
Abstract
Background:
Community-Based Health Insurance (CBHI) scheme refers to a non-profit type of health insurance for the informal sector. There is a paucity of information on this topic in Gudeya Bila, Ethiopia. This study aimed to assess the level of household (HH) satisfaction with the CBHI scheme and its associated factors.
Method:
A community-based cross-sectional study design was employed from November 1–30, 2020, and a sample of 630 HHs who enrolled in the CBHI scheme were included. A multi-stage sampling and systematic random sampling were employed. Data was entered into Epidata version 3.1 and analyzed using SPSS for windows program version 25. A 95% CI was calculated and variables having p-value < 0.05 were considered statistically significant. Descriptive statistics, bivariate, and multivariable logistic regression analyses were performed.
Result:
All HHs heads (630) with a response rate of 100% were involved in the study. The overall HH satisfaction on CBHI was 56.2%. Attending CBHI scheme-related meetings (AOR = 1.948, 95% CI = 1.16–3.27), healthcare provider respectfulness (AOR = 9.209, 95% CI = 2.73–31.06), able to get the ordered laboratory test service (AOR = 2.143, 95% CI = 1.127–4.072) and having paid extra money for drug supply at private health facilities (AOR = 0.492, 95% CI = 0.285–0.847) were independent predictors.
Conclusion:
HH satisfaction level on CBHI scheme was moderate. Attending CBHI scheme-related meetings, health-care provider respectfulness, being able to get the ordered laboratory test services and extra payments for drug supply were significant predictors of satisfaction with CBHI. Therefore, attention should be given to increasing the satisfaction of HHs with CBHI through improving the quality of health services.
Significance for the public health
Findings of this study will be used as baseline in filling the gap of information to increase the percent of CBHI enrollment in the catchment area. Besides, the result of this study will be used for health service planners and health managers for decision making on factors those affect the satisfaction of HHs on CBHI scheme. Further the findings obtained from this study will be used as base line for other researchers and will be used to improve health services for the community. A clear understanding of the factors associated with HH satisfaction on CBHI will help in deciding which interventions will have the greatest impact in improving HH satisfaction.
Background
Community-based health insurance (CBHI) schemes are an emerging and growing tool for providing financial protection to deprived individuals against health-related events. 1 Health insurance is one sustainable financing recommended by World Health Organization as part of Universal health coverage. 2 Globally, about 150 million people suffer financial catastrophe annually while 100 million are pushed below the poverty because of medical expenses. In some countries, up to 11% of the population suffers catastrophic expenditure for paying for their care which leads them to severe financial hardship each year, and up to 5% household forced into poverty due to health care expenses. 3 In developing countries, out- of-pocket (OOP) payments for healthcare financing aggravate the existing poverty. Low-Income countries face substantial challenges in financing healthcare. For many people health spending through OOP payments is difficult and due to this reason, millions of people fall into poverty. Also, in settings that lack effective health insurance policies, the poor people in low-income countries still suffer and die from health-related problems.4,5
Low-income countries face considerable challenges in financing healthcare. Public services are unavailable and unaffordable to the majority of poor people in these countries. Millions of people in developing countries still suffer and die from health-related conditions for which effective but underutilized interventions exist, particularly in settings that lack effective health insurance policies.6,7 Governments of low-income countries face the challenge of reducing the regressive burden of out of pocket (OOP) expenditure by expanding prepayment schemes that spread financial risk and reduce the spectrum of catastrophic healthcare expenditure. 8 There is some evidence that CBHI schemes have, on a small scale, played a role in reducing OOP payments and CBHI can potentially contribute to the empowerment of poor people in relation to health providers and policy-makers. However, literature on health insurance in low-income countries shows that, members of CBHI often continue to depend on out-of-pocket expenditure to cover more than 40% of their health needs. 9
