
Abstract
The COVID-19 pandemic forced us to reconsider our interactions with the world around us, shifting how we navigate public and private spaces every day. Most people in the United States previously thought nothing of touching railings or doorknobs, going to school or work while ill, or attending crowded events. Along with new health interventions and institutional practices, daily behaviors aimed at infection control, such as routine hand washing and wearing face masks when symptomatic, protected our communities from COVID-19.1,2 Many new interventions and practices are here to stay, but it is unclear which personal behaviors to protect against COVID-19 and other infectious diseases we should continue. Although the urgency of the COVID-19 pandemic may be fading, emerging infectious diseases such as mpox (formerly known as monkeypox) and polio underscore the potential value of transmission-mitigating behaviors.3,4
Which, if any, of these personal preventive behaviors adopted during the COVID-19 pandemic should people in the United States continue to practice? Intuitively plausible ethical arguments support individuals taking reasonable measures to avoid causing or propagating harm to other members of the community. As such, by failing to adopt easily implementable preventive behaviors, we live ethically suboptimal lives and violate our social contract to one another. As the world transitions from epidemic to endemic COVID-19, applying the lessons learned from the pandemic is crucial to mitigating old and new infectious disease threats. Along with the role of public health agencies to organize and communicate about communicable diseases, clinicians and public health workers have critical roles in establishing social norms for behaviors that prevent the spread of infectious diseases, given their professional responsibilities and statuses as trusted authority figures. 5
The Importance of Personal Preventive Behaviors After the COVID-19 Pandemic
In non-pandemic contexts, seasonal and endemic infectious diseases inflict substantial morbidity, mortality, and economic costs. Respiratory, gastrointestinal, and other endemic pathogens infect millions and kill tens of thousands of people in the United States each year. 6 Seasonal influenza alone typically kills 36 000 to 49 000 people annually in the United States and incurs more than $11 billion per year in economic costs. 7 Infection control measures implemented to limit the spread of COVID-19 led to massive reductions in the transmission of influenza and other endemic and seasonal infectious diseases.8 -10 Aggressive COVID-19 mitigation measures, such as transitioning to virtual schooling and closing large public venues, likely contributed substantially to the extreme drops in infectious disease incidence, but these measures are neither sustainable nor desirable in the long term. For example, imposing mandatory lockdown measures every year during peak seasonal respiratory disease periods would curb transmission, but the harms from disruptions to educational, economic, and social activities would greatly outweigh the benefits. In addition, the steep drops in endemic and seasonal infections following aggressive COVID-19 control measures have led to resurgences of these pathogens during the past several years among people who had limited exposures.11,12
Given the costs of drastic infection control measures, the impact of individual behaviors on decreasing preventable morbidity and mortality cannot be overlooked. Continued public adherence to personal preventive behaviors learned during the pandemic can substantially reduce the transmission of infectious diseases and prevent a sizable portion of their associated health, economic, and social harms.13,14
Personal preventive behaviors can help control transmission of many infectious diseases without disrupting important social activities. Many of these personal preventive behaviors were widely practiced during the COVID-19 pandemic, including hand hygiene, respiratory etiquette, self-isolation when symptomatic, wearing face masks, and vaccination (Table).15,16 Unlike lockdowns or travel restrictions, these behaviors would not reduce transmission to levels that could lead to substantial upward swings in incidence or hypervirulent resurgences of endemic or seasonal diseases. Rather, these behaviors would reduce unnecessary, preventable transmission, which should particularly benefit medically and socially vulnerable populations. Baseline endemic and seasonal infectious disease transmission would still occur and would continue to provide immune system exposures, although at lower levels than presently.
