
Abstract
Background:
Literature has reported differences in the epidemiology or natural history of non-communicable diseases among both the male and female sexes. Stratification of multimorbidity burden based on sex is crucial to identify and implement targeted prevention and control interventions for chronic diseases.
Objectives:
To determine the burden of hypertension, type-2 diabetes mellitus, and obesity; and to compare the related multimorbidity among male and female patients.
Methods:
The study was a retrospective analysis of 375 802 medical records from primary care centers. Data was extracted from March 2022 to March 2023. A multivariate probit estimation methodology was employed using a 3-equations multivariate multiple probit model to jointly estimate the association of a person’s sex with the diagnosis of the 3 chronic conditions: obesity, diabetes, and hypertension. A multinomial logistic regression analysis was conducted to allow each unique combination of these 3 chronic diseases.
Results:
Females had a relatively higher proportion of obesity (58.1% vs 41.2%), obesity and diabetes only (58.9% vs 41.1%), obesity and hypertension (63.6% vs 36.4%), and joint diagnosis with 3 conditions (65.7% vs 34.3%). Females’ participants consistently had a significantly higher likelihood of diagnosis compared with males except for diabetes (OR = 0.59, 95% CI: 0.56-0.62) and the combination of only diabetes and hypertension (OR = 0.67, 95% CI: 0.61-0.74). The likelihood of other combinations ranged from 1.04 (95% CI: 0.98-1.10) for only hypertension to 2.30 (95% CI: 2.10-2.53) for the joint diagnosis of all 3 conditions. An increased likelihood of a single or combined occurrence of 3 chronic conditions was observed with increased age.
Conclusion:
The multimorbidity distribution for diabetes mellitus, hypertension, and obesity differs significantly among male and female patients. The overall burden of morbidity, and mortality, however, tends to rise after 46 years of age, with the highest burden among individuals above 60 years of age.
Introduction
Globally, there is growing evidence regarding differences in risk, age at the onset of disease, and treatment outcomes among the male and female sexes, particularly for non-communicable diseases. 1 Males are considered an independent risk factor for hypertension, while relatively early onset and higher risk of type-2 diabetes mellitus have been reported among men when compared to women.1 -3 However, obesity, which is an established risk factor for many noncommunicable diseases is relatively more common among women as compared to men in all age groups. 1
Literature has described the various factors related to the observed differences in the epidemiology or natural history of communicable diseases among males and females (ie, differences in physiology and differences in psychosocial environment). The differences in physiology can be explained by the sex-specific gene expression of autosomes, and sex hormones. These differences not only determine the fat mobilization and distribution in the body but also affect insulin resistance, visceral obesity, as well as the risk of metabolic syndrome. Furthermore, sex hormones affect social behaviors, and psychological tendencies, such as males being more prone to be involved in potentially detrimental behaviors, such as alcohol use, drug abuse, smoking, and exposure to external built and natural environments, and psychological burdens or stress to place upon their families.3,4 In addition, hormones play a major role in facilitating the response to external stimuli. 5
Comparatively, females’ natural exposure to different kinds of stresses mainly relates to the lack of empowerment in society, low social status, and domestic responsibilities related to the household, which makes them prone to develop non-communicable diseases, such as hypertension and type-2 diabetes mellitus.3,6 The literature identified androgen deficiency as a major risk factor for increased visceral obesity, which results in adipocyte and endothelial dysfunction as a major cause of hypertension among men and postmenopausal women. 7 In addition, the differences in blood pressure readings, the nocturnal and diurnal variation in blood pressure, glycemic control, and treatment outcomes for hypertension, have been reported among both hypertensive men and women.7,8 Similarly, previously conducted studies reported that lower levels of testosterone in men and higher levels in women increase the risk of metabolic syndrome and diabetes.8,9 However, the crucial role of obesity as an independent risk factor for hypertension and type-2 diabetes mellitus is well supported by published evidence. 10 Moreover, obesity nullifies estrogen-related protection from cardiovascular disease (CVD) and raises the risk among premenopausal women with obesity. 11 Population-based studies from Sub-Saharan Africa, Taiwan, and other parts of the world have confirmed that multimorbidity with hypertension and type-2 diabetes is more common among adult males than females who are obese as compared to non-obese individuals. Factors, such as increasing age, male sex, obesity, and abdominal obesity, have already been characterized as the main risk factors for hypertension and diabetes.12 -15
Nevertheless, there is a dearth of quality evidence regarding the relative burden of multimorbidity, due to hypertension, type-2 diabetes mellitus, and obesity among males versus females. Comparing the actual burden of multimorbidity among males and females will result in better risk stratification. Stratification of the multimorbidity burden based on an individual’s sex will help in identifying and implementing targeted prevention and control interventions or measures to reduce the overall morbidity, and mortality by non-communicable diseases. This study aims to determine the sex and age differences in these conditions, and to compare the related multimorbidity.
