
Abstract
Background:
Despite the many touted benefits of community-wide face mask wearing, numerous communication campaigns and mandates, some people still refuse or fail to wear face masks in public settings. Hence, exposing themselves and others to the risk of infection by the severe acute respiratory syndrome coronavirus 2 and raise the potential for public healthcare systems to become overwhelmed once again. This study investigates demographic and hygiene factors related to propensity of face mask wearing in public settings.
Design and methods:
The self-administered online questionnaire contained the independent variables (demographic and hygiene factors) and the outcome variable (frequency of face mask wearing). Participants were recruited through convenience and snowball sampling techniques. Seven hundred and eight responses were collected from Malaysian adults between May and June 2020. The demographic characteristics of participants, differences in the frequency of face mask wearing across demographic factors and hierarchical multiple regression were analyzed.
Results:
The propensity of face mask wearing differs by gender. The hierarchical multiple regression revealed that being female, having personal protective equipment available and frequently washing hands were positively correlated with the frequency of face mask wearing. Moreover, the availability of personal protective equipment and the frequency of hand washing accounted for greater variation of the frequency of face mask wearing than gender.
Conclusion:
Future studies should adopt established psychosocial models in conjunction with normative and cultural factors for a better understanding of underlying motivations to engage in preventive health behaviors to shape improved hygienic and societal precautionary protective behaviors in different contexts.
Keywords
Introduction
The Coronavirus disease 2019 (COVID-19) has led to loss of many lives worldwide and presents an unprecedented challenge to public health. 1 Despite the availability of COVID-19 vaccines, we do not know whether people we come into contact with in public settings are up-to-date with their vaccines (e.g. unvaccinated or partially vaccinated) or may experience waning vaccine effectiveness over time.2,3 COVID-19 vaccines have not been 100% effective against all variants of the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). There have been reported cases of breakthrough infections among individuals who were fully vaccinated and individuals who received booster doses.2,4 People may suffer reinfections. 5 Take the Omicron variant as an example of what we have learned. It is highly transmissible4,6,7 and capable of significant immune evasion4,7 to overwhelm health systems.
The combination of reasons discussed above underscores the continued importance of nonpharmaceutical interventions. As such, face mask wearing by fully vaccinated people in public settings remains a sound preventive measure to maximize protection and prevent spreading all variants of SARS-CoV-2 to others.8,9 The proper use of face masks has significantly reduced the probability of contagion in public transport. 10 Wearing face masks proffer various benefits as face masks are easy to use, have good sustainability and benefit our health and the economy,11 –15 in contrast to other stringent measures (for instance, isolation, social distancing, and total lockdown) that have significant societal and economic costs.16,17 Wearing face masks as a precaution has escalated to double masking (i.e. wearing a cloth mask over a surgical mask). 18 The behavior to continue wearing face masks consistently post-vaccination is a sound precaution practice13,19 due to the new variants of SARS-CoV-2, breakthrough infection and waning immunity. A recent study found that the precautionary behavior of wearing face masks could significantly suppress the transmission of influenza. 20
However, there is heterogeneity in face mask wearing. The existing literature suggests that face mask wearing hinges on a variety of factors, including contextual factors. Many studies on face mask wearing during the COVID-19 pandemic researched demographic factors.17,21 –32 The two most commonly researched demographic factors associated with face mask wearing were a person’s gender and age. Studies found that women were more likely than men to wear face masks as a precaution during the COVID-19 pandemic.22,29,33,34 Stated differently, men are the weak links in hygiene discipline. 35 Regarding the relationship between a person’s age and face mask wearing, one study reported that different age groups exhibited different patterns. 32 Another study found that older individuals were more likely to wear face masks. 36 In contrast, other studies found that older individuals were less likely to wear face masks compared to younger individuals.27,29 In sum, the existing evidence regarding the relationship between age and face mask wearing is inconclusive.
