
Abstract
Ghana was the first sub-Saharan country to implement a National Health Insurance Scheme (NHIS). In furtherance of the nation’s Universal Health Coverage (UHC) goals, in 2008, Ghana actualized plans for a Free Maternal Healthcare Policy (FMHCP) under the NHIS. The FMHCP was aimed at removing financial barriers to accessing maternal and neonatal health services. This scoping review was conducted to map out the literature on the effects of the FMHCP under the NHIS on the utilization of maternal and infant health care in Ghana. Six databases including CINAHL, PubMed, Sage Journals, Academic Search Premier, Science Direct, and Medline were searched in conducting this review with key terms. A total of 175 studies were retrieved after the search and finally, 23 articles were included in the study after various stages of elimination. The review followed the reporting guidelines stated in the Preferred Reporting Items for Systematic and Meta-analyses Extensions for Scoping Reviews (PRISMA-ScR). The results showed an overall increase in the utilization of antenatal care, facility-based delivery, and postnatal care services. However, certain systemic issues persist regarding access to maternal and infant healthcare. Socio-demographic inequalities such as maternal level of education, place of residence, and economic status likewise barriers such as the existence of out-of-pocket payments, long distance to health facilities, and poor distribution of resources in rural areas hindered the utilization of maternal and infant healthcare. The country faces significant work to eliminate existing barriers and inequalities to ensure that it achieves its UHC goals.
Keywords
Introduction
Ghana and other sub-Saharan African countries continue to make significant efforts to attain universal health coverage. 1 Ensuring equity in the distribution of healthcare services and providing financial protection to healthcare consumers are key attributes of a system that is built to achieve universal health coverage. To this effect, several countries in the sub-region have introduced various health insurance schemes. Even though the characteristics of these health insurance policies differ, the central function of these schemes, as social interventions, is to offer financial safeguards against the expenses of healthcare services for a nation’s inhabitants, thereby aiming to democratize access to healthcare.2,3 Consistent with UHC, the central objective of NHIS is to guarantee that people, regardless of their financial resources, can access necessary healthcare services without enduring economic strain. 2 Even though national health insurance schemes are introduced to reduce the cost associated with healthcare and to increase access to healthcare across a particular set of health insurance, these aims are not always achieved. 4
A crucial element of Ghana’s healthcare system is the free maternal and infant health care policy. The policy was introduced in July 2008 in the face of worsening maternal and infant health outcomes—and, reportedly, at the behest of the British government. 5 Hitherto, in 2003, the country had piloted the exemption of maternal and infant health services from payment of medical fees. 5
Under the initiative, five broad benefits are afforded to perinatal women. First, pregnant women receive free antenatal care which includes medicines and two ultrasounds. 4 Second, pregnant women receive labor services such as normal delivery, assisted delivery, episiotomies, and C-section. 4 Third, postnatal care—services and medicines for two postpartum services—are covered under the initiative for new mothers. 5 Fourth, the initiative provides complimentary services for infants during the first three months of their lives. 5 Lastly, both mother and child benefit from any general benefits under the NHIS. 5
About twenty sub-Saharan African countries have taken some sort of action to roll out a national health insurance policy. A group of countries—Senegal, Burundi, Gabon, Kenya, Mali, Nigeria, Tanzania and Uganda—have functioning national health insurance policies.6–10 Like Ghana, each of these countries provides some form of free maternal healthcare. 3 Free maternal healthcare was important to improve the sub-region’s maternal and infant health outcomes. The near-universal adoption of free maternal healthcare policies by countries in the sub-region shows the premium that governments place on the policy in terms of enhancing their gains in maternal and infant health outcomes. However, limited comprehensive studies are available on the effects of the free maternal health policy on maternal and infant healthcare utilization. 11
In Ghana, a scoping review was conducted to examine the effects of the general national health insurance scheme. 12 But like its sub-Saharan African peers, no wide-ranging study has been conducted in Ghana to determine the implementation and impact of the FMHCP. In other words, empirical evidence does not say whether the expected goals of the free maternal healthcare policy have been attained. Some studies slightly touch on the issue; however, these were standalone studies. Meanwhile, evidence suggests that although the national health insurance has made certain gains, it has an equity problem. 13
Furthermore, the ability to differentiate between program implementation and its outcome in determining the impact of a program like the free maternal healthcare policy is critical. 14 The former assesses how well a health program is delivered, focusing on adherence to the program plan and quality of service delivery while the latter evaluates the impact of the program on target populations, measuring changes in health behaviors and outcomes. 14 Program implementation deploys methods like observations and interviews to measure indicators such as coverage and participant satisfaction. 14 Outcome assessment uses quantitative methods like surveys and statistical analysis to measure indicators such as mortality rates and behavioral changes. 14 With implementation evaluation focusing on process-related aspects and outcome assessment focusing on outcome-related aspects, both stages are vital for evaluating the effectiveness of health programs. 14
Given the centrality of free maternal healthcare policies in Ghana’s national health insurance, a study that examines the effects of the policy on maternal and infant healthcare is sacrosanct. Such a study would benefit similarly situated healthcare systems in sub-Saharan Africa, too. The question, “What are the effects of the free maternal healthcare policy on maternal and infant healthcare utilization in Ghana,” remains largely unanswered. After 15 years of the implementation of the free maternal healthcare policy, this paper provides evidence to this question.
