
Abstract
Aims
To investigate the different risk factors among different subtypes of patients with acute coronary syndrome (ACS).
Methods
A total of 296 patients who had ACS were retrospectively enrolled. Blood and echocardiographic indices were assessed within 24 hours after admission. Differences in risk factors and Gensini scores of coronary lesions among three groups were analyzed.
Results
Univariate analysis of risk factors for ACS subtypes showed that age, and levels of fasting plasma glucose, amino-terminal pro-brain natriuretic peptide, and creatine kinase isoenzyme were significantly higher in patients with non-ST-segment elevation myocardial infarction (NSTEMI) than in those with unstable angina pectoris (UAP). Logistic multivariate regression analysis showed that amino-terminal pro-brain natriuretic peptide and the left ventricular ejection fraction (LVEF) were related to ACS subtypes. The left ventricular end-diastolic diameter was an independent risk factor for UAP and ST-segment elevation myocardial infarction (STEMI) subtypes. The severity of coronary stenosis was significantly higher in NSTEMI and STEMI than in UAP. Gensini scores in the STEMI group were positively correlated with D-dimer levels (r = 0.429) and negatively correlated with the LVEF (r = −0.602).
Conclusion
Different subtypes of ACS have different risk factors. Our findings may have important guiding significance for ACS subtype risk assessment and clinical treatment.
Keywords
Introduction
Acute coronary syndrome (ACS) is characterized by decreased perfusion of heart muscle, and this includes unstable angina and myocardial infarction. 1 The main pathological feature of ACS is that unstable plaque rupture or erosion leads to complete or incomplete occlusive thrombosis. 2 ACS mainly includes three subtypes, including ST-segment elevation myocardial infarction (STEMI), non-ST-segment elevation myocardial infarction (NSTEMI), and unstable angina pectoris (UAP). 3 STEMI and the NSTEMI are called acute myocardial infarction (AMI). ACS is a serious acute and fatal disease, and has the characteristics of acute onset, rapid development, poor prognosis, and high mortality, thus threatening human health. 4
Many researchers have studied ACS-related risk factors.5,6 Traditional risk factors of ACS include smoking, overweight/obesity, hypertension, hyperglycemia, and hyperlipidemia.7,8 However, in recent years, some new factors have been identified as important independent risk factors for ACS, 9 such as plasma fibrinogen (FiB) levels, 10 serum cystatin C levels, 11 blood uric acid (UA) levels, 12 the neutrophil/lymphocyte ratio 13 and mean platelet volume. 14 Identification of these non-traditional risk factors has provided new basis for prevention and treatment of ACS. The subtypes of ACS and the associated risk factors in Xinjiang, China have not been reported.
This study was designed to investigate the risk factors and coronary lesions of different ACS subtypes, and further analyze their correlations. We hope to provide a theoretical basis for scientific management of cardiovascular risk factors and prevention of ACS.
Materials and methods
Patients
In this retrospective study, consecutive patients who visited the Emergency Department because of chest pain or chest tightness and were admitted to the Heart Center of the First Affiliated Hospital of Xinjiang Medical University from January 2017 to December 2017 were enrolled. All of the enrolled patients underwent percutaneous coronary intervention and had complete clinical data. The diagnosis of enrolled patients was according to the “2015 guidelines for the diagnosis and treatment of acute ST-segment elevation myocardial infarction” 15 and “2012 guidelines for the diagnosis and treatment of non-ST-segment elevation acute coronary syndrome”. 16
Patients who were enrolled in this study met the following inclusion criteria: (1) patients who were admitted with the diagnosis of ACS and fulfilled the criteria of either unstable angina or myocardial infarction;15,16 (2) the time from onset to admission was shorter than 12 hours; (3) patients received both coronary angiography (CAG) and echocardiography; (4) echocardiography and a blood examination for all enrolled patients were performed within the first 24 hours after admission; and (5) the medical history and hematology examination data during hospitalization were complete.