Despite the many touted benefits of community-wide face mask wearing,14 –16,23,37,38 and numerous communication campaigns and mandates, some Malaysians still refuse or fail to wear face masks in public settings. 39 Hence, exposing themselves and others to the risk of infection by the SARS-CoV-2. This study examined the correlations between contextual risk factors24,25 of demographic and hygiene (i.e. the availability of personal protective equipment (PPE) and frequency of hand washing) and the frequency of face mask wearing. Next, this study examined the extent to which hygiene factors explain variation in the frequency of face mask wearing over and above that accounted for by the demographic factors.
Methods
Study design
To achieve its aim, this quantitative study used a cross-sectional design similar to that of several prior studies conducted during the COVID-19 pandemic.23,28,40
Measures
The self-administered online questionnaire was adopted from several prior studies.25,26,41,42 The independent variables were grouped into demographic factors (gender, age, number of children under 18 years old living in the same household, ethnicity, and occupation), and hygiene factors: the availability of personal protective equipment—for example, hand gloves, hand sanitizer or face mask—(measured from 1 = never to 5 = always) and frequency of hand washing (measured from 1 = never to 7 = every time). The outcome variable was frequency of face mask wearing in public settings (measured from 1 = never to 7 = every time). The questions and response scales are in Supplemental Appendix A.
This online questionnaire was offered in the three major languages of Malaysia (Malay, English, and Mandarin) so that participants could choose a language they were most comfortable with when answering the online questionnaire. To minimize response and measurement biases, this study followed standard survey approaches to ensure there was no social pressure that would influence participants’ responses, no questions that would provoke respondents to feel defensive or threaten their self-esteem and no payoff or cost for particular responses.
Participants
This study was conducted according to the Declaration of Helsinki and was approved by the Research Ethics Committee of the author’s university.
Participants were recruited through convenience and snowball sampling techniques. 43 The selection criteria was Malaysians 18 years old or above. Participation in this survey was voluntary and participants could opt-out at any time. Moreover, participants’ anonymity and confidentiality of their responses were assured. All participants consented to participate in this online survey by clicking the “Next” button to begin answering the online questionnaire.
Data collection
The online questionnaire was hosted on the Google Forms, an online survey platform, which was a safe and feasible way of collecting data during the pandemic.21,41,43,44 The online survey was administered from May to June 2020. The links to access the online questionnaires were distributed digitally via social media and email across various parts of Malaysia.
Data analysis
The data were analyzed using the Statistical Package for Social Sciences (SPSS) version 26. The normality of distribution for the availability of PPE, frequency of hand washing and frequency of face mask wearing was checked by visual inspection of the normal Q-Q plot. Descriptive statistics analyzed participants’ demographic characteristics. Analysis of variance (ANOVA) checked for differences in the frequency of face mask wearing by gender, age groups, number of children, ethnicity, and occupation. Bivariate correlations between all variables were examined for multi-collinearity. To determine the relative importance of the independent factors, the hierarchical multiple regression analyzed the change in R2 (∆R2) statistic (i.e. addition to the prediction of the frequency of face mask wearing) associated with the hygiene factors entered later in the analysis (Model 2 in Table 4), over and above the prediction contributed by the demographic factors entered earlier in the analysis (Model 1 in Table 4). 45 Model 2 can be conceived as a complete model as it contains all the factors of Model 1 (reduced model) as well as hygiene factors. Thus, the partial F-test in regression analysis was used to determine which of the two models fits the data better. The test statistic is:

where SSER = sum of squares error for reduced model
SSEC = sum of squares error for complete model
n = sample size
K* C = number of additional factors in the complete model
KC = number of factors in the complete model
Results
A total of 708 valid responses were received. The dataset is available in Mendeley Data https://data.mendeley.com/datasets/hvg8wd6jdp/3. It appeared that there was no serious violation of the normality assumption. A box plot of the availability of PPE, frequency of hand washing and frequency of face mask wearing identified no consistent outliers. There were no missing data as participants were required to answer all questions.