Methods
A scoping review, also known as a systematic scoping review, was conducted to identify the effects of Ghana’s free maternal healthcare policy on maternal and infant healthcare utilization in the country. 15 The study’s aims were consistent with the rationale behind scoping reviews.15,16 At its core, scoping reviews are meant to explore broad, nascent research topics. 16 The nature of the research idea here is broad and emerging. Scoping review, therefore, enabled the researchers to obtain and synthesize wide-ranging literature to present a unified narrative on the effects of the free maternal healthcare policy. The review followed the reporting guidelines stated in the Preferred Reporting Items for Systematic and Meta-analyses Extensions for Scoping Reviews (PRISMA-ScR) by Tricco et al. 18 The review question considered in this study was guided by the Population, Concept, Context (PCC) mnemonic. 15 The population comprises women (pregnant women and mothers) and infants who use maternal and infant care services as well as healthcare workers who render maternal and infant care services. The concept is the free maternal healthcare policy (FMCHP) under the NHIS, and the context is the Ghanaian healthcare system. This culminated in the question, “What are the effects of Ghana’s free maternal healthcare policy under the NHIS on maternal and infant healthcare utilization?”
Informational sources and search strategy
Initially, a restricted search of Medline and PubMed was carried out to pinpoint articles related to the subject. The wording found in the titles and abstracts of pertinent articles, along with the index terms and MeSH terms employed to describe these articles, formed the basis for constructing a comprehensive search plan. Six databases—Science Direct, CINAHL, PubMed, Medline, Sage Journals, and Academic Search Premier—were used for the search. The electronic databases were searched between July and August 2023. Keywords—effects, impact, national health insurance scheme, maternal, infant, healthcare, utilization, and Ghana—were composed into a search string. Advanced searches, limited to the search title and/or abstract to maximize the precision of the search results, were carried out in each of the databases. A full detail of the search strategy and results from each database is presented in Table 1.
Search strategy and results.

(Impact OR influence OR effect OR outcome OR result) AND national health insurance AND Ghana AND (maternal OR infant) AND (implementation OR coverage OR use OR utilization).
Eligibility criteria
This review included articles that met the following criteria: (1) Peer-reviewed empirical studies published in English; (2) studies published between January 2008 to August 2023; and (3) quantitative, qualitative, and mixed method studies on the effects of FMHCP on maternal and infant healthcare utilization. The relevant intervention was the FMHCP under the NHIS. There was no exclusion based on the type of maternal or infant healthcare service received. The primary outcome was the impact of the FMHCP on the degree of utilization and access to services. The secondary outcome of interest was to examine factors that facilitated or hindered the use and access to maternal and infant healthcare services. We excluded the following: (1) studies that were not on Ghana’s free maternal healthcare policy; (2) editorials, reviews, opinions, and commentaries; and (3) papers written in other languages.
Selection and critical appraisal
All the studies retrieved from the literature search, which was conducted independently by the authors, were exported into Mendeley Reference Manager where duplicates were identified and merged. The studies were reviewed by title, and then by abstracts; that is, studies whose titles and abstracts were not consistent with the purpose of this study were eliminated. Three reviewers independently conducted the study selection process, and any disagreements regarding whether to include a study or not were resolved through a mutual agreement among these three (3) reviewers.
Every remaining full-text study after the initial eliminations was critically appraised using the Joanna Briggs Institute’s Critical Appraisal Tools by 3 reviewers. 18 Even though scoping reviews as outlined by Arksey and O’Malley do not typically require a methodological quality assessment of included studies, 17 we appraised each included study for methodological quality, reliability, and applicability. The JBI critical appraisal checklist is an evaluation tool designed to assess a study’s methodological quality and determine its potential for bias in its design and analysis. 18 The JBI critical appraisal checklist consist of 8 to 11 questions depending on the study’s methodology and providers responses like “Yes,” “No,” “Unclear,” and “Not Applicable.” Since the JBI critical appraisal checklist has no predetermined grading point for inclusion, the researchers decided to include studies that have at least 6 to 8 “yes” in the review. The JBI critical appraisal checklist questions used in this study can be found in Supplemental Appendix 1.
