
Abstract
Background:
Research on the quality scale of the healthcare supply chain is still limited. This study aimed to assess the information quality of the supply chain model with a focus on construct validity. Studies related to information quality measurement generally focus on measuring the dimensions of the completeness of medical records and consumer perspectives. We intended to assess the scale based on doctors needed as care coordinators on type 2 diabetes mellitus or the Non-Insulin-Dependent-Diabetes-Mellitus (NIDDM) program in primary healthcare.
Methods:
Sixty-four primary healthcare doctors with an age range of 24–51 years were involved in this research. The scale obtained was formed from the assessment of the point of view of a panel of experts through the content validity index (CVI). The exploratory factor analysis (EFA) method was used to explore the scale of information quality in the information supply chain model for the NIDDM chronic disease management program.
Result:
The data analysis results indicated three main factors that affected the quality of the information supply chain model of NIDDM, namely accessibility, safety, and efficiency of information related to NIDDM. The results of the validity and reliability of the data showed that the scale used in this research was valid and reliable with a Cronbach alpha coefficient of 0.861.
Conclusion:
The scale developed in this research could be used to explore the quality of the information supply chain of NIDDM management in primary healthcare. Each item on the scale could explain the variables according to their respective groups.
Introduction
Non-insulin-dependent-diabetes-mellitus (NIDDM) is a chronic disease with high treatment costs because it will last a lifetime for a person diagnosed with type 2 diabetes. Patients with NIDDM require continuing medical care with direct and indirect costs. Diabetes also has the potential to pose a risk of early complications if not treated properly. Diabetes and its associated complications impose a significant economic burden on the health care system and society, given the large expenditures spent on managing these complications. Preventative measures are needed to improve patients’ glycemic control, thereby preventing diabetes complications, which could potentially reduce the health and economic burden on the public health care system.1–3 Based on International Diabetes Federation (IDF) data for 2021, Indonesia is globally ranked fifth with 19.5 million adults aged 20–79 years living with diabetes. Referring to the IDF data, the number of people with Diabetes Mellitus in Indonesia is projected to increase to 28.6 million in 2045. 4
The increasing prevalence of NIDDM in various countries in the world should be anticipated with preventive and promotive actions by policy makers. 5 NIDDM is a non-communicable disease that has become a priority for primary health care policies. Primary health services are considered as basic health services in the community with preventive, promotive and limited curative efforts.6–8 Doctors in primary health care facilities have an important role as care coordinators. 6 A clinical information system is highly required to support the performance of doctors in the NIDDM chronic disease management program. 9 In the management of chronic diseases such as NIDDM, patients will require health services related to diabetes management throughout their life, so that a good supply of information is highly needed. The information supporting clinical decision making by doctors must be presented in a sequential and continuous manner.5,10,11 The NIDDM management program strategy of primary healthcare in Indonesia is supported by the national health insurance, specifically the Social Security Administrator for Health (known as BPJS Kesehatan in Indonesia) through chronic disease management programs to anticipate the economic burden and risk of complications that can arise from patients with NIDDM.12,13
There has been policy research on implementing NIDDM chronic disease management program strategies in primary healthcare and improving service quality with the support of information systems for good data presentation. The study on the application of digitization in the existing health service supply chain has mostly focused on the supply of medical devices, blood, and medicine.14–17 Study on the supply of medical data has not been widely conducted, and there has been no research that has developed a standard scale for measuring the success of strategies to improve the quality of information through the data supply chain in supporting the performance of doctors as care coordinators for the NIDDM management program. This study was conducted to develop a scale for measuring the quality of information supply chain of NIDDM management programs in government-owned primary services.
