
Abstract
The cost of healthcare is an issue of concern for both consumers and funders of healthcare in South Africa. The country spends approximately 8% of GDP on health care. Health care is financed through the public sector which covers 86% of the population and the private sector which covers 14% of the population. Medical schemes are the main source of healthcare financing in the private sector. Services covered by medical schemes include chronic diseases, emergencies, diagnosis, and treatment of a selected number of diseases. Primary health care services such as screening are limited. The aim of this study was to assess factors associated with members of medical schemes’ willingness to pay for a primary health care package in the private sector. A cross-sectional survey was conducted amongst principal members of medical schemes between July and September 2020. All principal members with access to an online questionnaire were eligible to participate in this study. Logistic regression was used to identify factors associated with willingness to pay for primary health care services. A total of 6512 members of medical schemes participated in the study. Thirty-five percent of the participants were willing to pay for the primary health care package. Factors influencing willingness to pay included marital status, employment status, income and household size. The study highlights the need for policymakers to consider socioeconomic factors when designing health care policies.
Introduction
The rising cost of healthcare and the rising burden of diseases is an issue of concern worldwide. 1 In South Africa, health care is financed through the public sector which covers approximately 86% of the population and the private sector which covers approximately 14% of the population. 2 In 2020, both sectors spent approximately 8.6% of Gross Domestic Product (GDP) on healthcare with nearly 50% attributed to private sector spending. 3 Medical schemes are the main source of funding for health care in the private sector. Membership on a medical scheme is voluntary and any person above 18 years, not a member of any other medical scheme and able to pay monthly contributions is eligible to become a principal member. 4
According to the Medical Schemes Act, medical schemes are mandated to provide a set of benefits called Prescribed Minimum Benefits (PMBs) to prevent members from incurring catastrophic health care expenses. The PMBs include a list of 26 chronic diseases, 271 conditions (known as diagnosis treatment pairs) and any emergency medical condition. 5 The current PMBs are said to be “hospicentric” as most of the services are accessed in a hospital setting. 6 Even though chronic non-communicable diseases (NCDs) such as hypertension, and diabetes remain the most prevalent conditions in the private sector, primary health care services such as prevention remain limited for members of medical schemes. Over the years, many stakeholders have commented that the PMBs are not responsive enough to the changes in healthcare needs of the population, current health technology and best clinical practice, burden of disease, health policy; as well as the financial impact on medical schemes and members. 7
The Medical Schemes Act makes provision for the PMBs to be reviewed every 2 years to address inconsistencies in regulations and to include health technologies that are cost-effective. 7 In line with the Council for Medical Schemes’ (CMS) proposal to implement decisions and policies based on evidence, a willingness to pay (WTP) study was considered necessary to provide evidence on members of medical schemes’ willingness to pay for a primary health care (PHC) package. Whilst WTP for health insurance studies have been conducted in several countries, the services individuals are willing to pay and factors associated with WTP may differ by country. For example, in Saudi Arabia, respondents were willing to pay approximately 40 USD a month for a National Health Insurance. 8 Factors associated with WTP included age, region, and education of participants. In Nigeria, households heads were willing to pay 1.68 USD per person per month for a contributory health insurance scheme. 9 Household size, level of education, occupation and household income were shown to have an influence on participants’ WTP. In South Africa, Chiwire et al assessed willingness to pay for public primary healthcare services among people attending primary health care centers in Cape Town. Overall, 60% of participants were willing to pay an average of R49.44 (<3 USD) for primary health care at public facilities. Factors associated with willingness to pay included employment, the facility providing care, the mode of transport and the frequency of visits to facilities. 10
For the private sector, it is not yet known whether medical schemes members are willing to pay for primary health care services. This study is relevant, as the current PMB package has limited PHC services. This study therefore aims to assess members of medical schemes’ WTP for the PHC package and factors that might influence WTP.
Methods
A cross-sectional survey was undertaken amongst principal members of medical schemes in South Africa between July and September 2020. In 2020, approximately 4 million people were principal members of medical schemes in South Africa. All principal members with access to an online questionnaire were eligible to participate in this study. Email letters with a link to the study questionnaire were sent to all medical schemes in South Africa with a request to forward the invitation and link to all their principal members to take part in the study. The invitation included a consent from which members were requested to sign if they were willing to participate with an option to opt in and out of the study at any given point.
