
Abstract
Introduction:
Virtual diabetes coaching through applications has the potential to improve self-management in people with Type 2 Diabetes Mellitus. However, applications designed for Asian’s diabetic have never been studied. Therefore, our study aimed to identify the effect of Guru Diabetes Apps-Based Health Coaching on the level of glycemic hemoglobin, knowledge, and quality of life in Indonesians, as one of Asian ethnicities.
Materials and methods:
This study used an experimental design. Participants with T2DM were recruited from three primary care health centers. The intervention included 3 months of virtual health coaching through the Guru Diabetes application. The daily monitoring of glycemic blood glucose, blood pressure, body weight, nutrition intake, and activity provided were used as baseline to conduct virtual in-person coaching. The glycemic hemoglobin level, knowledge level, and quality of life were assessed at baseline and post-enrollment. A multilevel modeling approach was used for statistical analysis.
Results:
A total of 66 respondents were enrolled, and 62 respondents (93.93%) remained in the study at 3 months. After completing the intervention, the HbA1c level decreased in all groups, however it did not differ among the groups. On the other hand, the results indicate significant improvement in the average diabetes self-management knowledge score (pre = 14.97 vs post = 19.07, p < 0.05) and quality of life score (pre = 54.34 vs post = 60.28, p < 0.05), with significant difference among the groups (p < 0.05).
Conclusion:
Participants in the Android Application-Based Health Coaching experienced a significant improvement in diabetes self-management knowledge and quality of life scores at 3 months. In conclusion, the Guru Diabetes Apps-Based Health Coaching has the potential to support people with T2DM in performing diabetes self-management at home.
Keywords
Introduction
Diabetes Mellitus (DM) is a chronic disease and a growing problem worldwide due to increased life expectancy and lifestyle modifications. DM is characterized by hyperglycemia and high glycated hemoglobin. Chronic hyperglycemia leads to damage and failure of various organs, including the heart, blood vessels, eyes, kidneys, and nerves. 1 Type 2 Diabetes Mellitus (T2DM) is increasingly common because of sedentary life style and obesity, and it is projected that 700 million people will be living with T2DM by 2045. 2 The prevalence of T2DM in adult is becoming prominent, and much of the increase is occurring in developing countries where the majority of patients are between 45 and 65 years old. 3 Therefore, programs that focus on lifestyle changes are urgently needed to prevent the disease. 4
People living with T2DM should receive education about diabetes self-management. This education should involve nutrition evaluation, and lifestyle recommendation should be tailored according to physical and functional ability. 3 Studies have also shown a significant reduction in the incidence of T2DM with a combination of maintaining a body mass index of 25 kg/m2, eating high-fiber, unsaturated fat, low glycemic index diet, regular exercise abstinence from smoking, and moderate consumption of alcohol. 3 Since lifestyle modification might impact psychological well-being and social life, which can directly worsen the glycemic index, person-to-person education of the populace remains key to controlling this emerging epidemic. 5
A behavioral medicine platform can be developed as an additional dan innovative way to improve diabetes management and prevention for global and diverse population. By applying behavioral medicine, patients can be individually assessed to identify the burden of adhering to lifestyle modification, which may vary among the patients. 6 A systematic review suggests that digital health coaching offers a promising strategy for long-term management of T2DM population, with similar benefits to in-person health coaching. 7
Digital health coaching uses motivation and behavior exchange theory frameworks to restructure individual health goals, and digital feedback systems to notice and intervene on goal-dissonant behaviors and outcomes. 8 The number of adults and older adults who report owning smartphone has more than doubled worldwide, expanding the prospects for improving care and outcomes in adults with chronic diseases through Android Application-Based Health Coaching. 9 Previous research has shown that older adults are interested in using technologies to manage chronic disease symptoms. Further, virtual health coaching has shown promise as a means of increasing patient-to-provider communication, encouraging diabetes self-management, and medication adherence, as well as motivating positive behavior change10,11
Many virtual health coaching models have been implemented to improve T2DM management in America and Europe, yet their application for Asians diabetes has never been studied. Older adults living in Asia or of Asian origin have unique preferences for information that require special attention, as one study suggests that Asian internet users perceived significantly less loneliness compared with their age peers who were not internet users. 12 Therefore, our study aims to identify the effect of Android Application-Based Health Coaching on the level of glycemic hemoglobin, knowledge, and quality of life in people with T2DM.