Exclusion criteria included the following: (1) the time from onset to admission was longer than 12 hours; (2) patients who previously had percutaneous coronary intervention or coronary artery bypass grafting; (3) patients complicated by other heart diseases, such as valvular heart disease and congenital heart disease; (4) patients complicated by acute and chronic inflammatory diseases; and (5) patients suffering from severe liver and kidney failure, autoimmune diseases, blood diseases, active infectious diseases, and malignant tumors.
No potentially identifiable human images or data are shown and we have de-identified all patients’ details. Verbal informed consent was obtained from each patient. This study was approved by the Ethics Committee of the First Affiliated Hospital of Xinjiang Medical University in January 2017, in Urumqi, Xinjiang, China (approval no: 20150225-80). Our study complied with the STROBE guideline.
Data collection
Basic information of patients with ACS included blood pressure, heart rate, age, sex, height, weight, body mass index, smoking history, hypertension, diabetes, history of dyslipidemia, and family history of coronary heart disease. The results of laboratory tests included the neutrophil/lymphocyte ratio, the platelet/lymphocyte ratio, red blood cell distribution width, mean platelet volume, levels of plasma FiB and D-dimer, serum cystatin C, and blood UA, N-terminal pro-brain natriuretic peptide (NT-ProBNP), high-sensitivity C-reactive protein (hs-CRP), creatine kinase enzyme (CK-MB), high-sensitivity troponin T (hs-cTnT), total cholesterol (TC), triglycerides (TG), low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C), fasting blood glucose (FBG), and glycated hemoglobin A1C (HbA1C), left ventricular ejection fraction (LVEF), and left ventricular end-diastolic diameter (LVEDD). Among the traditional and non-traditional risk factors of ACS, blood and echocardiographic indices were assessed within 24 hours after admission.
CAG
CAG was performed in all patients. ACS was defined as the presence of >50% coronary artery stenosis in any coronary artery or left main artery. The diagnosis of ACS was made by at least two experienced interventional physicians. Using a double-blind approach, the interventional physician was unaware of the patient’s case data.
The modified Gensini score 17 was used to assess the severity of coronary lesions. This score was categorized as follows: 1 point if the stenosis was < 25%; 2 points if the stenosis was between 26% and 50%; 4 points if the stenosis was between 51% and 75%; 8 points if the stenosis was between 76% and 90%; 16 points if the stenosis was between 9l% and 99%; and 32 points if the stenosis was 100%. On the basis of the Gensini score, the results of coronary lesions were divided into the three following groups: mild stenosis group (Gensini score of 0–30 points), moderate stenosis group (Gensini score of 30–60 points), and severe stenosis group (Gensini score >60 points).
The lesion coefficients were defined as follows: the lesion coefficient of the left main branch lesion was 5; the proximal, middle and distal lesion coefficients of the anterior descending or circumflex artery were 2.5, 1.5, and 1, respectively; and that of the right coronary lesion was 1. Additionally, the following lesion coefficients were defined: the lesion coefficient of the D1 diagonal branch lesion was 1; that of the D2 diagonal branch lesion was 0.5; that of the blunt limb branch lesion was 1; that of the right posterior descending branch lesion was 1; that of the left ventricular posterior branch lesion was 1, and that of the posterior branch lesion was 0.5. The Gensini score = ∑ (degree of coronary stenosis × lesion coefficient).
Additionally, according to the results of CAG, the Killip classification, lesion vascular site, lesion vessel count, lesion coronary score, and Thrombolysis in Myocardial Infarction blood flow grading were recorded. The lesions were recorded as left anterior descending lesions, left circumflex lesions, and right coronary artery lesions. When the degree of stenosis of any lesion was >50%, it was defined as single-vessel stenosis. If this condition occurred in two or three vessels, it was defined as double-vessel stenosis or three-vessel stenosis, respectively. A left main branch lesion was classified as two-vessel stenosis.
Statistical analysis
Statistical analysis was performed by using IBM SPSS 22.0 software (IBM Corp., Armonk, NY, USA). Non-parametric tests were performed on all measurement data. Measurement data that conformed to a normal distribution are expressed as mean ±standard deviation, and the t-test or one-way analysis of variance was used for comparison between groups. For measurement data that did not conform to a normal distribution, the median value (25th percentile, 75th percentile) was used and comparison between groups was performed by the independent sample rank sum test. Count data are expressed by number and percentage, and comparison between groups was performed by the chi-square test. Correlation analysis of continuity variables with a non-normal distribution was performed using the Spearman test. Using the three subtypes of ACS as the dependent variables, multiple risk factors with significant differences were analyzed by multivariate logistic regression analysis. A p value <0.05 was considered statistically significant.