Synthesis method
We used a convergent integrated approach method of synthesizing data extracted from both quantitative and qualitative studies simultaneously. 16 This approach is recommended when a review involves both quantitative and qualitative designs, and as our review included both qualitative and quantitative findings, we adopted this method. 16 Quantitative data underwent a process of transformation using a qualitative approach and were then combined with qualitative data using a convergent integrated method. The findings extracted from the data matrix were independently assigned codes by the three researchers. These codes were then compared and deliberated upon to establish agreement between the reviewers. The codes were further refined based on this agreement to arrive at the final set of codes. Similar codes were merged into sub-themes, and related sub-themes were grouped into overarching themes, as detailed in the results section.
Results
Search results and study characteristics
In total, 175 articles were retrieved from the six databases that were imported for screening. After merging duplicates, forty-six articles were left out, of which nine were eliminated based on their titles, and fourteen were eliminated based on abstracts. In the end, twenty-three articles were included in this study. Figure 1 summarizes the screening process. All of the included studies were published between 2013 and 2023. Figure 2 shows the breakdown of studies by the year of publication.
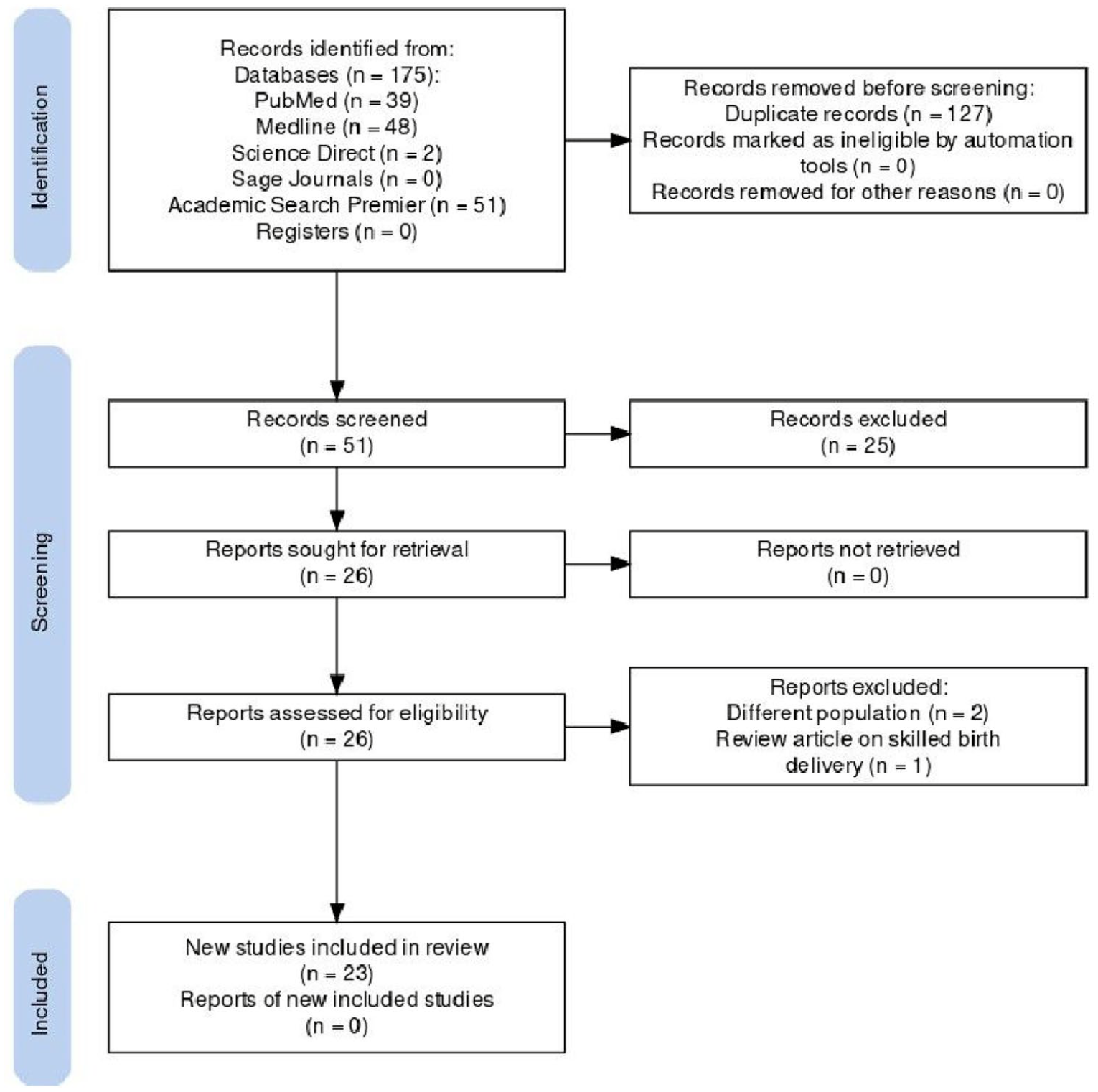
Prisma flow diagram.