Materials and methods
Study design
A quasi-experimental non-equivalent control group pretest-posttest design was used in this study to compare participants receiving Android Application-Based Health Coaching with patients in usual care. Purposive sampling was employed to select participants for this study. We recruited participants with T2DM from three primary care health centers and assigned them to one of two groups: the intervention or the control groups. A total of 66 respondents were enrolled in this study, of whom 62 (93.93%) completed the study. The intervention group consisted of 29 individuals, while the control group consisted of 33 individuals.
The minimum sample size was calculated using the sample size formula to ensure that the study had sufficient statistical power to detect meaningful differences between the groups being compared 13 :

Information:
n = number of samples
S = Deviation standard (1,1) 14
Zα/2 = Z score (confident interval of 95%), therefore Zα/2 = 1.96
Z1-β = Z score (power = 80%), therefore Z1−β = 0.84
μo–μa = The difference in mean score between intervention and control group, therefore the value was calculated as—0.37 – 0.23 = −0.6. 14
Based on the formula above, the minimum sample size was 27 each group.
Eligibility
Patients aged 20 to approximately 72 years, with T2DM and an HbA1c level of ≥6.5%, who were able to use an android smartphone, and provided consent to participate, were eligible for this study. Participants who live alone, were pregnant, had serious medical illness including end-stage-renal disease and heart failure, and had difficulty performing physical activity were excluded from the study. This exclusion criterion was implemented to ensure the safety and well-being of the participants.
Intervention
Regardless of their assigned group, all participants were instructed to download the application of “Guru Diabetes” application. The coach monitored the data on participants’ dietary habits, physical activity, drug adherence, and routine measurements of blood pressure and blood glucose during the coaching period. All participants were provided with basic diabetes education through short videos available on the application. Meanwhile, the control group received standard care from their clinic. Participants were instructed to record their dietary habits, physical activity, drug adherence, and routine measurements of blood pressure and blood glucose in the application on a daily basis. Patients were instructed to send photos of their diet through WhatsApp, and were able to send messages to the coach 24 h a day. Small group video calls were conducted every 2 weeks and in-person voice call was arranged as needed based on the data input in the application.
A health coach was defined as a behavior change specialist with expertise in chronic disease management. Health coaching in the study is a self-directed inquiry, in which the researcher holds a master’s degree in nursing and has undergone national coaching training. With the assistant of health coach, patients determined health-related goals and monitored their progress on daily basis. The health coach monitored the patients’ application input and provided immediate attention (24-hours/day and 7-day a week) in response to episodes of desirable progress, relapse, and resistance. The health coach protocol has been manualized, with an emphasis situations frequently observed when addressing behavior change in T2DM-affected patients.
Guru Diabetes application
Guru Diabetes uses a low-tech remote patient monitoring system to support health coaching. Health coaching working with Guru Diabetes are required to have a health coach certification, prior experience, motivational interviewing skills, and basic health knowledge. The automated daily prompts request information on blood glucose (fasting or non-fasting), blood pressure, body weight, dietary intake, exercise, and medication. Additionally, HbA1c is requested to be filled out at the beginning and end of 3-month period. Examples of the application’s features can be seen in Figure 1. As shown in Figure 1, the application also provides short video and news about diabetes self-management to improve patients’ motivation for positive behavior. Interestingly, the application also provides an automated calorie count based on patients’ daily intake and needs (Figure 2).

Examples of Guru Diabetes application features.

Automated calorie amount according to patients took and need provided by Guru Diabetes application.