Methods
This research utilized an exploratory mixed-methods (qualitative-quantitative) study design to develop an information quality measurement tool for the supply chain management of health information on the management of the chronic disease NIDDM. In the first stage, a questionnaire with a qualitative approach had been produced, namely through the stages of construct definition, domain content, and assessment items. In the next stage, an evaluation of the reliability and validity of the scale was conducted with a quantitative approach. Scale development requires additional time and research, since many procedures have to be used to refine the scale with various problems related to finally acquiring the final form of the scale.18,19 This manuscript is focused in detail on the discussion of the reliability evaluation stage by testing the initial factor structure that had been formed with its items through exploratory factor analysis (EFA). The EFA method in this research was used to reduce the dimensions of the observed factor variables, and were represented in an easy-to-understand form. The processed data had been analyzed by an expert panel consisting of eight experts: Three lay experts and five content experts covering three main factors that can explain the quality of information in the supply chain management of health information on the management of the chronic disease NIDDM. The ideal number of expert panels is a minimum of 5 people and a maximum of 10 people to obtain sufficient control of the deal opportunities.20–22 The results from the expert panel’s viewpoint judgment were assessed through the content validity index (CVI), from three latent factors (construct), where each factor has 5 items, which was reduced to 3 items each. Based on the CVI score criteria, the item ≤0.80 should be eliminated. 22
The results of the CVI, including factors and items, were then tested for construct validity using the EFA method19,23 which was conducted by recruiting 64 subjects in this research who work as doctors in the management of the NIDDM chronic disease from 50 government-owned primary healthcare facilities in a regency area in Indonesia with an age range of 24–51 years. The number of subjects in this research was in accordance with the standard number recommended by several literatures, where the minimum sample size in a validation research should be 5–10 times the number of instrument variables or the ratio of participants per variable or item (n:p) is 5:1.24,25 This research consisted of nine items, and the minimum number according to this statement must amount to 45 subjects. This research involved 64 subjects, so it had met the standard number of subjects in the validation research. EFA statistical analysis was conducted with SPSS 22 software (IBM Corp., Armonk NY). This research had obtained an ethical clearance from the Medical and health research ethics Committee (MHREC) of Universitas Gadjah Mada (number: KE/FK/0042/EC/202).
Results
All 64 subjects who participated in this research had an average age of 36.5 years, and were doctors in charge of managing NIDDM chronic disease in government-owned primary healthcare facilities. Table 1 shows the details of the basic characteristics of the participants.
Characteristics of participants.

The Kaiser-Meyer-Olkin Measure of Sampling Adequacy (KMO-MSA) test and Bartlett’s Test are tests to assess the feasibility of the question item variables for factor analysis. The results of the feasibility test of the question item variables in this research are presented in Table 2. The KMO-MSA results showed a value of 0.779 > 0.5, which means that the sample in this test was adequate for factor analysis. The significance of the value of Bartlett’s test must be ≤0.05 for the factor analysis to be acceptable. The results above showed a value of <0.000, which means that factor analysis could be conducted in this research.
Results of the KMO and Bartlett’s test.
Table 3 shows how much the formed factors can explain the variation of the data, and it can be concluded that the three factors could explain 68.69% of the total variance.
Total variance explained.

The results of the extraction value should be >0.5, so that the question items could explain the factors. Based on the output in Table 4, it can be concluded that the nine items were able to explain the factors. The best correlation was found in the following factors:
The first factor contains question items number 1, 2, and 3;
The second factor contains question items number 4, 5, and 6; and
The third factor contains question items number 7, 8, and 9.
Rotated factor matrix.

These were grouped based on the correlation value of the largest variable contained to a certain factor. These three factors indicated a value above 0.5, which means that they were feasible to summarize the nine question items. Based on the screen plot graph in Figure 1, the nine question items were observed to form three factors or dimensions (eigenvalue >1).

The scree plot graph shows the formation of the three constructs/factors in the instrument.
Reliability
Internal consistency was applied to assess the reliability of the questionnaire. Table 5 shows the cronbach’s alpha coefficient of 0.861 above the threshold >0.6 is an acceptable level of reliability, so it can be concluded that the questionnaire formed was reliable.
Cronbach’s alpha.