Number of publications per year.
Out of the included studies, nineteen were quantitative studies, and four applied mixed methods. Furthermore, eighteen of nineteen quantitative studies were cross-sectional in nature, with many using data from the Ghana Demographic and Health Survey (GDHS) or Ghana Multiple Indicator Cluster Survey. The primary goal of the GDHS was to produce reliable and up-to-date data on family planning, fertility, infant and child mortality, maternal and child health, and nutrition. 19 The Multiple Indicator Cluster Survey was developed by the United Nations Children’s Fund (UNICEF) as an international multi-purpose household survey project to assist countries collect data on a variety of indicators related to women’s and children’s health. 20
Quality appraisal
There were two types of observational studies retrieved: cohort studies (n = 2), and cross-sectional studies (n = 21). The Joanna Briggs Institute assessment checklists were used to assess the methodological quality of each study. 21 All 23 studies were maintained and included in the review after quality appraisal. The results of the appraisal are presented in Table 2, which sought to highlight the strengths and limitations present in both individual studies and a variety of studies.
Methodological assessment using Joanna Briggs institute critical tool.



Data extraction
Relevant findings from the included studies were extracted into a data matrix (Table 3) according to the author(s) and year of publication; the purpose of the study; methodology; sample; and outcome measured, analytical approach, and key findings and recommendations.
Data matrix and charting.

Type of evaluation and analytic approach
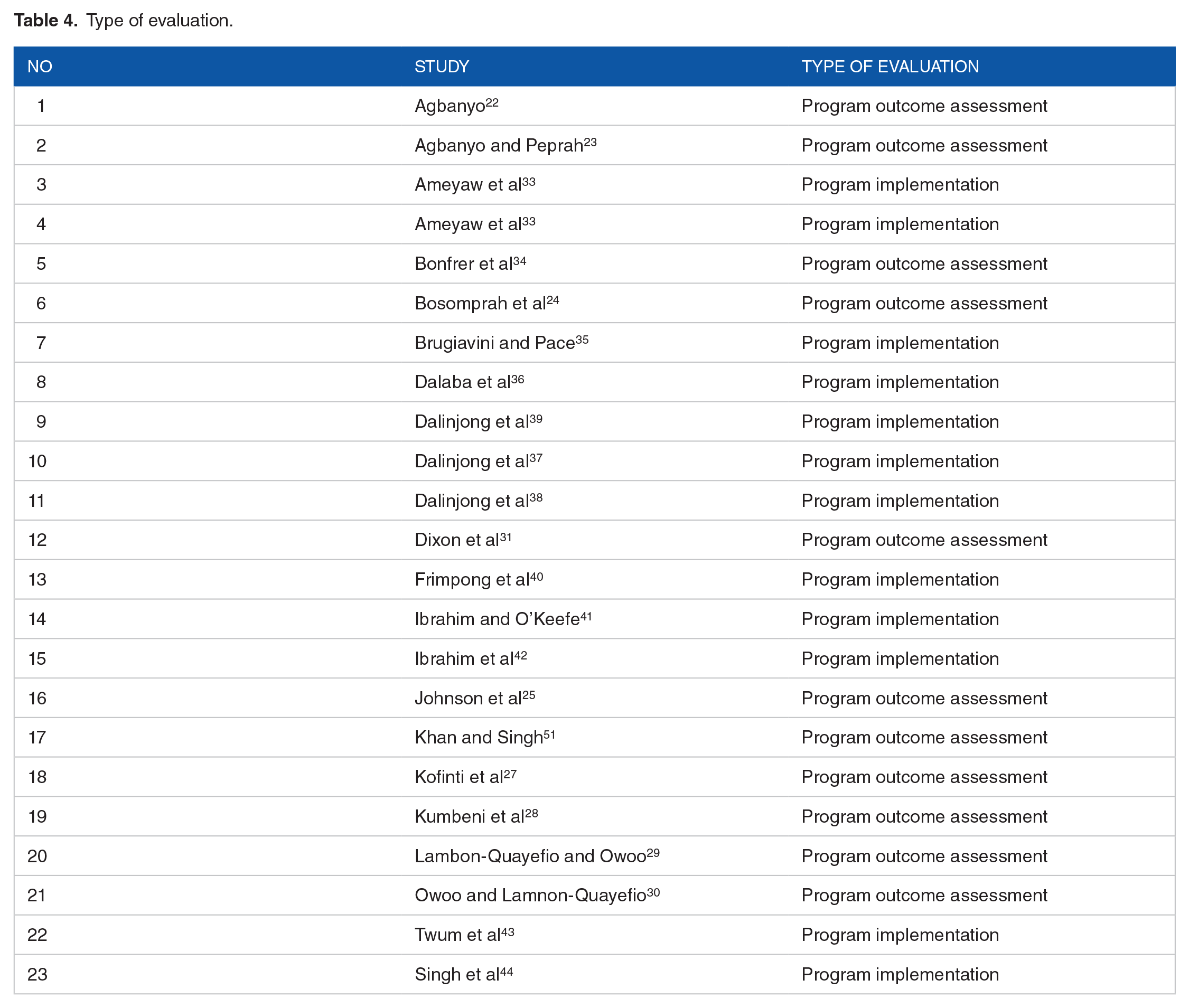
Ten studies focused on evaluation program outcome assessment22–31 and 13 focused on program implementation evaluation.32–44 (Table 4) Amongst the cross-sectional observational studies, 13 out of 1824–26,30–33,36,40,41,43,45,46 studies relied on regression models, 1 35 relied on both instrument variables and propensity matching, 229,34 relied on both propensity matching scores and the remaining 2 relied on instrument variables to evaluate and analyze the impact of the free maternal healthcare policy on their specific outcomes.22,23 For the 4 mixed method studies, 2 relied on descriptive statistics for their quantitative analysis and reported on using both thematic analysis as their qualitative approach.38,37,39 The remaining mixed method study reported descriptive statistics and inductive open coding as their qualitative analytical approach. 44
Type of evaluation.
Narrative synthesis of findings
Overall, all the twenty-three studies satisfied both the primary and secondary aims of this review. The findings of the studies were synthesized under broad themes including healthcare service use which comprised impact on antenatal care use, delivery care, and postnatal care, influence of neonatal mortality, existence of out-of-pocket expenditure, barriers, and inequalities existing in service use. Most studies revealed one or multiple inequalities existing using the policy.22–24,26–35,37,38,40,43,44,45,51 Below are the reported findings.