In Sub-Saharan Africa, out-of-pocket health spending constitutes a significant proportion of household expenditures, thereby exposing households (HHs) to a high risk of impoverishment and potential worsening of already poor health outcomes. 10 In Ethiopia from the total health expenditure the share of household contribution was 33% and most of this expenditure was OOP expenditure. Ethiopian Health Sector Transformation Plan (HSTP-I) targets to establish CBHI schemes in 80% of woredas and enroll at least 80% of HHs to reduce OOP health expenditure to less than 15%. 11
To overcome financial hardship, a national implementation pilot CBHI scheme was started in Ethiopia in mid-2011 as a pilot in 13 woredas of Oromia, Amhara, Southern Nations Nationalities and Peoples and Tigray regions.12,13 Until 2018, 39% of districts in the country had started the scheme with total enrollment rates in these woredas remain only 44% and nationally 15%. Recent reports indicates that there is low population coverage of 28% (in-country level) compared to the target set in HSTP-I (health sector transformation plan), 80%, and only 77% of CBHI enrolled households are renewing their membership cards that mean 23% of them are dropped out from CBHI enrollment due to dissatisfaction with CBHI scheme. 11
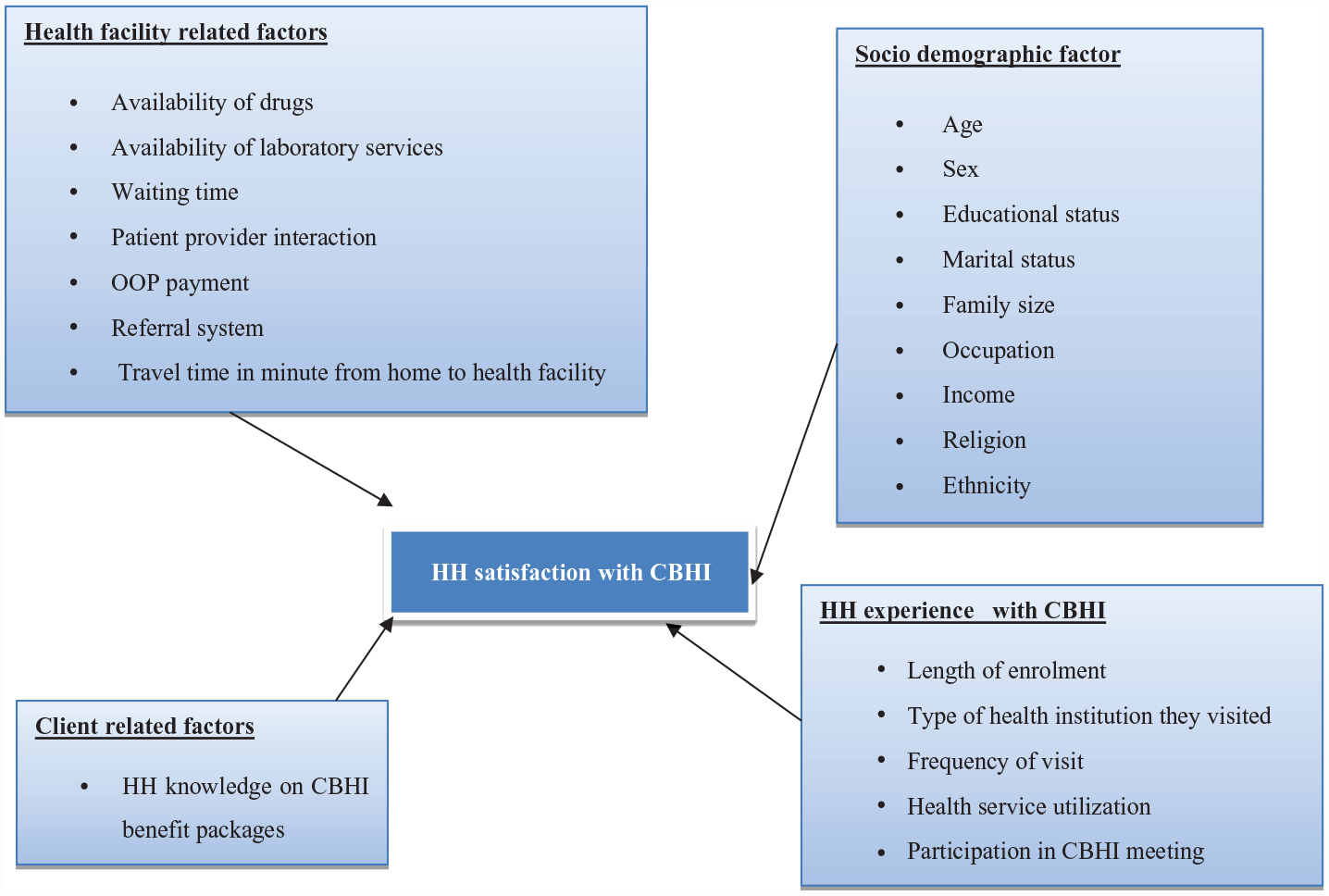
By 2014, extensive training and sensitization were given to district officials, kebele officials, health workers, health extension workers, community workers and community members on CBHI scheme as well as registering members has been started in study area. CBHI services were begun in Gudeya Bila district in October 2015 in all four health centers of catchment area. 14 To evaluate the quality and the effectiveness of various health care service deliveries, assessment of client satisfaction is very important. Consumer satisfaction with healthcare services is associated with contributing factors such as healthcare delivery process and health providers. 15 In Gudeya Bila district the enrollment coverage of households in CBHI scheme is 32% and the dropout rate is 12%. The CBHI scheme has been scaled up in this study area since the end of 2015. However, the enrollee’s magnitude of satisfaction and associated factors are not yet known. Despite the government emphasis on CBHI scheme expansion, household satisfaction and associated factors on CBHI scheme are not yet assessed in this study area whether this scheme satisfies enrollees and they have a positive perception toward the CBHI scheme. Then, assessing HHs’ satisfaction and identifying the associated factors influencing HH satisfaction on CBHI scheme is important in the country and the study area in particular. Therefore, this study aimed to assess the level of household’s satisfaction on CBHI scheme and its associated factors in the study area (Figure 1)
Methods and materials
Study area and period
Gudeya Bila is one of the districts in the East Wollega Zone and located at 252 km toward West of Addis Ababa (the nation capital). Based on 2020/2021 of Central Statistics Agency estimation the total population of the district are 78,906 of which 40,242 females and 38,664 males. About 4816(32%) HHs form total of 16,058 HHs enrolled to CBHI program. The district has 15 Kebeles (the smallest administrative unit in Ethiopia) and there are four governmental health centers and 15 health posts that provide health service for the community. The primary health potential coverage of the district is assumed to be 100%. From district health office up to health post level, it is staffed with 73 health workers with different professions, 37 health extension workers and 48 non-technical staffs with a total human power of 158. 18 The district made contractual agreement with Sire primary hospital, Ethiopia and CBHI beneficiaries are allowed to access hospital without penalty with a health center referral. The study was conducted from November 1-30, 2020.