Discussion
Exploratory factor analysis (EFA) was used to assess the construct validity of the scale. The scale tested for construct validity was a scale that had been declared valid based on the results of the CVI test. The scale in the form of a questionnaire consisted of three main factors, namely accessibility, safety, and efficiency, and was composed of nine question items. This scale was intended to measure the quality of information from the health information supply chain role model on the management of the NIDDM chronic disease in primary healthcare in supporting the performance of doctors. Details of the measuring scale are presented in Table 6.
Scale for measuring the quality of information from the Information Supply Chain of NIDDM.
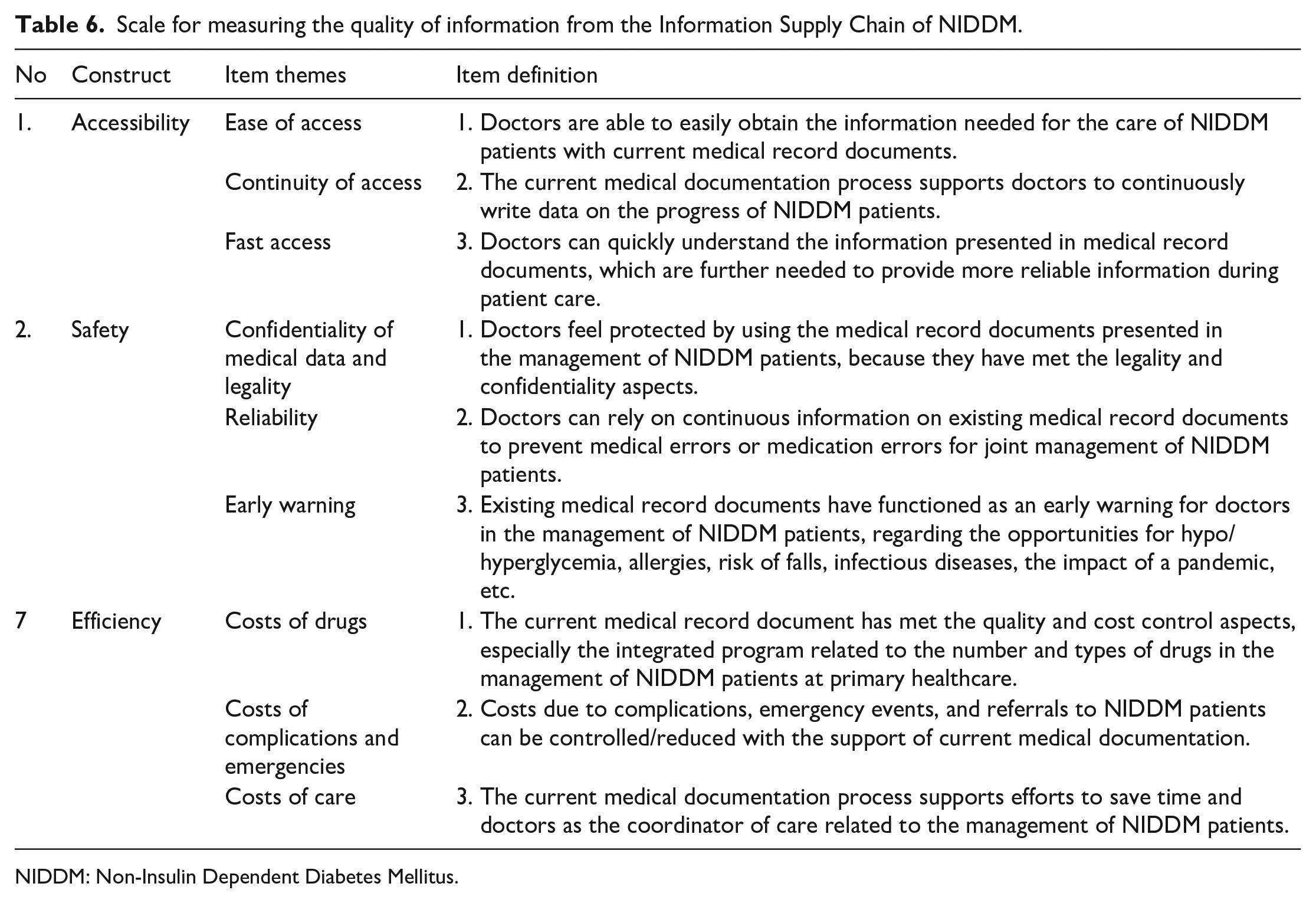
NIDDM: Non-Insulin Dependent Diabetes Mellitus.