Outcomes and measurements
The study measured three outcomes, including the change in HbA1c levels (%), diabetes self-management knowledge, and quality of life between baseline and 3 months among the two groups. Demographic and clinical information were collected at baseline. The laboratory parameter, HbA1c level was collected pre- and post-intervention. The quality of life was measured using Indonesian Version for Diabetes Quality of Life-Brief Clinical Inventory (DQoL-BCI), 15 while knowledge of diabetes self-management was measured using Indonesian Version of the Diabetes Knowledge Questionnaire 24 (DKQ-24). 16
Statistical analysis
The categorical data variables were presented as frequencies with percentages. A t-test was used to compare the mean 3-month HbA1c levels, knowledge, and quality of life levels between the two groups. The statistical analysis was set at a p-value of <0.05.
Ethics approval
Ethical approval was granted before the study was conducted. At the initial meeting, participants’ HbA1c findings were verified, and the study protocol was explained to them. After that, informed consent was obtained from them. Eligible patients then completed demographic, knowledge, and quality of life questionnaires. All data and information were anonymized according to the guidelines of the International Conference on Harmonization Good Clinical Practice.
Result
Of the 66 patients who volunteered for the study and provide informed consent, 33 were randomly allocated to the coaching group. Most of these patients (29 [87.8%]) completed the baseline survey. The intervention group was significantly younger (54.24 ± 0.56) than the control group (59.18 ± 10.24) (p =0.030). The residence distribution was also different between groups (p = 0.0001), with all intervention group participants residing in rural area (n = 29, 100%) while majority of control group participants residing in urban area (n = 20, 60.6%). Similarly, the distribution of housemates between the two groups was also significantly different (p = 0.0001), with most of the intervention group staying with their spouse and child/children (n = 22, 75.9%), while most of the control group stayed with their spouse (n = 15, 45.5%). Other demographic characteristics, such as duration of suffering from T2DM, gender, education level, occupation, marital status, hypertension, smoking, family history of DM, and complication, were similar between intervention and control groups (p > 0.05) (Table 1).