Study design
➢ A community-based cross-sectional study was conducted among randomly selected households who are enrolled in to CBHI schemes in Gudeya Bila district.
Population
➢ All households those enrolled in CBHI scheme in Gudeya Bila district from November 1-30, 2020 was taken as the source population. While, sampled households those enrolled in CBHI scheme in selected kebeles through multi-stage sampling method during the specified period was taken as the study population.
Eligibility criteria
➢ HHs head whose age is ≥ 18 years and enrolled and visited health facilities were included. While, HHs enrolled to CBHI scheme but who were displaced from selected kebele during data collection were excluded.
Sample size determination and sampling procedure
Sample size determination
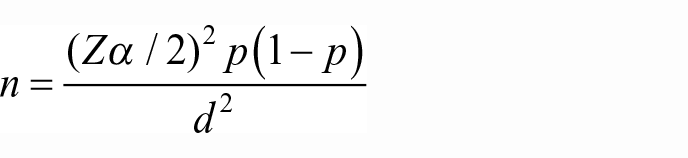
Sample size was calculated by using the single population proportion formula by assuming 54.7% of HHs enrolled in the CBHI scheme was satisfied with CBHI, 3 a confidence level of 95%, a 0.05 margin of error. Since the two-stage sampling was used, the sample size considers a design effect of 1.5.
Where:
n = calculated sample size
z = Confidence interval [95%]
d = margin of error at 0.05
p = proportion of household’s satisfaction with CBHI scheme which is 54.7%.
By substituting in to the formula we get the sample size

The calculated sample size was 381.Finally, multiplying by a
Sampling procedure
There are 15 kebeles found in the study area and the schemes were initiated in all kebeles. 18 A multi-stage sampling technique was employed to select the study participants. We applied simple random sampling method at each stage to select Kebeles. In the first stage, 50% of kebeles were selected using a lottery method and by this eight Kebeles were selected. In the second stage, households enrolled and visited health facilities with CBHI in the selected kebeles were identified using their enrollment identification numbers from the quarterly report registration book (the book that was written for the financial report from health centers to district CBHI facilitating office were used). Then, the sample size is proportionally allocated to each kebele according to their enrolled HH size.
Finally, the study participants were selected using systematic random sampling methods from registration book list at every Kth household in the frame from each kebele until sample size of that kebele reached as showed in this formula:

Sampling procedures among household satisfaction and associated factors with Community Based Health Insurance Scheme in Gudeya Bila District, East Wollega Zone, Oromia Region, Ethiopia, 2020.
Study variables
Dependent variable
➢ Level of household satisfaction on CBHI scheme (satisfied/unsatisfied).
Independent variables
➢
➢
➢
➢
Operational definitions
➢
➢
➢
➢
➢
Data collection tools and procedures
The structured questionnaire adapted from previous similar studies after repetitive reviewing2–4,16,17,19 was used. The questionnaire contains five sections which are socio-demographic characteristics of HHs (10 items), HH experience with CBHI (13 items), HH knowledge on CBHI benefit packages (seven items), health facility related services (13 items) and HH satisfaction on CBHI related questions (10 items by using a five-point Likert scale from strongly dissatisfied = 1 to strongly satisfied = 5). The data were collected by eight health extension workers under the supervision of two public health officers, who were capable of speaking Afaan Oromo. Face-to-face interview was administered to collect the data from study subjects.
Data quality assurance
To assure quality of data 1-day training was given for eight data collectors and two supervisors by the principal investigator on how to fill data on the prepared questionnaires. All collected data were checked for completeness, and consistency by the supervisor every day and onsite close supervision and technical supports was given by supervisors and principal investigator. The questionnaire was prepared in English and then translated from English to Afaan Oromo. Before the actual data collection, pre-testing was done by the data collectors on 32 persons (5% of sample size) in Gobu sayo district of East Wollega Zone and appropriate modifications were made after analyzing the pre-test result.