Sampling
A nonprobabilistic method was used to draw the sample from the population. Based on the primary outcome of willingness to pay, a binary outcome yes/no, and assuming a binomial distribution, the sample size was calculated on this distribution.

Where n is the sample to be calculated and p is the population from which the sample is determined. The total sample size was estimated at 960 after considering a population size of approximately 4 million, 95% confidence level, 5% margin of error and a design effect of 2 and 10% non-response rate.
Data collection instrument
An online questionnaire was developed in line with previous studies to explore members’ WTP for a PHC package.11,12 Google survey was used to collect data on socio-demographic characteristics, health-related characteristics and WTP. The questionnaire included a cover letter explaining the purpose of the study. The questionnaire was pretested on CMS employees to assess its quality, appropriateness, and the consistency of the questions. Eight responses were received.
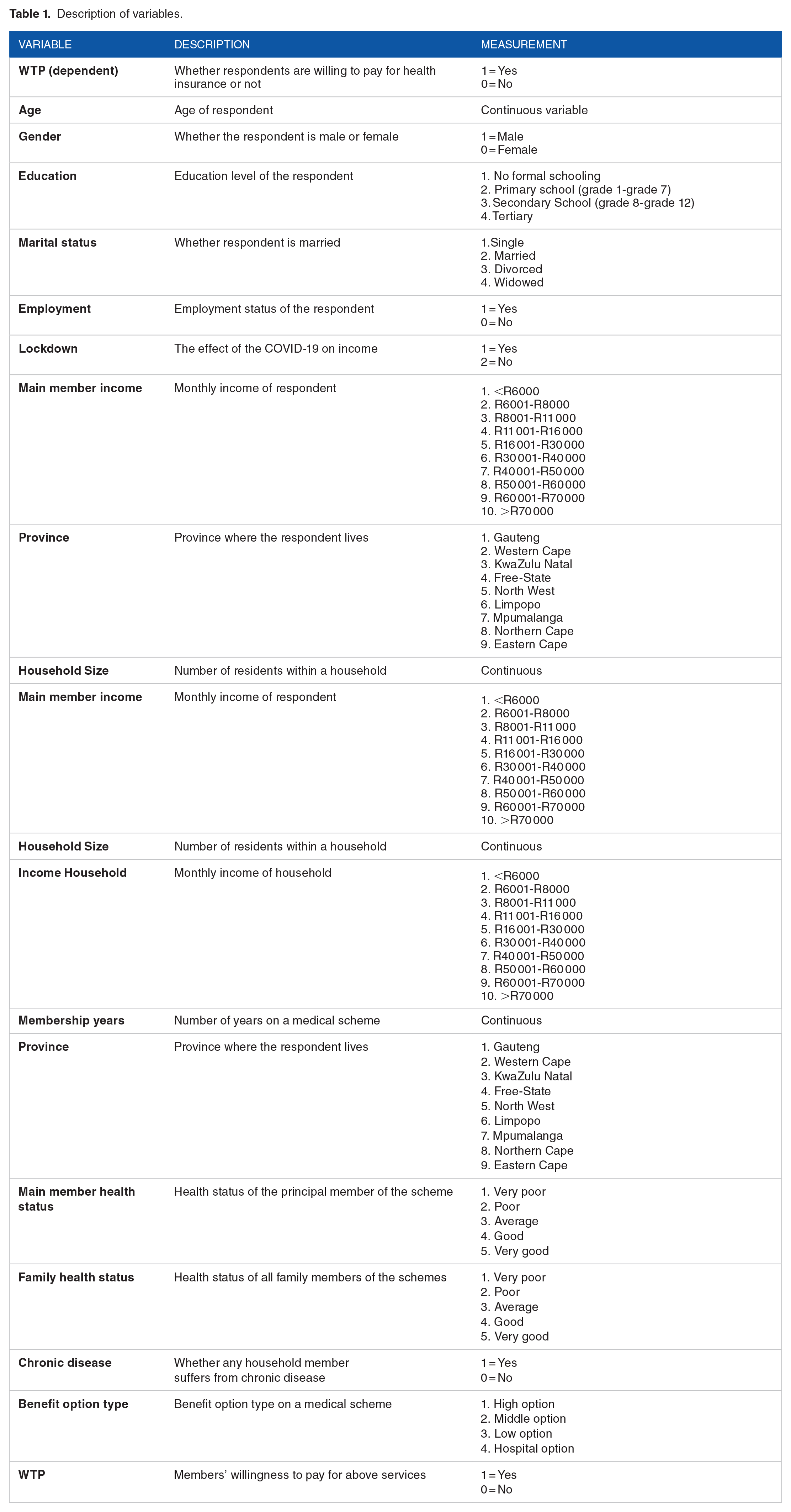
Description of variables
Table 1 is a description of the variables included in the analysis. The main variable of interest was willingness to pay. The variable took on the value of 1 if an individual was willing to pay for the proposed primary health care package and 0 otherwise. The independent variables included socio-demographic characteristics (gender, age, education, marital status, employment status, main member income, household income, medical scheme membership years, province and COVID-19 lockdown effect) and health-related characteristics (main member health status, family health status, chronic illness in family and medical scheme benefit option type).The variables were included based on their influence on WTP in previous studies.9,12-17
Description of variables.
The WTP question started with a statement that defined the current PMBs and the limitations of the PMBs (see Figure 1). Respondents were asked to imagine a scenario where the benefits could be increased to include a list of PHC services. Respondents were then asked whether they were willing to pay a monthly premium for the services. Respondents who were not willing to pay were asked to give reasons for not willing to pay for the additional services.

Scenario for eliciting WTP for PHC services.
Analysis Strategy