Upon analysis, the sample was found to be heterogenous. Table 1 shows the demographic characteristics of the participants. The participants consisted of roughly equal numbers of men (n = 345, 48.7%) and women (n = 363, 51.3%), diverse age groups (18–29 years old, n = 101, 14.3%; 30–39 years old, n = 213, 30.1%; 40–49 years old, n = 200, 28.2%; 50–59 years old, n = 159, 22.5%; 60 years old or above, n = 35, 4.9%), number of children in the household (none, n = 335, 47.3%), diverse ethnic groups (Malays, n = 348, 49.1%; Chinese, n = 234, 33.1%; Natives of Sabah and Sarawak, n = 85, 12%; Indians, n = 41, 5.8%) and various occupations (self-employed, n = 80, 11.3%; employee, n = 582, 82.2%; unemployed, n = 42, 5.9%; student, n = 4, 0.6%). Table 1 summarizes the analysis of variance (ANOVA) results. Women reported a significantly higher frequency of face mask wearing than men. However, there were no significant differences in the frequency of face mask wearing by age groups, number of children in the household, ethnicity or occupation. In addition to higher frequency of face mask wearing, women reported higher availability of PPE and frequency of hand washing (Table 2).
Population and sample demographic characteristics, frequency of face mask wearing and ANOVA results. Malaysia 2020.

n/a: data not available.
Department of Statistics, Malaysia https://statsgeo.mycensus.gov.my/geostats/mapv2.php#.
Including natives of Sabah & Sarawak.
Availability of PPE and frequency of hand washing by gender. Malaysia 2020.

Table 3 showed that the bivariate correlations between facemask wearing and hygiene factors (i.e. availability of PPE and hand washing) were greater than the bivariate correlation between facemask wearing and demographic factor (i.e. gender).
Bivariate correlations. Malaysia 2020.

Significant at the 0.05 level.
Significant at the 0.01 level.
Table 4 shows the results of hierarchical multiple regression. In model 1 (demographic factors), gender and age were positively correlated with face mask wearing. In model 2 (demographic factors and hygiene factors), gender, the availability of PPE and hand washing were positively correlated with the frequency of face mask wearing. Moreover, the availability of PPE and frequency of hand washing explicated a larger portion of variation (adjusted R2 = 0.228) in the frequency of face mask wearing than gender (adjusted R2 = 0.015). The average variance inflation factor (VIF) was near to one and the tolerance was greater than 0.2, indicating an absence of multicollinearity in model 2. There was no significant interaction between predictors.
Results of hierarchical multiple regression. Malaysia 2020.
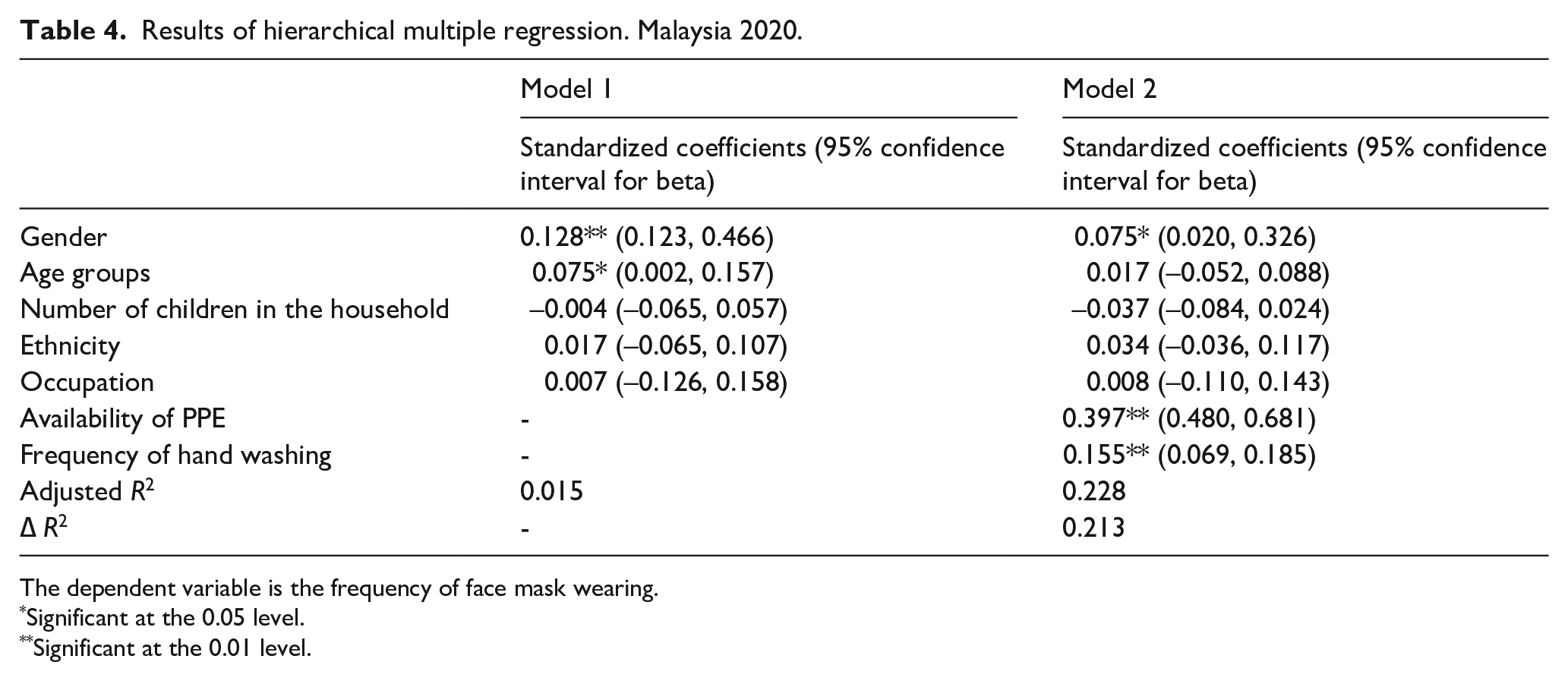
The dependent variable is the frequency of face mask wearing.
