
Abstract
Background:
Evaluation of coronary flow velocity reserve (CFVR) is the physiological approach to assess the severity of coronary stenosis and microvascular dysfunction. Impaired CFVR occurs frequently in women with suspected or known coronary artery disease. The aim of this study was to assess the role of CFVR to predict long-term cardiovascular event rate in women with unstable angina (UA) without obstructive coronary artery stenosis.
Methods:
CFVR in left anterior descending coronary artery was assessed by adenosine transthoracic echocardiograhy in 161 women admitted at our Department with UA and without obstructive coronary artery disease.
Results:
During a mean FU of 32.5 ± 19.6 months, 53 cardiac events occurred: 6 nonfatal acute myocardial infarction, 22 UA, 7 coronary revascularization by percutaneous transluminal coronary angioplasty, 1 coronary bypass surgery, 3 ischemic stroke, and 8 episodes of congestive heart failure with preserved ejection fraction and 6 cardiac deaths. Using a ROC curve analysis, CFVR 2.14 was the best predictor of cardiac events and was considered as abnormal CFVR. Abnormal CFVR was associated with lower cardiac event-free survival (30 vs 80%, p < 0.0001). During FU, 70% of women with reduced CFVR had cardiac events whereas only 20% with normal CFVR (p = 0.0001). At multivariate Cox analysis, smoke habitus (p = 0.003), metabolic syndrome (p = 0.01), and CFVR (p < 0.0001) were significantly associated with cardiac events at FU.
Conclusion:
Noninvasive CFVR provides an independent predictor of cardiovascular prognosis information in women with UA without obstructive coronary artery disease whereas, impaired CFVR seems to be associated with higher CV events at FU.
Keywords
Introduction
Cardiovascular disease is the leading cause of female mortality in all age groups in Western countries. 1 Although, in recent years the mortality from ischemic heart disease has been reduced, this decrease in women is less consistent than in men, with a worse prognosis and higher mortality in acute myocardial infarction compared with men. 2 Non-obstructive coronary disease is very common in women with suspected ischemic heart disease (IHD) 3 and 10–25% of women admitted for ACS do not have obstructive coronary artery disease.3–5 Although the relationship between coronary microvascular dysfunction (CMD) and atherosclerotic epicardial disease has not yet been fully explained, the main hypothesis is that it is a single disease process, where the response to intimal injury can vary according to sex, to the vascular remodeling and altered vascular reactivity.6,7 In women with initial preclinical atherosclerosis, a CMD is prevalent, and the abnormal coronary reactivity plays an important role in the pathophysiology of ischemic and non-obstructive coronary artery disease, while in men an alteration of endothelial function of epicardial vessels is predominant. 8
The WISE study, demonstrated that the microvascular function, assessed by invasive coronary flow reserve, is able to stratify the prognosis even in women without evident coronary disease at coronary angiography. 9 Therefore, the WISE study group researchers have Jproposed a flow chart that highlights the role of microvascular function evaluation, especially since today it can be studied in a non-invasive way with transthoracic echocardiography.10–13
The purpose of our study was to confirm the prognostic role of impaired coronary flow velocity reserve (CFVR) in the anterior descending coronary artery (LAD) assessed non-invasively by transthoracic echocardiography (TTE) in a female population with suggestive symptoms for unstable angina and in the absence of hemodynamically significant coronary lesions at coronary angiography (INOCA).
Methods
Study group
We studied 161 women mean age 65.2 ± 10.2 years admitted at our Cardiology Department from January 2012 to December 2014 for unstable angina (UA) and referred for CFVR studies for angina and nonobstructive lesion at coronary angiography (coronary stenosis <50%) and we follow them for a mean average of 32.5 ± 19.6 months. None of these patients had a history of asthma or advanced atrio-ventricular block or sick sinus syndrome. Patients with previous myocardial infarction, valvular disease, or patients undergoing PTCA of the left anterior descending artery were excluded from the study.