Responses from participants were captured in Excel and exported to Stata 13.0 (Stata Corp, College Station, Texas) for further cleaning and analysis. Given the large response rate as compared to the estimated sample, a listwise deletion approach was used to deal with missing data. 18 To assess how representative the study sample was to the population and to assess bias due to our sampling approach, we compared our realized sample and the medical schemes population by age, gender, and province. Descriptive characteristics of the surveyed populations was established using frequencies and percentages. The exploration of whether a person is willingness to pay for a PHC package was estimated using logistic regression because of its ability to deal with a dichotomous dependent variable and its well-established theoretical background.
Results
Socio-demographic characteristics
A total of 8155 responses were received from members of medical schemes. Of these responses, 1643 were excluded due to respondents not being a principal member or not responding to questions. The results of the socio-demographic characteristics are shown in Table 2. In total 6512 participants responses were included in the study. More than half of the participants were female (52.06%). Most of the participants (40.49%) were between the age of 41 and 60. An estimated 66.95 % of the participants had a tertiary qualification while 55.84% of the participants were married. Most (64.70%) of the participants were employed on a full-time basis while 9.99% were unemployed and 13.82% were on retirement.
Socio-demographic characteristics of participants.

R: South African Rand (1 USD = R16.5 in 2020).
A quarter of the participants’ income ranged between R16 001 and R30 000. Only 2.52% of the members had an income ranging between R60 001 and R70 000. Similar to main member’s income, 23.45% of the households had an income of between R16 001 and R30 000. Approximately, 56.76% of the participants had a household size of more than 3. Thirty-two percent of the respondents reported that they have been a member of a medical scheme for over 60 years while 16% of participants’ membership ranged between 40 and 50 years. Most of the participants were from Gauteng (45.01%), KwaZulu-Natal (16.93%) and the Western Cape (22.13%). Figures 2 and 3 show the percentage of study participants by age and province relative to the medical scheme population.

Percentage of study participants by province versus medical scheme population.

Percentage of study participants by age versus medical scheme population.