Personal preventive behaviors to continue after the COVID-19 pandemic a
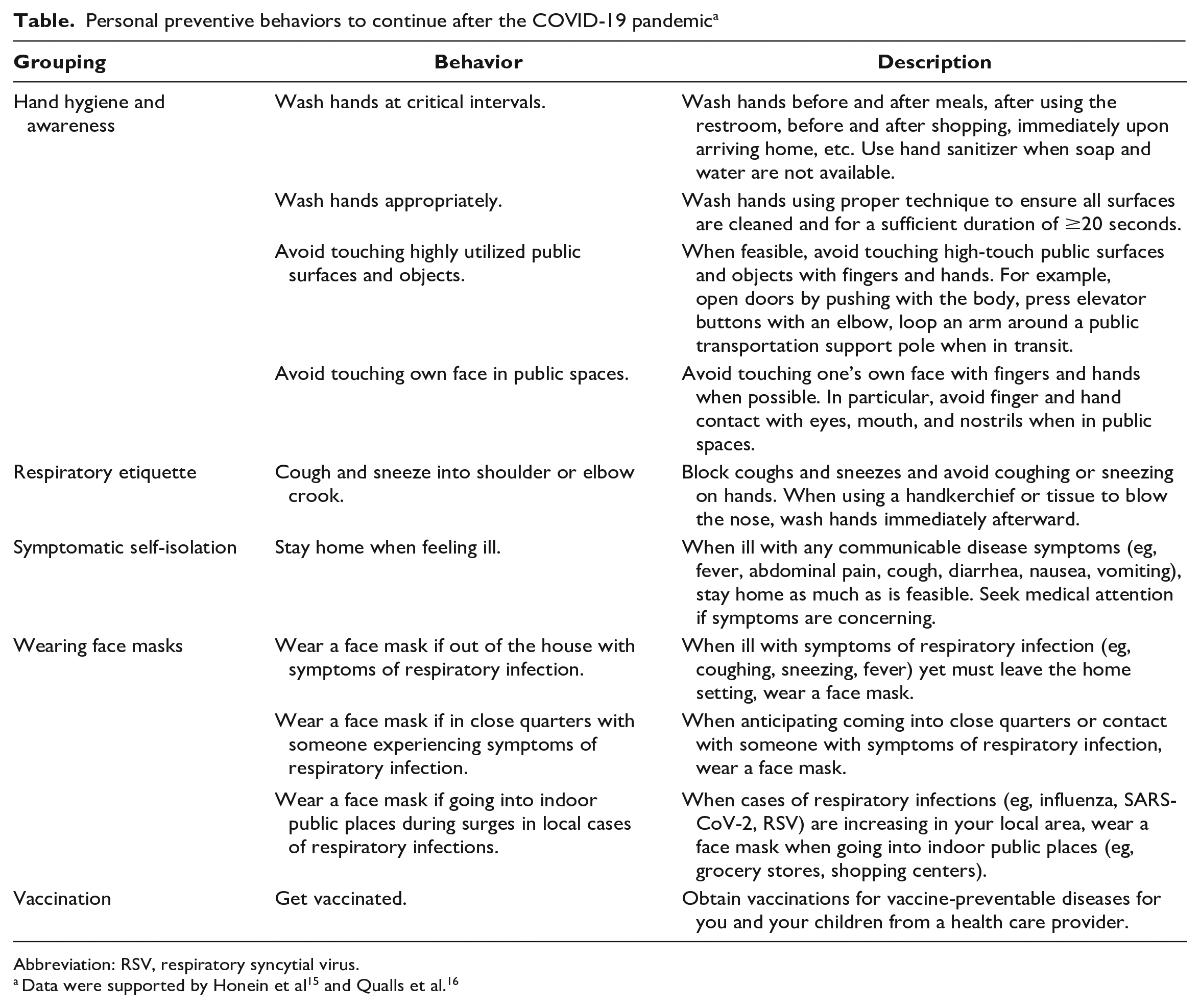
Abbreviation: RSV, respiratory syncytial virus.