Study protocol
Echocardiography was performed with different echo machines (Acuson Sequoia™ ultrasound unit Siemens, IE33 Philips, My-Lab 30 gold Esaote) using a broad-band transducer with second harmonic capability. A complete M-mode, two-dimensional echo Doppler (spectral and color) study was performed in all patients, to evaluate cardiac chamber and valve morphology and function. All echocardiographic examinations were performed by the same cardiologist (R.M.). Once the routine echo Doppler examination was completed, CFVR was evaluated by transthoracic Doppler. The method has previously been described in detail.10–13 Briefly, CFVR was evaluated in the LAD by CE-TTE during intravenous adenosine infusion. Adenosine was infused with a controlled-infusion pump (IVAC P4000 Anaesthesia Syringe pump) at an infusion rate of 140 μg/kg/min in 3–5 min. When the pulse wave Doppler pattern was not clearly detectable, a contrast agent (Levovist®, Schering AG, Berlin, Germany or Sonovue ® Bracco) was used as a Doppler signal enhancer. Non-invasive blood pressure and ECG were recorded at rest and every minute during adenosine infusion. Cardiac medications were not interrupted before adenosine, although methylxanthine-containing medications were withheld 48 h before the study. Beverages containing methylxanthine substances (coca-cola, tea, coffee, etc.) were prohibited for 24 h before the study. CFVR in LAD was calculated by one experienced echocardiographer, blind to the clinical data, as the ratio of peak diastolic velocity during hyperemia over peak diastolic velocity at rest (for each parameter the highest of three cycles was averaged.
Statistics
Values were expressed as the mean ± SD for continuous variables and as frequency and percentage for categorical variables. The Student’s t test was used for analysis of continuous data and the χ 2 test or Fisher exact test for categorical variables. Univariate and multivariate survival Cox analysis was performed to determine the risk of events for the variables considered. In order to analyze the predictive power of the CFVR in respect of adverse events, receiver-operating characteristics (ROC) curve analysis was generated. Kaplan-Meier method survival curves were used to summarize the follow-up experience in these patients. The differences in survival curves was tested with a log-rank statistic. In the analysis both deaths from cardiac causes and adverse events such as myocardial infarction, unstable angina, revascularization by angioplasty or bypass, or episodes of heart failure were considered. All data were analyzed by using SPSS 23.0 statistical software (SPSS, Chicago, IL), p = 0.05 was considered to be significant.
Results
Follow-up was attended by all of the 161 patients (100%). Clinical follow-up was performed by direct interview and/or visit of the patient or through an interview with a close relative for died patients. The average duration of follow-up was 32.5 ± 19.6 months. The clinical characteristics of the patients are shown in Table 1.
Characteristics of the study population.

Of the consecutive 161 patients referred to our laboratory, 161 had a diagnostic non-invasive assessment of CFVR (feasibility 100%) including those with large body habitus; 155 pts (96.3%) completed the protocol, 6 pts (3.7%) achieving early maximal vasodilator effect and adenosine infusion was stopped before protocol scheduled time. The test was well tolerated. No major complications were observed during all studies, such as death, myocardial infarction, sustained ventricular arrhythmia, or high degree atrio-ventricular block or convulsive seizures.
At the time of the study, 80% of patients were in menopause, 51% had hypercholesterolemia, 48% had hypertension, and about 20% had diabetes, metabolic syndrome, and were obese (BMI ≥ 30). About 60% were on therapy with cardioaspirin, 50% with beta-blockers and statins. The average value of CFVR in the general population was 2.62 ± 0.74.
During follow-up, there were 53 cardiovascular events (CE) 6 nonfatal myocardial infarction, 22 unstable angina, 7 PCI, 1 CABG, 3 ischemic stroke, and 8 episodes of congestive heart failure with preserved ejection fraction (HFpEF) and 6 cardiac deaths. For each patient it was considered just one cardiovascular event. The clinical characteristics of the patients who presented CE during follow-up are shown in Table 2. It is noted that, the patients who experienced CE at follow-up had a higher prevalence of the metabolic syndrome (30%, 16/53 vs 15%, 16/108, p = 0.02) and a CVFR value significantly lower than in patients without CE (2.17 ± 0.73 vs 2.8 ± 0.65, p < 0.0001).
Characteristics of patients who presented cardiovascular clinical events at follow-up.

Clinical determinants of prognosis
At univariate Cox regression analysis (Table 3) smoke and the presence of metabolic syndrome were directly related to the presence of adverse events at follow-up (p = 0.007), and CFVR was inversely correlated (p = 0.0001), but a history of diabetes mellitus, previous heart attack, family history of ischemic heart disease were not directly related. From the analysis of ROC curves, a value of CFR ≤ 2.14 (altered reserve) was the best predictor of CE (area under the curve = 0.74, p < 0.001, sensitivity 88%, specificity 63%). (Figure 1). In our population, 40 patients (25%) had CFVR ≤ 2.14 (altered reserve) and 121 (75%) a normal CFVR of LAD and event-free survival was significantly less in patients with altered CFVR compared to patients with normal CFVR as shown by Kaplan-Meier curves analysis (30 vs 80%, p < 0.0001, Figure 2). To assess any independent risk factors for CE we used multivariate Cox analysis by introducing into the model all variables statistically significant on univariate analysis or variables tending to significance (p < 0.1). At multivariate analysis, CFVR (HR 3.22, 95% CI 1.81–5.55, p = 0.0001), smoking habitus (HR 3.03, 95% CI 1.47–6.25, p = 0.003), and the presence of metabolic syndrome (HR 2.21, 95% CI 1.19–4.1, p = 0.01) were the only independent predictors of CE at follow-up.