Methods
This cross-sectional retrospective study used the electronic health records of all primary care centers in the Second Health Cluster in Riyadh, Saudi Arabia. Records were reviewed and data was extracted from March 2022 to March 2023. The total sample size obtained was 375,802 records after quality checking and removal of missing data. The variables considered in this study were as follows: Age, Sex, Body Mass Index (BMI), Obesity, Diabetes, Hypertension, and multiplicity of occurrence of chronic conditions. The clinical diagnoses were based on the physician diagnoses which are based on the guidelines from the Ministry of Health.
Data were reported as mean and standard deviation (±SD), median and interquartile range (IQR), or frequency and percentages (%). Categorical data were compared using the chi-square (χ2) test. To determine the association between the occurrence of obesity, diabetes, and hypertension, together with sex and age, 2 regression analyses were conducted. A multivariate probit estimation methodology was employed using a 3-equations multivariate multiple probit model to jointly estimate the association of the explanatory factors (eg, sex and gender). This included the diagnosis of the 3 chronic conditions of obesity, diabetes, and hypertension using a nonlinear (cumulative standard normal distribution) function to model the conditional probability function of these binary dependent variables. This functional form ensures that the predicted conditional probabilities of the dependent variable lie between 0 and 1. This 3-equation model was fitted using the simulated maximum likelihood of using the Geweke-Hajivassiliou-Keane (GHK) simulator through the utilization of the Cappelari-Jenkins Stata (version 12, StataCorp, TX, USA) routine (mvprobit). The rationale behind this methodological strategy is that these 3 chronic conditions are usually highly correlated; therefore, estimates of separate equations for each condition would be inefficient. As the explanatory factors were categorical, the Probit coefficient β was expressed as an odds ratio to facilitate comparisons between the categories.
Further, as these diseases are related and possibly complementary, a patient will likely be diagnosed with none, only 1, or jointly with more than 1 disease. A multinomial logistic regression analysis was conducted to enable each unique combination of these 3 chronic diseases (ie, obesity only, diabetes only, hypertension only, obesity and diabetes, obesity and hypertension, diabetes and hypertension, obesity and diabetes and hypertension, and with the base category being none of these) to be estimated separately using the IBMSPSS (version 23, INM Corp, NY, USA) NOMREG routine was used. In both models, the male group was fitted as the referent group, and age was categorized as: <25, 25 to 35, 36 to 5, 46 to 60, and >60 years. All the tests were 2-sided and a P-value <.05 was considered significant.
Results
The total study sample included was 375,802 patients. Of these, 186,664 (49.7%) were females. The mean (±SD) age was 39.7 (27.9), the median (IQR) was 36 (28-49), and the range (Minimum-Maximum) was 18 to 100 years. The mean (±SD) body mass index (BMI) was 27.9 (6.1), the median (IQR) was 27 (24-31), and the range was 15 to 51. Approximately one-third of the study subjects were obese, and 4.7% and 3.6% were diagnosed with diabetes and hypertension, respectively. Of all the patients diagnosed with none, only 1 or more of these 3 chronic conditions, those diagnosed only with obesity amounted to 108,851 (29%), only with diabetes 7,698 (2.1%), only with hypertension 4,862 (1.3%), only obese and diabetes 6,232 (1.7%), only obesity and hypertension 4,775 (1.3%), only diabetes and hypertension 1,784 (0.5%), and those jointly diagnosed only with these 3 chronic conditions to 1,952 (0.5) (Table 1).