Data processing and analysis procedures
The data obtained were entered in to Epidata version 3.1 and analyzed using SPSS windows version 25. Before final analysis the principal investigator performed data cleaning by looking at the distribution of the data, identifying outliers and checking back against the original data and analysis of descriptive statistics was carried out first. After completing the descriptive part of analysis, logistic regression analysis was used to determine factors associated with satisfaction to CBHI service package. First, bivariate analysis was carried out to assess the association of each independent variable with HH satisfaction on CBHI scheme. All independent variables with p-value of <0.20 and their crude odd ratio (COR) in bivariate logistic regression were entered into multivariate analysis to control confounding factors. The goodness of fit test was checked by Hosmer Lemeshow test was found to insignificant (p-value = 0.163), an omnibus test was significant (p-value = 0.000) which indicates the model was fitted. Adjusted odds ratio (AOR) along with 95% CI was estimated to identify factors associated with the magnitude of household heads satisfaction with the CBHI scheme by using multivariable logistic regression analysis. Finally, variables whose p < 0.05 in multivariable logistic regression were considered as the cutoff point for statistical significance.
Satisfaction on CBHI was assessed using 10 questions based on Likert scale ranging from strongly dissatisfied (1) to strongly satisfied (5). The internal consistency of the 10 items using Cronbach’s alpha was 0.869. For each question there is a response from 1 to 5 and the sum of responses for all questions was scored. After adding all 10 responses, we got a total satisfaction score of 20,094 and for each individual ranging from 15 to 50. From this total satisfaction by using SPSS we got a median value = 32. By using this median value (32) as a cutoff point, we have a dichotomized dependent variable either satisfied (total satisfaction ≥32) or unsatisfied (total satisfaction <32).
Ethical consideration
Before any attempt to collect the data, approval to conduct the study was obtained from Wollega University Ethical Review Committee. After this Gudeya Bila district administration was informed on study aim and objective and then the study permission was obtained and formal letter of consent from the administration was obtained. Each study participant was informed about the purpose of the study, the right to refuse to participate in the study, and confidentiality of the information was kept. They assured that they were not penalized for not participating if they wish not to participate and verbal consent was obtained from participants.
Result
Socio demographic characteristics of the respondents
A total of 630 respondents (502 males and 128 females) were participated in the interview making a response rate of 100%. The majority of respondents (82.4%) were married to one spouse. More than three-fourth (78%) of the respondents lives in rural area. The average family size was 5.8. Regarding their educational level, 339(53.8%) were attended grade 9 and above. About 601(95.4%) of the respondents were Oromo in ethnicity. Averagely, the respondents have annual income of 18,903 ETB (SD = 12,062) (Table 1).
Socio-demographic characteristics of respondents in Gudeya Bila District, East Wollega Zone, Oromia Region, Ethiopia, 2020 (N = 630).

Household experience with CBHI scheme
Household heads that had at least one family member that had fallen sick and visited health facilities at least one time since enrolled in CBHI scheme were included in this study. Among interviewed, about 51.4% of respondents were visited both health centers and hospitals in order to get health services when they were sick and 24.1% of them visited more than five times since enrolled in the CBHI scheme. The respondents were also interviewed about their experience in CBHI scheme. Accordingly, 69% of the enrollment was done by health extension workers (HEWs) and followed by health care professionals which accounts for 18%. About 84% of the respondents renewed their membership while the rest are new. The total average time of enrollment is 2.71 year. Most of respondents 67% said they become CBHI members because of CBHI premium is cheaper when compared to OOP and about 30.6% of respondents enrolled in to CBHI schemes because of illness or injuries occur in the household frequently. About 56.3% of respondents were participated in CBHI scheme related meeting and about 76% of respondents said that CBHI schemes need to be scale up to other districts and majority of (97.5%) respondents want to stay enrolled in the CBHI scheme (Table 2).
Respondents experience on CBHI scheme in Gudeya Bila District, East Wollega Zone, Oromia Region, Ethiopia, 2020 (N = 630).

Knowledge of households on CBHI benefit packages
The knowledge of respondents about CBHI was assessed using seven questions. Each question was based on a “yes” or “no” responses. Accordingly, 573(91%) of the respondents were responded “yes” ≥4 out of seven questions and they were taken as knowledgeable about CBHI benefit packages (Table 3).
Respondents knowledge on CBHI benefit packages in Gudeya Bila District, East Wollega Zone, Oromia Region, Ethiopia, 2020 (N = 630).