Baseline demographic characteristics of respondents of the study.
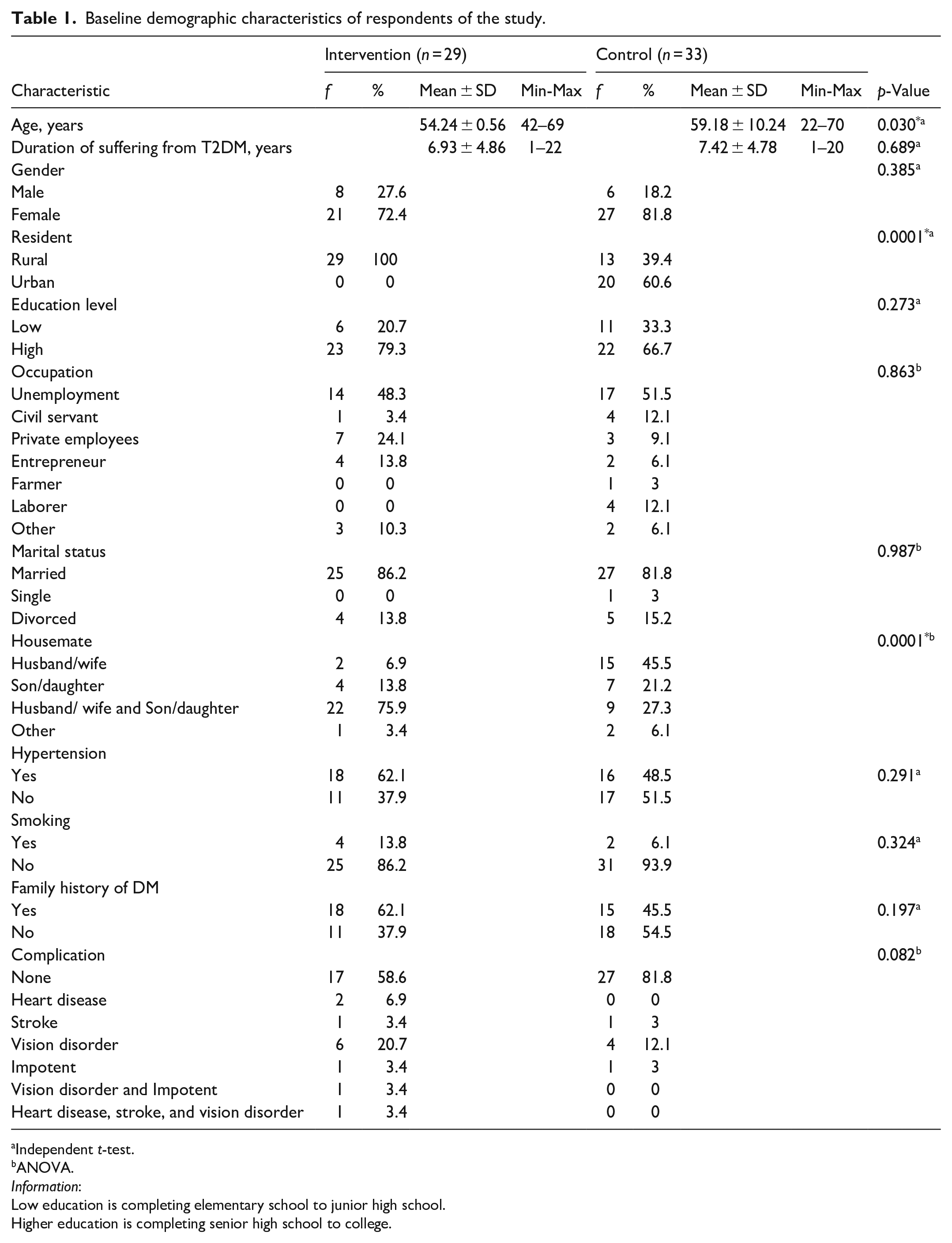
Independent t-test.
ANOVA.
Information:
Low education is completing elementary school to junior high school.
Higher education is completing senior high school to college.
HbA1c level, full self-diabetes management knowledge, and QOL data were collected from 29 respondents in the intervention group out of 33 participants. Meanwhile, complete data were collected from all 33 participants in the control group. Post- HbA1c level on both intervention (9.06 ± 2.05) and control groups (8.64 ± 1.63) are lower than pre- HbA1c level on both intervention (9.56 ± 1.95) and control groups (8.66 ± 1.69), but the decrease was not significant (p > 0.05). Moreover, the difference in the number of HbA1c level reductions between the intervention (−0.503 ± 1.60) and control (−0.018 ± 1.81) groups was not statistically significant (p > 0.271). However, the decrease tended to be greater in the intervention group compared to the control group (Figure 3).
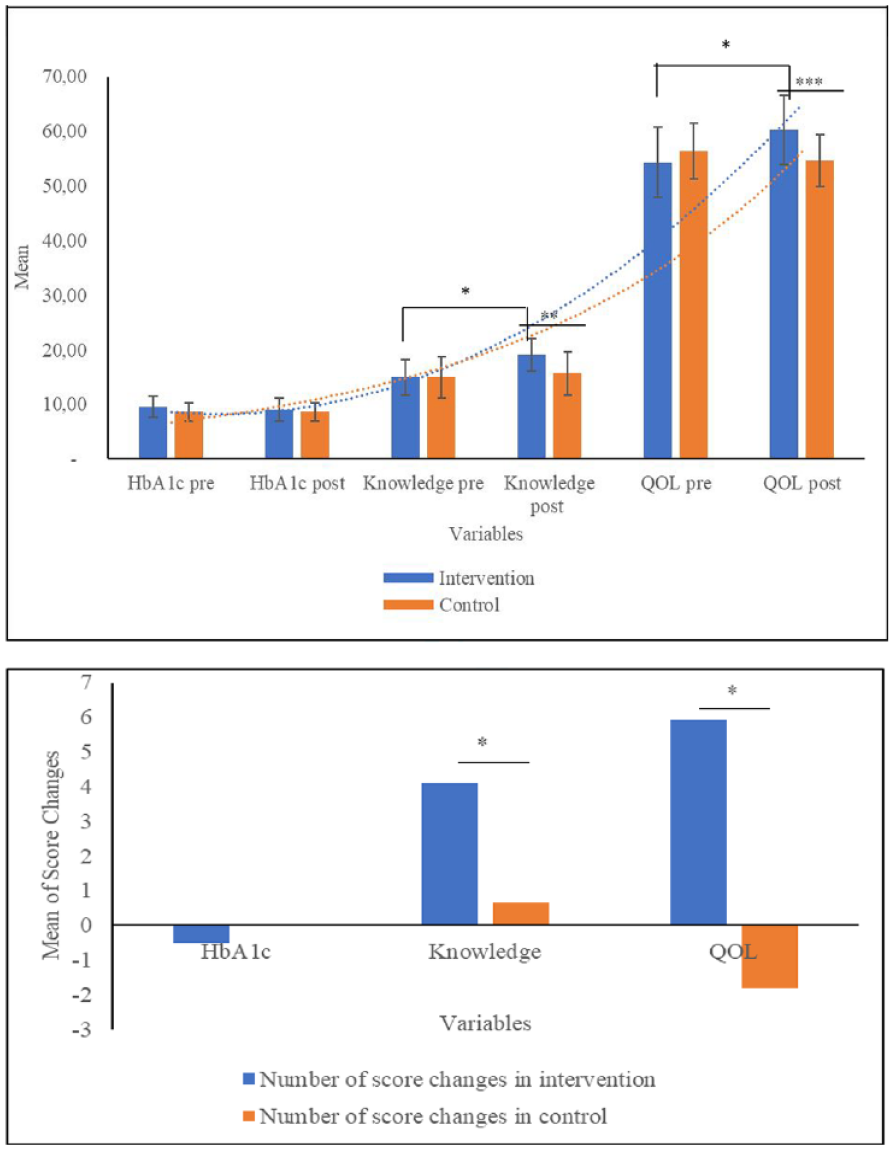
Android Application-based health coaching corroborated to improve self-management diabetes knowledge, and quality of life (QOL) in T2DM patients (*p < 0.05, **p < 0.001, ***p < 0.0001; Independent t-test).
Figure 3 also shows that Android Application-based health coaching helped improve self-management diabetes knowledge, and quality of life (QOL) in T2DM Patients. The knowledge score significantly increased in the post-intervention period of the intervention group (14.97 ± 3.27–15 ± 3.80, p = 0.0001), with an average increase of 4.10 ± 3.49 points. As the increase in knowledge level was higher in the intervention group compared to the control group, there was a significant difference in the average points increase between the two groups (4.10 ± 3.49–0.64 ± 3.96, p = 0.001). A comparison of the QOL scores before and after the intervention showed a significant difference (54.34 ± 6.44–60.28 ± 6.31, p = 0.006). When comparing the change in QOL scores between the intervention group (5.93 ± 6.38) and control group (−1.82 ± 5.19), a significant difference was found (p = 0.0001).