The repeated emergence of new SARS-CoV-2 variants such as Delta and Omicron during the pandemic further highlights the importance of personal preventive behaviors. During the summer of 2021, declining cases and deaths combined with rising vaccination rates in the United States prompted a relaxation of institutional restrictions and personal preventive behaviors. The subsequent Delta surge quickly overturned that fragile sense of ease and brought a return of those restrictions and behaviors. A similar pattern repeated after the massive Omicron waves in early 2022, followed by a gradual easing of mitigation efforts. The public must realize that SARS-CoV-2 is becoming endemic, and evolving behavioral and policy responses will determine the ongoing toll of preventable morbidity and mortality. These policy responses and personal behaviors will also help determine the extent of transmission of new emerging pathogens and can affect the course of future pandemics.
Pandemics Present Ethically Critical Opportunities for Change
As with epidemics and pandemics of the past, the COVID-19 pandemic can lead to positive political and social changes, creating a favorable environment for adopting behaviors and social norms that promote public health. For example, spitting in public and sharing cups or silverware with strangers became socially unacceptable as a result of the tuberculosis epidemics in the United States in the late 19th and early 20th centuries.
17
In 1919, following the global influenza pandemic, an article in Science proclaimed the following: The great lesson of the pandemic is to call attention to the prevalence of respiratory diseases in ordinary times, to the indifference with which they are ordinarily regarded and to our present inability to protect ourselves against them. They are not amenable to control through sanitary works as are typhoid, malaria, and so many other diseases. They must be controlled by administrative procedures, and by the exercise of appropriate measures of self-protection.
18
More recently, the 2003 SARS epidemic in Southeast Asia established lasting social norms among local populations to wear face masks in public when feeling ill or during surges of seasonal respiratory diseases, which likely facilitated adherence by people in the region to public health measures during the COVID-19 pandemic. 19 Researchers studying attitudes, habits, and health behaviors point to the beneficial effects of habits established for good reasons. 20 Once established, health-promoting behaviors can be protected by habits, particularly when reinforced with contextual cues. History shows that societies can adopt new and beneficial behaviors after experiencing a consequential epidemic. This is a critical moment to heed lessons learned about the feasibility and societal benefit of behaviors that help prevent infectious disease and to use this experience to normalize these habits in a non-pandemic context.
Although there are strong ethical reasons that support the continued use of some personal preventive behaviors beyond the COVID-19 pandemic, public health agencies must first establish appropriate guidance according to established principles, that is, by assessing burdens and benefits, effects on autonomy, equity, and efficiency.21,22 Many personal preventive behaviors have a low burden on individuals but a substantial potential benefit, as demonstrated from experience with COVID-19 and prior pandemics. However, individuals must adhere to the guidelines established by public health authorities for any measure to be effective.
Common sense tells us that we are ethically obligated to prevent harm from befalling others if we can do so without bearing excessive costs to ourselves. Moral philosophers call this the “duty of easy rescue”—an ethical obligation to assist others in grave need when doing so would result in only minor burdens or inconveniences to oneself. 23 A classic example illustrates the duty of easy rescue: imagine you are walking to a meeting, and you witness a small child drowning in a shallow pond near the sidewalk. You could easily save the child’s life by pulling the child out of the water, but this would muddy your clothes and make you late to your meeting. Most would agree that it would be wrong to let the child drown to avoid such minor burdens. 24 This argument can support an ethical obligation to receive vaccinations, for example, because the combined effect of high levels of vaccination can produce herd immunity, which provides a robust benefit to populations as a whole. 25 Similarly, it would be ethically wrong to refuse to continue easy, widely adopted behaviors, such as improved hand hygiene and staying home when symptomatically ill, because this refusal would contribute to preventable suffering and death from infectious diseases. Declining to make these modest changes would be a dereliction of our basic ethical responsibilities to each other.