Health-related characteristics
Table 3 shows the health-related characteristics of the study participants. Most of the respondents were in good (45.32%) or very good (21.25%) health. A small percentage reported poor (4.55%) and very poor health (0.81%). Family health status was reported as good by 47.94% of the respondents. Very poor family health status was reported by 0.80% of respondents. Most of the respondents (63.88%) reported the presence of a chronic illness in the family. Most of the respondents (38.65%) were on a medium benefit option while 22.71% had a hospital benefit option. Thirty-five percent of the respondents were willing to pay for the primary package.
Health-related characteristics.

Factors associated with willingness to pay
The results of the factors associated with willingness to pay are presented in Table 4. Members in age group 31 to 40, 41 to 40, and above 60 were less likely to be willing to pay for the PHC as compared to members between 20 and 30. Education and marital status had no significant association with WTP. Individuals employed full-time (1.49), part-time (1.66) and self-employed (1.74) were more willing to pay for the primary health care package as compared to unemployed individuals. In the bivariate regression, main member income above R30 000 was significantly associated with WTP for the PHC. In the multiple regression however, all income groups were less likely to be willing to pay for the primary package. Respondents whose income was affected by the corona virus disease (COVID-19) lockdown restrictions were also less likely (0.87) to be willing to pay for the PHC package.
Factors associated with willingness to pay.

Abbreviations: R, South African Rand; SE, Standard errors.
P-value: P < .001***, P < .01**, P < .05*.
Respondents with households of >3 were less likely (0.71) to be willing to pay for the PHC package compared to households with <3 members. Respondents with household income above R30 000 were more likely to be willing to pay for the primary health care package compared to household with income of less than R6000.
Reasons for not willing to pay
When asked for reasons why respondents were not willing to pay for the primary health package, 44.88% reasoned that they were already paying enough while 32,39% responded that they were already paying enough and will not have enough money to pay for additional services. Some participants (7.98%) also reasoned that they doubted that paying more will make a difference. The results are shown in Table 5.
Reasons for not willing to pay for primary health care package.

Discussion
The aim of this study was to assess members of medical schemes’ WTP for a PHC package and factors that might influence WTP. Thirty-five percent of study participants were willing to pay for the primary healthcare package. This was lower when compared to what was observed in a willingness to pay for primary health care at public facilities in the Western Cape Province (60%). 10 The difference is however not surprising given that members of medical schemes already pay monthly premiums to access care in the private sector while care in the public sector is financed through taxes.
Our study revealed that respondents who are self-employed, employed on a full-time and part-time basis were willing to pay for the package. To control for the effect of COVID-19 on participants’ WTP for the PHC package, participants were asked whether the lockdown restrictions affected their income. The results showed that participants whose income was affected were less likely to be willing to pay for the package. Having household income of less than R16 000 also reduced respondents’ willing to pay for the proposed PHC package. As income increased however respondents were willing to pay for the PHC package. These results are not surprising as several studies have shown a significant association between income and WTP for health insurance.19-22 Our results were also intuitive as respondents responded that “not having enough money” and “paying enough premiums already” were the reasons for not willing to pay for the PHC. These results are important for policymakers as approximately 30% of the participants reported household income of less than R16 000.
Our analysis also showed that larger households were less likely to be willing to pay for the PHC package compared to smaller households. The results are intuitive as monthly premiums on medical schemes depend on the number of beneficiaries registered on a medical scheme. This observation has been widely argued in literature,23-25 as the heads of larger households would have to pay a larger health insurance premium to cover each member in the household.
Our results also revealed that older individuals and those with high and medium benefits options were less likely to be willing to pay for the PHC package. The results are not surprising as medium and high benefit options turn to have additional services that are not included in the lower options. In addition, monthly premiums on these options is a bit higher than in the lower options.
Factors such as gender, education, membership years, province and health status had no significant influence on the WTP for a PHC package. While other studies have shown that educated individuals are more likely to be willing to pay for health insurance,26,27 our study showed no significant influence. Contrary results have been shown in Nigeria and Bangladesh, suggesting that individuals with higher education are less likely to be willing to pay for health insurance.9,28 Our results on health status also differed to those reported in Vietnam where Nguyen and Hoang have shown that having a chronic disease negatively influenced WTP for social health insurance. 16 Our results are however not surprising given that the current PMB package already covers existing chronic illnesses and hospital care.