Impact on antenatal care utilization
Ten studies pointed out increased utilization of maternal health care services, especially in antenatal care services.24,25,27,29–31,33,34,43,44 For example, in the study conducted by Bosomprah et al, 24 it was found that NHIS membership increased ANC attendance (at least 4 visits) of pregnant mothers. Subsequently, 87% of women who attended the required ANC number of visits delivered their babies safely and insured pregnant women were 2 times more likely to make minimum ANC visits than non-insured pregnant women. 24 Conversely, women who were not insured or had no NHIS coverage were less likely to use ANC services and have a trained birth delivery at a health facility rather, most of them preferred home deliveries. 27
Although several studies projected a substantial increase in early ANC utilization, Dixon et al 31 showed that the NHIS did not have a significant impact on the timing of the first ANC visit. Using the 2008 Ghana Demographic Health survey among 1610 women, they found that 57% of Ghanaian women received ANC within the first 3 months, however, there was no significant influence on the timing of the first ANC visit. 31
Impact on delivery care
Nine studies reported that NHIS significantly increased facility-based delivery with skilled birth attendants. Most pregnant women preferred delivery with skilled care over home deliveries since they were enrolled in the national health insurance scheme.22,25,27,29,31,33,34,43,44
A study conducted by Agbanyo in 2020, stated that the free maternal health policy increased NHIS enrollment of women and subsequently increased the chances of these enrolled women having facility-based delivery increased as well. 22 After the inception of the NHIS, a 20.3% increase in using facility-based delivery was recorded relative to home care delivery services among pregnant Ghanaian women. 22 A similar study showed that the likelihood of facility-based delivery among pregnant women increased by 5-fold due to the policy. 43
Furthermore, as facility-based delivery with skilled birth attendants increased, records showed that the number of caesarian sections increased as well during the NHIS era, thereby decreasing maternal and infant mortality.34,41
Impact on postnatal services
NHIS significantly improved the use of family planning services among mothers who had just delivered, and this was demonstrated in a reduction in the rates of mothers having unwanted pregnancies and increased spacing of their children just after having a baby. 34
Influence on neonatal mortality
Neonatal mortality was one of the areas examined concerning free maternal health insurance. Three studies reported the impact of the policy on neonatal mortality.29,41,42 Findings revealed that the NHIS significantly reduced the risk of neonatal deaths.29,42 Prior to the free maternal health policy, mothers who had 3 prior birth experiences were more likely to lose their infants in the NHIS era as compared to when the premium exemption was introduced. 42 The studies on the effects of the free maternal health policy on neonatal mortality were not unanimous, however.