Access to health services
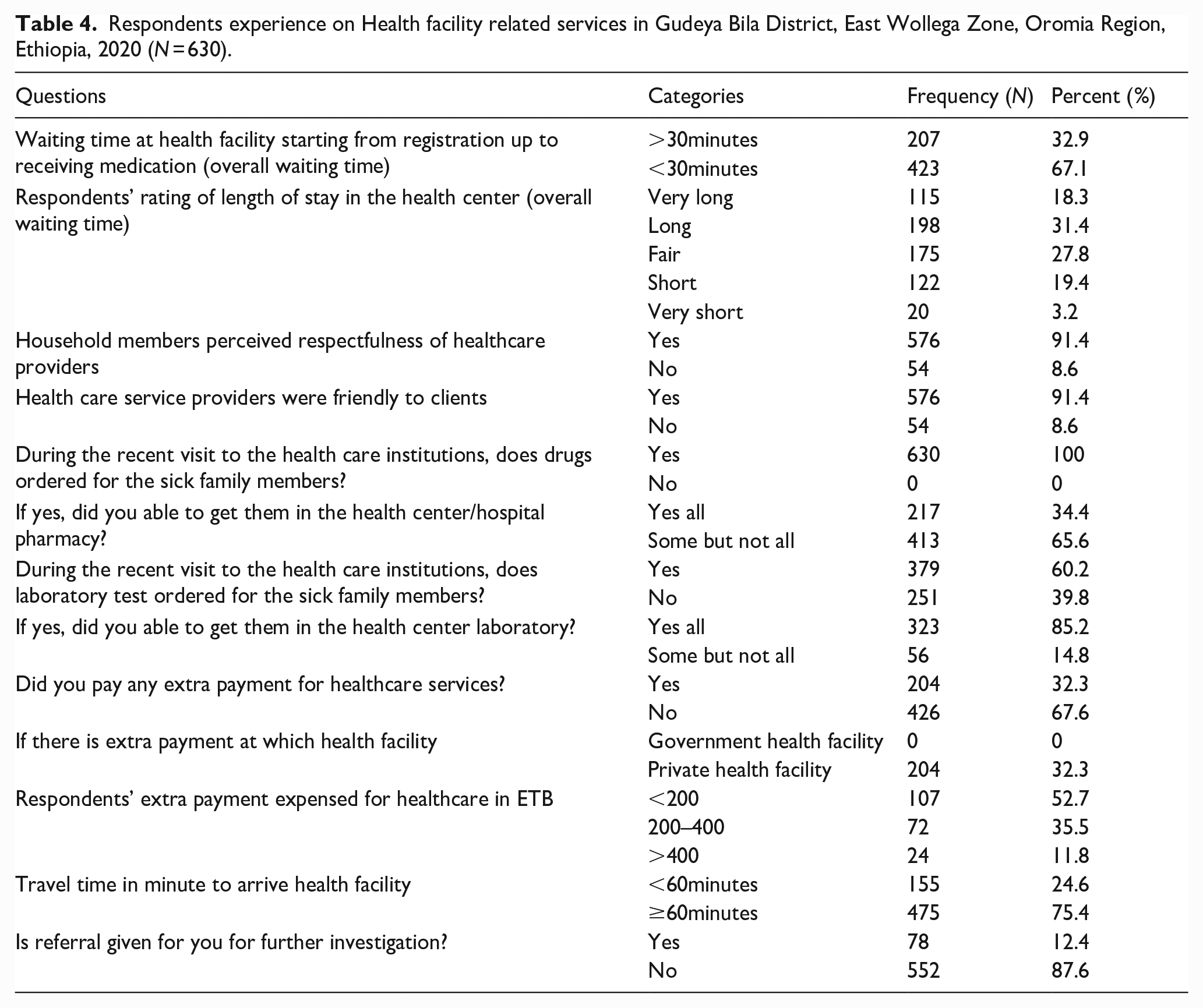
Nearly one-third (31.4%) of the respondents consider the waiting time to be long while about more than a quarter (28%) considered it as fair. Majority (91.4%) of the respondents said they got respect from healthcare providers. From the total respondents got prescription, only 34.4% of respondents get all the prescribed drugs from government health facilities. Laboratory services were ordered for 60.2% of respondents and of this, only 85.2% of them get all the ordered laboratory test services. About 204(32.3%) clients have paid extra money for service at private facilities when drug is not available in the health center or hospital. Respondents’ extra payment ranges from 45ETB to 800ETB and on average, the respondents have paid 240 ETB extra payments at private health facilities for drug supply which is not available in the health center or hospital additionally on CBHI premium (Table 4).
Respondents experience on Health facility related services in Gudeya Bila District, East Wollega Zone, Oromia Region, Ethiopia, 2020 (N = 630).
Level of satisfaction of the respondents with CBHI scheme
Satisfaction to CBHI was assessed using 10 questions based on Likert Scale ranging from strongly dissatisfied (1) to strongly satisfied (5). For each question there is a response from 1 to 5 and the sum of responses for all questions was scored (Table 5).