Results
Patients
A total of 296 patients were included in the study. Among them, there were 220 male patients and 76 female patients, and the ratio of male to female patients was 2.9:1. The mean age of the enrolled patients was 59.49 ± 12.44 years.
Univariate analysis of risk factors for different ACS subtypes
We performed univariate analysis to compare the differences in risk factors of different subtypes of ACS. Age, FBG levels, NT-ProBNP levels, and CK-MB levels in the NSTEMI group were significantly higher than those in the UAP group, and LVEF was significantly higher than that in the STEMI group (all p < 0.05) (Tables 1 and 2). Levels of TG, LDL-C, HDL-C, FiB, D-dimer, NT-ProBNP, CK-MB, and hs-CRP, LVEF, and LEVDD in the STEMI group were significantly higher than those in the UAP group, and CK-MB levels were significantly higher than those in the NSTEMI group (all p < 0.05). The proportion of patients with hypertension in the UAP group was significantly higher than that in the STEMI group (p < 0.05). Therefore, different subtypes of ACS had different risk factors.
Differences in traditional risk factors for different ACS subtypes.

Data are mean ± standard deviation or n (%).
ap < 0.05, comparison between the UAP and NSTEMI groups; bp < 0.05, comparison between the UAP and STEMI groups.
ACS, acute coronary syndrome; UAP, unstable angina pectoris; NSTEMI, non-ST-segment elevation myocardial infarction; STEMI, ST-segment elevation myocardial infarction; BMI, body mass index; FBG, fasting blood glucose; HbA1C, glycated hemoglobin A1c; TC, total cholesterol; TG, triglycerides; LDL-C, low-density lipoprotein cholesterol; HDL-C, high-density lipoprotein cholesterol.
Differences in non-traditional risk factors for different ACS subtypes.
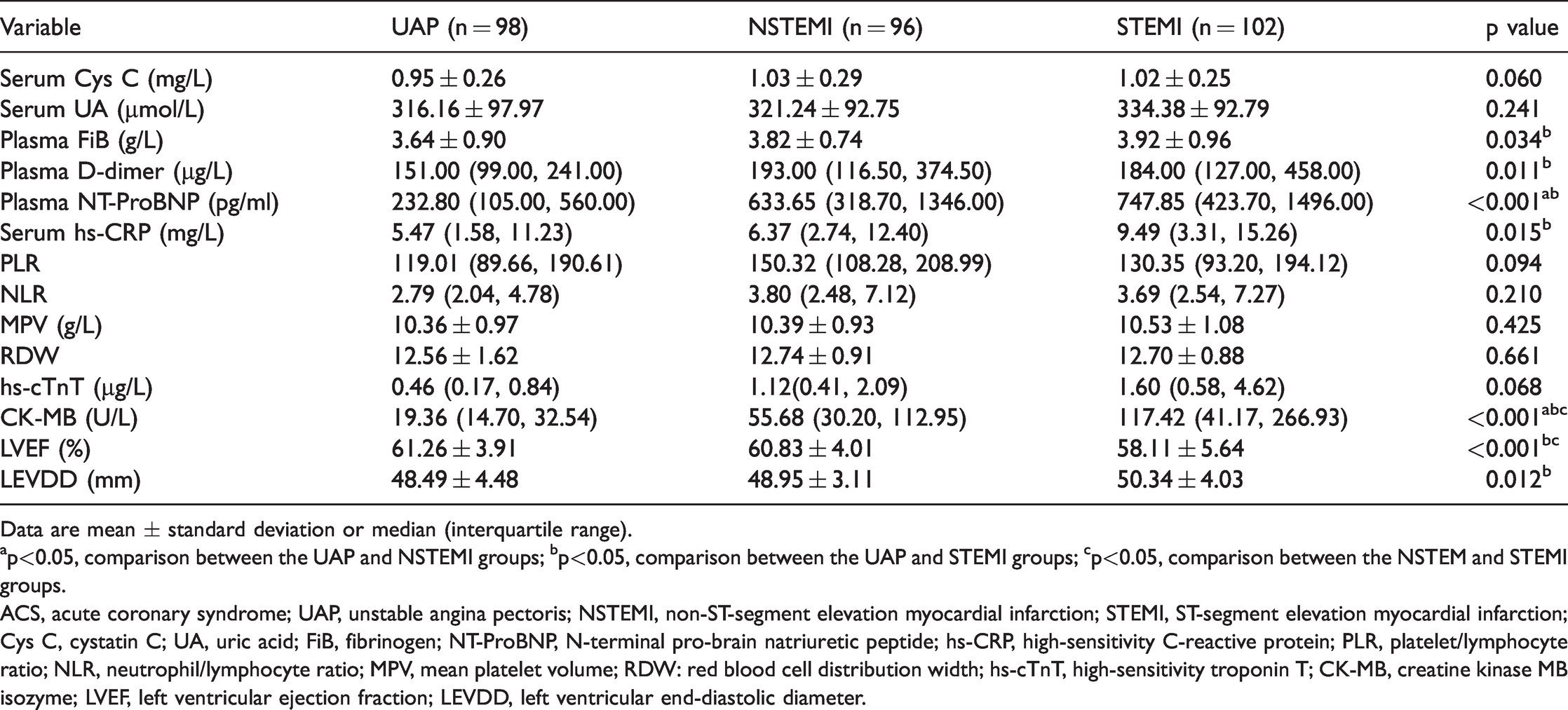
Data are mean ± standard deviation or median (interquartile range).