Significant at the 0.05 level.
Significant at the 0.01 level.
The calculated F value was 97.6, which is larger than the critical value of F (0.05, 2,701) of 3.00, which means that the addition of the availability of PPE and frequency of hand washing significantly reduced the unexplained variation in the model. In conclusion, the availability of PPE and the frequency of hand washing contributed to explain the frequency of face mask wearing and therefore should be retained in the model.
The correlation between the availability of PPE and the frequency of face mask wearing is low. Moreover, the variance inflation factors for the availability of PPE and the frequency of face mask wearing in the regression model suggested the absence of multi-collinearity.
Discussion
This study examined correlations of risk factors of demographic and hygiene with frequency of face mask wearing during the COVID-19 pandemic in Malaysia. Consistent with prior studies, this study found that women were more likely to wear face masks than men during the COVID-19 pandemic. Moreover, women also reported higher availability of PPE and frequency of hand washing than men during the COVID-19 pandemic. The ANOVA results suggested that there were no significant differences across other demographic factors (i.e. age groups, number of children, ethnicity and occupation) in terms of the frequency of face mask wearing, adding to the inconclusive results of prior studies. In sum, only gender seems to be consistently correlated with the frequency of face mask wearing.
Prior study found that face mask wearing was associated with various self-reported hygiene practices. 46 The correlations from this study added further empirical evidence to this notion in the context of the COVID-19 pandemic. The results from the hierarchical multiple regression revealed that the significant demographic factors (i.e. gender and age groups in model 1) only accounted for 1.5% of the variation in the frequency of face mask wearing compared to the hygiene factors (i.e. availability of PPE and frequency of hand washing in model 2) which accounted for an additional 21.3% of the variation in the frequency of face mask wearing. Stated differently, the hygiene factors explained more variation in the frequency of face mask wearing than the demographic factors. Moreover, the availability of PPE (β = 0.397, p-value < 0.01) and the frequency of hand washing (β = 0.155, p-value < 0.01) were relatively much more important than gender (β = 0.075, p-value < 0.05) in explaining the variability in the frequency of face mask wearing. In sum, this study highlights the small variation in the frequency of face mask wearing explained by the demographic factors in relation to the hygiene factors.