Patients’ Characteristics (n = 375 802).

In relative terms, in a stratified analysis, statistically significant differences exist between males and females. Compared with males, females present as a significantly higher proportion of patients diagnosed with obesity (59.1% vs 40.9%; P < .05), hypertension (54.3% vs 45.7%; P < .05), but with a significantly lower proportion of those diagnosed with diabetes (45.3% vs 53.7%; P < .05) (Figure 1). Regarding age, a significant (P < .05) increase in the proportion of patients diagnosed with each of the 3 chronic conditions was observed with increased age. The only exception was the obesity condition; those with age >60 years (16%) had a relatively lower proportion compared with those aged 25 to 35 (21.8%), 36 to 45 (25.2%), 46 to 60 (27.6%) but higher than those aged <25 years (Figure 2).
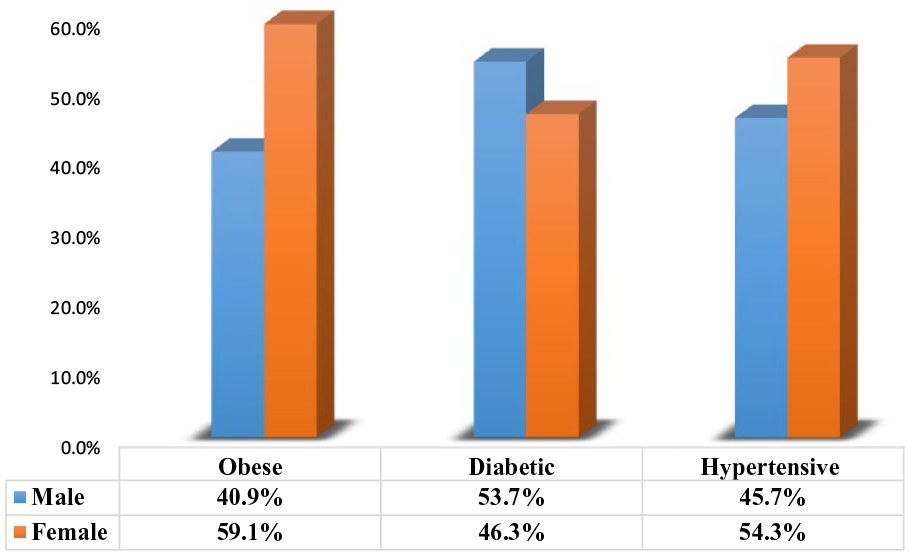
Percentage of patients diagnosed with the 3 chronic diseases by sex category (all P < .05).

Percentage of patients diagnosed with the 3 chronic diseases by age category (all P < .05).
In the stratified analysis that was conducted to compare the different combinations of diagnoses by sex, statistically significant differences were observed between males and females (P < .05). Compared with males, females had a higher proportion of obesity (58.1% vs 41.2%), obesity and diabetes only (58.9% vs 41.1%), obesity and hypertension (63.6% vs 36.4%), and joint diagnosis with the 3 conditions (65.7% vs 34.3%) but with a lower proportion of individuals not diagnosed with any of the 3 chronic conditions (45.5% vs 54.5%), diabetes alone (33.5% vs 66.5%), hypertension alone (47.3% vs 52.7%), and those diagnosed with diabetes and hypertension alone (35.9% vs 64.4%) (Figure 3). In a similar analysis stratified by age category, an increased proportion of individuals with these single or joint conditions was observed by age advancement. The only exception was that compared with individuals in other age categories, patients aged >60 years had a relatively lower proportion of those without any of these 3 chronic conditions (18%) or those diagnosed only with obesity (13.1%), except for those aged <25 years (10.24%) (Figure 4).