Cox univariate analysis.

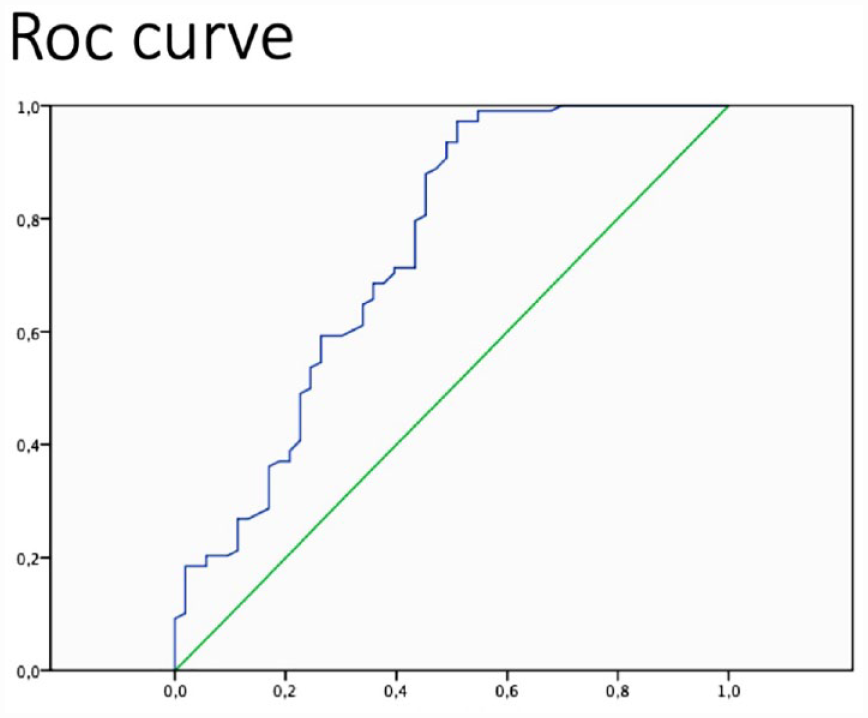
ROC curve that analyzes the predictive role of the coronary flow reserve against adverse events.
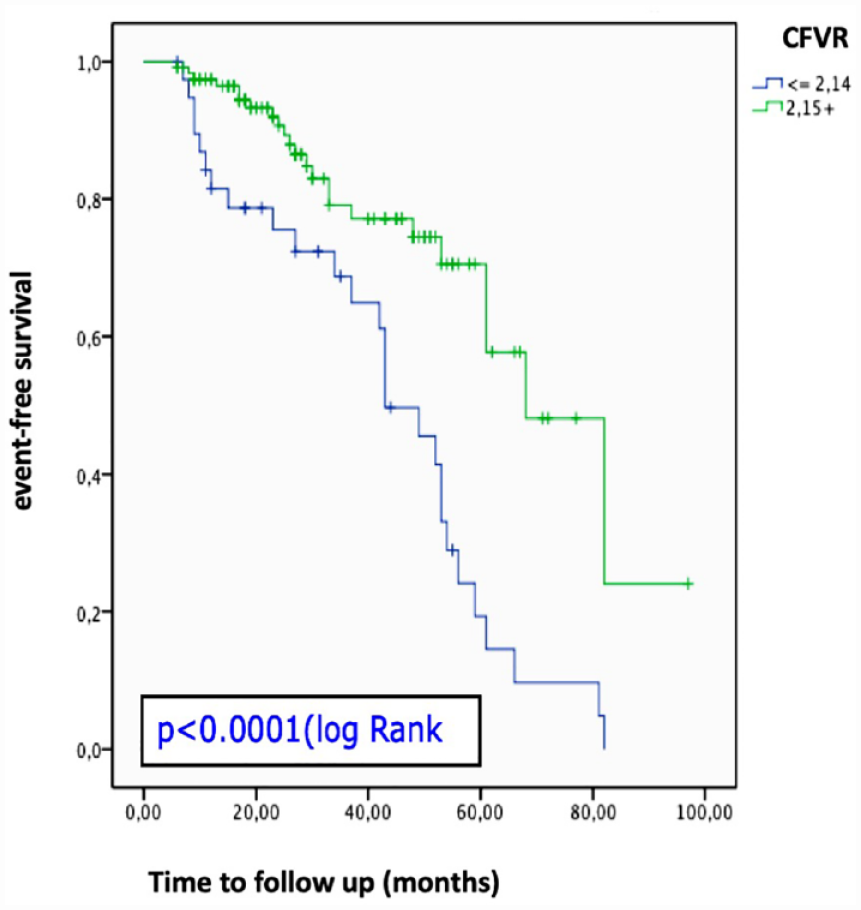
Kaplan-Meier survival curve for the population dichotomized based on the coronary flow reserve value obtained from the ROC curves.