Respondents level of satisfaction on CBHI schemes in Gudeya Bila Woreda, East Wollega Zone, Oromia Region, Ethiopia, 2020 (N = 630).

The overall satisfaction level of HHs on CBHI scheme
The median score of satisfaction level was 32. Respondents who scored more than or equal to 32 were considered as satisfied on CBHI, while those who scored less than median score were considered as unsatisfied. Of total respondents, 354(56.2%) of them scored more than the median satisfaction level and they were satisfied and whereas the left 276(43.8%) scored less than median satisfaction level. Based on this fact, 56.2% of respondents were satisfied on CBHI scheme in the study area during the study period (Figure 3).
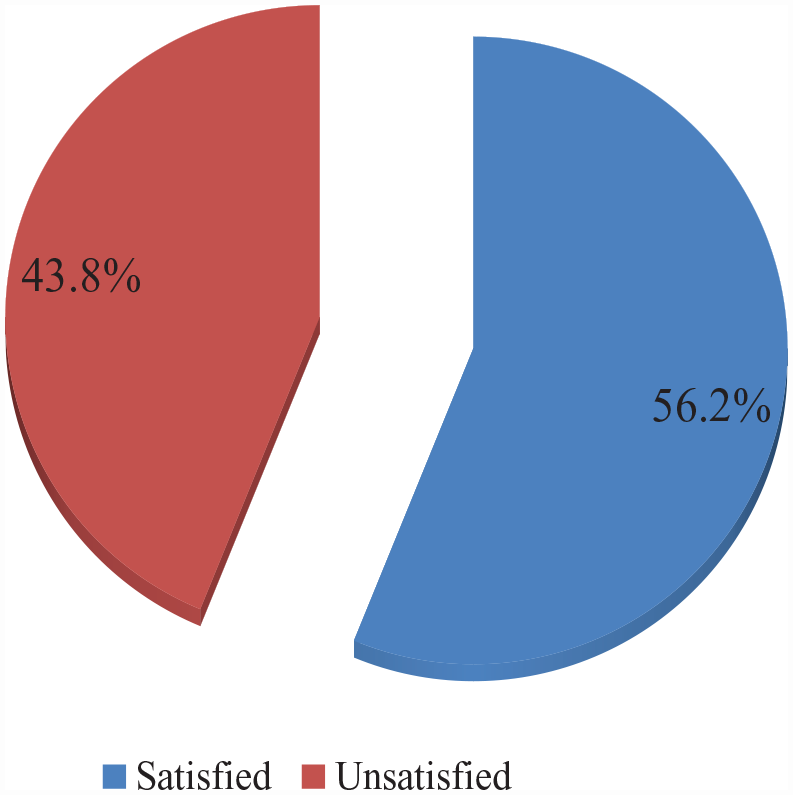
Overall satisfaction level of HHs on CBHI scheme in Gudeya Bila District, East Wollega Zone, Oromia Region, Ethiopia, 2020.
Factors associated with respondent’s satisfaction on CBHI schemes
In bivariate analysis 11 variables having p-value < 0.20 included in multivariable analysis. These variables were; marital status, occupation, residence, type of enrollment, participating CBHI scheme related meeting, provider respectfulness, able to get ordered laboratory test service, extra payment for drugs, waiting time, travel time and family size (Table 6).
Bivariate and Multivariable Logistic regression analysis results on factors associated with HH’s satisfaction on CBHI schemes in Gudeya Bila District, East Wollega Zone, Oromia Region, Ethiopia, 2020 (N = 630).