ap<0.05, comparison between the UAP and NSTEMI groups; bp<0.05, comparison between the UAP and STEMI groups; cp<0.05, comparison between the NSTEM and STEMI groups.
ACS, acute coronary syndrome; UAP, unstable angina pectoris; NSTEMI, non-ST-segment elevation myocardial infarction; STEMI, ST-segment elevation myocardial infarction; Cys C, cystatin C; UA, uric acid; FiB, fibrinogen; NT-ProBNP, N-terminal pro-brain natriuretic peptide; hs-CRP, high-sensitivity C-reactive protein; PLR, platelet/lymphocyte ratio; NLR, neutrophil/lymphocyte ratio; MPV, mean platelet volume; RDW: red blood cell distribution width; hs-cTnT, high-sensitivity troponin T; CK-MB, creatine kinase MB isozyme; LVEF, left ventricular ejection fraction; LEVDD, left ventricular end-diastolic diameter.
Multivariate logistic regression analysis of risk factors for different ACS subtypes
Logistic multivariate regression analysis was performed with the three ACS subtypes as dependent variables, and significant factors that affected the ACS subtypes, including age, levels of TG, LDL-C, HDL-C, FBG, NT-ProBNP, CK-MB, FiB, D-dimer, and hs-CRP, LVEF, LEVDD, and hypertension, as independent variables. NT-ProBNP levels, LVEF, and LEVDD were significantly associated with UAP (all p < 0.05). NT-ProBNP levels, LVEF, and hs-CRP levels were significantly associated with NSTEMI (p < 0.05). NT-ProBNP levels, LVEF, LEVDD, and LDL-C levels were significantly associated with STEMI (all p < 0.05) (Table 3).
Multivariate logistic regression analysis of factors affecting ACS subtypes.

ACS, acute coronary syndrome; SE, standard error; OR, odds ratio; CI, confidence interval; UAP, unstable angina pectoris; NT-ProBNP, N-terminal pro-brain natriuretic peptide; LVEF, left ventricular ejection fraction; LEVDD, left ventricular end-diastolic diameter; NSTEMI, non-ST-segment elevation myocardial infarction; hs-CRP, high-sensitivity C-reactive protein; STEMI, ST-segment elevation myocardial infarction; LDL-C, low-density lipoprotein cholesterol.