Discussion
Prognostic role of coronary flow reserve
Many women having symptoms and signs suspicious for ACS with normal coronary angiograms show an altered coronary reactivity.5–7 Furthermore, patients with angina and a normal coronary artery represent a very heterogeneous group of patients that includes patients with microvascular angina (MVA), coronary microvascular spasm, and/or vasospastic angina (VSA). 14 Therefore, it would be desirable in these patients to perform an accurate diagnosis of microvascular angina both by the assessment of endothelium-dependent coronary reactivity via acetylcholine infusion and/or independent endothelium coronary reactivity by adenosine. 15 Although, these tests were accurate in assessing CMD and MVA and clinically safe, they are rarely used in routine practice 16 and even in studies such as, WISE no more than 40% of patients perform a complete coronary reactivity evaluation during catheterization. Historically, the presence of symptoms of ischemia in the absence of obstruction of the epicardial vessels was considered an absolutely benign condition, 17 and patients were not specifically treated. However, recent data demonstrate an increase in risk of adverse cardiovascular outcomes in patients, both male and female, with non obstructive coronary artery disease, either with chronic ischemic disease or with acute myocardial infarction or both18–21 emphasizing the role of impaired endothelium and non–endothelium-dependent coronary microvascular reactivity in predicting adverse cardiovascular events. 16 In our population 5% of patients were hospitalized for HFpEF during follow-up and all had reduced CFVR and we know that HFpEF is more frequent in women and impaired CFR is independently associated with diastolic dysfunction and adverse events. 22
CMD is a well recognized prognostic factor in patients with non-obstructive coronary disease, recent meta-analyses have shown that patients with reduced CFVR have a higher incidence of mortality and MACE in follow-up in a wide range of pathologies and independently of the method used to study the CMD 23 and patients are often erroneously reassured that their symptoms are not of cardiac origin.
In the WISE study, women with CFR <2.32 detected with invasive Doppler flow–wire, have a significantly lower event-free survival compared to patients without coronary artery disease but with a normal coronary reserve. 16 Our study shows that 25% of women with UA and non-obstructive coronary disease had impaired CFVR, this data is consistent with the iPower study, 19 where 723 (43%) women with angina-like chest pain and no obstructive coronary artery disease, had markedly impaired CFVR. Our data confirm that non-invasive CFVR studies also in women with ACS/UA and no obstructive coronary artery disease is a largely feasible and safe method to study CMD and impaired CFR after having been adjusted for confounding factors as age, diabetes, and metabolic syndrome, is predictive of cardiovascular events at follow up as shown in other CFVR studies. 23 Former studies have highlighted the prognostic value of non invasive CFVR in patients with suspected ischemic cardiac disease 24 and in different clinical settings.25–28 The evidence found during our experience of the negative prognostic role of the compromised CFVR in the ischemic and non obstructive coronary artery disease, strengthens the pathophysiological role of CMD in ischemic heart disease in women. Impaired CFVR could in fact represent an initial manifestation of the ischemic disease and therefore it could play an important role in the diagnostic and prognostic classification of women with suspicious signs and symptoms for myocardial ischemia representing a new target for assessing the efficacy of new therapeutic interventions. Registry studies indicate that a large amount of patients with symptoms and signs suggestive of IHD have no obstructive coronary artery disease 2 and CMD can contribute to myocardial ischemia, symptoms,4–6,29 and prognosis.16,20 Therefore, in the absence of evidence of obstructive coronary artery disease, regardless of whether a functional or anatomical diagnostic algorithm is used in the suspicion of ischemic heart disease, it is important to rule out CMD with coronary vasomotor function tests, as suggested by different authors.14,16,30 Non-invasive CFVR is a highly feasible, 13 reliable bedside technique, widely available in all cardiology centers, not expensive and accurate to evaluate the effects of epicardial coronary stenosis10–12,31 and coronary microvasculature function.25–28,32,33 Others several non-invasive techniques allow an accurate evaluation of the coronary reserve and microcirculatory function, such as positron emission tomography 20 and cardiac magnetic resonance imaging 34 but they are certainly more expensive and less available and in the case of CMR several patients are excluded for