Percentage of patients with single or combined diagnosis of the 3 chronic diseases by sex category (P < .05).

Percentage of patients with single or combined diagnosis of the 3 chronic diseases by age category (P < .05).
The results of the multivariate multiple probit analysis are presented in Table 2. Compared with females, males were significantly less likely to be diagnosed with obesity (Odds Ratio (OR) = 0.73, 95% Confidence Intervals (CI): 0.72-0.74, P < .0001) or hypertension (OR = 0.95, 95% CI: 0.94-0.97, P < .0001), but more likely to be diagnosed with diabetes (OR = 1.12, 95% CI: 1.09-1.13, P < .0001). Concerning age, the increased likelihood of diagnosis with all 3 chronic conditions was observed with increased age. However, for obesity, those aged >60 years (OR = 2.06, 95% CI: 2.03-2.09) had a slightly significant lower likelihood of diagnosis compared with those aged 46 to 60 years (OR = 2.11, 95% CI: 2.08-2.14), although both had increased diagnosis compared with those in other age groups. In addition, for diabetes, those aged 25 to 35 years had a lower likelihood of diagnosis (OR = 0.99, 95% CI: 0.99-1.03) compared with the referent group (those aged <25 years), although this was not statistically significant. For hypertension, a hierarchical order was observed; while the increased likelihood of the disease with increased age, with those aged >60 years had the highest likelihood of the disease (OR = 5.64, 95% CI: 5.33-5.96 compared with the referent group; those aged <25 years).
Three-equations Multivariate Multiple Probit Regression Analysis.

ρ Obesity Diabetes P = .08, ρ Obesity Hypertension P = .09, ρ Diabetes hypertension P = .31.
In the multinomial logistic regression that was fitted to determine the likelihood of a single or combined occurrence of the 3 chronic conditions by sex and age category, females had consistently significantly higher likelihood of diagnosis compared with males, except for diabetes (OR = 0.59, 95% CI: 0.56-0.62) and the combination of only diabetes and hypertension (OR = 0.67, 95% CI: 0.61-0.74) (Table 3). The likelihood of other combinations ranged from OR = 1.04, 95% CI: 0.98 to 1.10 for only hypertension to OR = 2.30, 95% CI: 2.10 to 2.53 for the joint diagnosis of all 3 conditions. Regarding age, an increased likelihood of single or combined occurrence of the 3 chronic conditions was observed with increased age. Compared with those aged <25 years, the likelihood of diagnosis with only diabetes ranged from OR = 1.33, 95% CI: 1.29 to 1.36 in those aged 25 to 35 years to OR = 3.2, 95% CI: 3.10 to 3.29 in those aged >60 years.
Multiple Multinomial Regression for Likelihood of a Single or Combined Occurrence of the 3 Chronic Diseases by Sex and Age.

Overall referent group: No diagnosis.
For obesity alone diagnosis, however, those aged 25 to 35 years had a significantly lower likelihood of diagnosis compared with the referent group (those aged <25 years) (OR = 0.84, 95% CI: 0.75-0.94). Compared with those with only a diagnosis of obesity or diabetes, those with alone diagnosis of hypertension had more variation by age, with the older age category exhibiting higher likelihood. This pattern was also apparent in patients with all different combinations of diagnoses, although it was more pronounced in those jointly diagnosed with diabetes and hypertension alone (ranged from OR = 2.09, 95% CI: 0.85-5.19 in those aged 25-35 years to OR = 444.50, 95% CI: 199.2-991.87 in those aged >60 years) as well as those diagnosed with all the 3 conditions (ranged from OR = 2.06, 95% CI: 0.77-5.55 in those aged 25-35 years to OR = 564.27, 95% CI: 234.36-1,358.56 in those aged >60 years). However, these large estimates and associated wide confidence can potentially be explained by the relatively small sample size in these groups.