Although the concept of the duty of easy rescue is clear, the positive effects of personal preventive behaviors are usually invisible and have limited emotional salience: people do not know when washing their hands or covering their cough keeps someone else from getting sick. Therefore, framing this obligation based on the duty of easy rescue might leave people unmoved. Changing or maintaining good health-related behaviors requires other types of persuasion, such as appeals to individual interests and commitments, emphasis on families and local communities, and leadership from trusted figures.26,27 Clinicians and public health workers can play a key role in translating the duty of easy rescue into terms that are actionable and persuasive for their patients and communities.
Responsibilities of Clinicians and Public Health Workers to Influence Social Norms for Personal Preventive Behaviors
Each of us has an ethical duty to continue the modest personal preventive behaviors used during COVID-19 to help control infectious diseases in the post-pandemic “new normal” (Table). However, for such behaviors to be widely adopted, they must become socially normative. Social norms are rules for behavior that individuals follow because a critical mass of people in their community also follow them. 28 People typically avoid sneezing on each other or eating food from strangers’ plates because of social norms, not laws or regulations. Kosher and Halal dietary rules are examples of health-related social norms followed by particular religious groups. Strong social norms would allow people to adopt personal preventive behaviors as a matter of habit, thereby enhancing their widespread adoption and increasing the overall societal benefit of reduced infections.
Various individuals and institutions, from politicians to religious leaders to star athletes to social media influencers, can establish social norms. Among these many influences, clinicians and public health workers play central roles in sustaining new health behaviors. Specialists in epidemiology, infectious disease, and preventive medicine can lead research and public messaging about the value of personal preventive behaviors for reducing infection risk, and all practicing clinicians and public health workers can serve as role models and advocates. The shift in societal attitudes about smoking offers an example: clinicians and public health workers have played critical roles in reducing cigarette smoking in the United States by influencing individuals’ smoking behaviors and smoking policies throughout the past several decades.29,30 During the COVID-19 pandemic, clinicians and public health workers advocated for their patients and communities to adopt new behaviors to protect themselves and others from COVID-19. In the darkest days of the pandemic, uptake of preventive health measures was high in the United States, even with its cultural traditions of individualism and freedom of choice. 31
Despite this uptake of personal preventive behaviors, societies can easily revert to pre-pandemic behaviors. 32 Clinicians and public health workers should help maintain these social norms for personal preventive behaviors by continuing these behaviors at home and at work and by strongly (and nonjudgmentally) encouraging their patients and community members to do the same. 33 Clinicians and public health workers should adopt best practices for communicating the health implications of personal preventive behaviors while acknowledging the political divisiveness of COVID-19.34,35 Health communication experts recognize that trusted sources such as clinicians and public health workers are critical to the uptake of information. Communication must occur within the context of a trusted relationship and an environment that supports autonomy and choice. 36 Information provided to people about health risks and preventive behaviors should consider community context, promote solidarity, and focus on others in the community who are medically and socially vulnerable. 37 Risk perception may also play a role; one study found that awareness of negative consequences of the pandemic motivated adoption of preventive behaviors, and another study found that self-efficacy and awareness of the effectiveness of preventive measures were successful at motivating behaviors.38,39 While clinicians and public health workers are key figures in this communication process, it is important to acknowledge that trust in public health authorities diminished during the COVID-19 pandemic, with public health workers facing substantial backlash, including harassment and violence.40,41 The loss of trust in health authorities caused burnout and disillusionment among public health workers and impeded their ability to positively influence health-related social norms among some segments of the US population. 32
That said, individuals cannot bear the full burden of continuing personal preventive behaviors beyond the COVID-19 pandemic. Policies, systems, and structures at all levels of business, government, and civil society are involved in determining the social norms and practices that affect the spread of infectious disease. Clinicians and public health workers can help advocate for constructive social policy and regulatory changes to support the adoption of personal preventive behaviors. For example, many workers cannot afford to stay home during a respiratory or gastrointestinal illness because their employers do not offer paid sick leave or telework options. 42 Clinicians and public health workers should advocate for laws and organizational policies that empower people to reduce the spread of infectious diseases.