Maternal and infant health-related out-of-pocket expenditure
Five studies evaluated the existence of out-of-pocket (OOP) under the policy.28,35,36,37,39 The majority of women in the Kassena-Nanka municipality in the Northern region of Ghana, in the focus group discussion, concluded that maternal health services were not entirely free under the NHIS as they had to make certain cash expenses. 39 These out-of-pocket expenses included drugs that were either not covered under the scheme or at the time of delivery were out of stock at the health facility, hygiene supplies, and other prescribed items. Women estimated they made an average maternal health-related expense of GHC 33.50 (17 USD) on soaps, towels, and medications not covered under NHIS. 39 Studies found that out-of-pocket expenditures were made especially during birth emergencies, neonatal intensive admissions, and cesarean sections which were not covered entirely by the NHIS.35,37,39
Similarly, out-of-pocket expenses were either direct medical costs or indirect non-medical costs pregnant women had to make during the access to maternal and infant care services. 44 Because of the existence of these out-of-pocket expenses, women, especially in poorer towns, did not receive the appropriate maternal and infant healthcare services because they were not financially capable. 37 When the NHIS managers and providers were interviewed on their opinions on the existence of out-of-pocket expenses, they insisted that NHIS still covered the majority of maternal and child healthcare-related costs. They recognized that some families had to make out-of-pocket expenses which were occasioned by late reimbursements of funds to health facilities. 37 As high as 71% and as low as 19% of pregnant women made out-of-pocket maternal health-related expenses.28,36
Inequalities in the use of maternal and infant healthcare services
Nine of the studies established socio-demographic disparity affecting the utilization of maternal healthcare services despite the free maternal health policy of the NHIS.22,25,26,27,29,31,32,35,44 Low level of education inhibited NHIS enrollment among women and use of ANC services as well as skilled attendance at birth are among the inequalities-identified.22,26,27,29,31,33,41,42,45 The less educated pregnant women were, the less likely they were to benefit from the free maternal health policy.22,26,32,35,44 Likewise, it was clear that the rich remained more likely to use maternal health services and the NHIS than the poor.25,26,32,35,44
Rural-insured pregnant women had higher chances of having home delivery, a low rate of skilled birth attendance, and made a lesser number of ANC visits before delivery. 31 Insured urban women were more likely to use facility-based delivery during their time of delivery.26,27,35 It was reported that on perinatal mortality rates, urban-insured women had the higher number of neonatal deaths since the inception of the free maternal health policy under NHIS. 29
Barriers to the use of maternal and infant health care services
Nine studies pointed out barriers pregnant women and mothers face in the utilization of maternal healthcare services.22,23,26,33,35,37,40,43,44 According to Agbanyo, 22 Brugiavini and Pace, 35 and Khan and Singh, 51 high birth order was identified as a factor in reducing the use of ANC service and skilled birth delivery at a health facility by women who were enrolled on NHIS.22,26,35 Women who had more than one child were less likely to have a valid NHIS status by 5.2%, 13.6%, and 11.7% for their second, third, and fourth pregnancies respectively thus decreasing their use of maternal and infant health care services. 22
Long distances to NHIS registration centers by pregnant women who did not have a valid NHIS status the first time they sought ANC deterred them from enrolling and seeking maternal health care. 22 Similarly, long distances to referral hospitals reduced the use of maternal health services by insured women.29,37,44 Public clinics, which are primarily available in most rural communities, were inadequately resourced and had low service capacity thus even though most women from those communities were insured they were unable to have the necessary facilities or services (diagnostic testing and surgical theaters) to improve or increase maternal health care utilization despite the NHIS.23,37
Discussion
This study sought to map out the literature on the effects of Ghana’s National Health Insurance Scheme on maternal and infant healthcare utilization. This study made findings on the key components of universal health coverage: equity in access, financial protection, and quality of care.