Discussion
This study was conducted to assess the burden, and patterns of multimorbidity caused by hypertension, diabetes mellitus, and obesity in the adult population with the aim to compare the situation among men versus women. The study sample was comprised of an approximately equal proportion of male and female patients; however, approximately 30% of them were between the ages of 25 and 35 years with a median age of 35 years (IQR = 21 years). Only 32.4% of the study participants, though, were obese, while 4.7% were diabetic and only 3.6% were hypertensive.
The burden of multimorbidity in this study was relatively higher for the patients who suffered from obesity and diabetes mellitus, followed by hypertension and diabetes mellitus and obesity along with hypertension with the proportions of 1.7% and 1.3%, respectively. Among all 3 morbidities, female patients were found to share a considerably more significant burden of obesity and hypertension. The global trends in obesity also show a higher prevalence of obesity in women compared to men for all age groups. 16 The relatively higher burden of obesity among men and women is mainly observed between the range of 50 to 65 years of age and then declines slightly after that. 16
However, male patients were found to share a more significant proportion of type-2 diabetes mellitus. This finding can be further explained by the previous evidence that reports a prevalence of type-2 diabetes in the male sex, as compared to females. 17 This male predominance for type-2 diabetes mellitus, however, is reported to be reversed when compared to females in the postmenopausal age. This can be further explained by the role of androgens in the pathophysiology of type-2 diabetes mellitus, as well as differences in cardiometabolic risk profiles of men and women at similar ages, and the same BMI.17,18
The highest burden of obesity was observed among patients between 36 and 60 years of age, while the burden of diabetes mellitus and hypertension was higher among patients at the ages of 46 years and above, with the highest proportions among patients with ages greater than 60 years of age. The age-specific distribution of obesity is relevant, as mono-morbidity shows the highest burden of obesity among age groups ranging between 36 to 45 and 46 to 60 years of age. However, the highest burden of diabetes mellitus and hypertension as mono-morbidity was observed among patients 46 years of age and above. This can be explained by the widely known expression of hormones, gender-specific roles, social behaviors, the natural history of non-communicable diseases, as well as lifestyle-related risk factors.
The study found a negative association of male sex with obesity and hypertension compared to females as the reference group. The male sex, nevertheless, was found to present a positive association with type-2 diabetes mellitus. These findings correlate with the newly emerging evidence that reports a relatively higher risk of early onset pathogenesis for cardiovascular disease among females, which is in contrast to previous theories that emphasize delayed development of hypertension among females.17,18 However, the sex-based prevalence of diabetes mellitus and hypertension may also vary in different stages of life and in different age groups. 17 The likelihood of all 3 chronic diseases, that is, diabetes mellitus, hypertension, and obesity), among different age group categories, showed a persistent rise, with advancement in age, with the highest likelihood among individuals aged 60 years and above. This finding corresponds with the current evidence and can be explained by the increased risk of cardiometabolic disorders with a rising age irrespective of sex.12,14,17
This study also assessed the likelihood of multimorbidity caused by diabetes mellitus, hypertension, and obesity among females as compared to males by applying multiple multinomial regression. The study identified that the females were more likely to be obese but less likely to be hypertensive as compared to males. The odds for hypertension were statistically insignificant and might be affected by the role of obesity in developing hypertension which reduces the protective effect of estrogen among females.3,11 Moreover, the literature reports an inverse relationship between age at the onset of hypertension and BMI, which is relatively more evident in males compared to females. 19
When multimorbidity was assessed, it was found that the likelihood of suffering from obesity and diabetes mellitus together was 1.6 times more among females as compared to males. Similarly, the likelihood of having obesity and hypertension together was 2 times higher among females, compared to the likelihood of presenting with obesity and hypertension as multimorbidity among males. This finding, though, is in contrast to previous evidence; it can be explained by the considerably higher burden of obesity among women in the current study sample, which makes them prone to the development of hypertension, as supported by previous evidence.19,20 Furthermore, the likelihood of having all 3 chronic diseases, namely diabetes, hypertension, and obesity, was 2.3 times higher if the individual were a female compared to the male, possibly resulting in the neutralization of estrogen effects due to BMI. 19
Nevertheless, it was observed that being a female reduced the likelihood of having diabetes and hypertension simultaneously as multimorbidity compared to males. This finding is well supported by previous evidence that identified hyperglycemia as a risk factor for hypertension among men compared with women with type 1 diabetes or type 2 diabetes mellitus.19,21 This study found variability in multi-morbidity based on the variation in age groups. The statistically insignificant odds for multi-morbidity due to diabetes mellitus and hypertension were observed among individuals aged between 25 and 35 years. Similarly, the study found no statistically significant results for the likelihood of developing multimorbidity caused by the simultaneous occurrence of all 3 chronic diseases diabetes mellitus, hypertension, and obesity. This can be explained by age-related physiology and lifestyle-related factors, as well as the possible role of the long latent phase of chronic diseases.