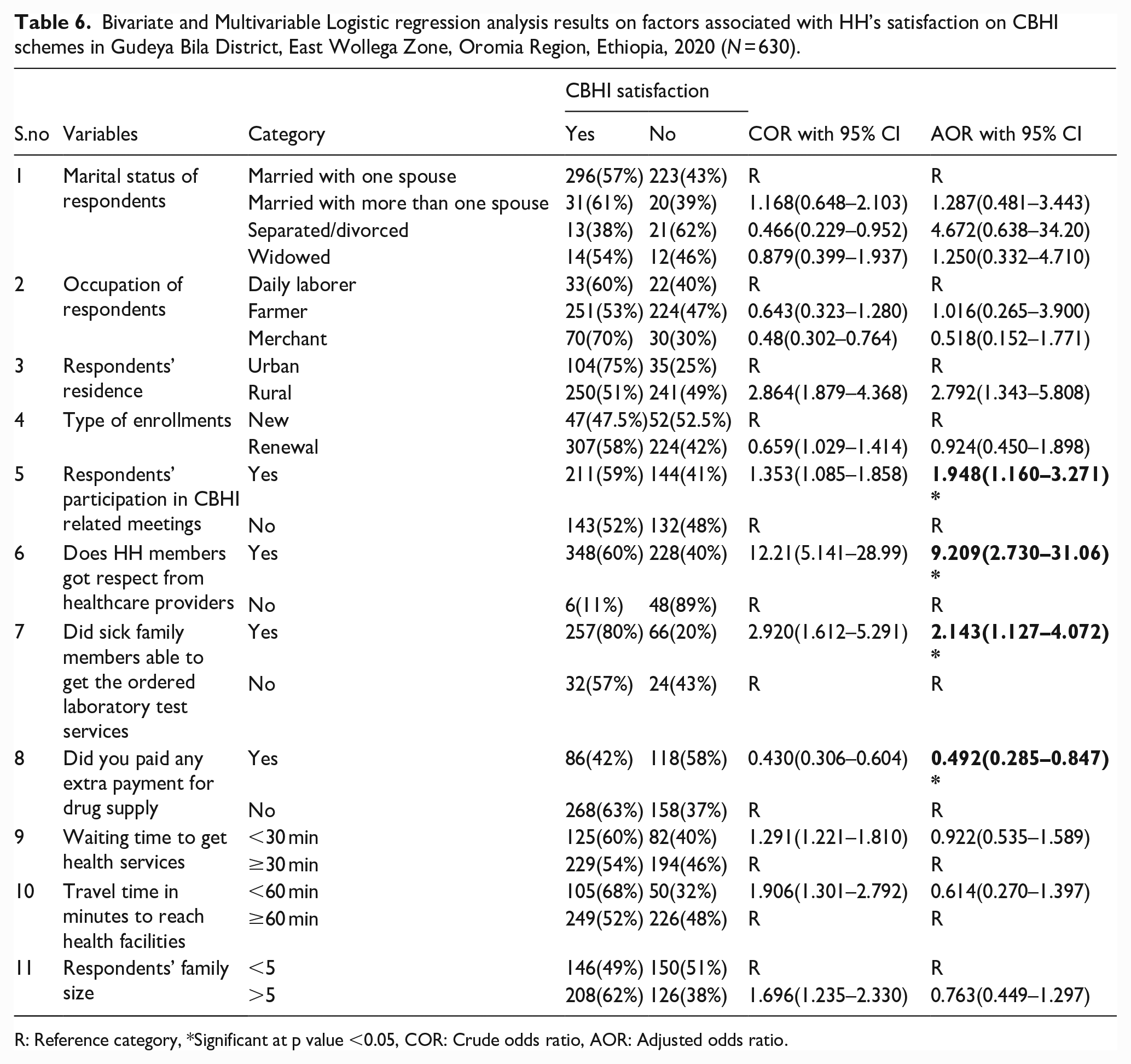
R: Reference category, *Significant at p value <0.05, COR: Crude odds ratio, AOR: Adjusted odds ratio.
Among the independent variables entered into multivariable analysis; participation of CBHI schemes related meeting, household members who get respect from healthcare providers, sick family members able to get the ordered laboratory test services and paying extra money for drug supply were factors significantly associated with outcome variable. The odds of household head satisfaction were 1.948 times higher for HHs participating in CBHI schemes related meeting than those not attended the meeting (AOR = 1.948, p = 0.012, 95% CI = 1.160, 3.271). For those household heads who get respect from healthcare providers, the odds of household head satisfaction were 9.209 times higher than those who did not get such respect (AOR = 9.209, p = 0.000, 95% CI = 2.730, 31.06). The odds of household head satisfaction were 2.143 times higher for sick family members who get the ordered laboratory test services than those who did not get such service (AOR = 2.143, p = 0.020, 95% CI = 1.127, 4.072). The odds of household head satisfaction were 0.049 times less for HHs having paid extra money for drug supply when compared with those enroll who get the prescribed drugs (AOR = 0.049, p = 0.011, 95% CI = 0.285, 0.847) (Table 6).
Discussion
The overall satisfaction level of households on CBHI scheme in Gudeya Bila District during the study period was 56.2%. This result was in line with the study conducted in Sheko district, Southwest Ethiopia and Anilemo District, Hadiya Zone, Southern Ethiopia which showed household satisfaction on CBHI is 54.7% and 54.1% respectively.4,18 However, the finding was lower than the study conducted in Damotwoyde district, Wolaita Zone, Ethiopia in which the household satisfaction on CBHI schemes was 91.38%. 16 In contrast, the study conducted on household satisfaction with health insurance in Nigeria indicated the clients’ satisfaction of 42.1% which is lower than what was revealed by this study. 19 This variation may be due to the study settings, socio-demographic characteristics of respondents and duration of study period. 18
Participation in community-based health insurance schemes related meetings were significantly associated with satisfaction of HHs on CBHI schemes in the study area. The possible explanation were respondents who attend the meetings may have basic understanding of the role of CBHI; how the CBHI scheme works and know what is being offered by the scheme. Out of respondents who attended CBHI related meeting, majority of them had good knowledge on CBHI benefit packages. Such participation may help enrollments to know their right and responsibility and may help them to ask the needed health services according to the contractual agreement. It is in line with study conducted in Kilte Awelaelo District, Tigray Regional State Ethiopia, which indicated that, attending CBHI related meeting have positive impact to participate in the scheme. 5
As cited in this study, healthcare providers’ respectfulness during service provision makes a significant association with HHs’ satisfaction on CBHI scheme. In agreement with this finding, studies revealed that healthcare provider respectfulness during service provision determines their level of satisfaction and healthcare provider respectfulness during service provision increased satisfaction of respondents with CBHI scheme.16,20 Besides, the study conducted in health care facilities of North Shewa Zone, Ethiopia have showed that respectful care of health work force is a deep sense to alleviate clients suffering, developing the inner sense, sharing their pain to address patients core needs. 21 Such healthcare providers’ respectfulness may increase satisfying to working environment and leads to fewer complaints of clients and create better relationship between health workers and patients which may leads to HH satisfaction on CBHI scheme and increase the quality of health care.
