the highest emission level of PM2.5 was from production areas (material receiving areas), and the lowest was in non-production areas (administrative units). In addition, employees working in production units, such as raw material receiving unit, cement milling unit, and cement packing unit, were eight, three, and two times more likely to develop chronic respiratory symptoms, respectively, compared to the workers in the non-production unit (administrative unit). 37 High PM concentration may contribute to chronic respiratory problems among workers in these high dust exposure units. As expected, the highest concentrations of fine particles were registered in the production area, as it is the type of location with the highest number of sources of emission. The statistical analysis reveals significant differences between the production and non-production areas. Once again, the non-production area had the lowest mean concentration values of particles in this fraction, while the production area had the highest.
We further examined the respiratory health symptoms by interview based on ST. George’s Respiratory Questionnaire. 28 Our results presented that workers are likely to have shortness of breath and wheezing. The result of coughing and chest-related complaints was lower than the symptoms of shortness of breath and wheezing. Exposure to a high concentration of PM, particularly PM2.5, has been reported to induce respiratory tract irritation and a higher risk of having a chronic cough, dyspnea, sputum production, wheezing, chest tightness, shortness of breath, phlegm, and nose irritation. 30 A previous animal study reported that high exposure to the fine particulate matter had been known to develop significant pulmonary inflammation, airway hyperresponsiveness, and promote airflow obstruction. 38
Smoking, production workers, and a long work period are the risk factors in our study. The previous studies also found that smoking, workers in production jobs, and long years of employment correlate with lung impairment. 39 Those studies suggest that the workers had a high risk of respiratory symptoms and impairment of lung functions, potentially caused by increased exposure to not only PM2.5 but also smaller PM fractions.
This study has limitations regarding design study and health effect measurement. This cross-sectional study can not show the causa effect relationship, and it only describes the association between PM2.5 exposure and lung impairment among workers. Nevertheless, our results are consistent with the current literature. Instead of its limitation, we believe our study will assist increase awareness about PM among workers and develop suitable occupational health programs.
Conclusion
This study found that the fiber cement roof industry showed high concentrations of PM2.5. The mean concentrations of PM2.5 were higher than the WHO and US-EPA standards. Almost a quarter of workers get abnormal results (lung restriction, obstruction, and both). This fraction may correlate with the interview result, where the abnormal group reported more wheezing and shortness of breath. The workers are most likely to have shortness of breath and wheezing. Meanwhile, the symptoms of coughing and chest-related complaints were lower than shortness of breath and wheezing. Smoking, production workers, and long work periods also correlate to abnormal lung function. However, the smoking habit factors have a more significant impact than the job factor (production and non-production) and the duration of work.
Our study recommended the industry constantly maintain its programs, such as using enclosed ventilation, filtered cabins, and local exhaust ventilation. The industry should keep using the wet process to prevent dust generation and water suppression from preventing dust spread, as well as to wear respiratory protection for workers exposed to higher amounts of particulate matter. Furthermore, we recommended the industry implement follow-up programs for workers with abnormal lung function by observing trends based on the results of medical examinations indicating abnormal lung function for further occupational health programs to be implemented for workers. Although the study has some limitations, the results will help improve public awareness of PM in the workplace.
Footnotes
Acknowledgements
The authors would like to acknowledge Dion Zein Nuridzin and Ema Fiki Munaya for technical help.
Author contribution
Conceptualization, S.M.N and D.H.R.; methodology, S.M.N and D.H.R.; writing—original draft preparation, S.M.N, D.H.R, F.A.P and S.S.; writing—review and editing, D.H.R, F.A.P, S.S. and S.F; supervision, S.M.N.; All authors have read and agreed to the published version of the manuscript
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Ministry of Research, Technology and Higher Education, the Republic of Indonesia, grant year 2019 and 2020. Decree Number 8/AMD/E1/KP. PTNBH/2020 and Agreement/Contract Number 332/PKS/R/UI/2020.
Institutional review board statement
The study will be conducted according to the guidelines of th Declaration of Helsinki, and has been approved by the Health Research Committee, National Institute of Health Research and Development (HREC-NIHRD), Ministry of Health of Republic Indonesia. Ethics clearance number: LB.02.01/KE.68/2019. The ethical approval was valid for a year.
Significance for public health
This article describes the association between PM2.5 exposure and lung impairment among workers. In this study, the PM2.5 exposure was higher in production area than non-production area. Regarding the health examination of the workers, almost a quarter of workers had lung restriction, obstruction, and combination of both. The workers are most likely to have shortness of breath and wheezing due to PM2.5 exposure.
Availability of data and materials
All data generated or analyzed during this study are included in this published article.