Factor 1 in the form of an accessibility construct consisted of three question items that were developed according to the needs of doctors in supporting performance, namely ease of access, continuity of access, and fast access. According to Wixom and Todd in 2005, the perceived use value of information is strongly influenced by information satisfaction. Accessibility is one of the most important items of a quality system. Accessibility is described as the ease of accessing or extracting information from the system.26,27 As stated by Eppler in 2006, accessibility is defined as a continuous and unobstructed way to obtain information.26,28 Referring to the combined definition of Eppler in 2006 and Wixom and Todd in 2005, accessibility can be perceived as information that must be accessed continuously without many obstacles, which means that it can be related to fast access criteria. Supply chain management provides a significant impact on better access to health services.29,30 This is certainly very useful in supporting the performance of doctors in NIDDM chronic disease services, where patients with NIDDM need access to health services for the management of their disease throughout their life.
Factor 2 is a safety construct consisting of three theme items, namely confidentiality of medical data and legality, reliability and early warning. The safety factor was chosen in this research, because it was found to be correlated with the quality of information from information systems on health services, specifically on the management of chronic diseases that require continuous data.31,32 Management of chronic diseases with high costs and prone to emergency complications, such as NIDDM, requires continuous medical data support to assist doctors in performing quality services. Previous research had suggested that supply chain management provided significant benefits for improving patient safety.17,30,33 Confidentiality of medical data and legality play an important role in ensuring the safety of doctors in carrying out their performance as coordinators of health services.34,35 Researchers see this opportunity, especially in the chronic disease prevention program at the primary healthcare. The program runs in collaboration between health workers from the main health center to a network in the form of Integrated Health Post for Non-Communicable Diseases (POSBINDU-PTM) with a family approach to increase the reach of community targets. Documentation is a method of communication with members of the care team, using medical records as an effective method to support communication, collaboration, and coordination of care.35,36
Factor 3 is an efficiency construct consisting of three theme items, namely costs of drug, care, and complications and emergencies. Research conducted by Joep Top in 2015 found a correlation between cost and increased information. 26 In this research, authors intended to identify the efficiency construct based on health services, especially in the management of NIDDM chronic disease, namely drug costs, and complications and emergencies costs, as well as costs of care, which include the time and energy that must be spent by doctors in providing health services. Supply chain management had an important impact on reducing costs and improving performance in healthcare organizations.15,17,30 The authors found that the chronic disease management program at the primary healthcare does not only involve doctors as care coordinators, but also other health workers both at the primary healthcare and their network service units. The supply chain management is realizing its goals and collaborating among supply chain suppliers to achieve system efficiency. Supply chain coordination and cooperation are operating with connections throughout the chain with materials and information flowing smoothly throughout supply chain operations in achieving efficiency.37,38
The results of the study indicate that the compiled scale has acceptable validity and reliability. Each item on the scale can be explained according to its respective group of variables. The results of the research showed that the compiled scale had acceptable validity and reliability. Each item on the scale could explain the variables according to their respective groups.
This study has practical implications for providing guidelines for stakeholders to evaluate the quality of information from the supply chain model in the NIDDM chronic disease. The information supply chain model can help to improve the performance of doctors as a care coordinator in primary healthcare. This study has several limitations since it is only focused on primary healthcare, and the results may not be suitable for implementation in larger hospitals with complex business processes.
Footnotes
Acknowledgements
The authors are grateful to Lembaga Pengelola Dana Pendidikan (LPDP) Indonesia for the provision of assistance to conduct this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Lembaga Pengelola Dana Pendidikan (LPDP) Indonesia.