Regarding equitable access to maternal and infant healthcare services, the findings showed mixed results regarding equitable access. Increase in access to maternal and infant healthcare services was observed in this study.22,23,25,29,32,33,35,36,43,45 Likewise, an upshot in the usage of postnatal services was observed. 36 The positive effects of the policy in increasing access to maternal and infant health services are supported by literature. 47 Free health insurance policies tend to increase access to health care, mainly because they address affordability concerns. This is particularly true in low- and middle-income countries like Ghana where financial barriers often undermine access to healthcare.12,47 The framers of universal health coverage recognized this fact by encouraging health policymakers to subsidize healthcare, either partially or fully.48–50 Ghana’s free maternal policy, as evidenced in this study, suggests that subsidization of health insurance is a credible way to boost access to healthcare.
The gains made in terms of increased access to maternal and infant health services were not absolute, however. This study showed that the policy has equitable access challenges. Even though about 20% increase was observed in facility-based delivery after the program was rolled out, pregnant women who were not enrolled in the National Health Insurance Scheme at the time of their pregnancies were likely to use ANC services, and consequently, have facility-based delivery. 26 According to the framework of the policy, pregnant women are automatically enrolled. 26 However, a pregnant woman must have been a registered member of the National Health Insurance Scheme before enjoying this automatic enrollment. 26 Women who were not members at the time of their pregnancy could register for free, but it appears that women who were not registered before they got pregnant were reluctant to register after getting pregnant. 29 This inertia on the part of the unregistered, newly pregnant women could explain the disparity in facility-based delivery among those who were enrolled in the National Health Insurance Scheme before becoming pregnant and those who were not enrolled when they became pregnant. The level of education of the women could also account for this disparity. The level of education of women affected the program as women with lower levels of education were less likely to access healthcare under the policy.22,30,43,51
There was also an urban-rural disparity in access to healthcare under the policy, with rural women disproportionately affected.26,30 The lopsided nature of the policy is an indictment of the policy which was heralded as pro-poor. The uneven geographical distribution of access to care under the program could be attributed to the underlying systemic challenges facing the entire healthcare infrastructure in the country. The country’s healthcare system is urban-centric; urban areas have more health facilities and more health human resources than rural area.52–54 So, even though the policy is open to all women regardless of their location, women in rural areas are deprived, to a substantial degree, of the opportunity to visit well-equipped health facilities. This finding underscores the complex context of health policies. 14 Health policies do not operate in isolation. 14 They must be linked to the overall healthcare system and socioeconomic aspects of the settings in which they exist. 14 The mere provision of free maternal and child healthcare policies does not, in itself, cure underlying issues with the distribution of healthcare infrastructure and personnel in the country.
Just like equitable access, the policy has not yet fully achieved its goal of ensuring financial protection thus far.34,38,55 As high as seven out of every ten pregnant women made some form of out-of-pocket expenses.34,38 These expenses were mainly in 2 categories. The first involved services that were not covered under the policy.30,37,56 The second pertained to costs related to cash expenses made by pregnant women and their families in the form of auxiliary items such as purchasing soaps and towels. 55 These out-of-pocket expenses made by pregnant women were not only found in the context of Ghana’s insurance scheme, but it was present in sub-Saharan countries like Kenya.57,58 The resultant effect of the prevailing out-of-pocket expenses is harshly felt by poorer people in society. 37 Protection from the risk of financial hardship is central to universal health coverage.59,60
Costs related to medical emergencies are the typical type of catastrophic health expenditure that universal health coverage seeks to avoid. 60 This has not been the case for the policy. Various factors may account for this. One such factor is the lack of clarity of the policy. Some providers were of the view that the policy covers medical emergencies while consumers held the opposite view. 37 An earlier study had established that the health insurance scheme, as a whole, has fundamental challenges in clarity and this study shows that lack of precision affects the free maternal and infant health policy too. 12
Also, late reimbursement of healthcare providers has compelled some providers to charge out-of-pocket fees that were not envisaged under the FMHCP. Likewise, the NHIS is bedeviled by fiscal challenges that threaten the sustainability of the program. 61 The irony of it all is that the sustainability problems facing the scheme are partly due to large exemptions such as the free maternal and infant policy. 61 This presents a conundrum for policymakers: the benefit that they seek to bestow contributes to the sustainability challenges of the program which grants the same benefit. Low renewal rates by members of the scheme also stagnate financial inflow which is passed to subscribers such as perinatal women. 2
Neonatal death was higher among urban-insured women than uninsured urban women and rural-insured women. This finding may appear counterintuitive because people in urban areas are more likely to access health facilities. 29 However, this finding brings quality of care, which may explain the finding, into focus. 29 The higher population in urban areas likely increases demand for perinatal healthcare services in such areas. Higher demand naturally puts pressure on healthcare professionals and facilities and this pressure could compromise the quality of care that women receive, thus, leading to neonatal deaths.29,62 In other words, free maternal health policies are incomplete unless interventions that ensure quality of care are integral to the health insurance programs.