Comparison of coronary lesions in different ACS subtypes
The mean Gensini scores of coronary lesions in the UAP, NSTEMI, and STEMI groups were 53.35 ± 43.65, 70.20 ± 41.35, and 77.55 ± 43.80, respectively (Table 4), with a significant difference among the three groups (p < 0.05). The degree of coronary stenosis was significantly higher in the NSTEMI and STEMI groups than in the UAP group (p < 0.05).
Comparison of different coronary artery lesions in different subtypes of ACS.
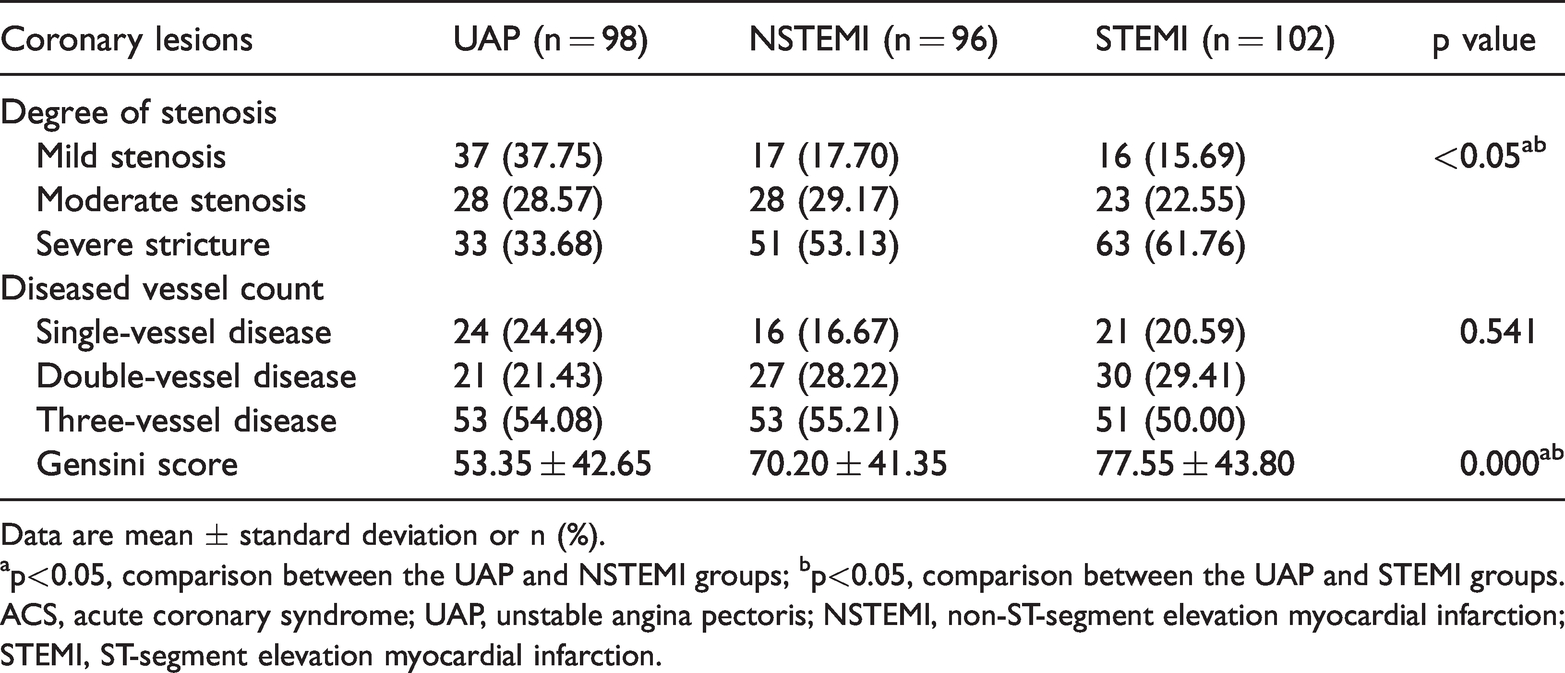
Data are mean ± standard deviation or n (%).
ap<0.05, comparison between the UAP and NSTEMI groups; bp<0.05, comparison between the UAP and STEMI groups.
ACS, acute coronary syndrome; UAP, unstable angina pectoris; NSTEMI, non-ST-segment elevation myocardial infarction; STEMI, ST-segment elevation myocardial infarction.