Responding to Concerns About Personal Preventive Behaviors
Patients might raise concerns about perceived infringements on their rights to liberty or autonomy when counseled to wear face masks or to avoid crowds when symptomatic. The personal preventive behaviors described here impose minimal constraints on individual freedoms and are justified by the positive consequences resulting from their widespread adoption: preventing avoidable death, suffering, and economic burdens. Behavioral scientists with decades of experience working on HIV-related behavioral challenges have recommended emphasizing autonomy, choice, and empowerment, as well as appealing to people’s values, perspectives, and lived experiences when communicating about COVID-19 preventive behaviors.43,44 Clinicians and public health workers can therefore frame their arguments for voluntarily adopting personal preventive behaviors by emphasizing the self-protective benefits for patients. Including information that these behaviors can help protect loved ones and community members while avoiding the need for burdensome mandatory public health measures is also beneficial.
Clinicians might be concerned about the opportunity costs of advocating for these personal preventive behaviors when patients have other pressing concerns in clinical encounters with limited time. However, messages about personal preventive behaviors can be delivered succinctly and remain convincing. Emerging evidence suggests that discussing the community benefits of health interventions such as vaccines or infectious disease testing with patients can improve acceptance of those interventions. 45 Clinicians have responsibilities not only to the health of their patients but also to communities. 46 The public health responsibilities of clinicians are clear in their obligations to report certain communicable diseases or to warn others about disease threats, even when these actions are contrary to a patient’s preferences (eg, in cases of sexually transmitted infections or multidrug-resistant tuberculosis). Despite the need for clinicians to balance competing clinical priorities, given their roles as trusted sources of guidance about health-related behaviors, they should take opportunities during clinical visits to establish new social norms to help make historic improvements in public health.
Some people might question the preventive behaviors that we have endorsed in this article (Table). The quality of evidence for the effectiveness of these behaviors varies, and discussion is still needed about which behaviors should be continued and why. Some behaviors are supported by epidemiologic studies and others by mechanistic studies (eg, bacterial load on surfaces).47 -51 Further research is needed to better assess their effectiveness, but these low-effort personal preventive behaviors were widely adopted during the COVID-19 pandemic because of their potential to have meaningful effects on community health. Clinicians and public health workers must stay informed about new findings on the best methods to control infectious disease transmission, and additional research should address health communication strategies and practices to help support and maintain new behavioral norms of infection control.
Conclusions
The COVID-19 pandemic provides valuable lessons on the importance of low-effort personal preventive behaviors that help protect against infectious diseases. More extreme public health measures such as lockdowns cannot and should not be continued indefinitely. The goal in a post-pandemic world is not to lower infectious disease risks to zero at all costs; rather, we should work to normalize personal preventive behaviors that are worth continuing. For individuals, the ethical duty of easy rescue supports adopting or continuing personal preventive behaviors even after the COVID-19 pandemic. For clinicians and public health workers, professional and ethical duties to care for the health of their communities support promoting these behaviors to establish new social norms for infection control.
We acknowledge the need for additional research and reasonable debate about which behaviors, organizational practices, or government policies should be adopted for a post-pandemic context. However, the personal preventive behaviors that we highlighted involve relatively low effort and minimal disruption to daily living yet offer potentially substantial benefits to public health. The importance of maintaining personal preventive behaviors is particularly underscored by the continual emergence of SARS-CoV-2 variants of concern and other emerging infectious disease threats. The COVID-19 pandemic presents a golden opportunity to start changing social norms to protect our communities from ever-present endemic and seasonal infectious diseases and from future emerging infectious diseases.
Footnotes
Disclaimer
The Walter Reed Army Institute of Research has reviewed this material, and there is no objection to its presentation or publication. The opinions or assertions contained herein are the authors’ private views and do not necessarily reflect the policies or positions of the Walter Reed Army Institute of Research, Global Emerging Infections Surveillance Branch, US Army, US Department of Defense, or US government.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.