Poor protection against financial risk, combined with inequalities in access to healthcare, can have a negative impact on the quality of care provided under the policy. Quality of care is another cornerstone of universal healthcare. In this study, some women indicated that they prefer home delivery. 26 Even though this finding was not directly linked to the quality of care of the services under the program, evidence from elsewhere shows concerning trends in the quality of care under the NHIS. Researchers have established that long waiting time and poor attitudes of healthcare personnel toward clients undermines the quality of care under the scheme.63,64
The increase in antenatal care service and facility-based delivery was 1 significant policy achievement. This finding is consistent with the impact of various kinds of health insurance schemes that operate similar free maternal healthcare policies .57,65,66 For instance, the introduction of the National Fund for Health Insurance and Social Guarantee of Gabon (NFHISG) in 2008 saw a two-third increase in the utilization of ANC, facility-based delivery, and postnatal visits among women of reproductive age. 66 In Kenya, the “Linda Mama” is an initiative under the National Hospital Insurance Fund (NHIF) that enables all pregnant women in Kenya to be eligible for free maternal health services after registration. 58 The NHIF reported a 29.5% increase in the utilization of maternal and infant health care 2 years after its implementation in 2013 under a presidential directive. 57
This current review found that the NHIS caused a significant reduction in neonatal mortality. Once the free maternal healthcare policy increased access to maternal healthcare utilization, it was expected that there would be a reduction in neonatal mortality as well established that most of the risk factors associated with neonatal death are preventable during ANC visits. Therefore, as women went for the ANC, the medical team would have helped them promote their health, thus decreasing the risk of neonatal deaths.
Strengths and limitations
This study’s strength lies in its comprehensive approach and the first review aimed to extensively map out the literature on the effects of Ghana’s FMHCP on maternal and infant health care utilization. Some limitations have been identified during the conduct of this review. Since database searches were the primary method used to find studies, studies that were not published or just accessible online could not have been included, and those studies could not further undergo quality appraisal since that was outside the scope of study inclusion.
Conclusion and Recommendations
This scoping review provides evidence that Ghana’s free maternal and healthcare policy has impacted and improved the utilization of maternal healthcare services including antenatal services, facility-based delivery, and family planning services. However, these improvements cannot be taken for granted as some systemic barriers and inequalities can undercut the objectives of the policy. Ghana, and similarly situated African countries, should take measures to remove the bottlenecks that impede the realization of the full benefits of a policy like free maternal and child healthcare. The government of Ghana must see to it that it achieves its primary goal of ensuring that the poor and vulnerable in society are protected against difficulties in accessing healthcare. Furthermore, out-of-pocket payment must be curtailed by catering for auxiliary costs associated with seeking maternal and infant healthcare. Also, stakeholders should roll out comprehensive information campaigns, which would create awareness of the NHIS and its free maternal health policy.
Supplemental Material
sj-docx-1-his-10.1177_11786329241274481 – Supplemental material for The Effects of Ghana’s Free Maternal and Healthcare Policy on Maternal and Infant Healthcare: A Scoping Review
Supplemental material, sj-docx-1-his-10.1177_11786329241274481 for The Effects of Ghana’s Free Maternal and Healthcare Policy on Maternal and Infant Healthcare: A Scoping Review by Emefa Awo Adawudu, Kizito Aidam, Elisha Oduro, Dennis Miezah and Allison Vorderstrasse in Health Services Insights
Footnotes
Acknowledgements
We would like to acknowledge Dr. Favorite Iradukunda for providing guidance and proofreading this review.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
EAA created the research question, conducted search, analyzed the data, and wrote the manuscript. KA conducted articles search and contributed to manuscript writing. EO created the research question, analyzed the data, and contributed to manuscript editing. DM analyzed the articles and contributed to manuscript editing. AV contributed to writing and reviewing the manuscript.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.