Correlation analysis between the Gensini score of different ACS subtypes and their risk factors
Spearman correlation analysis was performed on the Gensini scores of different ACS subtypes and their risk factors. We found that the Gensini score in the UAP group was positively correlated with NT-ProBNP levels (r = 0.548, p < 0.05) (Table 5). The Gensini score in the NSTEMI group was positively correlated with NT-ProBNP, FiB, and hs-CRP levels (r = 0.482, r = 0.277, and r = 0.324, respectively; p < 0.05). Additionally, the Gensini score in the NSTEMI group was negatively correlated with HDL-C levels (r = −0.325, p < 0.05). The Gensini scores of STEMI group were positively correlated with NT-ProBNP and D-dimer levels (r = 0.429 and r = 0.556, respectively; p < 0.05), and negatively correlated with LVEF (r = −0.602, p < 0.05).
Correlation analysis between Gensini scores of different ACS subtypes and their risk factors.

Data are r values with p values in parentheses.
ACS, acute coronary syndrome; UAP, unstable angina pectoris; NSTEMI, non-ST-segment elevation myocardial infarction; STEMI, ST-segment elevation myocardial infarction; HDL-C, high-density lipoprotein cholesterol; NT-ProBNP, N-terminal pro-brain natriuretic peptide; hs-CRP, high-sensitivity C-reactive protein; FiB, plasma fibrinogen; LVEF, left ventricular ejection fraction.
Discussion
We retrospectively studied the risk factors of different ACS subtypes. Multivariate logistic regression analysis showed that NT-ProBNP levels and LVEF were related to the three different ACS subtypes, especially for STEMI. LEVDD was an independent risk factor for UAP and STEMI, and it showed a significant effect on STEMI. The level of hs-CRP was an independent risk factor for NSTEMI, and LDL-C levels were an independent risk factor for STEMI. In brief, our data showed that there were differences in independent risk factors for different ACS subtypes.
We also performed Spearman rank correlation analysis on the severity of coronary artery stenosis (Gensini score) and risk factors in different ACS subtypes. We found that the degree of coronary artery stenosis was positively correlated with NT-ProBNP levels. Additionally, the degree of coronary artery stenosis was positively correlated with FiB levels in the NSTEMI group, positively correlated with D-dimer levels in the STEMI group, negatively correlated with LVEF in the STEMI group, and negatively correlated with HDL-C levels in the UAP group. Therefore, our study suggests that different indicators should be used to assess and predict the degree of coronary stenosis in different ACS subtypes.
Studies have shown that the NT-ProBNP level is important predictor of cardiovascular events and severity of coronary artery disease in patients with ACS.18,19 When ventricular myocytes are stimulated by volume load, hypoxia, and ischemia, a large amount of NT-ProBNP is released. 20 As the ischemic burden caused by myocardial infarction increases, more myocardial cells are damaged and higher NT-ProBNP levels are released into the blood. 21 In this study, plasma NT-ProBNP levels in patients in the NSTEMI and STEMI groups were significantly higher than those in patients in the UAP group. NT-ProBNP levels in different ACS subgroups increased with the severity of coronary artery disease. This finding indicates that NT-ProBNP levels may be used as an independent predictor for myocardial ischemic necrosis and severity of coronary artery disease, which is consistent with a previous report. 22
The LVEF and LVEDD are commonly used indicators to evaluate left ventricular systolic function. Myocardial ischemic necrosis causes abnormal ventricular wall pulsation, uncoordinated function, and decreased heart function, which further lead to enlargement of the LVEDD and a reduction in the LVEF. 23 Our study showed that the LVEF in the STEMI group was lower than that in the UAP group, and the LVEDD was significantly higher than that in the UAP group. This finding indicates that there may be ventricular remodeling after AMI. Moreover, Spearman correlation analysis was performed on the Gensini scores of different ACS subtypes and their risk factors. We found that the Gensini scores in the STEMI group were negatively correlated with the LVEF, suggesting that a lower LVEF may predict more severe coronary stenosis.