The high likelihood of developing multi-morbidity due to diabetes, hypertension, and obesity was observed with advancement in age. However, the very high values of odds (95%) in confidence intervals estimated for multi-morbidity in the older age groups (ie, 46-60 and >60 years) can be explained by the relatively fewer individuals or patients, in these age groups or categories. The literature identifies multi-morbidity as an essential indicator for increased service utilization in any healthcare setting. 22 In the current study’s population, the likelihood of multi-morbidity due to selected non-communicable diseases increased after 35 years of age, reflecting the possible burden and type of healthcare services required to fulfill the population’s healthcare needs. Such a form of evidence can also be helpful in the detailed planning of disease management, including screening strategy and related services.
The most frequent multimorbidity estimated among male patients was hypertension and diabetes mellitus, while among female patients, the most commonly occurring multimorbidity was obesity and hypertension. The positive association between hypertension and the development of diabetes mellitus and the increased risk of hypertension among obese, which is widely reported in published literature.19,23 Meanwhile, the most frequent multimorbidity observed among female patients was obesity and diabetes, however, among male patients, the most frequent multimorbidity was diabetes mellitus and hypertension.19,20,24 This finding can be explained by the naturally high prevalence of obesity among women and its strong association with glycemic control and diabetes. However, the relatively higher burden of hypertension and diabetes is already well established by previous research that explains the higher burden of diabetes in men.22,23
The current study offers a unique opportunity to estimate and compare the burden of morbidity and multi-morbidity based on sex differences and different age groups with a considerably large sample size. Nonetheless, this study had a few inherent limitations. The use of electronic records did limit the availability of potential confounders, including smoking, socioeconomic class, level of physical activity, marital status, and family history of chronic diseases, particularly diabetes mellitus, hypertension, and obesity. Moreover, the generalizability of these findings with a similar population can be affected by any possible differences between the study population and the actual target population to whom generalizations can be made. Further, the data were taken from primary healthcare centers so there might be a chance of under prevalence of diabetes and hypertension (Berkson’s paradox). Another important limitation is that ethnicity is hugely influential in the HT/diabetes/obesity triad and is not mentioned here. As is the different ethnicity-specific BMI cut-offs for obesity 30 kg/m2 in the White population, and 23.9 kg/m2 in South Asians. It is also worth mentioning the caveat that hypertension and diabetes are themselves heterogeneous conditions, with large differences in aetiology between, for example, hypertension in the young or elderly or across ethnicities. This will affect the relationship with the 2 other morbidities if everything is averaged together.
Conclusion
The multimorbidity distribution for diabetes mellitus, hypertension, and obesity significantly differs among male and female patients. Individuals over 35 years old are more prone to have at least one of the selected chronic diseases of diabetes mellitus, hypertension, and obesity. The overall burden of morbidity, and mortality, however, tends to rise after 46 years of age, with the highest burden among individuals above 60 years of age. Furthermore, it can be determined that large-scale prospective studies must be conducted inclusive of all the potential confounders to determine the sex- and age-based differences in the morbidity, and multimorbidity caused by diabetes, hypertension, and obesity.
Footnotes
Acknowledgements
The authors highly acknowledge the contribution of all study participants.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.