Discussion
The intention behind implementing Android Application-Based Health Coaching was to refocus the approach toward a specific population – T2DM patients – through the design of virtual health coaching using the “Guru Diabetes” application. The program resulted in significant improvements in patients’ knowledge of self-diabetes management and has the potential to improve the quality of life of individuals suffering from T2DM. Unfortunately, although the decrease in HbA1c levels was greater intervention group than in the control group, the difference was not significant. The heterogeneity of respondents’ characteristics such as age, rural or urban residency, and housemates, might have contributed to this finding. Another possible explanation could be found by including the duration of the intervention in the analysis. Similar to our study, a previous health coaching study showed a non-significant decrease in HbA1c after 6 months of intervention, 17 while 12 months health coaching resulted in an improvement of glycemic control. 18 Another study revealed that providing care and support with a mobile phone for 8 months improved clinically relevant diabetes-related health outcomes by increasing knowledge and self-efficacy for self-management behaviors. 19 Another important thing to consider when conducting coaching is to shorten the session and lengthen the duration of each session. 20
By using a mobile phone, Android Application-Based Health Coaching automatically motivates individuals to adopt a healthy lifestyle by predicting health risk early, providing personal recommendation, and evaluating personal goals. 21 A previous study argued that human coaches cannot be replicated with an automated system, as they have to deal with individual as unique individuals, expressing empathy and flexibly expanding the scope of support based on their understanding of their needs. 22 Therefore, this study established virtual health coaching without missing social cues by conducting scheduled small group video calls via WhatsApp. The small group discussion video calls in this study were conducted six times, biweekly, to explore the patients’ goals initially, to motivate them to complete the study, and to identify any barriers to accessing the application. The meetings were fully attended by 80% of respondents.