Among health services, laboratory service is one measure that proved quality of services in a health facility. Among health facility related services, laboratory service was positively associated with satisfaction of HHs on CBHI schemes in the study area. As indicated in this study, respondents who get the ordered laboratory test services had 2.143 times more likely to be satisfied. This association may be suggesting that accessibility of health services determines the satisfaction of HHs to community-based health insurance scheme. In agreement with this study, other studies have revealed that laboratory service determines HH level of satisfaction on CBHI and improved laboratory services were one of the reasons for HH’s satisfaction.4,16,20
Extra payment due to lack of services in the health facilities is one factor that members couldn’t resist since CBHI program is launched to minimize catastrophic extra payments. According to this result, HHs who paid extra payment for drug supply had less likely satisfied on CBHI scheme than those who get prescribed drugs. This finding was in line with different studies conducted at different sites.20,22 This may be due to enrolled HHs did not get the ordered drugs in health facilities and enforced to buy drugs from privet clinics which might be the reason for less satisfaction of households on CBHI schemes.
Different studies revealed that, among the major factors that make the client dissatisfied with the health care services at public health institutions is lack of drugs in the health facilities. In line with this finding, the study conducted in Tigray regional state showed that HHs were exposed to extra payments at time of service. 20 In similar way study conducted in South Wollo Zone revealed that, large numbers of households were exposed for additional healthcare payment even if they are member to CBHI scheme. 22
According to this finding and different studies,5,20,22 members of CBHI schemes which are expected to get service without any extra payment at the time of service are now obliged to pay for drug supplies. Such experience may hinder members from renewing their membership which may leads to dropouts from the scheme and non-members from enrolling in CBHI scheme since there is still extra payments are requested.
Strength and limitation of the study
As the strength of the study, the primary data were collected from community which may reveal the real picture exist in the community. As a limitation, it was only focused on the demand side point of view (households who enrolled), and the supply side view (provider side) was not explored.
Conclusion and recommendation
Conclusion
The level of household heads satisfaction toward CBHI scheme at the study area was moderate. Households’ attending CBHI scheme related meeting, Household members who get respect from healthcare providers, and sick family members who able to get the ordered laboratory test services were found to be positively associated to satisfaction of HHs on CBHI scheme. This study also revealed that extra payments for drug supply at private health facilities during services was found to be negatively associated with satisfaction of HHs on CHBI scheme.
Recommendation
Based on this finding, we recommend for Gudeya Bila district betterment especially on identified determinant factors of HH satisfaction as follows:
➢ The district health office and health facility management committee should look for different mechanisms to enable catchment health facilities to have essential drugs and supplies.
➢ Health facility management bodies should give attention to laboratory services and making the services easily accessible for the enrolled members all the time.
➢ CBHI scheme board and management bodies are recommended to conduct continuous supervision of HH satisfaction level to deduce methods to improve health care service delivered by health facilities.
➢ It is highly suggested that, a detailed and extensive study should be conducted by adding qualitative aspects to get the clear picture of the whole situation of the problem.
Footnotes
Acknowledgements
We are grateful to all staff of Wollega University Institute of Health Science School of Public Health for their valuable contribution and unreserved cooperation during the study. We also extend our thanks to data collectors, respondents, and supervisors for their valuable effort and participation during study.
Authors’ contributions
All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval and consent to participate
Before any attempt to collect the data, approval to conduct the study was obtained from Wollega University Ethical Review Committee. After this Gudeya Bila district administration was informed on study aim and objective and then the study permission was obtained and formal letter of consent from the administration was obtained. Each study participant was informed about the purpose of the study, the right to refuse to participate in the study, and confidentiality of the information was kept. They assured that they were not penalized for not participating if they wish not to participate and verbal consent was obtained from participants.
Consent for publication
“Not applicable”
Availability of data and materials
The finding of this study was generated from the data collected and analyzed based on stated methods and materials. The original data supporting this finding are available from the corresponding author on reasonable request.