The public health response to the COVID-19 pandemic requires large-scale and significant modifications to individual behavior.15,47 Thus, the public health response imposes significant psychological loads on individuals. For this reason, insights from the domain of psychology can potentially align human behavior with the recommendations of epidemiologists and public health experts. 15 A search in the Web of Science found 37 articles similar to this study with demographic factors as the dominant correlates of face mask wearing (Supplemental Appendix B). Although there were 15 health related factors, but only three studies used the health belief model. In sum, despite the calls to adopt sociopsychological models 48 and social and behavioral science theories 49 to investigate preventive health behavior, the review here suggests little progress in this research direction for face mask wearing during the current pandemic. It is recommended that future studies related to face mask and behavior should utilize more social psychology theories. Moreover, normative and cultural factors (e.g. uncertainty avoidance) should be incorporated given the variation in face mask wearing across communities and countries.
This study had several limitations. First, the sample was not representative. Hence, the results are not generalizable. Furthermore, because this study utilized snowball sampling technique as part of data collection strategies, the response rate was unknown. Next, this study used an online survey. Thus, excluded physical contacts with people with no internet access, limited digital literacy or a low level of literacy. However, this limitation is inevitable considering the safety of both participants and researcher during the COVID-19 pandemic. Lastly, the results might be subjected to social desirability bias due to self-report by participants.
Conclusion and recommendations
For more than 100 years, face mask was used to fight various infectious diseases, for instance, the Manchurian plague (1910–1911), the Spanish flu (1918), the Severe Acute Respiratory Syndrome (SARS) (2003), the influenza A (H1N1) (2009), and the COVID-19 pandemic (from 2019). It is envisaged that face mask wearing will continue to be an effective health preventive behavior to deal with future infectious diseases.
Face mask usage is both physiological and psychological.47,50 –52 A recent study found that there are other motivations beside hygienic motivation for wearing a face mask. 53 Identifying the psychosocial and behavioral factors affecting the practice of precautionary behavior of face mask wearing15,22 contributes to effective intervention and policymaking that will increase face mask wearing compliance rates for the present and future pandemics, in line with the recommendation of World Health Organization Director-General to improve country readiness for future outbreaks. 54 This study provided empirical evidence that hygienic factors explained more variance in the frequency of face mask wearing than demographic factors. Adopting established psychosocial models, such as the Protection Motivation Theory 55 and the Health Belief Model,36,48 plus normative and cultural factors, can lead to a better understanding of underlying motivations to engage in preventive health behaviors to protect oneself and others in different contexts. Future public health policies would benefit from a better understanding of underlying motivations for preventive health behaviors in different contexts to shape improved hygienic and societal precautionary protective behaviors appropriate for living in the new norm of coexistence with SARS-CoV-2 or its latest variants.
Supplemental Material
sj-docx-1-phj-10.1177_22799036231197192 – Supplemental material for Correlations of demographic factors and hygiene factors with face mask wearing during the COVID-19 pandemic and suggestion for future research: A cross-sectional study of adults in Malaysia
Supplemental material, sj-docx-1-phj-10.1177_22799036231197192 for Correlations of demographic factors and hygiene factors with face mask wearing during the COVID-19 pandemic and suggestion for future research: A cross-sectional study of adults in Malaysia by Kim Hoe Looi in Journal of Public Health Research
Footnotes
Data availability statement
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Xiamen University Malaysia Research Fund [Grant number: XMUMRF/2019-C4/ISEM/0022].
Ethics approval
This study was conducted according to the Declaration of Helsinki and was approved by the Research Ethics Committee of Xiamen University Malaysia (reference number: REC-2004.01).
Significance for public health
Identifying the psychosocial and behavioral factors affecting the practice of precautionary behavior of face mask wearing contributes to effective intervention and policymaking that will increase face mask wearing compliance rates for the present and future pandemics. Future public health policies would benefit from a better understanding of underlying motivations for preventive health behaviors in different contexts to shape improved hygienic and societal precautionary protective behaviors appropriate for living in the new norm of coexistence with SARS-CoV-2 or its latest variants.
Supplemental materials
Supplemental materials for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.