The study involved in-person interaction conducted via WhatsApp messages or voice calls, based on data inputted in the Guru Diabetes app. Through phone conversations or messaging, coaches were able to assess patients’ condition, instruct them on adopting a healthy lifestyle, and help them set goals and plans for recovery. Patients, in turn, were able to learn about building a healthy lifestyle, resulting in significant improvements in their quality of life and knowledge. The 15–30 min in-person interaction also included feedback on diabetic diet, timely medication use, exercise, self-care, and stress management techniques. During the past 10 years of virtual health coaching studies, it has been found that personal feedback was lacking. 23 Feedback and coaching are most valuable when both patients and coaches exhibit a growth mindset, and when coaching can be provided in the moment and over time.
If people with T2DM could be taught health coaching, which could encourage them to develop healthy habits and improve their ability for self-care, the progression of the disease could be positively affected. With the support of Guru Diabetes Apps, we provided short duration video education about diabetes self-management that could be accessed anywhere and anytime by patients. A study about virtual coaching through short video can build self-awareness, encourage changes in lifestyle, motivate physical activity, and maintain positive interpersonal relationships. 24
We noted limitations of our study. First, caution in interpreting the present findings is advised due to the small number of respondents and heterogeneity in age, residency, and housemates. Second, our study noted that the timing and length of intervention, predictors of success, impact of specific coach-client interaction, and demonstration of increase achievement of sustainable behavioral changes are still in their infancy. Third, the acceptance of technology based intervention is challenging in low socio-economic and rural areas.
Based on the findings of this study, the Android Application-Based Health Coaching has the potential to improve the diabetes self-management knowledge and QOL of T2DM patients. Future study needs to identify trends and generate data that would inform larger, more definitive prospective studies. Additionally, technology anxiety, resistance to change, and a lack of trust in the use of devices for self-management need to be considered when implementing future interventions.
Limitation
The erratic internet connection posed a significant challenge for participants attempting to complete the application, particularly when engaging in video calls. Respondents experienced interruptions or glitches on their mobile devices, leading to forgotten or incomplete application submissions, especially during night time hours.
Footnotes
Author contributions
All authors have contributed significantly and all authors agree with the content of the manuscript.
Availability of data and materials
All data generated and analyzed for the review are available upon request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval and consent to participate
The ethic approval was granted by the Medicine Faculty Ethic Committee (process number: KE/FK/0935/EC/2021). When participants agreed to an initial meeting to discuss the study, their HbA1c findings were verified, the study protocol was explained, and inform consent was obtained. Eligible patients then completed demographic, knowledge, and quality of life questionnaires. All data and information were anonymized according to the International Conference on Harmonization Good Clinical Practice guidelines.
Significance for Public Health Section
Our study found that the Guru Diabetes application enriched diabetes self-management knowledge and improved the quality of life for people living with T2DM. This application can be used to support virtual health coaching conducted in diabetes communities. Additionally, the application can also be used to assist public health centers in providing health education related to diabetes self-management. This application helps T2DM patients to explore their potential in changing their health habits according to their condition. Guru Diabetes App-based health coaching will solve the issue of a lack of nurses, a high workload of nurses and the limit of funds available in public health center.