Levels of hs-CRP are the most important indicator for inflammation, and can promote adhesion and migration of inflammatory cells to the vascular endothelium, thereby initiating and accelerating development of atherosclerosis. 24 Tanveer et al. 25 showed that instability of atherosclerotic plaques was positively correlated with hs-CRP levels. Studies have reported that plasma hs-CRP levels are an effective indicator for assessing the vulnerability of coronary atherosclerotic plaques, which could reflect the severity of coronary artery lesions in patients with ACS.26,27 Our study showed that hs-CRP levels were an independent risk factor for NSTEMI. The level of hs-CRP increased with the severity of coronary lesions.
Coagulation and abnormalities of fibrinolysis play an important role in the occurrence and development of ACS. High FiB levels lead to increased blood viscosity, induction and promotion of accumulation of red blood cells and platelets, and acceleration of thrombosis. These are considered to be a potential risk factor for ACS. 28 Peng et al. 29 retrospectively analyzed the cumulative survival curves of 2253 patients with ACS and found that elevated FiB levels increased all-cause mortality and cardiac mortality in patients with ACS. Therefore, elevated FiB levels have a predictive value for the risk of death in patients with ACS. Our study demonstrated that FiB levels reflected the severity of coronary artery disease in patients with NSTEMI.
D-dimer is a specific product of fibrin degradation and elevated levels of D-dimer aggravate endothelial cell dysfunction, 30 which in turn induces aggravation of myocardial damage. Reihani et al. 31 found that plasma D-dimer levels could be used as a marker with high sensitivity and specificity to distinguish between AMI and UAP. Similarly, we also found that plasma D-dimer levels were significantly higher in patients with STEMI than in patients with UAP, and there was a close correlation between D-dimer levels and severity of coronary lesions. Therefore, plasma FiB and D-dimer levels in patients should be tested on admission.
Excessive LDL-C levels and/or low HDL-C levels lead to impaired endothelial function, accelerating the formation of atherosclerotic plaques. 32 Therefore, LDL-C and HDL-C can be used as risk factors for atherosclerotic lesions.33,34 Wang et al. 35 showed that LDL-C was a risk factor for ACS and could be used as an effective indicator for assessing the vulnerability of coronary atherosclerotic plaques. Islam et al. 36 also found that HDL-C levels were significantly negatively correlated with cardiovascular risk, and contributed to risk stratification and management in patients with ACS. Additionally, elevated HDL-C levels reduce the risk of cardiovascular disease. 36 Our study showed that LDL-C was an independent risk factor for STEMI. HDL-C levels were negatively correlated with coronary artery stenosis in patients with UAP.
There are some limitations to this study. First, this was a single-center, retrospective study. Second, the study population was the local population in Xinjiang, which may have resulted in bias caused by regional differences. Third, the number of cases included in this study was small. Fourth, a prediction model was not established. Therefore, a prospective, large-scale, multicenter study with a large number of enrolled subjects should be performed to further investigate and validate the relevant risk factors for different subtypes of ACS and their effect on prognosis.
In summary, our study shows that hs-CRP is an independent risk factor for NSTEM, LDL-C is an independent risk factor for STEMI, and LVEDD is a common independent risk factor for UAP and STEMI. These findings suggest that the risk factors of different ACS subtypes and the severity of coronary lesions are different. Moreover, different risk factors have different effects on the degree of coronary artery disease in different ACS subtypes. Therefore, analysis of the differences in risk factors will be helpful in individualized prevention and treatment and will have important guiding significance for assessment of risk and clinical treatment of different ACS subtypes. Strengthening intervention of risk factors of ACS subtype is important for prevention and treatment of cardiovascular complications and improvement of prognosis.
Footnotes
Author contributions
Juledezi Hailati, Lei Zhang, Xiaoyun Ma, Jiangping Liu, Zhiqiang Liu, Yuchun Yang, and Pengyi He performed the study. Juledezi Hailati, Lei Zhang, and Xiaoyun Ma analyzed the data. Lei Zhang, Juledezi Hailati, and Xiaoyun Ma wrote the manuscript. Muhuyati Wulasihan designed the study, collected funds, and reviewed the manuscript.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Natural Science Foundation of China (81760062).