The results of our study are important as they come at a time when South Africa is preparing for the implementation of the National Health Insurance (NHI). The NHI is a financing mechanism that seeks to realize universal health coverage (UHC) for all South Africans. It is envisaged that primary health care will be the “heartbeat” of the NHI. 29 The lack of PHC in medical schemes and members’ unwillingness to pay for PHC highlights the need for alternative financing mechanisms as PHC forms the foundation of a sustainable health system. 30 Given the large enough sample and the representativity by gender, age and province, these results can be generalized to the rest of the medical scheme population.
Strengths and limitations
The main strength of this study is that it is the first study to assess members of medical schemes’ willingness to pay for a PHC package in the private sector in South Africa. The demographic profile of our study sample closely matched that of the medical scheme population. The study therefore provides some evidence on members’ (who are already for medical schemes) WTP for a primary health care package.
The main limitation of the study was the use of an online questionnaire limiting the sample to members with access to internet. Selection bias could therefore be a problem. In addition, the use of the online questionnaire did not allow for interaction and visual cues, to probe for more information. Recall bias could have been a problem due to various recall periods of illness and expenditure behaviors. We however assume that the bias in reporting was consistent across respondents. While the questionnaire was pre-tested on CMS staff, the low response rate from the piloted population could also serve as a limitation. The use of a cross-sectional study design could also serve as a limitation because the results capture participants’ opinion at that point in time; not much can be said about changes of views over time or possible differences due to seasonality and time effects.
Conclusion
This study shows that up to 35% of participants may be willing to pay for a primary health care package. Factors influencing willingness to pay included age, marital status, employment status, member’s income, and household income. Most of the participants who were not willing to pay reasoned that they are already paying enough premiums for their current packages and will therefore not have enough money for the proposed PHC package. The results of this study are important for funders and policy makers as they highlight factors that are associated with willingness to pay for primary health care services. The results therefore highlight the need for policy makers and funders to consider socioeconomic factors when developing health care policies.
Supplemental Material
sj-docx-1-his-10.1177_11786329241274479 – Supplemental material for Factors Associated With Willingness to Pay for Primary Health Care Services in South Africa: A Cross-Sectional Survey of Medical Schemes Members
Supplemental material, sj-docx-1-his-10.1177_11786329241274479 for Factors Associated With Willingness to Pay for Primary Health Care Services in South Africa: A Cross-Sectional Survey of Medical Schemes Members by Evelyn Thsehla, Charles Hongoro, Jacqui Miot, Kate Kgasi, Edmore Marinda, Esnath Maramba, Alister Chabi, Barry Childs, Olurotimi Modupe and Olufunke Alaba in Health Services Insights
Supplemental Material
sj-docx-2-his-10.1177_11786329241274479 – Supplemental material for Factors Associated With Willingness to Pay for Primary Health Care Services in South Africa: A Cross-Sectional Survey of Medical Schemes Members
Supplemental material, sj-docx-2-his-10.1177_11786329241274479 for Factors Associated With Willingness to Pay for Primary Health Care Services in South Africa: A Cross-Sectional Survey of Medical Schemes Members by Evelyn Thsehla, Charles Hongoro, Jacqui Miot, Kate Kgasi, Edmore Marinda, Esnath Maramba, Alister Chabi, Barry Childs, Olurotimi Modupe and Olufunke Alaba in Health Services Insights
Footnotes
Acknowledgements
The Authors would like to thank the medical schemes and the members that participated in this study.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Abbreviations
Authors’ Contributions
Ethics Approval and Consent to Participate
This study was carried out in accordance with the Declaration of Helsinki. The study was approved by the CMS as part of the PMB review process. The CMS is a statutory body that collects and disseminate information about private health care in South Africa. Data was accessible through legislation (Medical Schemes Act, No. 131 of 1998, ss7), 5 ethics approval was therefore waived. 31 Written informed consent was obtained from all participants prior to participating in the study. The informed consent highlighted the right not to continue with the study and the anonymity and confidentiality of all collected data. No personal identifiers were collected from participants.
Consent for Publication
N/A.
Availability of Data and Materials
Data used for the study is available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.