claustrophobia, severe renal impairment, large body size, or patients with pacemakers and implantable cardioverter defibrillators. A hybrid evaluation of the coronary reactivity in these women when using both intra coronary acetylcholine infusion in the cath lab to assess the endothelium-dependent reactivity and intravenous adenosine infusion in the echo lab to assess non–endothelium-dependent microvascular reactivity, could give an easily and complete evaluation of coronary reactivity and a better physiopathological classification of these patients. In our study the impaired CFVR, the smoker habitus and the metabolic syndrome were the only prognostic factors of cardiovascular events at follow-up. Metabolic syndrome was frequent in our population and more prevalent in women with impaired CFVR, confirming the negative role of metabolic syndrome in women. 35 After all, over 80% of our population was in menopause and although WISE data do not support a direct role for estrogen deficiency in the CMD during menopause, the women often present obesity, hypertension, insulin resistance, and dyslipidemia, factors related to metabolic disorder hormone related.
At the present time, there are no targeted therapies for CMD, also because the pathogenesis is multifactorial.16,29 Recently, Ford et al. 14 showed that tailoring medical therapy guided by invasive coronary reactivity testing improves angina in patients with no obstructive CAD. Certainly, as can be seen from the clinical characteristics of our population, there is a strong correlation between the risk factors of atherosclerosis and microvascular dysfunction. Close monitoring of risk factors such as smoking, diabetes, obesity, metabolic syndrome, and hypercholesterolemia is therefore a must in this category of patients. Given this correlation, these patients should be treated as patients with atherosclerotic coronary artery disease. Furthermore, different drugs such as beta blockers, angiotensin converting enzyme (ACE) inhibitors, and high-intensity statins36,37 have shown an improvement in microvascular function. Probably The Women’s IschemiA TRial to Reduce Events In Non-ObstRuctive CAD (WARRIOR) trial 38 which compares intensive medical therapy (IMT) that includes high-intensity statins and angiotensin converting enzyme inhibitors (ACE-I) or receptor blockers (ARB) may indicate a more adequate therapeutic strategy to improve the prognosis of women with microcirculatory dysfunction.
Limitations
The first limitation of our study is the low number of patients. Secondly, we did not subject our patients to a cardiac resonance study to rule out the presence of myocardial fibrosis which certainly has a negative prognostic impact. Moreover, Mygind et al. 39 in the iPOWER study found no correlation between CMD and myocardial fibrosis assessed with cardiac magnetic resonance imaging, suggesting that myocardial ischemia secondary to CMD does not cause myocardial fibrosis. Thirdly, coronary stenosis was defined as >50% lumen diameter narrowing assessed by quantitative angiographic analyses, no intravascular ultrasound or optical coherence tomography were used in our patients, both intra-coronary diagnostic techniques that provide more detailed images of coronary vessels during cardiac catheterization. Lastly, TTE allows the evaluation of CFVR in almost all patients exclusively on the anterior descending artery, and only in 60–70% of patients in the posterior descending coronary artery, but this is not a limitation in the study of CMD which is mostly diffuse in all coronary territories and even in an invasive way, coronary reactivity is evaluated in a single vessel, more often the left anterior descending coronary artery was the preferred vessel. 14
Conclusions
Our study confirms the feasibility and prognostic role of transthoracic echocardiography non-invasive CFVR in women with symptoms and signs of ischemic heart disease in the absence of obstructive coronary lesions, highlighting the important prognostic role of the functional state of the coronary microcirculation in the early stages of atherosclerotic disease. The non-invasiveness of CFVR examination, its safety profile and the low cost make this examination useful in the follow-up of patients with suspected IHD due to the possibility of being able to repeat the exam many times. CFVR could be considered as a routine exam in the diagnostic and prognostic classification of women at risk of cardiovascular disease. At the moment, in the absence of specific treatment, patients with microcirculatory dysfunction should be treated by keeping under careful control cardiovascular risk factors and medications such as statins, aspirin and ace-inhibitors.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent to use medical records for scientific purposes was obtained from all patients. The study was approved by the Ethics Committee of our University Hospital.